
Abstract
Purpose:
We aimed to investigate the efficacy and safety of single-dose autologous serum eye drops (ASEDs) for treatment of persistent corneal epithelial defects (PEDs).
Methods:
About 34 eyes of 26 patients treated from March 2016 to May 2020 with a single dose of ASEDs for PEDs that did not respond to conventional treatment were retrospectively evaluated. Patient demographics, predisposing factors, size, and duration of the PED, duration of treatment, and dosage of ASEDs, PED healing time, success rate of the ASED treatment, and follow-up time after the onset of ASED treatment were recorded. Autologous serum eye drops (20%) were prepared by diluting the serum with preservative-free artificial tears in single-dose vials. Vials were stored at −20°C and used daily after dissolving.
Results:
The mean patient age was 47.0 ± 18.5 years, and 13 (50%) of the patients were male. The most common indication for ASEDs was PED after keratoplasty. The mean duration of ASED treatment was 8.5 ± 6.3 months, and mean follow-up time was 22.8 ± 12.2 months. Autologous serum eye drop treatment was effective in 25 (73.5%) eyes and partially effective in 5 (14.7%) eyes. None of the eyes displayed complications related to the treatment.
Conclusion:
In patients with PED for whom conservative treatment is insufficient, ASEDs prepared by dilution with preservative-free artificial tears in single-dose vials and administered based on the daily use principle appear to be effective and safe.
Keywords
Introduction
The healthy corneal epithelium acts as a protective barrier against infectious agents via tight junctions and prevents the penetration of infection into the deep ocular structure. Disruptions in this protective epithelial layer can lead to infection, stromal ulceration, perforation, and scarring.1,2 In cases where corneal epithelization is delayed for >2 weeks despite conventional treatment, persistent epithelial defects (PEDs) may occur. 1 Persistent epithelial defects of the cornea can result from tear film abnormalities; ocular surgeries; neurogenic, infectious, and immunological disorders; lid abnormalities; trauma; chemical burns; corneal epithelial and basement membrane disorders; and metabolic disturbances such as diabetes mellitus.1 –7
Tears provide lubrication for the cornea and contain epidermal growth factor (EGF), fibroblast growth factor (FGF), transforming growth factor beta (TGF-β), nerve growth factor (NGF), insulin like growth factor (IGF), fibronectin, lysozyme, Ig A, and serum anti-proteases, which are thought to maintain epithelial health.5,8 –10 EGF, FGF, and fibronectin have been shown to accelerate the healing of epithelial defects10 –13; vitamin A reduces squamous metaplasia in patients with dry eye14,15 and inhibits corneal collagenases of antiproteases such as α2 macroglobulin, providing benefits in alkaline burns 16 ; and lysozyme and Ig G have antibacterial properties.14,16 On the other hand, TGF-β slows epithelial healing and causes scarring and fibrosis. 17
Artificial tear preparations do not contain essential tear components. However, studies have demonstrated that serum contains essential tear components in concentrations comparable to natural tears.5,8
Serum is what remains in the wake of blood clots. Growth factors are released into the serum from platelets during coagulation.1,8,18 These factors are important for cell migration and differentiation at the ocular surface. Concentrations of TGF-β, IGF-1, FGF, vitamin A, fibronectin, and lysozyme are higher in serum than in tears, while concentrations of EGF, NGF, and IgA are lower than those found in tears.18 –22
The use of blood-derived topical therapy in external ocular surface diseases was first reported by Ralph et al. 23 Different methods for the preparation of ASEDs that involve various steps have been described in the literature.18 –24 Today, it is widely used in the treatment of ocular surface diseases related to various etiologies.19,20,23 –25 However, because the serum must be specially prepared for each patient and stored under suitable conditions during the day, the use of autologous serum is limited. We prepared ASEDs in single-dose vials and demonstrated the results in eyes treated with these single-dose ASEDs in cases of PED.
