
Abstract
Purpose:
To report a case of endophthalmitis following bleb needling in a patient previously implanted with a PRESERFLO® MicroShunt.
Methods:
Case report.
Results:
A 40-year-old woman with bilateral malformative glaucoma repeatedly operated on in childhood underwent PRESERFLO® MicroShunt implantation in her right eye and six needling revisions (NRs) and a surgical revision due to unsatisfactory intraocular pressure (IOP) control due to bleb encapsulation. About 3 months after the surgical revision the bleb encapsulation relapsed and she underwent a further NR with betamethasone. About 4 days after the last NR, she experienced visual acuity reduction and was therefore advised to come immediately to the hospital for an unscheduled visit, showing up with hypopyon and diffuse vitreous haze. A clinical diagnosis of endophthalmitis (later confirmed by bacteria culture tests) was made and she was treated with pars-plana vitrectomy with silicone oil and intravitreal antibiotics. Preoperative visual function was luckily completely restored.
Conclusions:
Endophthalmitis can occur after NR in an eye with PRESERFLO® MicroShunt implant which therefore does not prevent reflux of bacteria from a filtering bleb to the anterior chamber.
Introduction
Glaucoma is a progressive optic neuropathy and one of the main causes of irreversible blindness worldwide. 1 Increased intraocular pressure (IOP) is the main risk factor for the onset and evolution of glaucoma, and lowering IOP by drugs, lasers or surgeries is mandatory to prevent or reduce the damage of the optic nerve. 2
Traditional surgical approaches typically provide substantial, long-term IOP reduction. They include: trabeculectomy (+/- augmentation with 5-fluorouracil, mitomycin C), non-penetrating drainage surgery (deep sclerectomy), shunt procedures (Valved and Non-valved implants) and cyclodestructive procedures (cyclodiode, cyclocryotherapy).
Among these surgical strategies, trabeculectomy remains the most commonly performed, and it is considered the gold standard for patients with progressive glaucoma despite medical and laser treatment. Deep sclerectomy is considered safer than standard trabeculectomy, but less successful in IOP lowering. Shunt surgery is generally used for patients with uveitis, aphakia or previous failed trabeculectomy, whereas cyclodestructive procedures are usually preferred for painful and/or poorly sighted eyes or when all other measures have failed.2,3
These interventions are burdened by many potential complications, including infections, persistent hypotony and bleb-related problems. 3
In recent years, several new surgery procedures have been developed to effectively reduce IOP in a safer and less traumatic way, with the use of Minimally Invasive Glaucoma Surgery devices (MIGS). 4
The PRESERFLO® MicroShunt (Santen, Osaka, Japan), is a MIGS inserted via ab-externo approach. The device is made of a nonreactive and biocompatible material known as SIBS (polystyrene-block-isobutylene-block-styrene), and shunts aqueous humour from the anterior chamber to a filtering bleb under the conjunctiva and Tenon’s capsule. 5 The safety and efficacy of PRESERFLO® MicroShunt implantation has been evaluated in a large number of clinical trials. 6
Endophthalmitis following glaucoma surgery is a rare but devastating complication with a reported incidence ranging from 0.2% to 9.6%. 7 Endophthalmitis may either arise after trabeculectomy, especially after the introduction of antimetabolites, as well as after MIGS implantation. Moreover, there are several postoperative procedures that can lead to endophthalmitis, including needling revision (NR), laser suture lysis, compression suture and autologous blood injection. 7 NR is an accepted procedure to improve IOP control in poorly filtering blebs. It can be performed either at the ophthalmic surgical microscope or at the slip lamp and its effectiveness can be augmented with different antifibrotic drugs like 5-fluorouracil (5FU), mitomycin C (MMC) or betamethasone. 8
To the best of our knowledge, this is the first case of endophthalmitis following NR of an encapsulated bleb in a patient that previously underwent PRESERFLO® MicroShunt implantation for uncontrolled IOP.
Case description
Informed consent to publish clinical information and images was signed by the patient.
A 40-year-old woman suffering from bilateral malformative glaucoma, uncontrolled despite multiple previous surgeries (two angle surgeries and two trabeculectomies in childhood) and maximum tolerated medical therapy (Brimonidine Tartrate 0.2% b.i.d., 0.5% timolol/0.005% Latanoprost b.i.d., oral acetazolamide 250 mg b.i.d.– and no medication for other conditions), underwent PRESERFLO® MicroShunt implantation in her right eye.
