
Abstract
Purpose
The intravitreal dexamethasone implant (DEX-I) is an alternative to anti-VEGF for the first-line treatment of diabetic macular oedema (DME). However, several questions remain regarding its routine use and its place in certain situations not always specified in current recommendations. A national consensus approach was, therefore, initiated by French retinal experts.
Methods
An iterative Delphi consensus approach was used. A steering committee (SC) of seven experts analysed data from the literature to formulate statements divided into five key areas of treatment. These statements were submitted to the independent and anonymous electronic vote of 87 French retina experts among whom 39 expressed their opinion and therefore constituted the voting panel.
Results
After two rounds of voting, 22 and 7 of 38 statements received a strong consensus and a good consensus, respectively. The consensus level was higher for statements regarding first-line indications and safety of DEX-I compared to those regarding efficacy assessment, reprocessing time or pathophysiological biomarkers. The panellists recommended the preferential use of DEX-I for patients with limited availability for multiple injections, those who needed to undergo cataract surgery or who had a recent cardiovascular history, and as a therapeutic alternative to anti-VEGF in patients with a history of vitrectomy, retinal serous detachment, hyper-reflective points or dry exudates in optical coherence tomography (OCT). However, some statements proposed by SC experts were not validated.
Conclusion
This study provides some key recommendations to clinicians treating diabetic macular oedema, which may be useful when using intravitreal dexamethasone implants in daily practice.
Keywords
Introduction
Diabetic macular oedema (DME) is the most common manifestation of diabetic retinopathy (DR) and the main cause of blindness in diabetic patients.1–3 Up to 50% of eyes with DME involving the centre of the macula can lose multiple lines of visual acuity (VA) over a two-year period. 4 The prevalence of DME increases with age and DR stage 5 approaching 30% in patients with diabetes for 20 years or more. 6
The management of DME has changed profoundly in recent years. Laser photocoagulation previously considered the standard treatment has been gradually replaced by pharmacological treatments, such as anti-VEGFs and corticosteroids, which are now used as first-line treatments. 7 Two anti-VEGFs (ranibizumab or Lucentis®, Novartis, and aflibercept or Eylea®, Bayer) and a biodegradable dexamethasone implant (Ozurdex®, Allergan-Abbvie) received their marketing authorisation in Europe for first line DME indication. Their results, based on large-scale pivotal studies but conducted on patient populations that were both compliant and selected on strict inclusion and exclusion criteria, cannot be fully extrapolated to daily clinical practice. 8 Thus, “real-life” studies on more general populations of DME patients provide complementary results. 8
The widespread use of anti-VEGFs as first-line treatment has shown that a significant number of patients - 25 to 40% according to literature - did not achieve an optimal anatomical or functional response.9–12 In addition, the presence of certain ocular or systemic comorbidities, the frequency of injections and the cost of these treatments may limit their use. 13
The intravitreal dexamethasone implant (DEX-I) improves and then stabilises the visual acuity (VA) of DME patients; it has a good safety profile and an acceptable economic weight. 14 It therefore represents an alternative first-line treatment for DME. However, several questions remain concerning its routine use and its place in certain specific situations which are not always specified in current recommendations. In addition, France being one of the countries in the world with the highest level of DEX-I experience - around 15% worldwide patient exposure - it seemed relevant to us to develop a consensus based on this strong national experience.
A national consensus approach was, therefore, initiated by French retinal experts with the aim of establishing recommendations on how to use DEX-I in the treatment of DME based both on data in the literature and the experience of French retinal experts and a panel of French ophthalmologists. A modified Delphi method was chosen to establish these clinical practice recommendations.
Materials & methods
The Delphi method is an iterative consensus approach based on information collected from a panel of participants with expertise in the subject under consideration.15–21 This method has been widely used in many therapeutic areas and several times in ophthalmology22–32 and in DME in particular.12,33–37 In this structured approach, the interviewed experts provided their opinion individually and anonymously, and expressed their degree of agreement on different statements with the aim of obtaining a consensus on a specific and well-defined subject.
According to French and international methodological indications,16–19,38,39 our study was structured as a modified Delphi consensus conducted with French experts from April to September 2020. The expert opinion gathering took place in two voting rounds based on a questionnaire drawn up by a steering committee (SC).
As recommended by the French National Authority for Health and certain authors, the participants indicated their level of agreement using a nine-point Likert scale ranging from 1 (strongly disagree) to 9 (strongly agree).38–40 The percentage of scores and median were calculated for each statement separately in each voting round.
After analysing the literature, a strong consensus was reached for a statement when more than 75% of the scores were ≥7 and the median score was ≥8. When only one of these two parameters was satisfied, the statement was considered to have obtained a good consensus.16,17,41
Steering committee and questionnaire
The SC was composed of six ophthalmology experts brought together and moderated by the first author of this article. A first virtual meeting took place. After discussing the elements of an analysis of the literature on the subject, the SC members formulated 40 statements divided into five key areas of DME treatment by DEX-I, namely pathophysiology, indications for the dexamethasone implant as first-line treatment, time to retreatment, efficacy criteria and safety. International recommendations, elements reported in the literature and the clinical experience of the SC members served as the basis for formulating statements for the first round of voting.