Methods
This retrospective cross-sectional study was approved by the institutional review board and adhered to the provisions of the Declaration of Helsinki for research involving human subjects. Informed consent was obtained from each patient before starting ASED therapy. About 34 eyes of 26 patients treated from March 2016 to May 2020 with single-dose ASEDs for corneal epithelial defect persisting for >2 weeks despite conventional treatment in a tertiary referral hospital were included in this study. Patients who used amniotic membrane products, growth-factor derivative products [Epidermal Growth Factor (EGF), Insulin-like Growth Factor (IGF), etc.], scleral contact lenses, or RGTA matrix therapy; patients with active ocular or lid infections, lid abnormalities contributory to epithelial defect, or a descemetocele; and pregnant and lactating women were excluded from the study.
The characteristics of patients (age, gender, and medical history), predisposing factors, symptoms, size, and duration of the PED, duration of treatment and dosage of ASEDs, PE healing time, success rate of the ASED treatment, and follow-up time after the onset of ASEDs were recorded. Patients were evaluated before the administration of ASEDs, at the third and seventh days after initiation, and then at 2-week intervals until treatment ceased. After the treatment ended, a monthly follow-up was continued. All eyes underwent thorough ophthalmic evaluation; corneal fluorescein staining was performed at baseline and all follow-up visits. The PEDs were measured in the longest diameter and its perpendicular diameter, after administration of 2% fluorescein dye using a standard slit lamp under 10× magnification. The area of the equivalent rectangle was calculated by multiplying the two measured diameters. 26 All examinations were done by the same investigators.
Treatment methods
After diagnosis of PED, all patients were instructed to apply preservative-free sodium hyaluronate 0.15% (Luroan® single dose eye drops, Deva Holding A.S., Istanbul, Turkey) every hour while awake, moxifloxacin 0.5% (Moxai®, Abdi İbrahim A.S., Istanbul, Turkey) four times daily, and carbomer gel (Lipotears® 0.2% gel, Bausch & Lomb A.Ş. Istanbul, Turkey) nightly. Loteprednol 5% (Lotemax®, Bausch & Lomb, A.Ş., Istanbul, Turkey) was added when there was inflammation of the ocular surface. In addition, 20% ASEDs were applied to the eyes of all patients with epithelial defects resistant to conventional therapy. The frequency of application was every 2 h while awake until epithelial healing began; thereafter, application was gradually tapered off until the epithelial healing was completed. All patients were followed up for a minimum of 6 months.
Outcome measures included effectiveness of treatment according to Tsubota’s grading system, 1 duration of healing after initiation of ASEDs, and any adverse effects. The PED treatment was considered “effective” if healing occurred within 2 weeks, “partially effective” if recovery occurred between 2 and 4 weeks, and “ineffective” if recovery was not achieved in 4 weeks.
Preparation technique of ASEDs
Routine virology testing including HbsAg, antibodies to HCV and HIV was performed. An average of 30 ml of blood was taken by phlebotomy from the antecubital vein into tubes without anticoagulant (BD sterile Vacutainer® SST™ II Advance vacuum tubes). The tubes were left upright for a minimum of 4 h at 4°C before they were centrifuged at 3000g for 15 min. An average of 10–15 cc of supernatant serum was obtained. Supernatant serum was transferred into a 1 cc disposable PPD injector under sterile conditions. Then, using sterilizing filters, 0.1 cc of AS was added to the preservative-free artificial tears (Polyvinyl Alcohol + Povidone, Refresh® single dose eye drops, Abdi Ibrahim A. S., Istanbul, Turkey) in a single vial, and 20% ASEDs were prepared. Approximately 90–100 vials of ASEDs were obtained at a time. Each vial was closed and placed in a ultraviolet-A (UV-A) proof box coated with aluminum foil to avoid vitamin-A degradation. The boxes were labeled with name, date of preparation, and dosage frequency and identified as serum for topical use in the eye. The vials were stored at −20°C for a maximum of 3 months. Before use, a single vial was moved to the 4°C region of the refrigerator and stored there on treatment day; the remaining serum was discarded at the end of the day.
