
Abstract
Purpose:
To assess the efficacy and safety of dexamethasone 0.7 mg implants (DEX-I) in patients with diabetic macular edema (DME) either naïve to therapy or refractory to anti-VEGF treatment, in a single-center, real-world setting.
Methods:
Patients diagnosed with DME and treated with DEX-I were retrospectively enrolled in the study and split in two groups: naïve (Group 1, n = 64) and refractory (Group 2, n = 64) to treatment. Patients were evaluated at baseline, at 1 month, and every 3 months after each DEX-I implant. Main outcome measures were change in best-corrected visual acuity (BCVA) and central macular thickness (CMT) from baseline to follow-up visits.
Results:
Significant improvements in BCVA were observed in treatment-naïve patients at 6 months following the first and second DEX-I injection (p = 0.0023 and p = 0.0063, respectively), with significant reductions in mean CMT at 6 months after all DEX implants. In treatment-refractory patients, mean CMT was significantly reduced from baseline to 6 months (p < 0.05) after all DEX-I injections, although no changes were observed in BCVA.
Conclusions:
DEX-I improved visual acuity and macular edema mostly in treatment-naïve patients, suggesting DEX-I may be a viable first-line treatment option in DME.
Keywords
Introduction
Diabetic macular edema (DME), a common complication of diabetic retinopathy, is characterized by a multi factorial pathogenesis involving the upregulation of vascular endothelial growth factor (VEGF) and inflammatory mediators. For the management of DME, VEGF inhibitors and corticosteroids have been utilized effectively, however, treatment response can vary considerably suggesting that VEGF plays a key role in DME in some eyes, whereas cytokines prevail in others.
Chronic forms of DME appear to be more responsive to corticosteroid treatment 1 and inhibition of VEGF is not completely effective in all patients, with studies showing an improvement of ⩾3 lines in best corrected visual acuity (BCVA) in up to 40% of eyes and of ⩾20/40 for up to 60%, despite six consecutive monthly injections of VEGF inhibitor.2,3 Hence, due to the upregulation of various inflammatory mediatorsin DME, and the wide anti-inflammatory properties of corticosteroids, it seems appropriate to utilize corticosteroids for DME management. 4
Dexamethasone (DEX) is the leading molecule in the class of corticosteroids and its intravitreal biodegradable implant (Ozurdex, Allergan Inc., Irvine, CA, USA), containing 700 µg of active drug, has been developed to prolong molecule half-life in the vitreous for up to 6 months. In the European Union, dexamethasone implants (DEX-I) are indicated for the treatment of adults with visual impairment caused by DME, who are pseudophakic or considered insufficiently responsive to, or unsuitable for, anti-VEGF therapy. 5
The aim of the present study was to further characterize the real-life efficacy and safety of DEX-I in DME patients who are naïve to therapy or who switched from previous anti-VEGF treatment to DEX-I in an Italian ophthalmology center.
Materials and methods
Study design and study population
Patients with a diagnosis of DME and treated with DEX-I 0.7 mg were retrospectively enrolled between February 2015 and August 2018 in this single-center study, performed at the Ophthalmology Department of Ospedali Riuniti, Foggia, University in Foggia (Italy), and followed for at least 6 months.
Main inclusion criteria were age ⩾18 years and a confirmed diagnosis of type 1 or type 2 diabetes managed with oral antidiabetic agents and/or insulin with HbA1c<8% at baseline, non-proliferative diabetic retinopathy, DME with central macular thickness (CMT) >300 µm, and treatment with DEX-I. For patients who received bilateral treatment with DEX, both eyes were included. Exclusion criteria were proliferative diabetic retinopathy, ocular hypertension or glaucoma, associated conditions (such as uveitis, retinal vein occlusion, age-related macular degeneration orneovascular glaucoma), recent intraocular surgery that has probably caused postsurgical macular edema, and prior macular laser treatment within 3 months of commencing DEX-I. Patients who underwent more than five intravitreal injections of anti-VEGF or previously treated with other corticosteroid molecules were also excluded.
Based on previous treatments for DME, patients were split into two groups: Group 1 included subjects naïve to treatment for DME; Group 2 included patients previously managed with anti-VEGF agents (⩽5 intravitreal injections; mean 3.7) with a poor clinical response, which was defined as a reduction less than 50 µm of CMT and improvement in BCVA of less than five letters Early Treatment Diabetic Retinopathy Study (ETDRS).
All patients in both groups were treated with DEX-I at a dosage of 0.7 mg (Ozurdex; Allergan, Inc, Irvine, CA); a single-use applicator system was used to inject DEX-I into the vitreous through the pars plana. Retreatments were possible every 4 months in case of refractory or relapsing DME. Refractory DME was established as aggravation of BCVA by 2 ETDRS lines or diminution of less than 10% of retinal thickness on optical coherence tomography (OCT). Relapsing DME was defined as a complete response 1 month after DEX implant, with a worsening in visual acuity and/or OCT at the fourth month.