Panel of voting experts
To obtain strong expertise and wide national representation, the experts from the voting panel were selected based on several criteria: experienced ophthalmologists (min. 30 y.o.), acquired knowledge and expertise in the treatment of DME (min. 5 years of experience), speakers at national conferences (French Society of Ophthalomology congresses and/or Lyon Eye Retina congresses) and/or involvement in DME projects (clinical researcher and/or trainer). They covered the whole French territory and represented the various modes of practice: hospital, private practice, mixed. The quantitative objective of this study was to bring together 25 to 30 voting experts. Estimating a participation rate of around 33%, the SC invited by email 87 ophthalmologists recognised as retina specialists to participate in the Delphi. The participants remained anonymous throughout the process and had no interaction with the SC whose members did not take part in the vote, in accordance with the methodological recommendations in force. 38
Voting round 1
The panel of 87 experts was invited to participate by email containing a link to an online survey platform. For this first round of voting, a free space for comments was made available to respondents for each statement, thus giving them the opportunity to develop or explain their choice. At the end of the first round, the scores and comments of the participants were summarised for each item.
A second virtual meeting was then held during which the SC members discussed the results:
12 statements with a strong consensus (i.e. + 75% of scores ≥7 AND median ≥8) were validated in extenso and directly included in the final recommendation. 1 statement with a good consensus (i.e. +75% of scores ≥7 OR median ≥8) was directly accepted 5 statements with a good consensus (i.e. + 75% of scores ≥7 OR median ≥8) were proposed for the second round of voting because the SC thought that a better wording inspired by the vote #1 comments would lead to a larger consensus (i.e. strong consensus instead of good consensus) 20 statements without consensus were reformulated or modified based on the comments of the voting experts and submitted to the second round of voting. Among them, 6 (30%) reached a strong consensus, 5 (25%) a good consensus and 9 (45%) did not improve. 2 statements were considered redundant and suppressed
Voting round 2
Using the same individual email system with personalised access to the internet response platform, the first-round panellists were invited to participate in the second round of voting; this time based on a questionnaire composed of 25 statements. Note that experts approached for the first round but who did not respond were not included in the second round. As several first-round respondents indicated in the comments space that they did not feel sufficiently expert to respond to certain statements, the option “I don't know” was added to the possible second-round responses. When selected, the response was extracted from the final statistical analysis.
As predetermined by the SC, the process was concluded after two rounds (Figure 1).
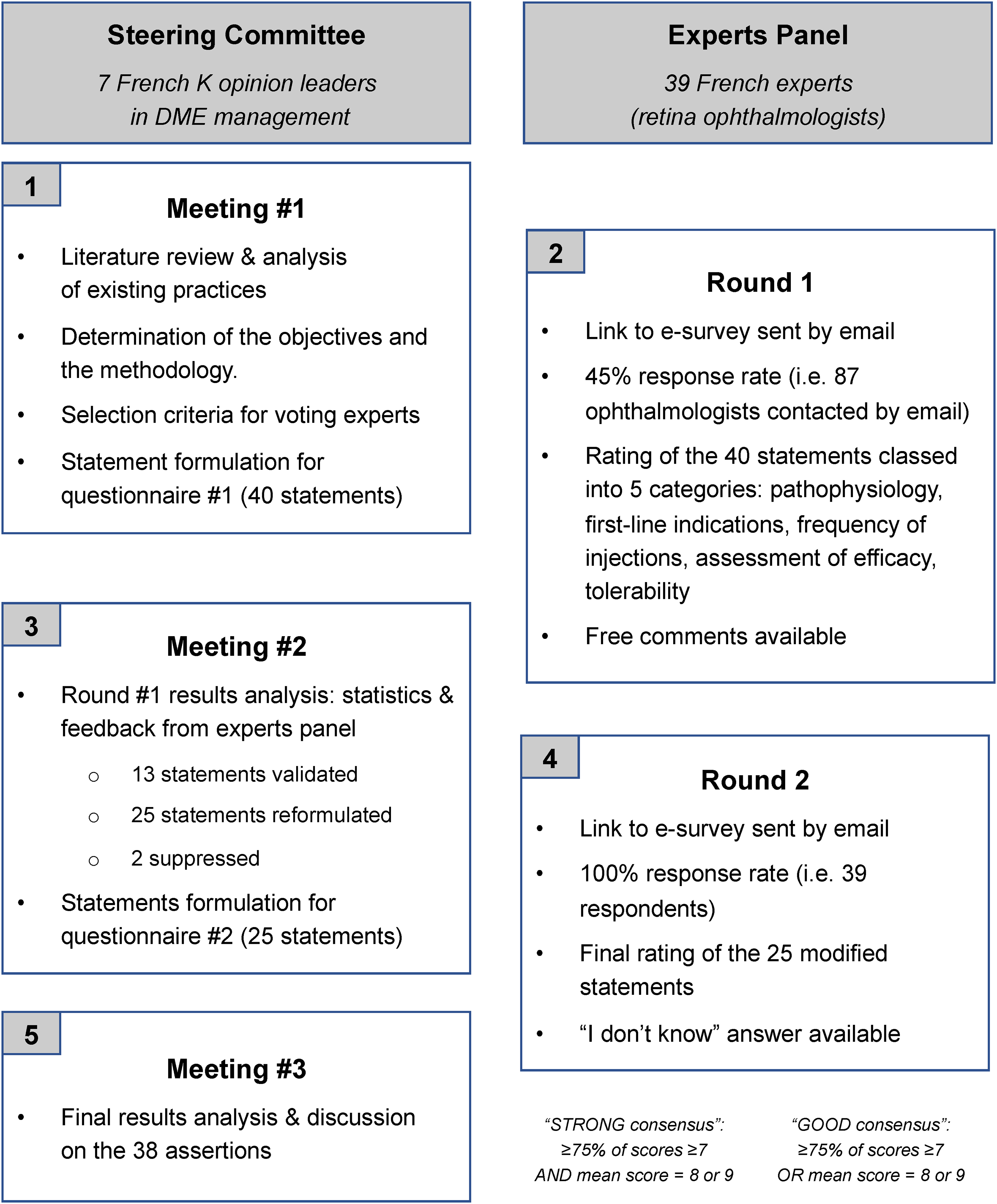
The modified Delphi method used in the study.
