
Abstract
Purpose
The aim of this article is to describe an innovative and minimally invasive surgical technique for posterior vitrectomy combined with secondary intraocular lens implantation, using a sutureless scleral fixation Carlevale intraocular lens (I71 FIL SSF Carlevale lens. Soleko IOL Division, Italy).
Methods
The technique was conducted with only three transconjunctival sclerotomies and a corneal tunnel to perform intraocular lens explantation, posterior vitrectomy and Carlevale intraocular lens implantation. It is easier, quicker, and less invasive than the traditional technique with conjunctival peritomy, two scleral flaps and five sclerotomies.
Results
Surgery was performed uneventfully on three eyes of three patients. Two of them presented a luxation of the intraocular lens into the vitreous chamber, while one patient presented an intraocular lens subluxation. No complications were observed after a 5 to 8 months of follow-up. The intraocular lenses were well positioned, no conjunctival erosion was noted, and the intraocular pressure remained normal at all stages.
Conclusions
This is the first report of a combined procedure of IOL explantation, posterior vitrectomy and secondary IOL implantation using only three transconjunctival sclerotomies. This appears to be less invasive and it causes less discomfort to the patient. We suggest considering this technique in all those cases requiring a combined procedure in absence of a proper capsular support.
Keywords
Introduction
Secondary lens implantation is the technique of choice in case of secondary aphakia or intraocular lens (IOL) complications, such as IOL opacification and IOL dislocation. 1 One of the most popular surgical approaches is scleral fixation of the IOL, which can be performed using different techniques, either sutureless or requiring suture fixation. 2 Sutureless scleral fixation presents several advantages, since it reduces suture-related risks, such as suture degradation, endophthalmitis, and chronic inflammation. The Carlevale IOL (I71 FIL SSF Carlevale lens. Soleko IOL Division, Italy) is a hydrophilic foldable IOL recently designed for posterior chamber sutureless scleral fixation. At the extremity of the two haptics flexible plugs are positioned, which need to be anchored to the sclera. They are designed to prevent the backward movement of the haptic into the eye after the scleral fixation. 