Complete evaluation was performed at baseline, at 1, 4, and 6months after each DEX implant, and included measurement of BCVA in log MAR, slit lamp examination, intraocular pressure (IOP) assessment with Goldmann tonometer, ocular fund us examination, and OCT.
Patient data were collected and reviewed for demographic data, HbA1c values, stage of retinopathy(non-proliferative or proliferative), previous treatments for DME, BCVA, CMT, IOP, additional treatment (as well as extra DEX implants or a different intravitreal therapy or macular laser) or cataract surgery throughout follow-up.
Spectral domain optical coherence tomography (Heidelberg Spectralis) was used for OTC scans.
Primary efficacy endpoints included the change in BCVA and CMT from baseline to each follow-up visit. Secondary endpoints included the number of DEX implants dispensed, extra treatments required, and the percentage of cataract extraction and IOP-lowering treatment through the study duration.
Statistical analysis
Statistical analysis was performed on the overall population; comparison of treatment naïve versus non-naïve patients was assessed through group analyses.
Continuous variables were described through means and standard deviations (SD), while categorical variables were described through frequencies and percentages. To evaluate the association between qualitative variables, univariate analysis was performed using double-entry contingency tables and computing chi-square and odds ratio with 95% confidence intervals, with a significance level of ⩽0.05.The assessment of significant differences across the mean of continuous variables relied on the t-test at a significant value of ⩽0.05. Bartlett’s test was used to explore the distribution of variables. Data were processed by STATA-MP software, version 15.0 for Mac OS X.
Results
A total of128 patients with DME were included in the study; 64 each in Group 1 and in Group 2. Overall mean age (± SD) was 69.9 ± 8.7 years (Group 1 = 72.0 ± 9.4 years; Group 2 = 67.7 ± 7.4 years).There were no differences between the two groups at baseline regarding sex, lens status (22 pseudophakic eyes in Group 1 vs 18 in Group 2) and visual acuity; a statistically significant difference was observed forbaseline CMT (±SD) (524.6 µm ± 114.9 µm in Group 1 vs 482.4 µm ± 101.4 µm in Group 2; p = 0.0147).
In Group 1, 42 eyes (65.6%) were phakic at baseline, while 46 eyes (71.8%) were phakic at baseline in Group 2.
The mean follow-up (±SD) was 12.0 ± 7 months in Group 1 and 14.3 ± 6 months in Group 2 (p > 0.05). The mean number of DEX-I injections (±SD) was lower, but not significantly different, in Group 1 vs Group 2 (1.96 ± 1.12 and 2.06 ± 1.2, respectively). Nevertheless, when considering the mean number of injections (performed before and during the observation period), fewer injections were registered in Group 1 vs Group 2, as expected (1.96 ± 1.12 and 5.7 ± 1.3, respectively; p = 0.0000).
During the study period, 28 eyes (44%), 20 eyes (31%), 9 eyes (14%), and 7 eyes (11%), respectively, received 1, 2, 3, and 4 DEX implants in Group 1; for Group 2, this was 27 eyes (42%), 19 eyes (30%), 11 eyes (17%) 3 eyes, and 7 eyes (11%), respectively.
In Group 1, improvement in BCVA was significant from baseline to 6 months following the first and second DEX implants (p = 0.0023 and p = 0.0063, respectively); no differences versus baseline were observed after the third and fourth injections (Figure 1(a)). Regarding anatomical outcomes, a significant reduction in mean CMT from baseline to 6 months was observed after all DEX implants (p = 0.0001, p = 0.0001, p = 0.0010, and p = 0.0108 after the first, second, third, and fourth injections, respectively) (Figure 1(b)). In Group 2, no significant difference in visual acuity from baseline to 6 months was observed after all injections (Figure 2(a)), while mean CMT reduction from baseline to 6 months was significant at all time points after DEX-I injection (p = 0.0001, p = 0.0001, p = 0.0016, and p = 0.0122 after the first, second, third, and fourth DEX injections, respectively) (Figure 2(b)).