Results
Participation
Out of the 87 ophthalmologists invited to participate, 2 (2.3%) declined to take part and 46 others (52.9%) did not respond to either the invitation email or the reminder email. Overall, the number of experts included in the study was 39, i.e. a participation rate of 44.8%. There was no attrition between the two rounds: all the experts who participated in the first round responded to the second round.
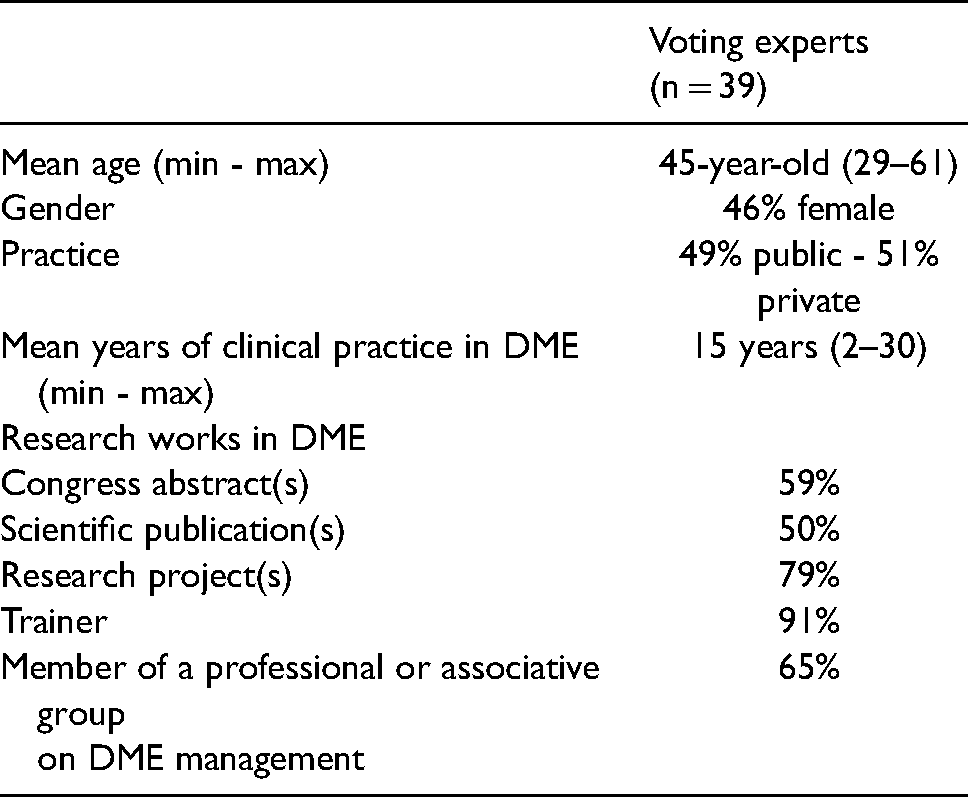
A summary of the characteristics of the voting experts is shown in Table 1. The average experience of DME varied from 2 to 30 years (mean 15 years). In addition to their clinical practice, a significant proportion of respondents conducted research in DME: writing scientific publications (50% of voters) and/or presentation at conferences (59%) and/or specific project (79%). Ninety-one percent were trainers and 65% were a member of a professional or associative group on DME management.
Characteristics of the Delphi panel.
Statements
After round 1, a strong consensus ( + 75% of votes ≥ 7 and median ≥ 8) and a good consensus ( + 75% of votes ≥ 7 or median ≥ 8) were reached for 12 and 6 statements, respectively. Following presentation of the results of the first round, discussion between the SC members led to the reformulation of 25 statements and the removal of 2 statements that had become irrelevant. After the second round of voting, among the remaining 38 statements, a strong consensus and a good consensus were obtained for 22 (57.9%) and 7 (18.4%) statements respectively, i.e. an overall consensus of 76.3%; and 9 statements (23.7%) achieved no consensus.
The distribution of votes, median and results is presented for each area in Tables 2 to 6.