3 The traditional surgical technique for IOL implantation requires the opening of the conjunctiva, the creation of two scleral flaps and two sclerotomies 180 degrees apart. The lens is injected into the anterior chamber through a corneal tunnel, and the two plugs are externalized through the sclerotomies under the scleral flaps using two crocodile tip forceps, with the so-called ‘handshake technique’.4,5 When posterior vitrectomy is also required—that is, to remove an IOL dislocated into the vitreous chamber and/or the pathological and prolapsed vitreous—the standard technique involves the construction of three additional sclerotomies, to perform a three-port pars plana vitrectomy.4–6 From 2018 to April 2021, 24 Carlevale IOLs have been implanted in our center, mainly due to aphakia and IOL subluxation.
In this paper, we applied an innovative and less invasive surgical approach in three eyes requiring IOL explantation, vitrectomy, and secondary IOL implantation. This technique can be very useful for all those cases requiring both vitrectomy and secondary IOL implantation in the absence of a capsular support.
Methods
All the patients were operated by the same surgeon (PL) under peribulbar anesthesia. Supplemental Video 1 includes all the surgical steps that are described in detail in this report. After displacing the conjunctiva, two 25-gauge cannulas are positioned inferotemporally and superonasally 180° apart and 1.5 mm posterior to the limbus into the ciliary sulcus. A 25-gauge cannula is positioned superotemporally 3.5 mm posterior to the limbus into the pars plana, with an angled insertion (Figure 1). A corneal tunnel is done superonasally where the cannula has been previously positioned and a limbal corneal paracentesis is done inferotemporally 180° apart. Additional corneal paracentesis may be done according to the surgeon's needs during the operation. Forceps and hooks are inserted through the tunnel and the paracentesis, to grasp the luxated IOL and move it into the anterior chamber. When possible, scissors are used to section the IOL in two parts after ocular viscoelastic is injected into the anterior chamber. Alternatively, the IOL can be folded into the anterior chamber and subsequently explanted. Rigid IOLs need larger corneal or sclero-corneal incisions for explantation. Using forceps, the IOL fragments and the capsular bag are removed through the corneal tunnel. A bimanual technique is used for