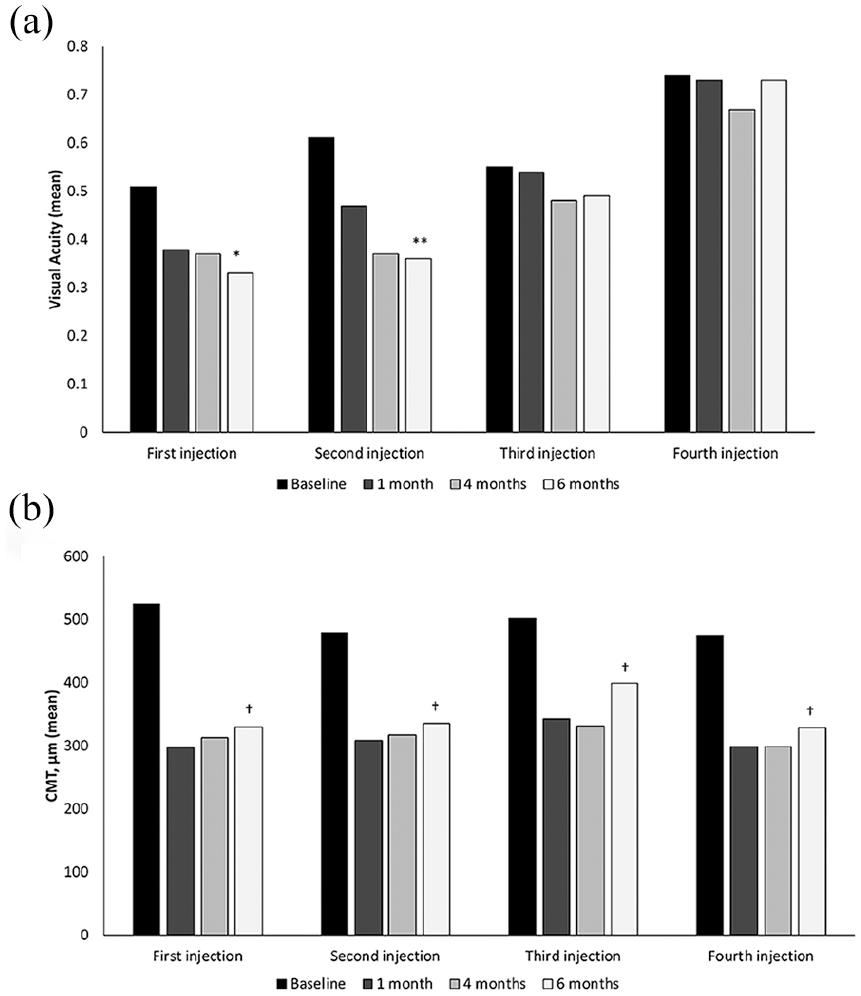
Efficacy outcomes in treatment-naïve DME patients. Mean change from baseline to different timepoints after the first, second, third, and fourth DEX-I injection in: (a) visual acuity (BCVA logMAR score) and (b) CMT (measured with OCT).
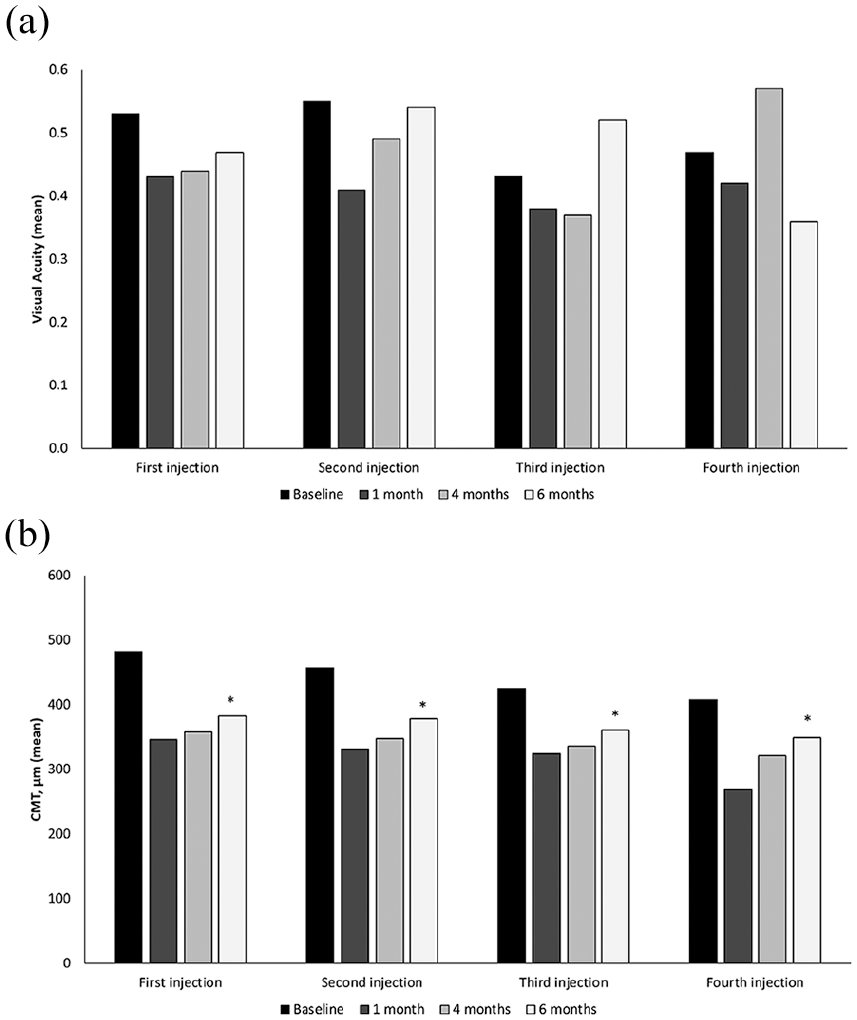
Efficacy outcomes in non-naïve DME patients. Mean change from baseline to different timepoints after the first, second, third and fourth DEX-I injection in: (a) visual acuity (BCVA logMAR score), (b) CMT (measured with OCT).