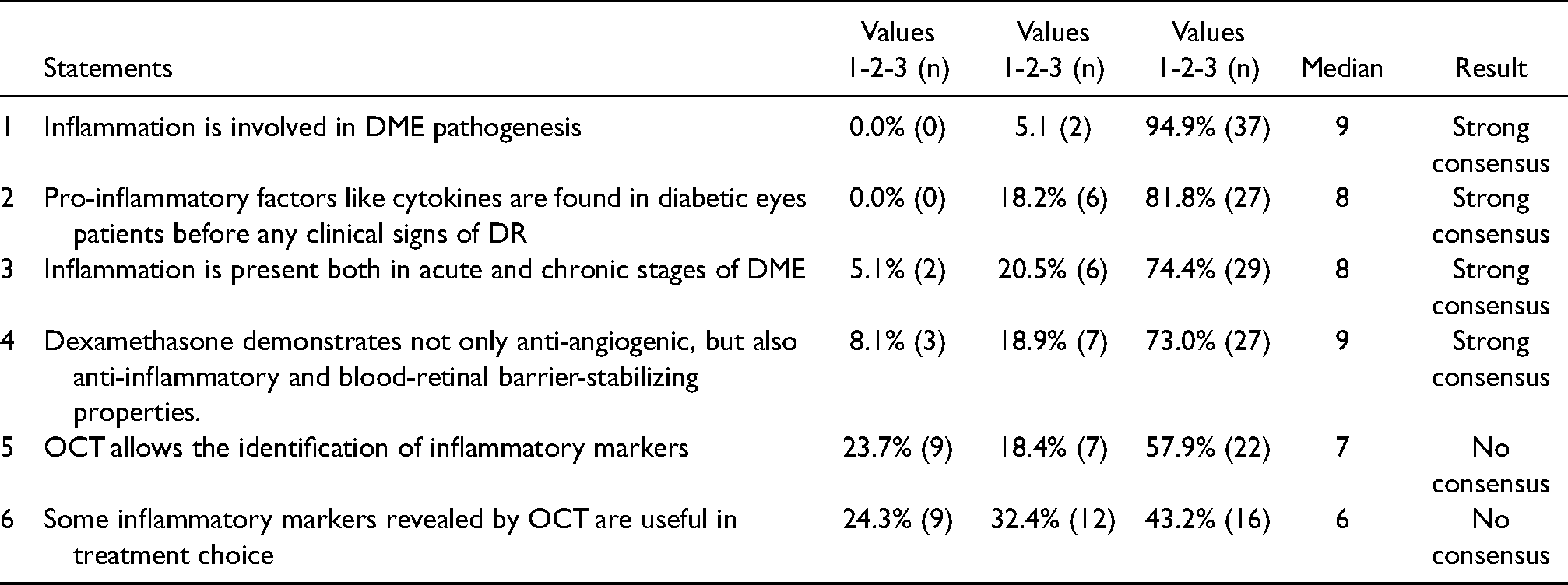
Statements relating to DME pathophysiology.
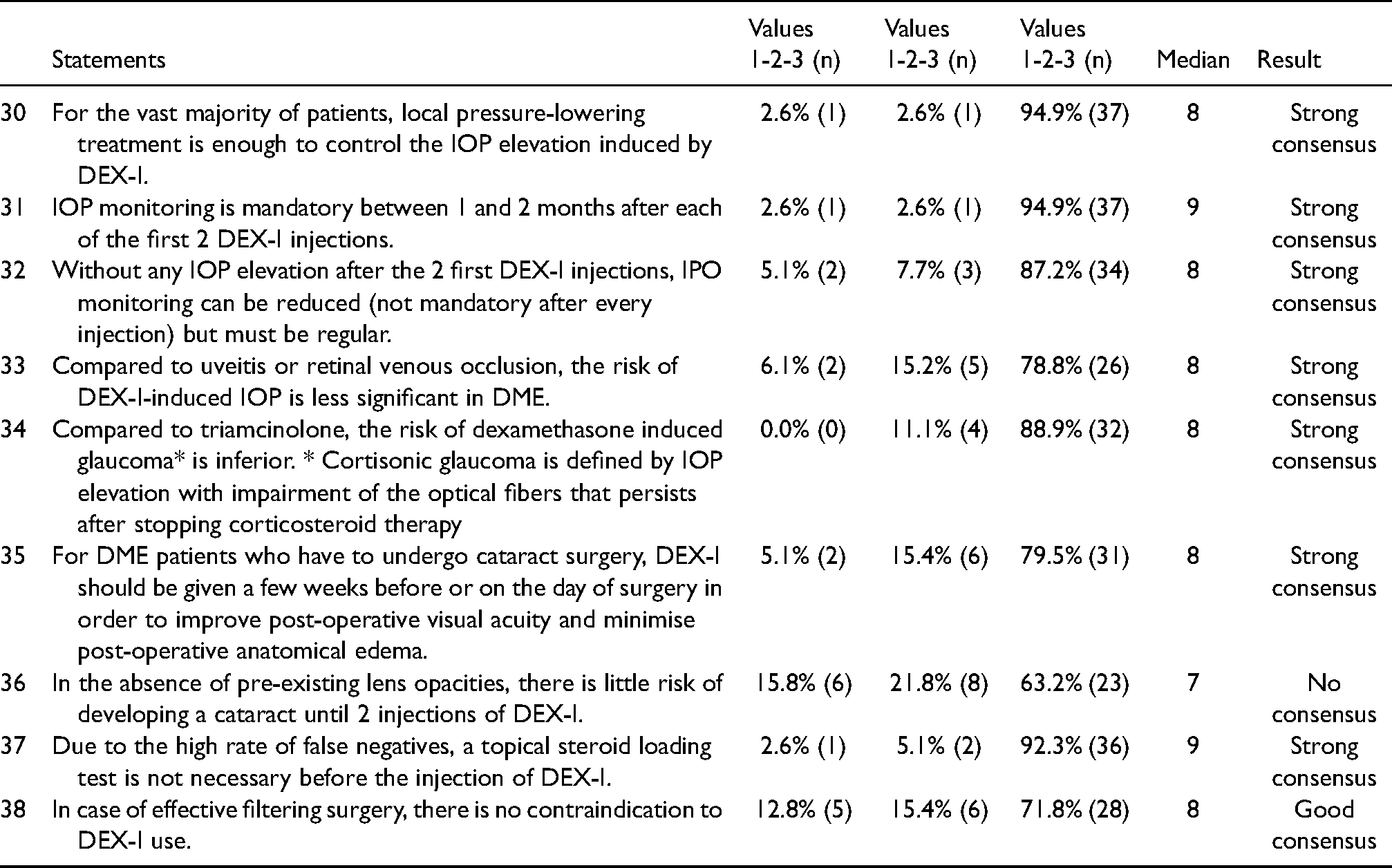
Statements relating to the safety of DEX-I.