several of the previously described surgical steps. Balanced saline solution is infused through the inferotemporal cannula, while the instruments—that is, the vitrector and the light probe—are inserted through the other two cannulas (Figure 1). Core vitrectomy is performed. Ocular viscoelastic is injected into the anterior chamber. Infusion can also be moved from the inferotemporal to the superotemporal cannula, to maintain the intraocular pressure stable during secondary IOL implantation. A Carlevale IOL (Figure 2) is injected through the corneal tunnel. At the same time, a crocodile forceps is inserted through the inferotemporal cannula to grasp the plug opposite to the injection site (Figure 3). Once grasped, the plug is externalized through the sclerotomy, while removing the cannula concurrently (Figure 4). A crocodile forceps is then inserted through the inferotemporal corneal paracentesis to hold the superior haptic of the IOL to make the subsequent steps easier. A second crocodile forceps is inserted through the superonasal cannula and the second plug is grasped, then externalized through the sclerotomy while removing the cannula (Figure 5). Prior to their usage, both the forceps are slightly bent manually, to perform the previously described steps more easily. Viscoelastic is injected into the anterior chamber throughout the whole procedure, to work safely, to maintain an adequate depth of the anterior chamber, and to protect the endothelium. The correct positioning of the IOL is then verified. Further check is done to ascertain that the two plugs are correctly positioned through the sclerotomies and covered by the conjunctiva. Viscolelastic is aspirated and the corneal tunnel is sutured with 10.0 Vicryl. All cannulas are removed. No conjunctival sutures are needed.
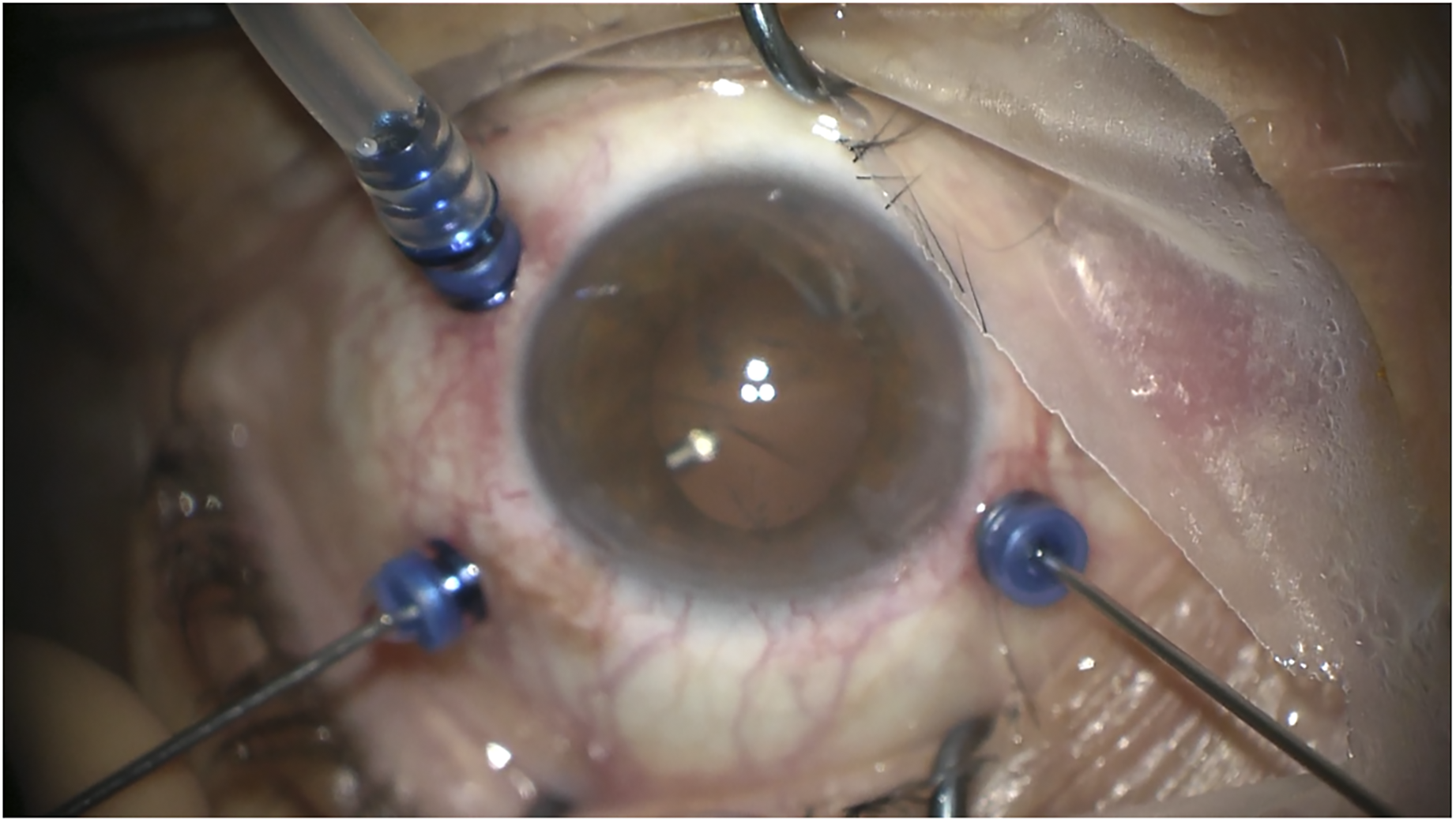
All the pictures represent a left eye viewed from above (surgeon position). This figure depicts the position of the cannulas. Note that the cannulas at 4 o’clock and 10 o’clock are placed 1.5 mm posteriorly to the limbus, while the 2 o’clock cannula is positioned 3.5 mm posteriorly to the limbus. Prior to core vitrectomy, infusion is started through the 4 o’clock cannula, while the light probe is inserted via the 10 o’clock cannula and the vitrector enters through the 2 o’clock one.
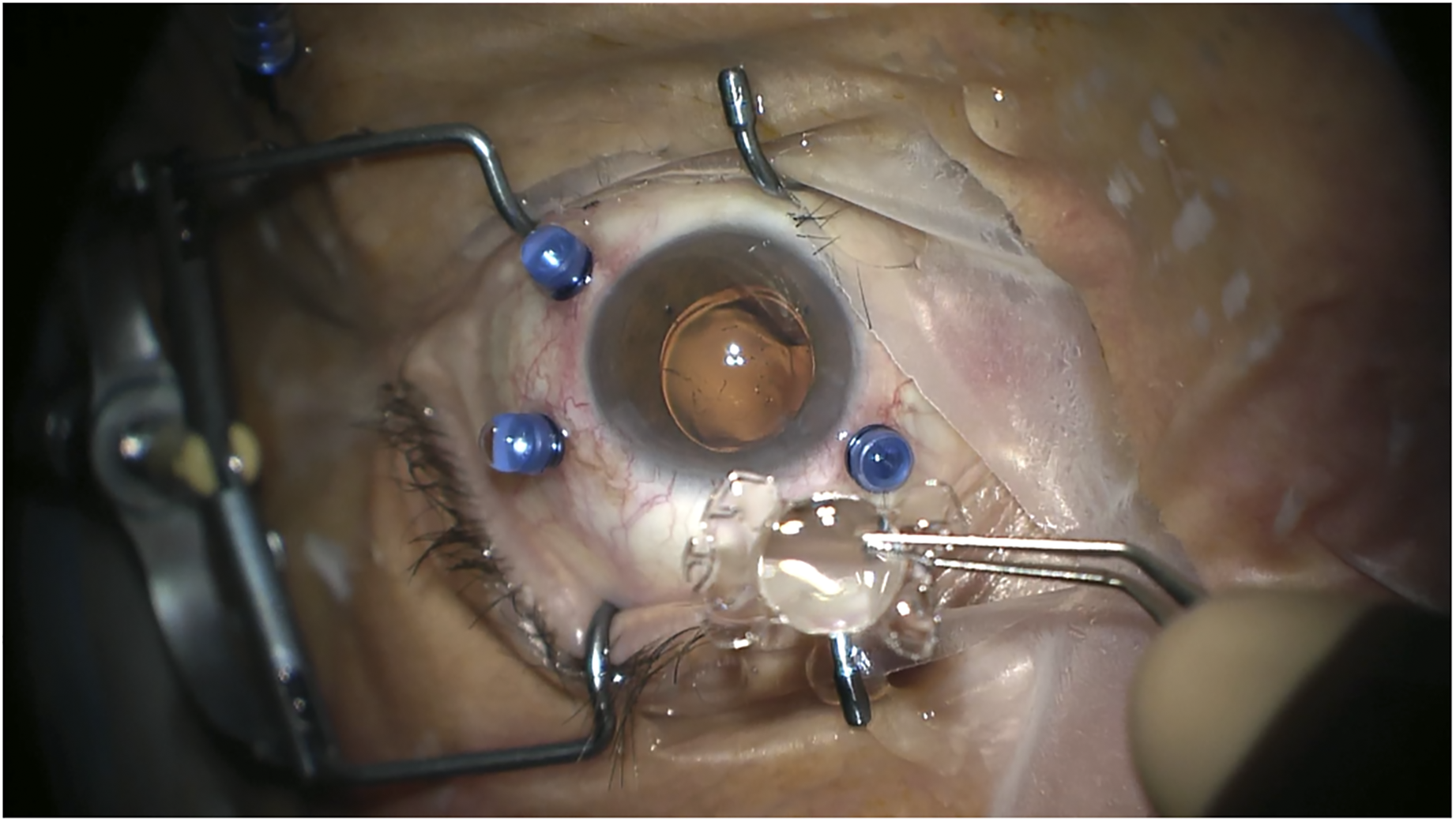
The Carlevale intraocular lens (IOL) prior to implantation.