The left eye was functionally lost due to glaucoma. She had undergone uneventful phacoemulsification and in-the-bag IOL implantation in her right eye 1 year before the PRESERFLO® MicroShunt surgery.
Preoperative best correct visual acuity (BCVA) and IOP were 3/10 and 24 mmHg respectively. About 1 week after surgery (Figure 1), BCVA was stable and IOP decreased to 13 mmHg. However, 1 month after PRESERFLO® MicroShunt implantation, IOP control and bleb function became unsatisfactory due to recurrent subconjunctival scarring and bleb encapsulation. Therefore, she underwent six consecutive bleb NRs with betamethasone and lidocaine at the slit lamp. Each procedure was done after disinfection with povidone iodine and was followed by 1 week of topical ofloxacin q.i.d. and throughout the whole follow up she was treated with topical dexamethasone 0.2% q.i.d.
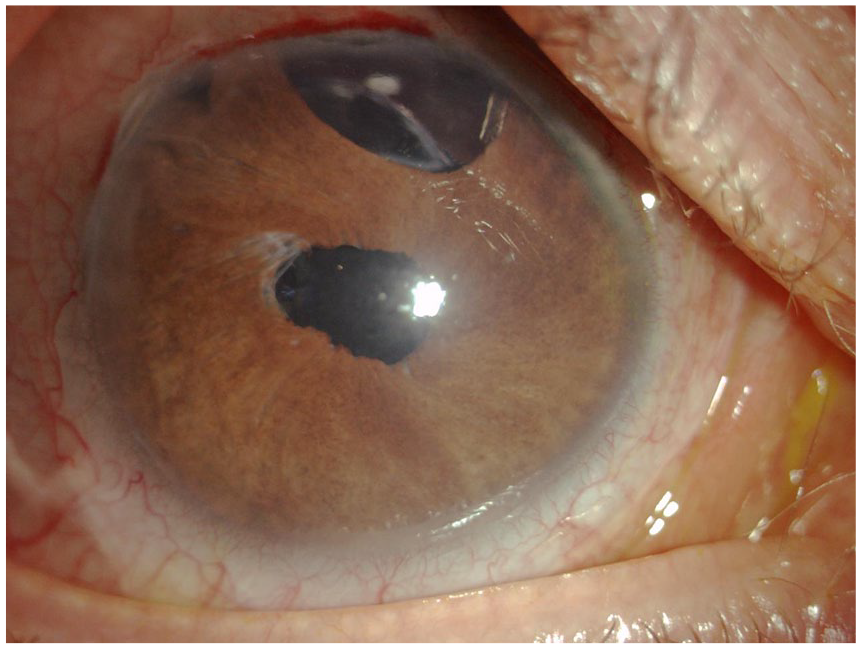
Anterior segment photograph of PRESERFLO® MicroShunt implantation.
About 4 months after device implantation, owing to continuous recurrence of bleb encapsulation (Figure 2), she was brought to the operative room for surgical revision with MMC and bleb filling with cross-linked hyaluronic acid (HealaFlow, Anteis S.A, Geneva, Switzerland). About 3 months after the surgical revision there was a new recurrence of encapsulation, with rising IOP and a huge filtering bleb (Figure 3). Therefore, we decided to perform one last NR with lidocaine and bethamethasone, before giving up and starting a topical hypotensive therapy.
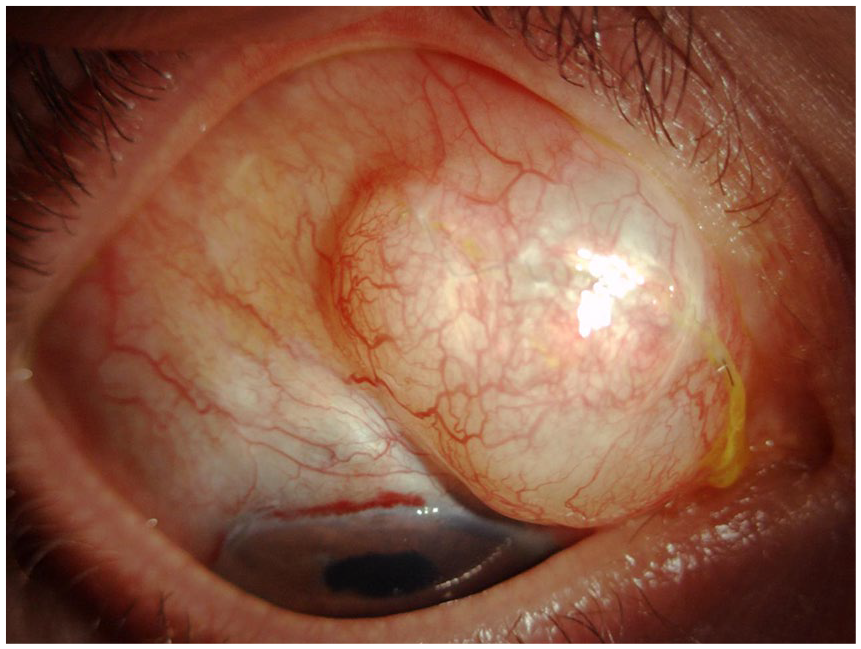
Photograph of bleb encapsulation before surgical revision.