Pathophysiology
The importance of inflammation in DME was recognised with strong consensus by panellists regarding its involvement in the development of the disease, the presence of biomarkers in the pre-symptomatic stage and its involvement in both the acute and chronic phase (Table 2). Experts also recognised with strong consensus the combination of anti-inflammatory, anti-angiogenic and blood-retinal barrier stabilising properties of dexamethasone. However, there was no consensus agreement regarding the ability of OCT to identify inflammatory biomarkers and to guide treatment choice.
Indications for the dexamethasone implant as a first-line treatment
A strong consensus was obtained regarding the potential of the dexamethasone implant to rapidly achieve a good anatomical response in the vast majority of treatment-naïve DME patients, as well as avoiding the use of a first-line anti-VEGF in patients with a recent cardiovascular history (Table 3).
Statements relating to DEX-I first-line indications.
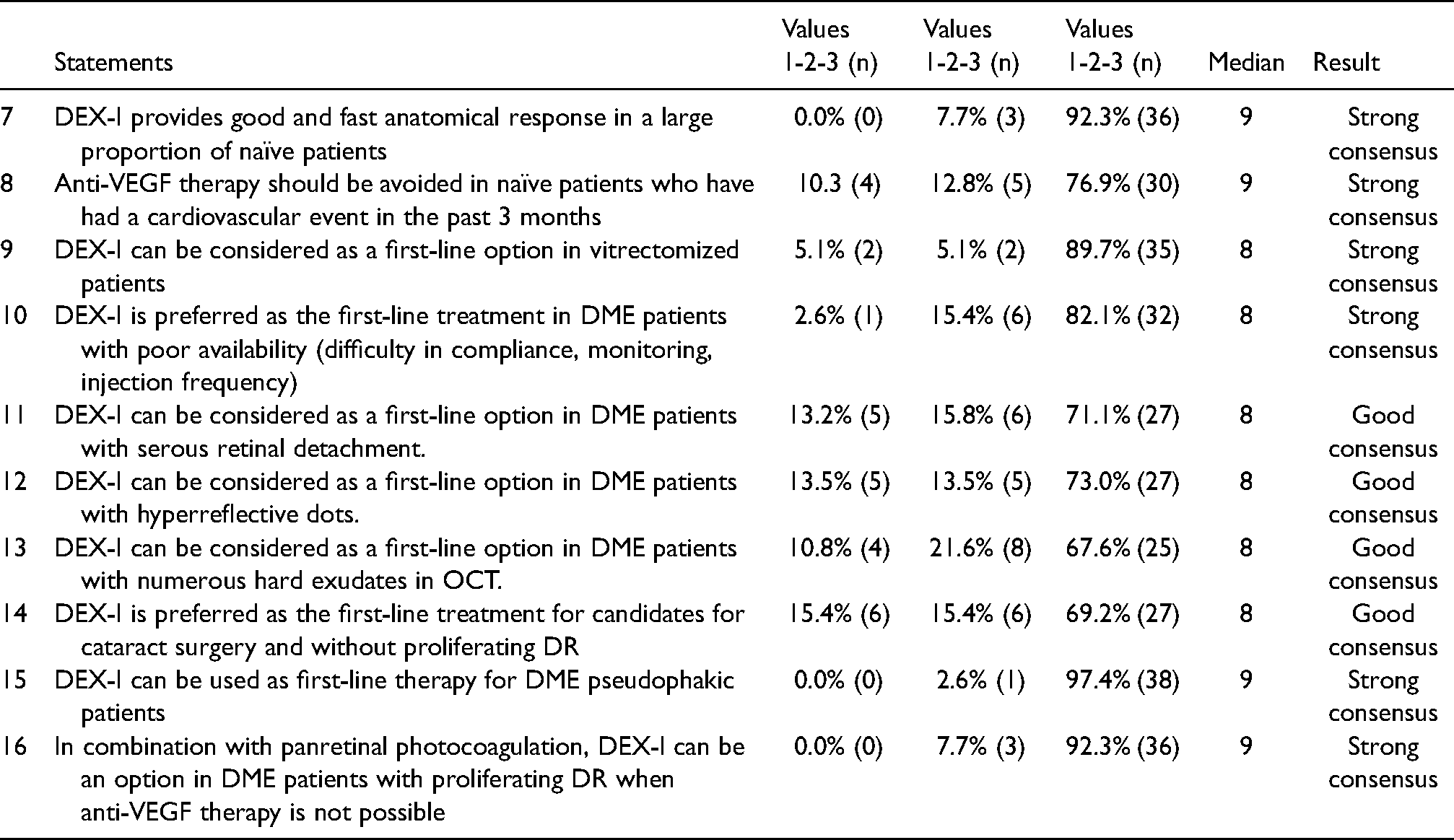
According to the experts, the dexamethasone implant was preferred as first-line treatment in DME patients with limited availability (difficulty in compliance, monitoring and/or injection frequency; strong consensus) and in those for whom cataract surgery was planned (good consensus).