In Group 1, comparing BCVA and CMT from baseline to last follow-up visit, there was a significantly statistical difference for both values (p = 0.0032 and p = 0 respectively), while in Group 2 was significant only CMT value (p = 0) without remarkable change of BCVA (p = 0.4469).
When comparing naïve vs non-naïve patients at 6 months, the overall efficacy of DEX-I injection on improvement in BCVA (mean log MAR BCVA score ± SD) was higher in Group 1 than in Group 2 after both the first (0.33 ± 0.31 vs 0.47 ± 0.32, respectively; p = 0.0335) and second DEX implants (0.36 ± 0.30 vs 0.54 ± 0.33, respectively; p = 0.0468). No differences were seen vs baseline after the third and fourth injections (Figure 3).

Mean BCVA logMAR scoresinnaïve and non-naïve DME patients at baseline and at different timepoints after the first, second, third, and fourth DEX-I injection.
Comparing the two groups, substantial dissimilarities in mean CMT (±SD) were observed after the first DEX implant at each follow-up visit (Figures 4 and 5), with mean CMT significantly lower in Group 1 compared with Group 2 at 1, 4, and 6 months (297.7 ± 55.6 µm vs 346.8 ± 82.1 µm, p = 0.0001; 312.9 ± 94.1 µm vs 358.1 ± 88.0 µm, p = 0.0029; and 329.5 ± 72.5 µm vs 382.5 ± 87.3 µm, p = 0.0017, respectively). No significant between-group differences were reported after the second, third, and fourth injections (Figure 6).
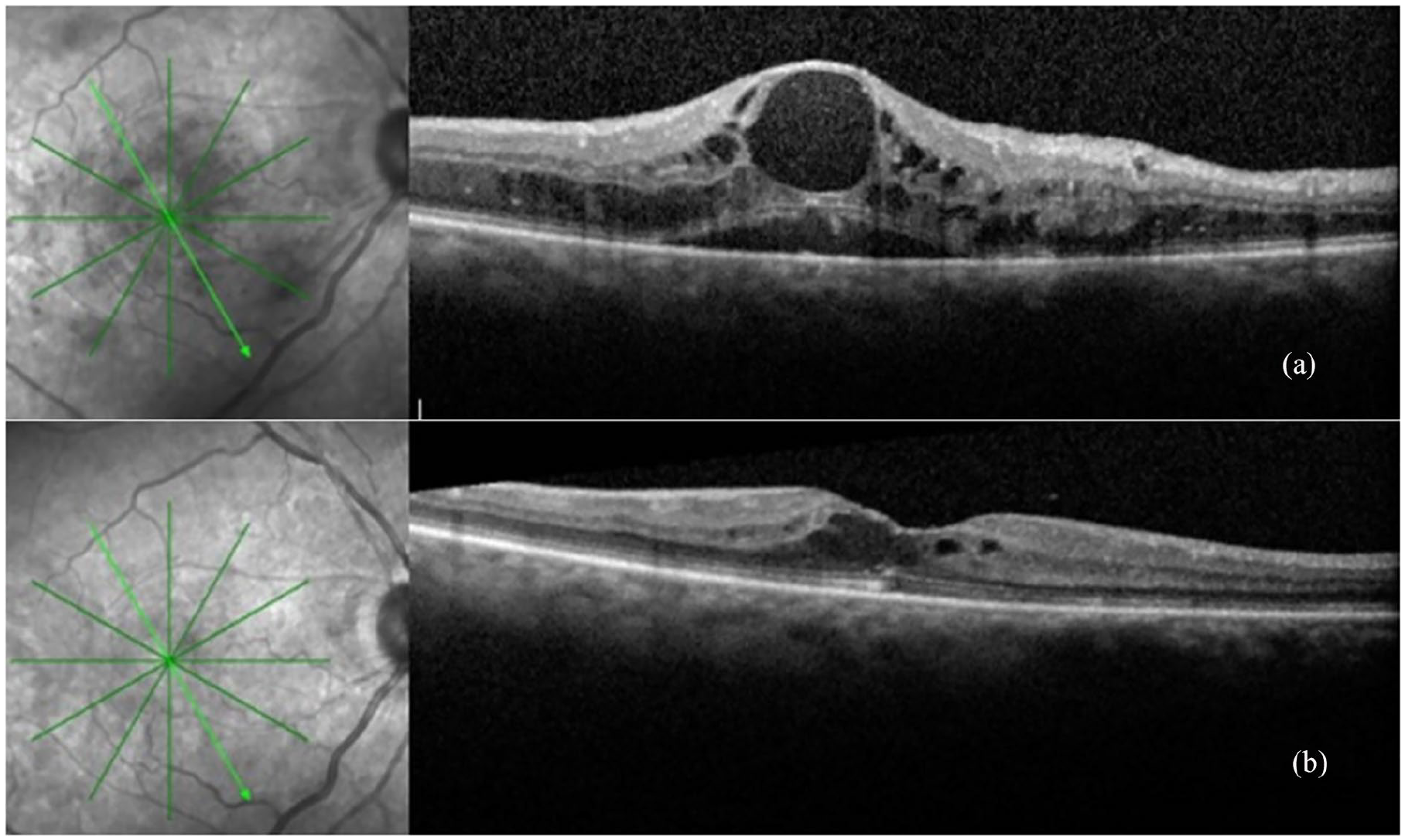
Optical coherence tomography evaluation in a representative patient from the naïve subgroup (a) pre- and (b) post-DEX-I injection.
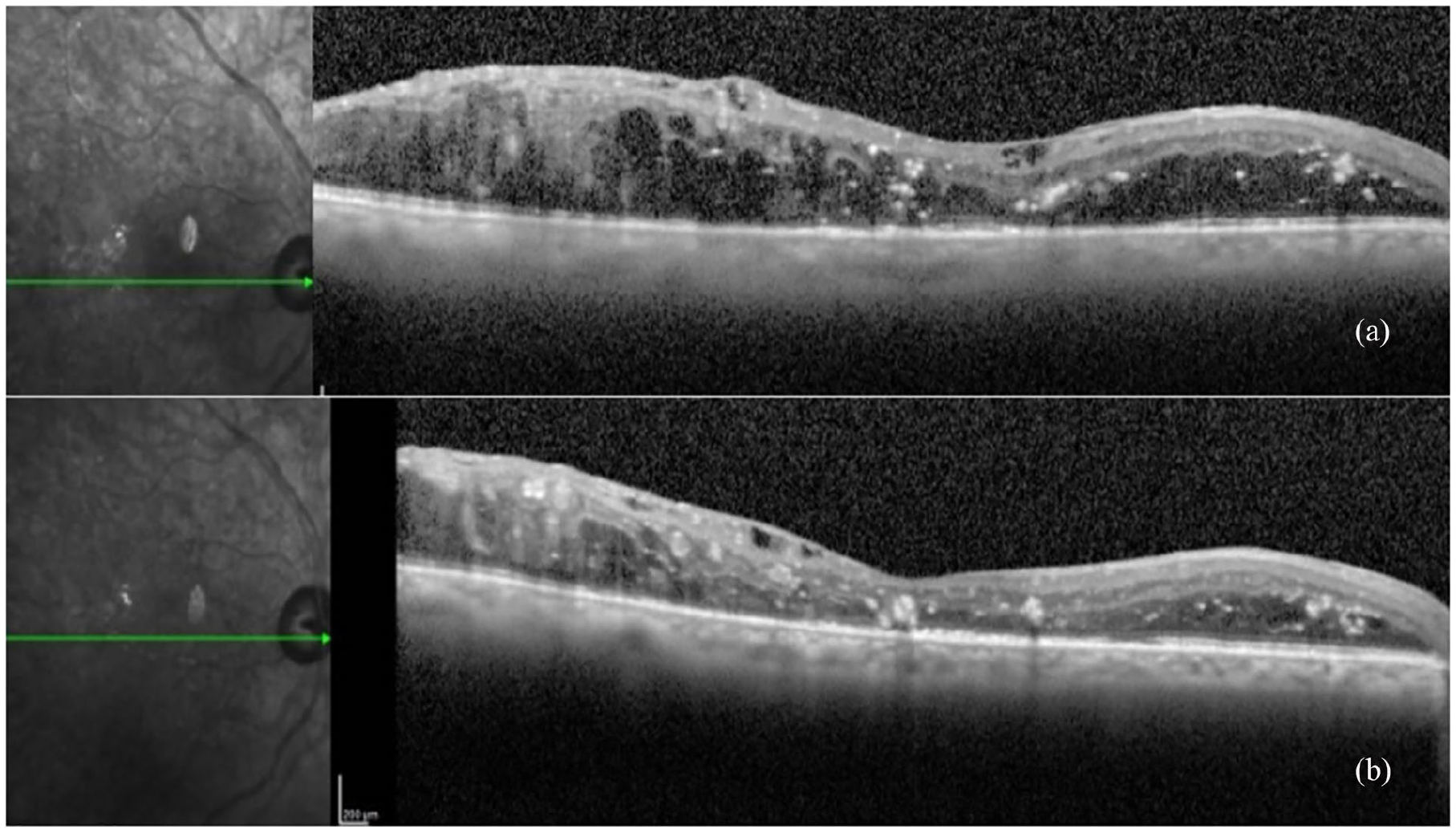
Optical coherence tomography evaluation in a representative patient from the non-naïve subgroup (a) pre- and (b) post-DEX-I injection.
