
Abstract
We report three cases of congenital medulloepithelioma, which is an extremely rare clinical pattern of a tumor rare by definition. The aim of this study is to underline the clinical features of advanced medulloepithelioma in newborns.
Keywords
Introduction
Intraocular medulloepithelioma is a rare, non-hereditary unilateral neoplasm, which arises from the primitive medullary epithelium. The ciliary body is the main structure involved. In rare cases, this tumor can develop from the optic nerve, the iris and the retina. The age of presentation is usually between 2 and 10 years. 1 This tumor was termed “CarcinomePrimitif” by Badel and Lagrange, 2 later Verhoeff 3 called it “Teratoneuroma”. Fuchs 4 defined it as “Dictyoma” as he observed that the principal histological feature was a net-like pattern of cell ribbons. This term, deriving from Greek, means “net”. 5
“Medulloepithelioma” is the latest definition, introduced by Grinker. 6
We report three cases of congenital medulloepithelioma, which is an uncommonclinical variant of this rare tumor.
The aim of this study is to describe the clinical features of advanced medulloepithelioma in newborns. A differential diagnosis with neonatal retinoblastoma is really challenging because they share many common clinical signs and symptoms.
Medulloepitheliomashows in 5% of all cases a correlation with DICER1 syndrome (in association with pleuropulmonary blastoma).
Case reports
Case 1
A 40-day-old male was referred to our hospital forleft eye pain, eyelid hyperemia and leukocoria. Ophthalmic examination under general anesthetic (EUA) revealed orbital cellulitis, buphthalmos, corneal edema, hyperemia, and a bulky, whitish mass occupying the posterior chamber. Intra-ocular pressure was 44 mmHg.
The right eye was normal.
UBM scan of the left eye revealed an isoechogenic mass involving the entire posterior chamber without calcification, with large feeder vessels. Magnetic resonance (MR) imaging showed a largemass that was hyperintense on T1-weighted images and hypointense on T2-weighted MR images. Thoracic Computerized Tomography revealed multiple giant pulmonary cystic lesions in the left lung and smaller ones in the right lung. The diagnosis was therefore pleuropulmonary blastoma in association with medulloepithelioma – DICER1 Syndrome. The patient also underwent genetic test for DICER1 but neither a pathogenic variant nor any variant of potential clinical interest was identified.