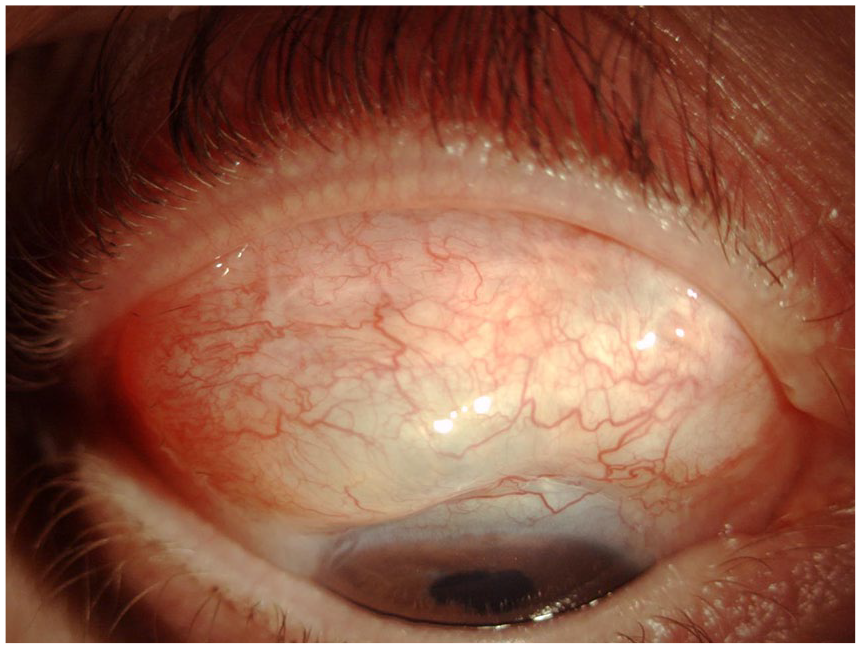
Photograph of bleb encapsulation before the last and fatal NR.
About 4 days after the procedure, the patient complained about ocular redness and reduced visual acuity and was therefore asked to come to the hospital immediately.
BCVA had dropped to hand motion, IOP was 35 mmHg. At the slit lamp, we observed moderate conjunctival hyperemia and chemosis, with no discharge, minimal corneal edema, and a 0.5-mm hypopyon. Surprisingly, the bleb was moderately elevated, non-ischemic, with clear content, apparently untouched by any infection. The fundus could not be observed due to vitreous haze, and an echogram showed a slightly opaque vitreous cavity, with no evidence of retinal detachment.
Considering the clinical presentation an endophthalmitis was highly presumable, despite an apparently quiet bleb, and we therefore decided for a straightforward pars plana vitrectomy. This proved very appropriate, since in less than 3 h, while we admitted the patient, waited for a negative test for SARS-Cov-2 RNA in an oropharyngeal swab, and prepared the emergency operating room, the hypopyon had already become 3-mm high.
A therapeutic pars plana vitrectomy combined with anterior chamber washing and vitreous sampling for microbiological tests was performed. Several hyalinized vessels were noticed in the peripheral retina during the procedure. Vitreous cavity was filled with silicone oil and intravitreal antibiotics (amikacin and vancomycin) were injected. Vitreous microscopic analysis identified Staphylococcus epidermidis as the supposed agent of the infection, and cultural tests and antibiogram confirmed the hypothesis, revealing the growth of a strain of S. epidermidis resistant to quinolones and sensitive to aminoglycosides and vancomycin. Topical reinforced tobramycin and vancomycin were therefore continued once every hour during wake.