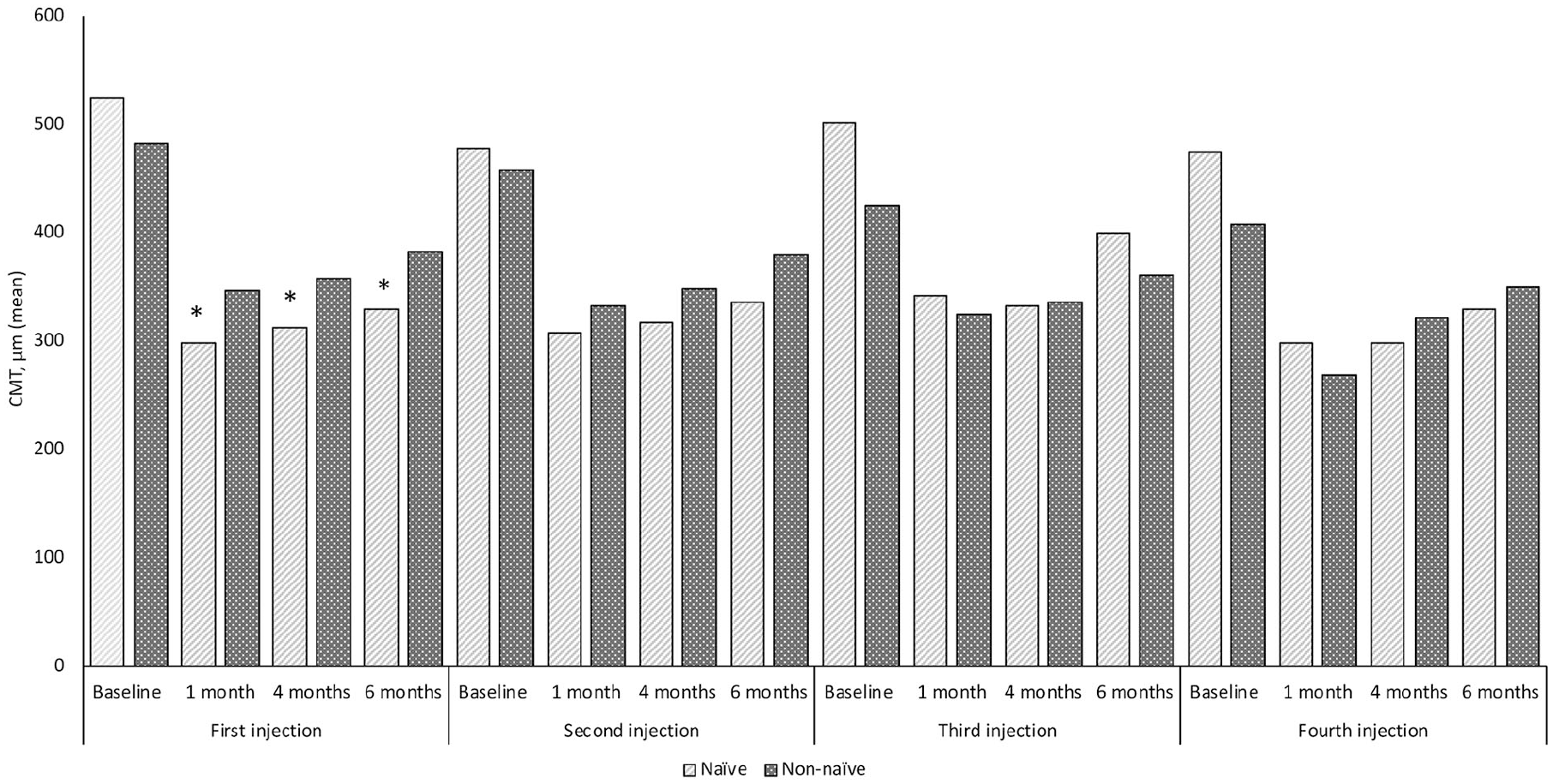
Mean CMT in naïve and non-naïve DME patients at baseline and at different time points after the first, second, third, and fourth DEX-I injection.