The DEX-I was also considered as a first-line treatment option in patients with a history of vitrectomy (strong consensus), or with retinal serous detachment, hyper-reflective dots or numerous dry exudates in OCT (good consensus).
According to the experts, DEX-I can also be used in pseudophakic naïve patients and in combination with panretinal photocoagulation (PRP) in DME patients with proliferative diabetic retinopathy when anti-VEGF treatment was not possible (strong consensus).
Time to retreatment
Regarding the time between two injections of DEX-I, which the voting experts agreed to be between three and five months in the first year, a strong consensus was obtained on the need to proceed with a new injection without waiting for a drop in VA or major anatomical recurrence. For a patient presenting with recurrence after a dexamethasone implant, retreatment was felt to be possible as soon as exudative signs (whatever their importance) reappeared, without waiting for a drop in VA (Table 4).
Statements relating to the frequency of DEX-I injections.
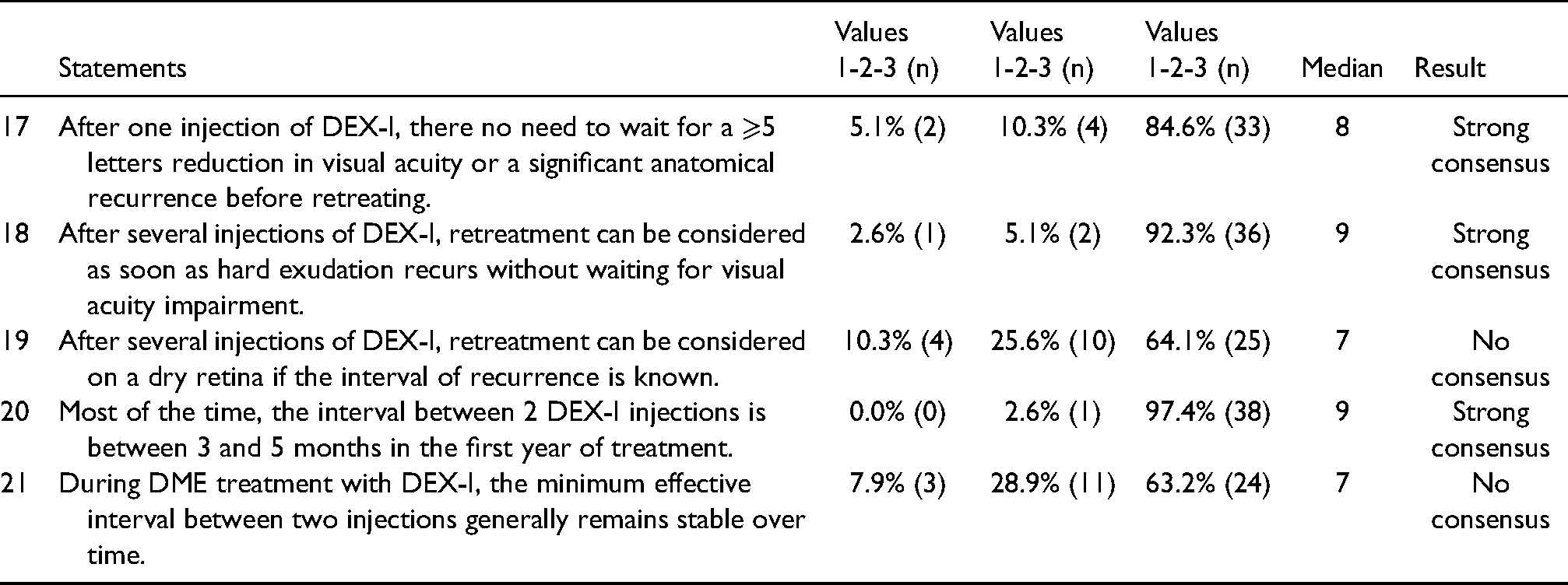
However, the stability of the interval between two injections was not fully recognised by the experts, in whom only 64% (median of responses = 7) stated that retreatment could be considered before exudative recurrence (i.e. in a dry retina) when the time interval to recurrence was known.