The patient left the hospital 8 days after surgery, with a BCVA improved to 1/10 and a 16- mmHg IOP in her right eye on submaximal hypotensive medication. She was prescribed reinforced vancomycin and reinforced tobramycin six times daily, dexamethasone sodium phosphate 0.2% b.i.d., 2% dorzolamide/0.5% timolol b.i.d., 0.5% apraclonidine t.i.d. and oral acetazolamide 250 mg b.i.d. 1 week after, the reinforced drops and the topical dexamethasone 0.2% were withdrawn and an association of tobramycin and dexamethasone q.i.d. was prescribed in substitution.
On the last control visit, 1 month after surgery, BCVA was 3/10 and IOP was 14 mmHg. The device was still in place and the filtering bleb was present but somehow encapsulated again. The patient is presently scheduled for silicone oil removal and we are carefully monitoring her IOP. In case of a new IOP rise there is still the possibility to add a topical prostaglandin analogue and eventually to perform a mild cyclophotocoagulation.
Conclusion
Nowadays, MIGS devices are playing an important role in the management of glaucoma patients. Studies have reported similar results between MIGS devices implantation and trabeculectomy, but with a safer profile and fast recovery with MIGS than with traditional surgery. 5
In fact, traditional glaucoma surgeries could have early complications include wound leakage and hypotony, shallow anterior chamber, serous or haemorrhagic choroidal effusions and late complications such as bleb-related endophthalmitis, bleb leakage, ocular hypotony and associated maculopathy or choroidal haemorrhage, bleb failure and painful blebs. All patients must be informed of the warning signs of endophthalmitis and instructed to seek ophthalmic care immediately if they develop a red eye or other signs of infection. Late-onset bleb-related endophthalmitis is a potentially devastating complication of filtering surgery. 3
MIGS devices with subconjunctival filtration, like PRESERFLO® MicroShunt and XEN Gel Microstent, can obviously be associated with bleb-related complications. Careful postoperative bleb management is nevertheless crucial to achieve the optimal IOP control. 9 In fact, modulation of episcleral fibrosis and scarring process is important to ensure filtering bleb functionality and surgical success. Although reduced by the outspread of antimetabolites, bleb fibrosis and encapsulation is still a predominant cause of surgery failure. NR is a postoperative manoeuvre commonly employed to restore bleb functionality by lysing the fibrous adhesive bands between conjunctiva and episcleral. In order to further reduce inflammation and tissue fibrosis, several substances can be delivered in the subconjunctival space contextually to bleb needling, including 5-FU, MMC and steroids (i.e. betamethasone). 8
Although highly effective with a success rate of 48%–80%, 10 NR may induce several complications such as leakage, failure of filtration and endophthalmitis.
The incidence of endophthalmitis after PRESERFLO® implant surgery is actually unknown.
This device has been introduced in Europe since 2012 and the longest retrospective observational study analysed the outcomes of 23 patients with POAG that received the implant, either solo or in association with phacoemulsification. The safety profile was excellent and no evidence of endophthalmitis was reported. The reported complications included: one surgical failure due to bleb encapsulation requiring the placement of a second MicroShunt, two choroidal detachments resolved with conservative management, one tube blockage necessitating of fibrin removal from the lumen, one persistent ocular hypertension that required late-stage needling, and one early bleb leak that spontaneously resolved within 2 weeks. 5
This case, being complex and burdened by several previous surgeries, did surely not represent a typical indication for MIGS implantation, but this was decided after discussing the options with the patient because she preferred not to undergo a tube implantation (Baerveldt) for the higher risks connected to this procedure. In fact, the conjunctiva appeared mobile and was relatively spared in the upper nasal sector and we therefore decided to implant there the device instead of choosing the superior or superotemporal sectors, and we also accessed the surgical site with a limbus-based conjunctival incision rather than the conventional fornix-based conjunctival pocket to spare a very adherent band of tissue in the limbal area. In this way we could skip the fibrotic area and shunt the aqueous more posteriorly thanks to the length of the device.
Since endophthalmitis has been reported after NR augmented with several substances (i.e. 5FU, MMC), we supposed that in our case its occurrence is likely linked to the needling procedure itself rather than to the PRESERFLO® surgery. However, as far as we know, this is the first case of endophthalmitis following a bleb NR in a patient previously implanted with PRESERFLO® MicroShunt.
The removal of an intraocular device as a suspected source of contamination remains an unclear topic; in our case, we decided to keep the PRESERFLO® MicroShunt in the anterior chamber since quite surprisingly no leakage from the bleb neither any sign of blebitis was evident.
In conclusion, although PRESERFLO® MicroShunt implantation is an effective and relatively safe procedure, it may lead to potentially severe complications such as sight-threatening endophthalmitis, especially when postoperative invasive management of the bleb is required.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.