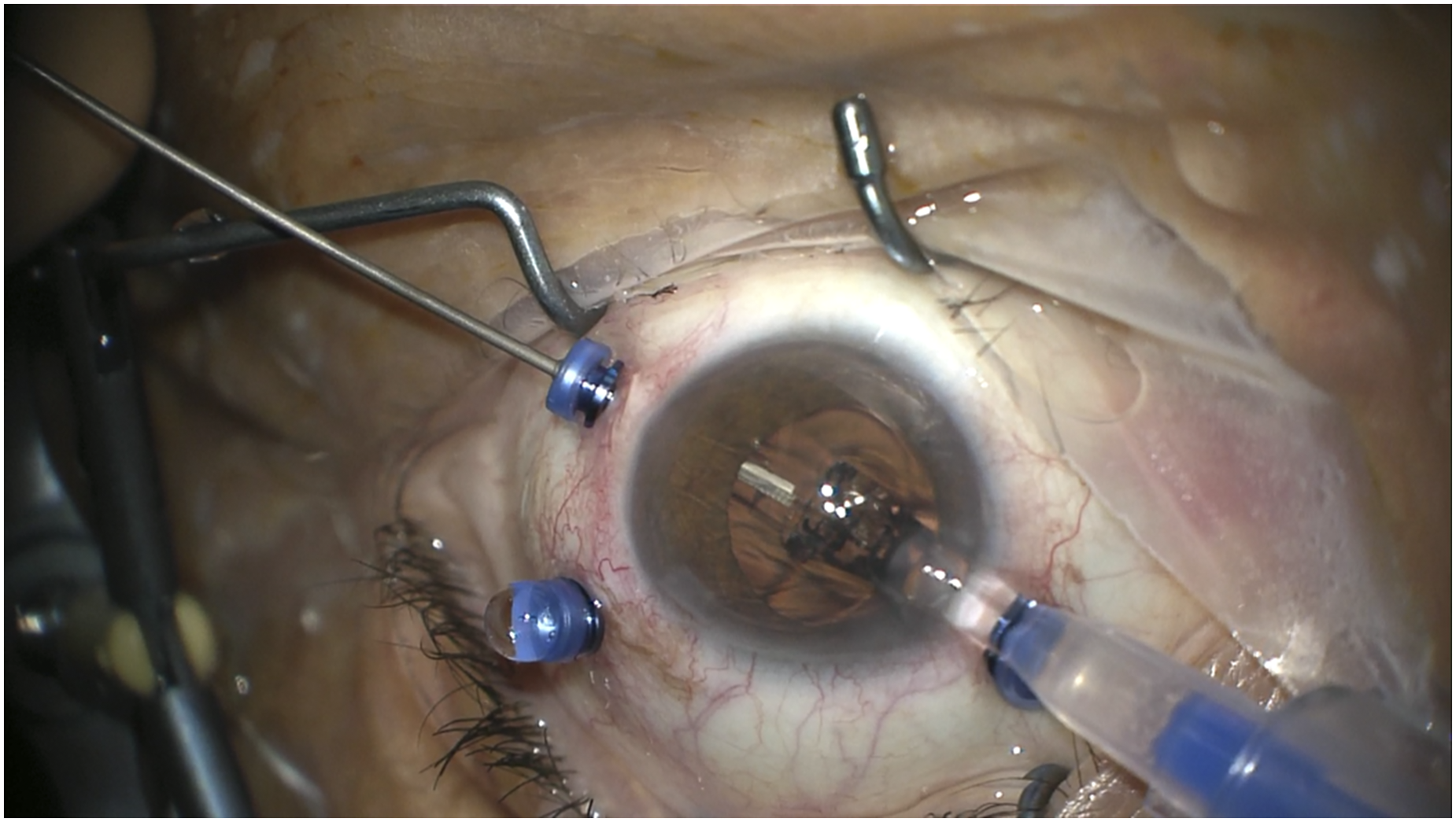
The Carlevale intraocular lens (IOL) is injected through the 10 o’clock corneal tunnel, while a crocodile forceps is inserted through the 4 o’ clock cannula to grasp the IOL plug.