Among the phakic eyes, 17 (40.4%) eyes in Group 1 and 8 (17.3 %) eyes in Group 2 underwent cataract surgery (p = 0.016). In Group 1, mean pre-surgery visual acuity (mean log MAR BCVA score ± SD) was 0.55 ± 0.30 and mean post-surgery visual acuity was 0.28 ± 0.25, with a significant difference (p = 0.0034). In contrast, in Group 2 mean pre-surgery and post-surgery visual acuity was, respectively, 0.56 ± 0.28 and 0.50 ± 0.42, with no significant difference (p = 0.3717).
Four eyes in Group 1 (6.25%) and 13 eyes in Group 2 (20.3%) needed therapy for increased IOP (>20 mmHg) (p = 0.019); all cases were managed with topical medications only, and none required surgery. No other adverse events were reported.
During the study period, no patient underwent macular laser photocoagulation.
Discussion
This retrospective study investigated the efficacy and safety of DEX-I injections in 128 patients with a diagnosis of DME, either naïve to treatment or previously managed with anti-VEGF agents, in a real-world setting in Italy. From a clinical efficacy endpoint, substantial melioration in visual acuity from baseline to 6 months of follow-up was observed in patients naïve to treatment after the first and second injections (p = 0.0023 and p = 0.0063, respectively), but not in patients previously treated with an anti-VEGF agent. On the other hand, a significant reduction in CMT was seen from baseline to 6 months after all DEX-I injections in both groups. The same results were evident when comparing BCVA and CMT from baseline to last follow-up visit (p = 0.0032 and p = 0 respectively in Group 1 and p = 0.4469 and p = 0 respectively in Group 2).
When directly comparing the two populations at 6 months, the gain in visual acuity was significantly higher in Group 1 (treatment-naïve) than in Group 2 (non-naïve) following the first (p = 0.0335) and second injection (p = 0.0468), while a significant difference in CMT reduction was evident in favor of treatment-naïve patients after the first injection at all-time points (p = 0.0001, p = 0.0029, p = 0.0017, after 1, 4, and 6 months, respectively).
The lack of significant gain in BCVA in naïve patients after the third or fourth DEX implant is of interest. We presume that this was anatomic, and may have been due to the rearrangement or lack of photoreceptors cells. Certainly, the reason for the lack of visual recovery after the third or fourth DEX implant was not due to the development of cataracts, because in Group 1 only one of 17 eyes underwent cataract surgery after the third implant, while 16 eyes underwent cataract surgery after the first or second implant (data not shown). It is worth noting, however, that in Group 1 only 16 eyes underwent 3 or 4 DEX implants, while 48 eyes were treated successfully with only 1 or 2 DEX implants.
Various randomized clinical trials and real-world experiences have examined the efficacy and safety of DEX-I. The registrational trials in DME were the MEAD studies, which consisted of two identical, randomized, Phase 3 protocols that evaluated the use of DEX-I 0.7 mg and DEX-I 0.35 mg in 1,048 patients with DME over 3 years. 6 Both DEX-I doses achieved the primary efficacy endpoint, measured as a ⩾15-letter increase in BCVA from baseline to 3 years, with visual acuity significantly improved compared with a sham procedure (p ⩽ 0.018 for both comparisons); substantial reductions in CMT from baseline were also demonstrated. 6 The safety profile of DEX-I was characterized by an increase in IOP in 30.8% of DEX-I 0.7 mg treated patients and by cataract-related adverse events in 67.9% of patients receiving the DEX-I 0.7 mg implant.6,7
The efficacy (improved BCVA and reduced CMT) and acceptable safety profile of DEX-I 0.7 mg were further supported by a post-hoc analysis of the MEAD trials in treatment-refractory patients with DME previously treated with laser therapy, intravitreal anti-VEGF agents, intravitreal triamcinolone acetonide, or a combination of these options. 8
In line with this post-hoc analysis, several retrospective and prospective real-world studies have demonstrated the efficacy and safety of DEX-I in DME patients who are naïve to treatment and in those refractory to previous treatments, but with additional advantages in treatment-naïve patients.9–12 For example, a recent multicenter study on329 eyes from 282 patients reported that treatment with multiple 0.7 mg DEX-I injections improved median BCVA (p < 0.001) and decreased median central retinal thickness from baseline (p < 0.001) both in eyes already treated with vitrectomy, laser photocoagulation, or intravitreal therapies (80.7% of evaluated eyes) and in eyes naïve to treatment (19.3%). 12 However, a higher percentage of treatment-naïve eyes gained 15 or more letters from baseline compared with previously-treated eyes (65.4% vs 52.7%, respectively). In our study, the significant improvement in visual acuity from baseline observed in treatment-naïve patients is aligned with results reported in these studies. It should also be highlighted that whilst baseline visual acuity was similar between treatment groups, baseline CMT was significantly higher in treatment-naïve compared with non-naïve patients. This is an important item for the evaluation of the efficacy, because it further emphasizes its value. In addition, our study confirmed a lower number of needed DEX-I injections in patients naïve to treatment vs patients shifted from other therapies, as demonstrated in three other investigations.9,11,13