All preparation was performed under sterile conditions using a sterilizing filter and single-use sterile supplies to avoid microbial contamination. Blood samples from each patient were manipulated in succession. Three vials were chosen randomly at the end of preparation for culture. In addition, the vial that was opened on the day of the control visit was also cultured.
Visual acuities were expressed in logarithm of the minimum angle of resolution logMAR.
Statistical analysis
Statistical analysis was performed using SPSS Statistics for Windows, version 18.0 (IBM Corp., Armonk, NY, USA). The numerical data are presented as mean ± standard deviation. The Student’s t test was used to compare changes in numerical variables before and after the treatment. The categorical data were presented as percentages. p Value <0.05 was considered statistically significant. Spearman’s correlation coefficient was used for correlations.
Results
About 34 eyes of 26 patients were included in the study. The mean patient age was 47.0 ± 18.5 (median 49.5 range (9–72)) years, and 13 of the patients were male (50%). Systemic diseases were hypertension (19.2%), diabetes mellitus (15.3%), and rheumatoid arthritis (11.5%). Cultures were negative in all samples.
The most common indication for ASEDs was insufficient epithelization after keratoplasty. Other ASED indications and the indications for keratoplasty are summarized in Table 1.
Causes of the PEDs and the indications of previous keratoplasty.
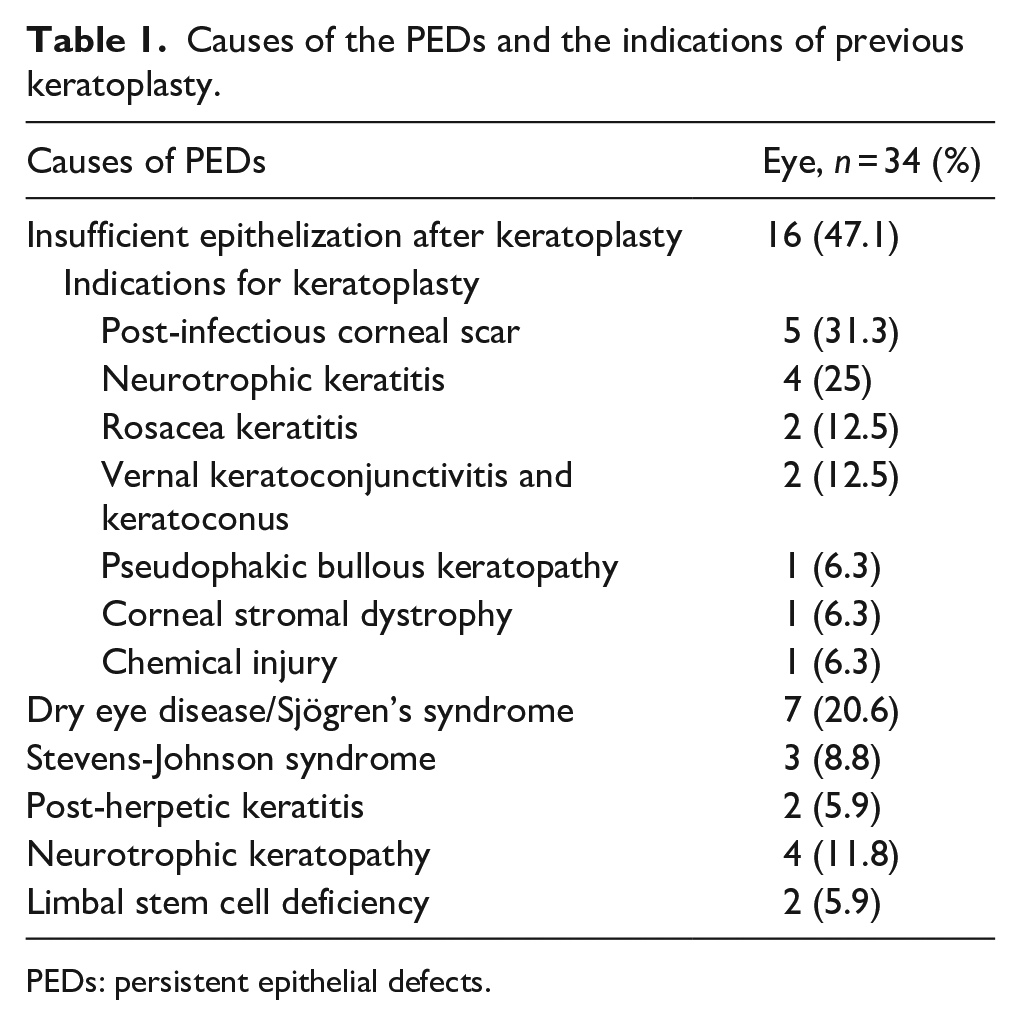
PEDs: persistent epithelial defects.