Efficacy criteria
The panel experts considered, with a good level of consensus, that non-response to anti-VEGF could be defined by the absence or incomplete efficacy after three to six months of treatment and for DEX-I by the absence of efficacy after two injections if DME was recent (Table 5). Consensus was not obtained regarding the lack of response to DEX-I for long-standing DME patients.
Statements relating to the assessment of efficacy of first-line treatments in DME.
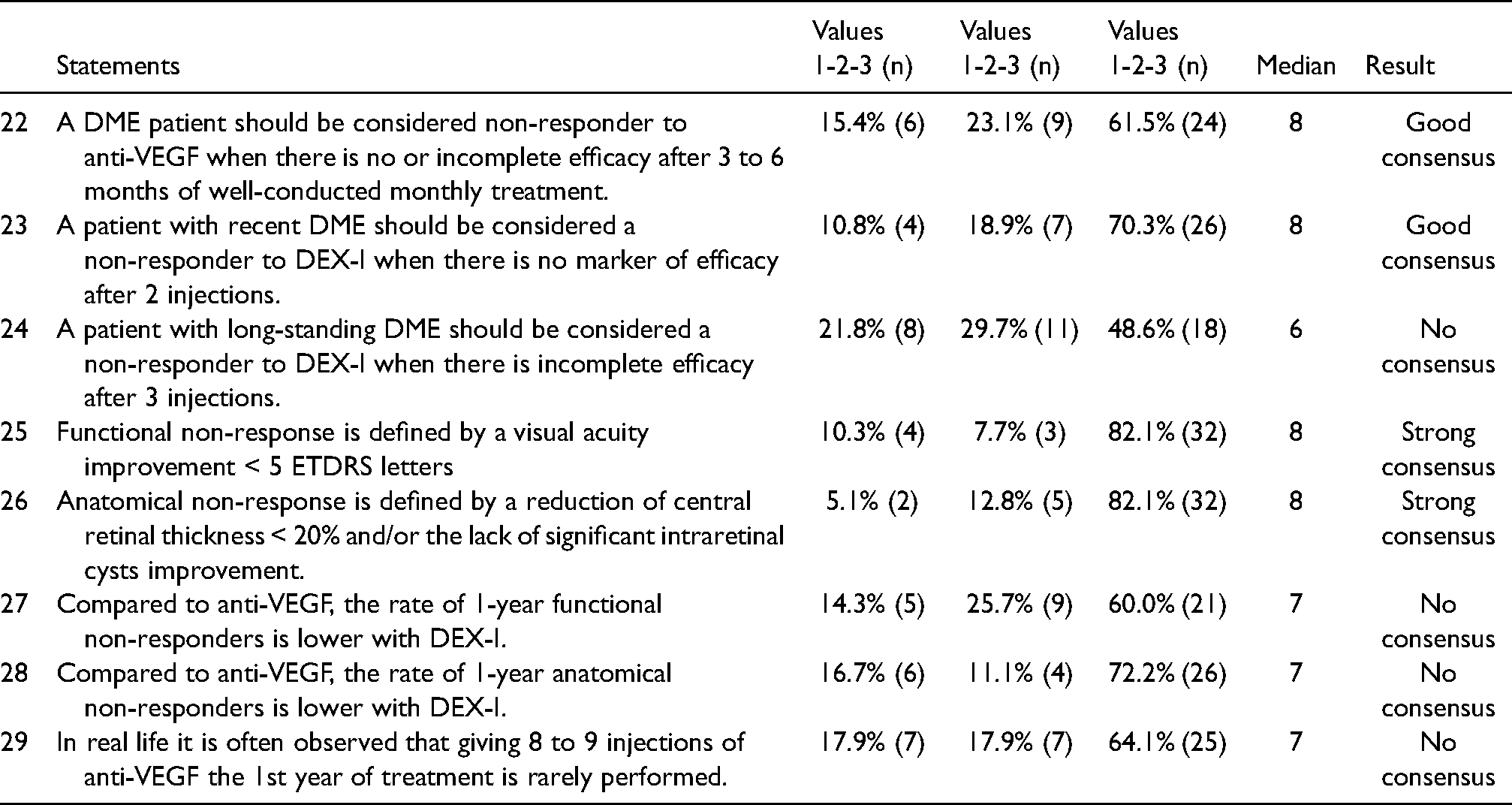
The panel reached a high level of consensus regarding the definitions of functional non-response (visual acuity gain of less than five letters) and anatomical non-response (reduction in central retinal thickness on OCT of < 20% and/or absence of significant intraretinal cysts improvement) (Table 5).
However, no consensus was reached on the lower rate of functional or anatomical non-responders at one year with DEX-I versus anti-VEGF. No consensus was reached also regarding the difficulty to perform in real life the 8 to 9 injections of anti-VEGF needed the first year of treatment (only 64% of agreement & median of responses = 7).
Safety
With regard to increased intraocular pressure (IOP) potentially induced by dexamethasone, the five statements proposed by the SC met strong consensus: lower risk of increased IOP in DME compared to uveitis or retinal vein occlusion; no use of the topical steroid loading test as a predictive factor; monitoring required approximately one to two months after the first two injections but possibly reduced thereafter; topical pressure-lowering treatment sufficient to control IOP increase in the vast majority of cases (Table 6).
Voting experts also widely acknowledged that the risk of corticosteroid-induced glaucoma was lower with dexamethasone vs. triamcinolone. They also agreed that - for patients with DME who need cataract surgery - DEX-I injection was preferred in the weeks leading up to the day of surgery.