Enucleation of the left eye was performed as final treatment in this case, since the advanced clinical status of ocular pain with a poor visual prognosis and a high risk of local infiltration were all alarming signs. The histopathologic examination showed the presence of a malignant teratoid medulloepithelioma with areas of necrosis and hemorrhage, without optic nerve infiltration. The patient died as a result of pulmonary complications associated with cystic lesions (as shown in Figure 1).
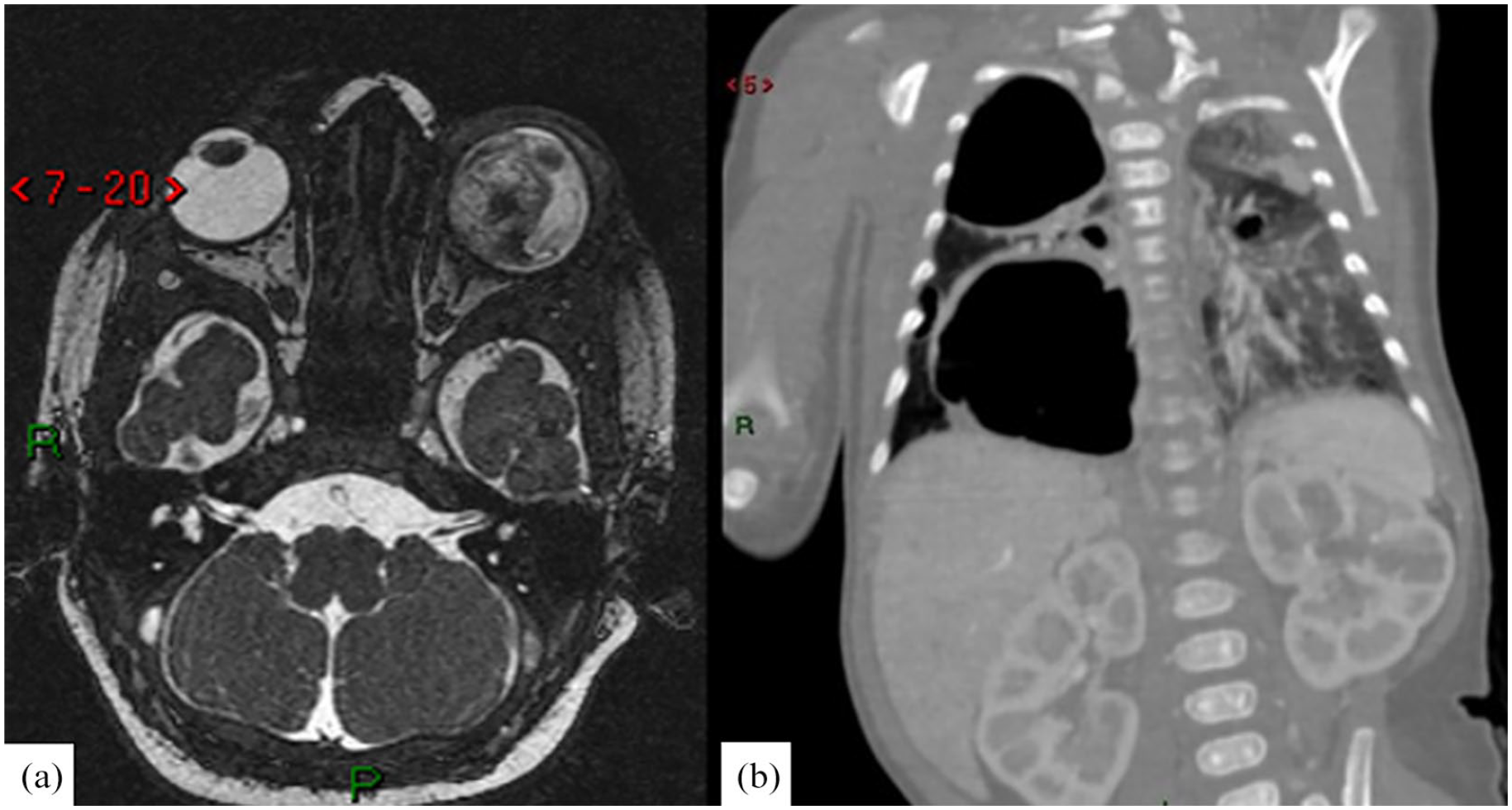
Case 1: (a) T2-weighted image showing a huge heterogeneous mass in the left eye and (b) CT scan showing large cysts of upper, middle and lower lobes of right lung. The thick-walled cysts are associated with signs of atelectasis. Normal kidney lobulation can be seen in this coronal view, no congenital kidney anomalies havebeen demonstrated.
Case 2
A 7-day-old female was referred to our institution for leukocoria and buphthalmos of the left eye. Ophthalmic examinationunder general anesthetic (EUA) revealed rubeosis iridis, cyclitic membrane, and a big mass occupying the whole vitreous chamber. Intraocular pressure was 40 mmHg.
The right eye was normal.
Magnetic resonance imagingconfirmed the presence of a mass in the posterior chamber of the left eye that was dislocating the lens. The signal intensity of the lesion was not homogeneous in both T1- and T2-weighted images. Enucleation of the left eye was performed as unique treatment for a painful blind eye and difficult differential diagnosis with neonatal retinoblastoma. Histopathologic examination revealed the presence of a malignant teratoid medulloepithelioma of the ciliary body with infiltration of choroid and of the intraocular portion of the optic nerve. Genetic examination was not performed. After 5 years of follow-up, there is no recurrence of the tumor and the patient is alive and in good health (as shown in Figure 2).