Before ASED treatment, the PED areas were 5.9 ± 3.1 mm2 in all patients and 9.2 ± 1.7 mm2 in patients for whom ASED treatment was ineffective. The mean duration of PED before the introduction of ASEDs was 19.0 ± 6.0 days.
About 30 (88.2%) eyes healed at a mean time of 9.4 ± 4.7 days, and four eyes (11.8%) were not healed at 4 weeks. The mean duration of ASEDs usage was 8.5 ± 6.3 months, and mean follow-up time was 22.8 ± 12.2 months. Treatment with ASEDs was effective in 25 (73.5%) eyes and partially effective in 5 (14.7%) eyes (neurotrophic keratopathy (n = 3), Steven-Johnson syndrome (n = 1), and dry eye disease (DED)/Sjögren’s Syndrome (n = 1)). Signs of worsening, including enlargement of the epithelial defect and stromal thinning, were observed in 4 (11.8%) eyes (Steven-Johnson syndrome (n = 1), DED/Sjögren’s Syndrome (n = 1), neurotrophic keratopathy (n = 1), and penetrating keratoplasty (PK) with large-diameter grafts due to post-infectious scar (n = 1)). Although the frequency of ASED application was increased to hourly, there was no improvement in the lesions. Amniotic membrane transplantation and lateral tarsorrhaphy were performed in three eyes to stabilize the ocular surface. In addition, one eye required PK.
After cessation of ASEDs, recurrence of PED was observed at the fourth day in an eye with neurotrophic keratopathy, at the seventh and ninth days in two eyes with postherpetic keratitis, and healing occurred after the second course of ASEDs treatment at the third day in the eye with neurotrophic keratopathy and at the third and fourth days in the eyes with postherpetic keratitis. The characteristics of the patients are summarized in Table 2.
The characteristics of the patients and treatment results.