Different from previous studies, the present results did not document an improvement in visual acuity in treatment-refractory patients during DEX-I treatment. This is in contrast with observations in the above-mentioned studies and in the post-hoc analysis of the registrational MEAD trials.8–12
The worse outcomes observed in non-naïve patients may be linked to delayed initiation of DEX-I treatment, where retinal damage could be more advanced and therefore adversely affect functional results.11,13 This hypothesis is supported by the finding of a reduced visual recovery after cataract surgery in non-naïve patients. While there was a significant difference between mean pre-surgery visual acuity (0.55 ± 0.30) and mean post-surgery visual acuity (0.28 ± 0.25) in Group 1 (p = 0.0034), there was no significant difference between pre-surgery and post-surgery visual acuity in Group 2.
On the other hand, the current study has shown that despite no gain in visual acuity, DEX-I improved retinal anatomical outcomes in treatment-refractory patients, a finding which has also been observed in clinical trials and real-world studies.8,9,11,13,14 This finding suggests that a rapid switch to DEX-I therapy, in the case of failure of clinical response to anti-VEGF agents, may be warranted.
In terms of the anatomical characteristics of DME, the presence of serous retinal detachment or multiple intra-retinal hyperreflective dots (HRD) or foci are arguments supporting an inflammatory etiology of DME. Serous retinal detachment has recently been reported as being associated with higher levels of inflammatory cytokines within the vitreous and aqueous humor of eyes with DME, suggesting there is a significant inflammatory component, especially an increase in interleukin-6 levels. Activated retinal microglial cells have been related to some of the HRD, which can be observed in OCT. These HRD in eyes with DME are referred to as OCT biomarkers of retinal inflammation. Accordingly, it can be inferred that DEX-I could be preferred instead of anti-VEGF therapy for patients with inflammatory biomarkers, although this hypothesis needs to be demonstrated within a clinical setting.15–19
From a safety profile, this study demonstrated a statistically significant difference in IOP increase and the need for cataract surgery between treatment-naïve patients and patients refractory to previous treatment, which is in agreement with the known safety profile of DEX-I injections.5–8 Moreover, no local or systemic safety adverse events were seen during the follow-up period. It should be acknowledged that fewer patients underwent cataract surgery in Group 2 compared with Group 1 (8 vs 17 eyes) despite there being no significant difference in the number of phakic eyes at baseline. Whether this is significant is unknown due to the small patient numbers involved.
Considering the positive risk/benefit profile, DEX-I is recommended in current European guidelines as either first- or second-line therapy in patients with DME 20 and represents a valid therapeutic alternative to other medical treatments, as demonstrated in head-to-head comparisons with anti-VEGF agents in the BEVORDEX Study, where treatment with DEX-I 0.7 mg resulted in a similar proportion of patients with improvement in BCVA ⩾10 letters from baseline to 12 months compared with bevacizumab, but with a lower mean number of injections (2.7 vs 8.6 for DEX vs bevacizumab, respectively). 21
Our real-world study has some limitations, including its single-center setting and retrospective design. On the other hand, the large sample size in both patient groups, and the complete clinical assessment and diagnostic examinations performed in all patients represent a strength of the study and support the results.
In conclusion, naïve DME patients treated with DEX-I injections over a mean of 6 months showed significantly greater improvement in visual acuity, requiring less DEX-I injections compared with patients refractory to anti-VEGF agents. This study further reinforces the available literature regarding the utility of early treatment of DME with DEX-I as a possible first-line treatment option.
Footnotes
Acknowledgements
Writing and editorial assistance was provided to the authors by Health Publishing & Services Srland funded by Allergan SpA, Italy at the request of the investigator. All authors met the ICMJE authorship criteria. Neither honoraria nor payments were made for authorship.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Summary statement
Treatment-naïve DME patients achieved significantly greater improvements in visual acuity and significant reductions in CMT after 6 months’ DEX-I treatment compared with baseline. Treatment-refractory patients also achieved significant reductions from baseline to 6 months in CMT, but visual acuity was unchanged, suggesting DEX-I may be a viable first-line treatment option.