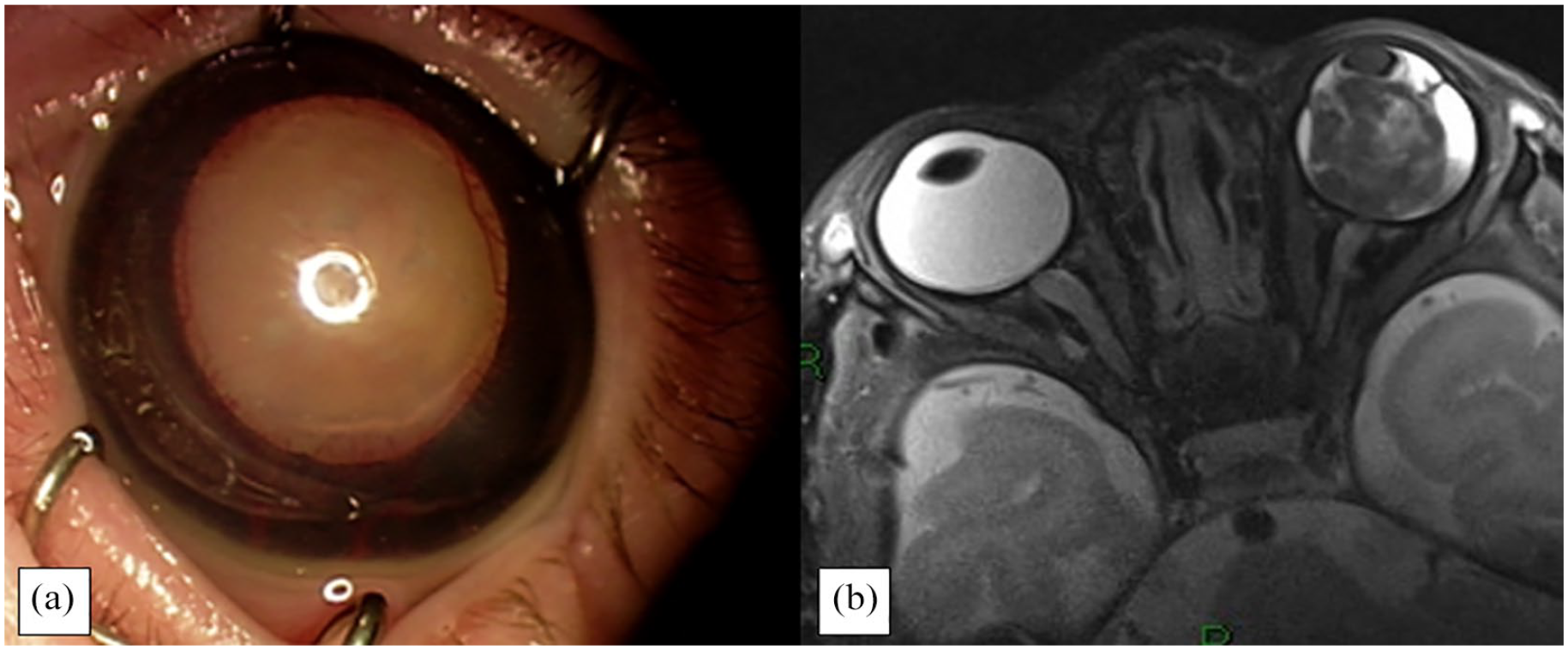
Case 2: (a) retrolental fibrovascular cyclitic membrane and (b) T2-weighted image showing a non-homogeneous mass in left eye.
Case 3
A 10-day-old female was referred to our institution for buphthalmos and an anterior chamber mass in the left eye. Ophthalmic examination under general anesthetic (EUA) showed corneal edema and a whitish mass filling the upper part of the anterior chamber. Intraocular pressure was 38 mmHg.
The right eye was normal.