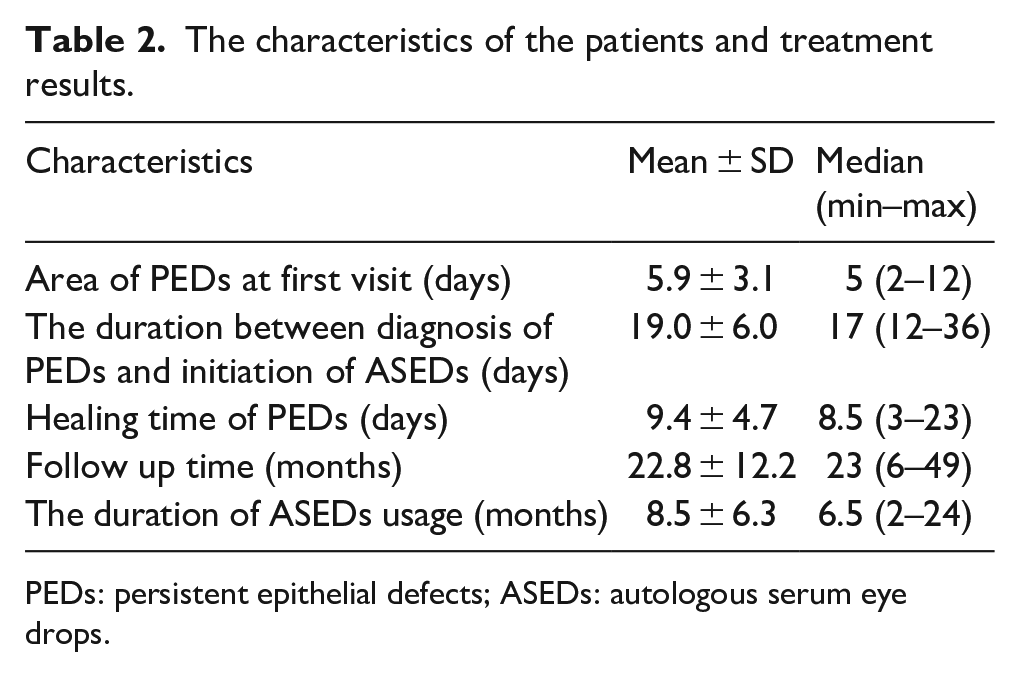
PEDs: persistent epithelial defects; ASEDs: autologous serum eye drops.
The frequency of dosing varied among eyes, although 44.1% were prescribed ASEDs for use in 2-h intervals while awake. The ASED dosages and treatment results are summarized in Table 3.
The ASEDs usage dose and treatment results.
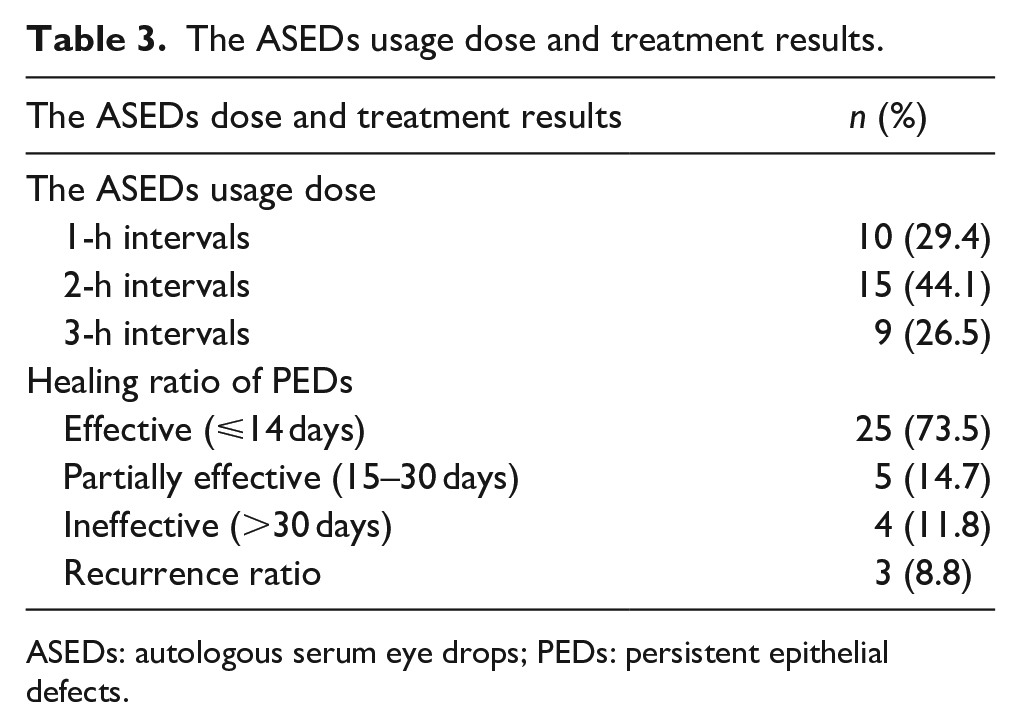
ASEDs: autologous serum eye drops; PEDs: persistent epithelial defects.