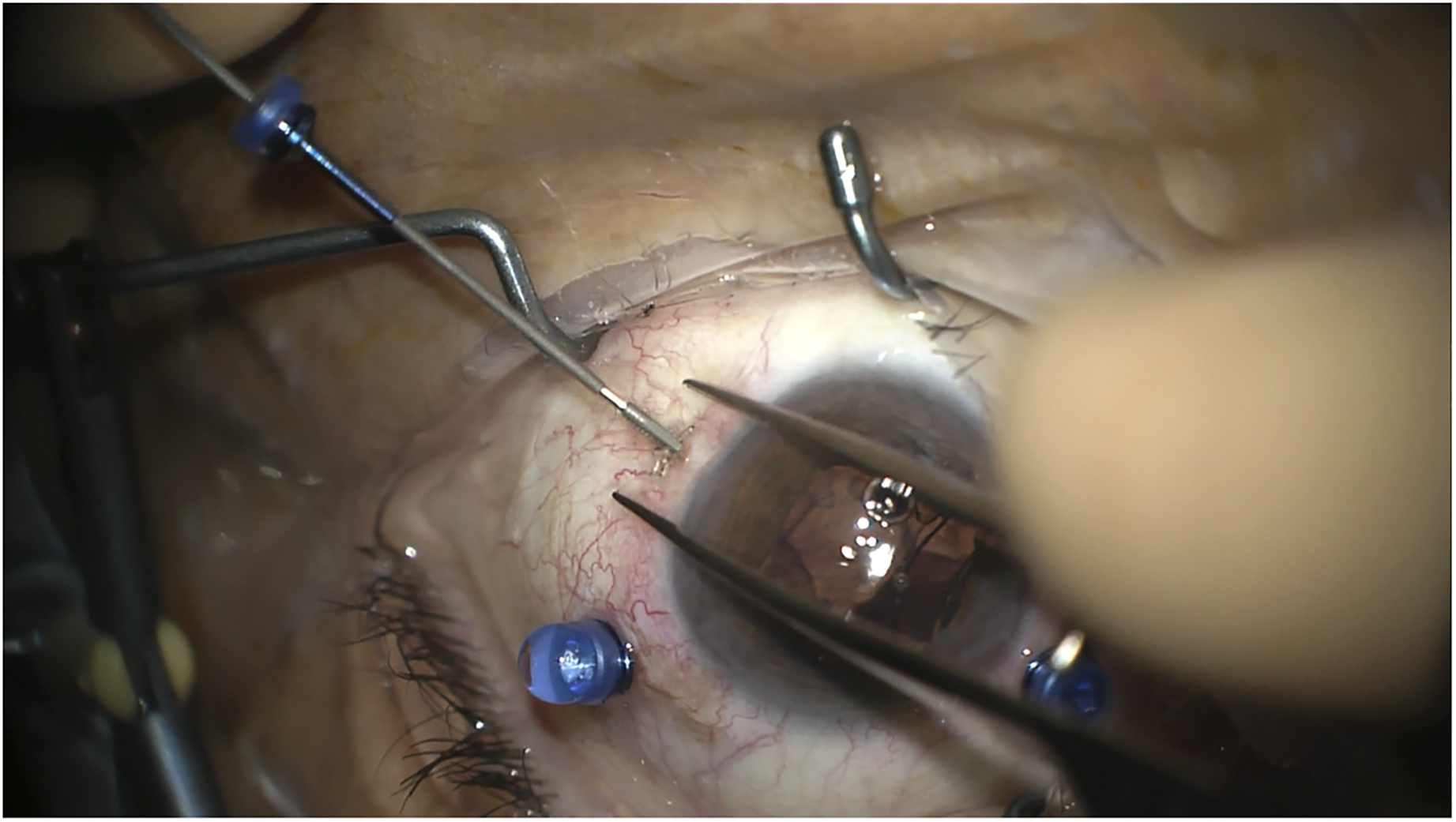
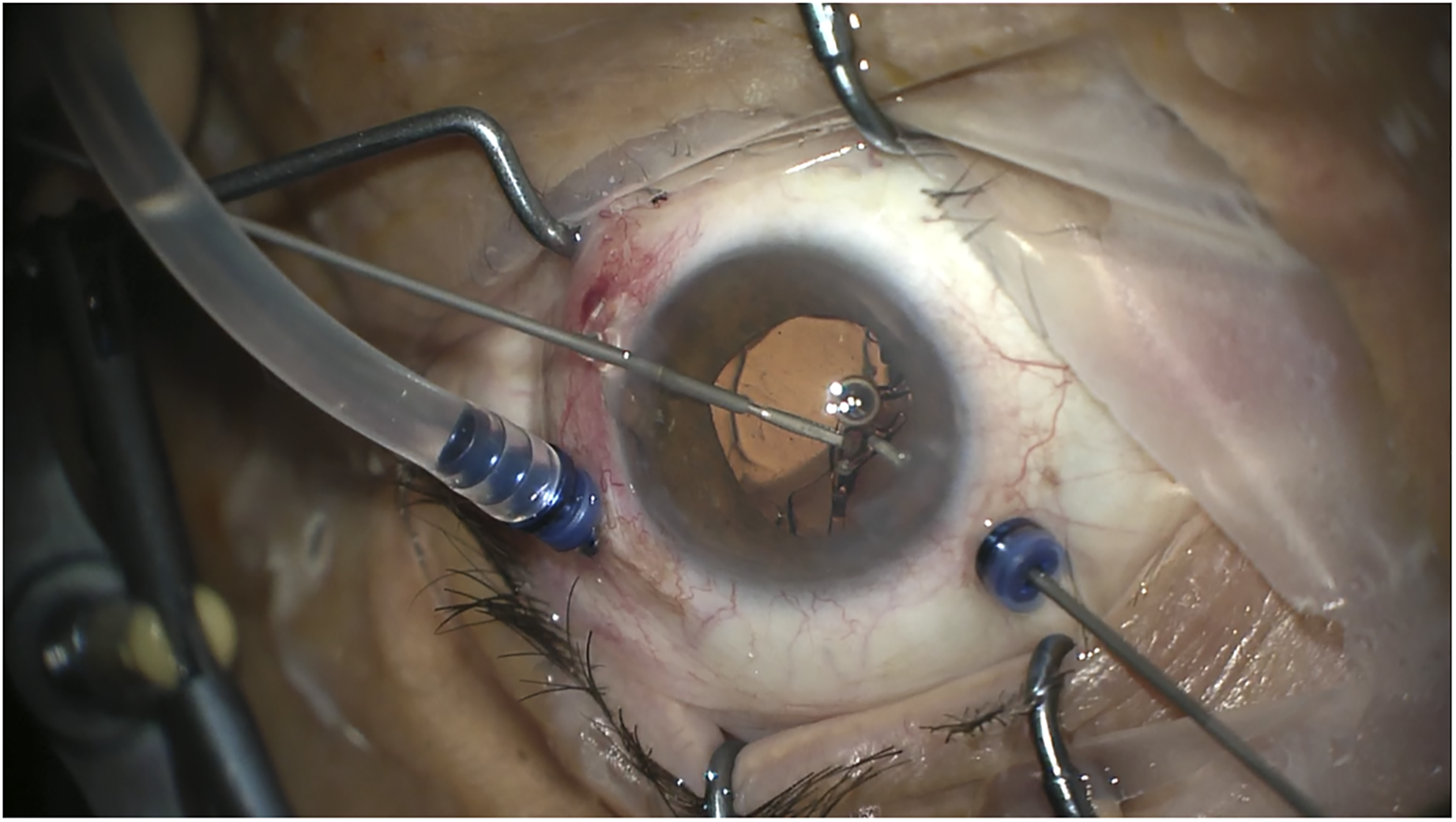
The first intraocular lens (IOL) plug is externalized by the forceps. At the same time, the cannula is removed.
The second intraocular lens (IOL) plug is grasped using two crocodile grasping forceps.
Results
The described technique was performed on three eyes of three patients with excellent results.