Magnetic resonance imaging revealed a big ciliary body mass that was hyperintense on T1-weighted images and hypointense on T2-weighted images, and suspected extraocular extension. Total retinal detachment was detected.Enucleation of the left eye was performedas treatment of choice for anterior chamber invasion and poor visual prognosis. In addition, during the procedure the suspected extraocular extension reported in MR imaging was confirmed. Histopathologic examination revealed the presence of a malignant, non-teratoid medulloepithelioma with calcification and sclera infiltrations.Genetic examination was not performed. After 4 years of follow-up, there is no recurrence of the tumor and the patient is alive (as shown in Figure 3).
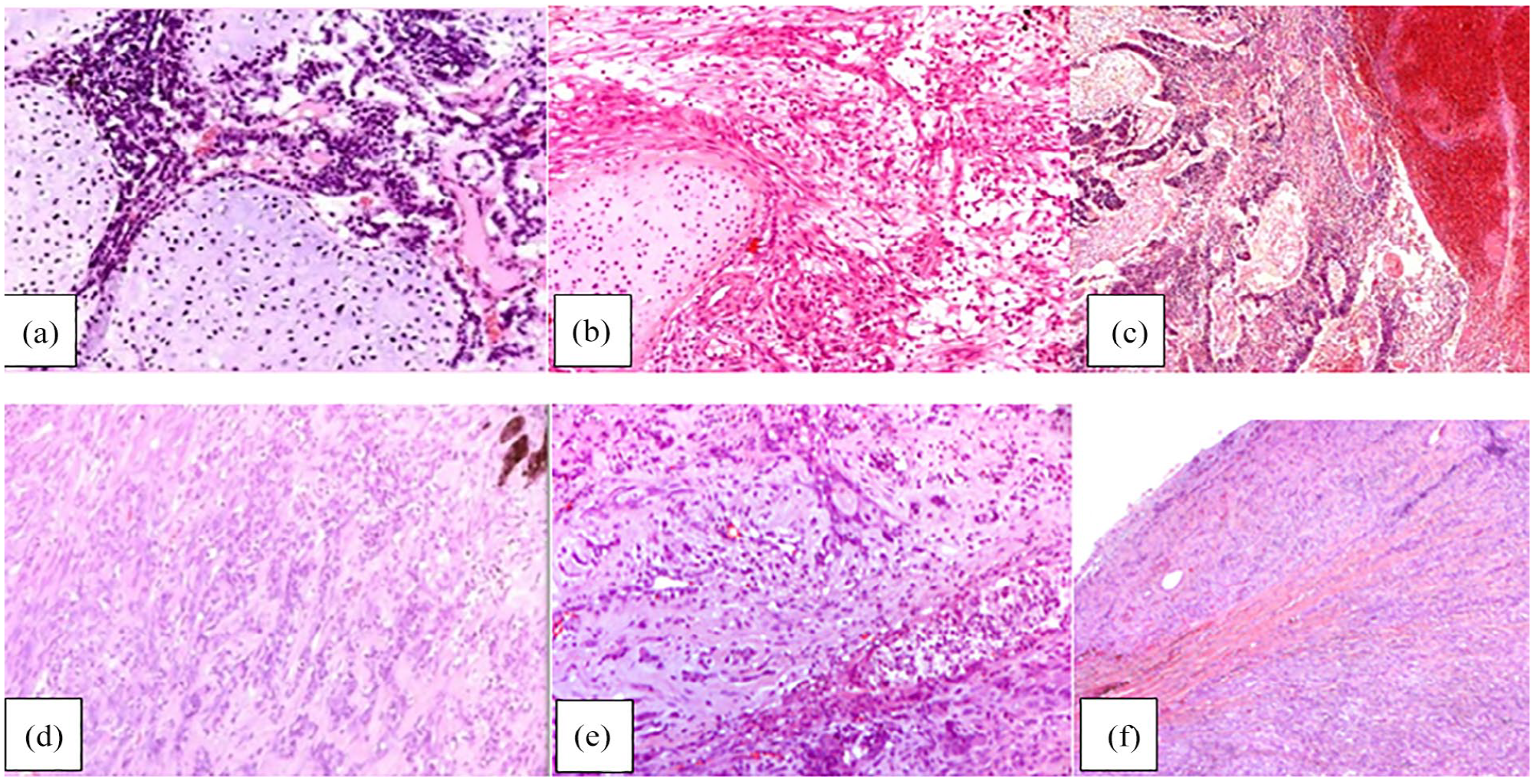
Case 1, malignant teratoid medulloepithelioma: (a) neoplastic cells arranged in tubules and cords, admixed with areas of necrosis and hemorrhages, (b) poorly differentiated neuroblastic component and islands of hyaline cartilage, and (c) extensively necrotic tumor area, in which a cartilage islet can be recognized.