The mean BCVA was 1.8 ± 1.0 logMAR at the time of PEDs diagnosis and 1.5 ± 0.9 logMAR at the last visit (p = 0.6).
Healing time of PEDs correlated with the PED area (r = 0.800, p < 0.001), but it was not correlated with the time between PED diagnosis and initiation of ASED treatment (r = 0.195, p = 0.268).
None of the patients had a secondary infection or inflammatory reaction related to ASEDs.
Discussion
Persistent epithelial defects are complex and multifactorial in terms of etiology and symptoms, and they are difficult to treat. Successful results have been reported regarding the safety and efficacy of ASEDs in patients for whom conventional treatments fail.18–22,24,25,27
The successful epithelization ratio in patients using ASEDs varies between 43% and 91.5%, depending on clinical protocols, predisposing factors, and the severity of the disease.1,4,27–30 In our study, PEDs that emerged due to various etiologies and did not respond to conventional treatment within 2 weeks were treated with 20% ASEDs. Complete epithelialization was achieved in 88.2% of the eyes at a mean of 9.4 days. This ratio is similar to study results in the literature, including studies that used a higher serum concentration (50%–100%).5,27–30
In similar studies the average healing time for PEDs was 19.3–204 days, and there was a correlation between PED duration and healing time.1,5,19–25,31,32 In our study, there was no correlation between PED duration and healing time. This may be due to the shorter window between PED diagnosis and initiation of ASEDs, compared to the literature.
In our study, the PED area was larger in eyes with ineffective epithelization than in all eyes, and in a departure from the literature, the PEDs area and epithelial closure duration were correlated.1,33,34
In addition, in the four eyes in which epithelization did not occur at the end of 4 weeks, severe predisposing etiologies were present. Additional surgical interventions such as amniotic membrane transplantation, lateral tarsorrhaphy, and tectonic keratoplasty were required when epithelial healing could not be achieved. These findings demonstrated that the area of the epithelial defect, widespread damage to the conjunctiva and limbal stem cells, and severe tear deficiency may be the most important factors informing successful treatment and healing of PEDs.
In 3 (8.8%) eyes, PEDs recurred when the ASEDs were discontinued and after complete re-epithelization. This indicates that, in some eyes, the use of ASEDs for an extended period may be required to prevent recurrent corneal PEDs after the first epithelization. Therefore, long-term follow-up of these patients is important. In our study, the duration of ASED treatments and the follow-up periods for patients were quite long compared to the literature.27,35,36
In the literature, different methods in various steps have been described for preparing ASEDs including serum amount, clotting time, centrifugation time and force, dilution rate, and diluents (Table 4).1,6,19,21,31,37,38
Variations of ASEDs preparation.