The first patient was a 72-year-old man. Cataract surgery was performed in his left eye 18 years earlier, and it was complicated by posterior capsule rupture. He presented to our clinic with IOL subluxation and cortical remnants in the vitreous chamber in the left eye. His visual acuity (VA) improved from 20/40 preoperatively to 20/20 postoperatively, and it remained stable after an 8-month follow-up.
The second patient was a 77-year-old woman, suffering from severe myopia and myopic choroidal neovascularization in both eyes. After receiving a single session of photodynamic therapy, choroidal neovascularization stabilized and she underwent cataract surgery in the left eye. A total of 11 years later, she presented a complete luxation of the complex IOL, capsular bag, and capsular tension ring into the vitreous chamber in the left eye. Before surgery, she was able to count fingers at 30 cm, while after the operation her VA improved to 20/400. This result was maintained after an 8-month follow up.
The last patient was an 85-year old man, who presented to our clinic with an IOL luxation into the vitreous chamber in the right eye. Four years earlier he had already undergone explantation of a subluxated IOL and implantation of iris-fixated IOL in the right eye. He also suffered from macular dystrophy in the right eye. While before the operation his VA was 20/50, postoperatively he improved to 20/32, with a 5-month follow up.
Also, as in all the cases the IOLs were well centered, no tilting was present, the plugs were well positioned beneath the conjunctiva without any signs of erosion; we considered the anatomical results excellent. No postoperative complications were registered during the follow up; in particular, intraocular pressure remained within a normal range at all times.
Conclusions
At present, the Carlevale lens represents a very useful tool for several cases requiring secondary IOL implantation, even the most complex ones. Its unique design allows for its stable scleral fixation without the need for sutures. The originally described implantation technique requires the sculpting of two scleral lamellas 1.5 mm posterior to the limbus, usually at 0° and 180°, which cover the two T-shaped harpoons of the IOL. 5 However, it has already been described that the two plugs can be positioned beneath the conjunctiva without complications.3,7
When performing secondary IOL implantation, combined vitrectomy may be needed, for example to remove a subluxated IOL or an IOL dislocated into the vitreous chamber. The traditional setting requires the positioning of three trocars 3.5 mm posterior to the limbus, thus performing a three-port pars plana vitrectomy. If needed, the luxated IOL and/or capsular bag can be removed through a corneal incision. Thereafter, the Carlevale lens can be injected and fixated through the sclera, therefore requiring two additional sclerotomies for haptics fixation. This maneuver increases the invasivity of the procedure. However, the technique that we describe implies the use of three sclerotomies for both vitrectomy and scleral fixation of the IOL. Two sclerotomies are placed into the ciliary sulcus and one into the pars plana. This presents several advantages. First of all, invasivity is reduced. By using the same cannulas for both vitrectomy and IOL fixation the number of incisions needed are reduced, therefore decreasing postoperative patient discomfort. Performing three-port vitrectomy with this setting does not impair either the effectiveness or the safety of the procedure. Moreover, this maneuver also decreases operating times. It is also much easier to position two cannulas instead of sculpting two scleral flaps. The externalization of the two harpoons while simultaneously removing the cannulas using crocodile grasping forceps is a maneuver which can be easily performed by surgeons experienced with this type of procedures. The presence of the cannulas is helpful when inserting the instruments thus avoiding unnecessary stress to the surrounding tissues.
In conclusion, this technique appears to be very promising and we advise surgeons to consider using it when performing combined vitrectomy and IOL implantation in all those cases lacking a proper capsular support. A larger case series will be useful to confirm the lack of postoperative complications and the excellent anatomical results.
Supplemental Material
sj-docx-1-ejo-10.1177_11206721211049102 - Supplemental material for Combined transconjunctival sutureless three-port vitrectomy and scleral fixation of intraocular lens
Supplemental material, sj-docx-1-ejo-10.1177_11206721211049102 for Combined transconjunctival sutureless three-port vitrectomy and scleral fixation of intraocular lens by Carla Danese and Paolo Lanzetta in European Journal of Ophthalmology
Footnotes
Declaration of conflicting interests
Carla Danese declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Paolo Lanzetta reports personal fees from AERIE, personal fees from APELLIS, personal fees from BAYER, personal fees from BIOGEN, personal fees from CENTERVUE, personal fees from NOVARTIS, personal fees from ROCHE, outside the submitted work.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.