Discussion
Medulloepithelioma is a rare tumor, andthe presence of this tumorin a newborn is an extremely rare condition. In fact, there is no population-based information on incidence and prevalence about medulloepithelioma in literature and only few studies describe this tumor in newborns (as shown in Table 1).7,8
Clinical characteristics of presented cases.
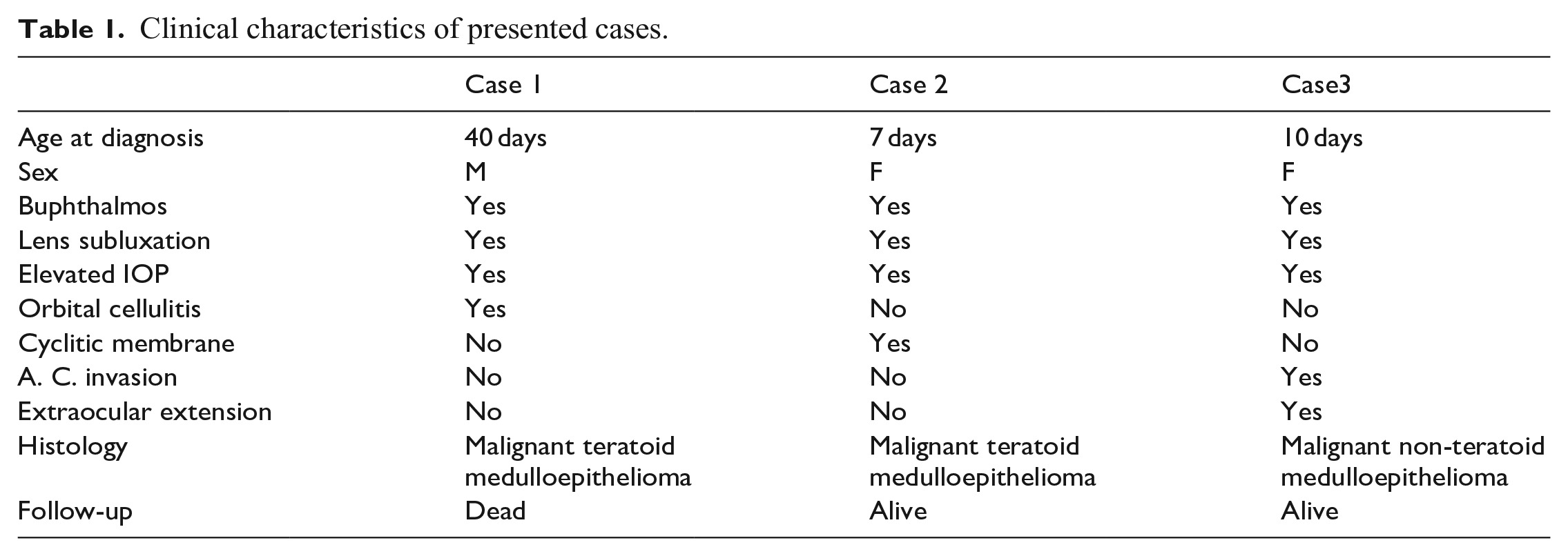
Our three casesare congenital, with an average age at presentation of 19days, while the age of presentation is commonly between 2 and 10 years of age.