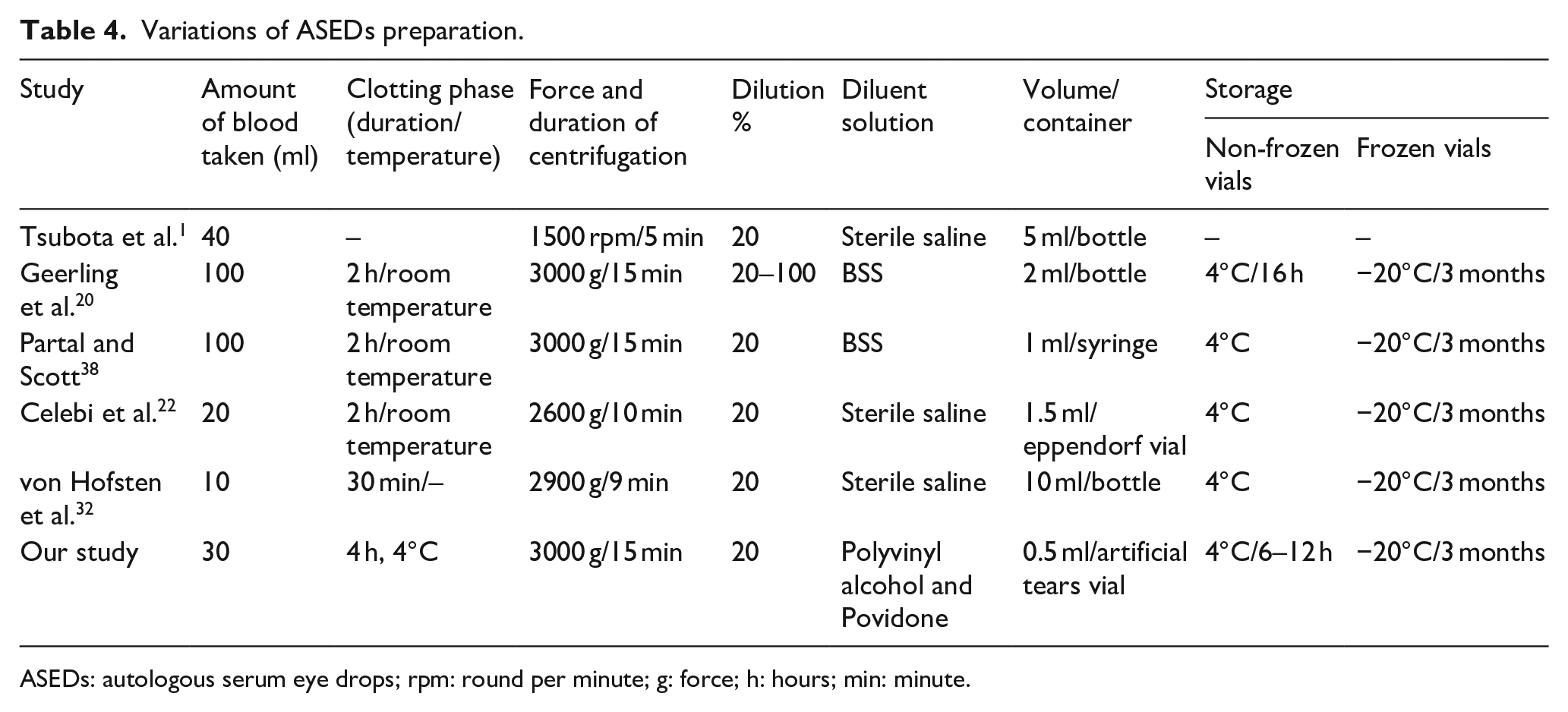
ASEDs: autologous serum eye drops; rpm: round per minute; g: force; h: hours; min: minute.
Serum can be stored for 7 days at 4°C and for 3–6 months at −20°C without decreasing the concentrations of vitamins and growth factors, while concentrations of these substances are more variable at room temperature. It has been reported that when the waiting time before centrifugation is long, the growth factor concentration becomes higher.1,39–41 Although different clotting times have been reported in the literature, in clinical practice the most common duration is the 2-h waiting period.19,31,37 In our study, the serum was kept at 4°C for 4 h before centrifugation, as this provides the advantage of longer coagulation time, and the drops were delivered to the patient on the same day. As the presence of growth factors and vitamins in ASEDs prepared by various methods were studied and reported in previous publications, these concentrations were not tested in our study.
Different centrifugation times and forces result in different concentrations of growth factors. Tsubota et al.1,18 have suggested a 1500 rpm centrifugation for 5 min. However, in vitro studies have demonstrated that higher force and longer centrifugation times provide better separation of serum than blood clot, without inducing hemolysis, and more balanced growth factor levels.1,8–11,13,20 These in vitro studies showed a five-fold decrease in TGF-β concentration and a two-fold increase in EGF concentration when compared to previous studies.1,20
Liu et al. 21 also reported that platelet membranes, which induce apoptosis, remain in the supernatant serum at low rpms or short centrifugation times. Based on these results from the literature, we prefer a 3000g centrifugation force for 15 min.