There is no correlation with sex; with regard to our cases, they are one male and two females.
From literature, general symptoms of medulloepithelioma are, in order of prevalence: loss of vision, painful eye, leukocoria, conjunctival congestion, and strabismus, althoughit is often completely asymptomatic. Therefore many patients are treated for secondary effectsbefore thetumor mass is discovered.1,9 Our cases, however, share the same advanced and critical clinical status.
All three cases present buphtalmos as a common sign at diagnosis associated with leukocoria; another common feature is represented by a voluminous mass that involves the whole posterior chamber causing lens subluxation in all three cases.
Intraocular pressure was high in all patients, averaging 40 mmHg.
Case number 1 showed orbital cellulitis associated with a red, painful eye, a sign of advanced general inflammation caused by the tumor.
Case number 2 showed cyclitic membrane, a fibrovascular membrane that develops across the back of the lens as a result of inflammation.Cyclitic membrane is a relevant clinical sign, useful to differentiate medulloepithelioma from neonatal retinoblastoma.
Case number 3 had anterior chamber invasion and transscleral extension of the tumor, clear signs of the aggressive growth pattern of this tumor.
Medulloepithelioma can be categorized into teratoid and non-teratoid types, each of which can be subclassified as benign or malignant. 9 Regarding the histopathology of our cases, there is the confirmed diagnosis of a malignant medulloepithelioma that was teratoid in 2 out of 3 cases in association with intralesional necrosis and hemorrhages, while one was non-teratoid.
In 5% of medulloepitheliomas there is a correlation with DICER1 syndrome, which is associated with pleuropulmonary blastoma, characterized by a rare intrathoracic tumor that can develop in children with preexisting pulmonary cystic lesions. Nowadays we identify three pathologic types of pleuropulmonary blastoma:
- Type I: purely cystic tumor
- Type II: cystic and solid tumor
- Type III: solid tumor 1
Our first case was included in the presenting pattern of DICER1 syndrome, with pleuropulmonary blastoma type II. Both lungs were involved with cystic and solid tumor, the right onein particular. Type II and III present the worst prognosis for the malignancy of the tumor and the systemic diffusion of metastasis. Case number 1 died from lung failure due to DICER1 syndrome. Case number 2 and 3 are alive with no recurrence following enucleation. Follow-up was 5 and 4 years, respectively.
The management of this tumor may vary depending on the size and on transscleral invasion or metastasis. Enucleation is usually performed in big tumors and relapses. Plaque brachytherapy is used in small- or medium-sized tumors with a favorable prognosis. Cryotherapy may play a role in small tumors or in limited small relapses.1,9 Our cases underwent enucleation due to the advanced clinical stage characterized by a big mass filling the entire vitreous chamber, and to the risk of local invasion and systemic diffusion of the tumor.
Advanced clinical stage is common in congenital neoplastic lesions, in which tumor growth is fast. This could be explained by the following three hypotheses:
• Cancer cells maydevelop at an early stage after conception, consequently they would have a long time to grow.
• Tumors that originate in the uterus show an abnormal growth pattern.
• The fetal environment is particularly suitable for the growth of immature elements. 10
It is reasonable to identify two distinct phenotypes of this tumor according to the period of manifestation: neonatal medulloepithelioma and childhood medulloepitheolioma. The former presents an advanced clinical status at diagnosis and is characterized by: buphthalmos, leukocoria, big mass in posterior chamber and high intraocular pressure (in differential diagnosis with retinoblastoma), whilemedulloepithelioma in infants is mostly characterized by ciliary body mass, rubeosis iridis, lens subluxation, and secondary glaucoma.
Footnotes
Informed consent
The informed consent for publication of the images has been gathered from the parents of all cases.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.