Although studies have reported that the efficacy of ASEDs increases with high concentrations,5,30,36,37 many studies have reported that dilution of serum at a 20% concentration provides a sufficient effect.1,18,19,22,41 High concentrations of ASEDs can cause immune reactions in the form of immunoglobulin deposition and limbitis and ocular irritation associated with extra viscosity.5,19,32
In addition, repeated, large-volume phlebotomies may cause anemia. When the serum is diluted at a 20% concentration, more vials can be obtained using a smaller amount of blood. This may reduce repeated phlebotomies, dilute TGF-β1, and prevent complications due to increased viscosity or immune-mediated reactions.
In our study, ASEDs were prepared in 0.5 ml tubes by diluting the serum at a 20% concentration. Thus, taking 30 ml of blood from the patients at 3-month intervals was sufficient, and no patient had serious ocular discomfort.
Although the serum can be bacteriostatic due to antibacterial agents such as IgG, lysozyme, and complement factors, it is also a suitable growth medium for microorganisms due to its high protein content. For this reason, ASEDs can be contaminated when kept out of the refrigerator or after contact of the tip with the hands or eyelids.37,42,43
Dilution of the serum with chloramphenicol, ceftazidime, and gentamicin or preparation with sterilizing filters has been shown to reduce bacterial contamination.5,37,44,45 However, antibiotics and preservatives added to ASEDs may cause allergic or toxic reactions, and the procurement and dosing of these are difficult.19–43
In order to reduce the risk of contamination in our study, ASEDs were prepared using sterilizing filters in the operation room and by adding 0.1 ml of serum to 0.4 ml preservative-free artificial tear vials. No preservatives or antibiotics were added. After opening a vial, it was used for a maximum period of 12 h. As a result of these precautions, toxic and immunological reactions or secondary infections due to ASEDs were not observed in our patients. The preparation of ASEDs without preservatives or antibiotics reduced the cost.
The volume of ASEDs prepared in the literature was between 1.5 and 10 ml at 20%–100% concentrations, and it was recommended that ASEDs be discarded after daily use.6,19–22,31,37,38 However, this requires repeated phlebotomies and increases the cost of serum preparation and the work-load of healthcare personnel.
Other blood-derived eye drops such as allogenic serum, umbilical cord serum and platelet rich plasma can be used to treat PEDs when conventional treatments fail.4,8,46–48 However the emergence of legal problems in the preparation of umbilical cord serum and allogenic serum eye drops, and the need for special equipment in the preparation of PRP eye drops are the main disadvantages that limit their use.8,27 Since autologous serum drops do not have these disadvantages, we prefer to use ASEDs in our clinic.
In eight patients with heterogenous diagnoses (neurotrophic keratopathy (two patients), rosacea keratitis, vernal keratoconjunctivitis, and keratoconus, dry eye disease/Sjögren’s syndrome, post-herpetic keratitis, Steven-Johnson syndrome, limbal stem cell deficiency) both eyes were included. The inclusion of both eyes of a single patient may lead to statistical bias. However, despite their common systemic backgrounds, these paired eyes had different final outcomes, which were classified as effective, partially effective, and ineffective.
In our study, the artificial tears vials contained 0.5 ml of 20% serum. This enabled the drops to be prepared with fewer blood draws and less blood. Additionally, this prevents healthcare personnel from repeating the same tasks each day, reduces cost, minimizes the risk of toxic and immune reactions as well as contamination, and the preparation time is short. Due to these advantages, preparation can be made available to more patients, and patient compliance can be sustained.
In conclusion, a single-dose vial containing ASEDs prepared by diluting serum with non-preservative artificial tears seems to be practical, effective, and safe in PEDs that develop due to various predisposing factors.
Footnotes
Author’s note
TC. Ankara Kecioren Training & Research Hospital, Clinical Research Ethics Committee, Project Number: 2012-KAEK-15/2162.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.