The absence of a contraindication to using the dexamethasone implant in case of effective filtration surgery reached a good consensus.
However, the potentially low risk of developing cataract for up to two injections of dexamethasone implants in the absence of pre-existing crystalline opacities did not obtain a consensus agreement.
Discussion
Depending on the patient profile, several recommendations position the DEX-I as a possible alternative or even a preferred choice in DME therapeutic management.7,12,34,36 However, questions remain regarding its routine use and discrepancy exists between DME management in clinical practice, recent scientific evidence, and existing recommendations. The purpose of this focused study was, therefore, to establish both precise and pragmatic recommendations of DEX-I utilization by addressing all aspects of its use: presence of inflammation biomarkers, preferential or alternative indications, time to retreatment, assessment of efficacy, management of safety, all relying both on data from the literature and on the experience of French retinal experts.
The involvement of inflammation in the development of DME and its presence at all stages of the disease was consensual in our study. However, the inflammatory origin of the markers identified in OCT (i.e. hyperreflective dots, serous detachment…) and their utility in the choice of treatment were not recognised by the panellist experts. Although some recommendations have positioned DEX-I as first-line treatment in case of inflammatory DME pattern,7,12 no consensus was reached in the present study and the panel preferred to remain cautious about these statements.
In our study, the preferred prescription of DEX-I in the first-line setting was recognised in several situations: patients with a cardiovascular history of less than three months (for whom an anti-VEGF should be avoided); patients for whom the frequency of anti-VEGF injections in the first year presents a risk of poor adherence (patients not readily available, with adherence difficulty, monitoring or pace of injection); patients without proliferative diabetic retinopathy for whom cataract surgery was planned. DEX-I was also recognised as a possible first-line alternative to anti-VEGF in patients with a history of vitrectomy, with retinal serous detachment, hyper-reflective dots, numerous dry exudates in OCT and in pseudophakic naive patients. These results are broadly in line with recent recommendations favouring DEX-I in patients for whom cataract surgery is planned, or who are not readily available for the intensive frequency of anti-VEGF administration or with a history of vitrectomy.7,34,36
Panellist experts using our Delphi method established with strong consensus that it was not necessary to wait for a decrease in VA to retreat a DME patient with DEX-I. However, in eyes with a known interval of recurrence, retreatment before any anatomical recurrence, i.e. on a dry macula, was adopted by 64% of voters but did not obtain consensus according to the rules defined in our study. A specific definition of the “anatomical recurrence” was provided in the questionnaire i.e, increase of 50 microns or more in CSMT using SD-OCT imaging). 42 Treatment with DEX-I in PRN (pro re nata), as documented in several recent studies,43–46 could explain this caution. A difference was observed with anti-VEGF, widely used in age-related macular degeneration (AMD) with systematic retreatment at regular intervals, even in the case of dry retina, and this has certainly influenced the management of DME with these same drugs.33,47,48. Compared to PRN regimen, proactive regimen is known to provide better results in DME eyes treated with anti-VEGF in real life,49,50 however this has not been yet demonstrated for DEX-I treatment.
Our study found a consensus on the fact that the average interval between two DEX-I injections was between three and five months in the first year. However, only 46% (round 1 of our Delphi consensus) and 63% (round 2) of panellist experts admitted that this interval increased (round 1) or was stable (round 2) over time. Data in the literature from both pivotal 51 and real-world studies 52 showed that this interval increases over time. Besides, a recent German Delphi found a broad consensus on this statement (82%). 34
Another surprise from our study was the lack of consensus (64%, median = 7 out of 10) regarding the difficulty of administering eight to nine anti-VEGF injections in the first year of treatment, while data showing the risk of under-treatment with anti-VEGF drugs have been reported numerous times.47,48,53–57 A recent analysis of 32 observational articles with anti-VEGFs in DME found an average number of injections of 5.8 over an average follow-up of 15 months. 8 It, therefore, seems that French retina specialists knowing these real-world data, nevertheless considered that they have organised their practice to be able to manage these number of injections for their patients. Recent changes in clinical practice (optimisation of follow-up visits, use of fixed or proactive regimen) may have improved DME treatment in real life, however only a quantitative assessment of clinical practices can confirm this perception. As such, the authors of this article who record their activity in the Fight Retinal Blindness registry (information available at savesightregistries.org) acknowledge that the actual average number of anti-VEGF injections in their expert centre was significantly lower than their expectations. 58 Between patient tiredness, intercurrent systemic disease related to diabetes, temporary unavailability of the injecting ophthalmologist and programming errors, the causes of potential delay are multiple and lead to a reduced number of injections at the end of the first twelve months, lower than that of randomised and controlled pivotal studies.
While the definitions of functional non-response and anatomical non-response were very broadly agreed in our Delphi method, the waiting time before switching to another therapeutic class was less consensual. The French experts considered that it was generally necessary to wait three to six months for an anti-VEGF to be considered ineffective; their Spanish colleagues considered it to be three injections 12 and the Italians six injections. 36 Regarding the post-dexamethasone switch, our panellists recommended waiting for two injections without efficacy in a recent DME, but did not approve to consensus the wait for three injections in the case of a long-standing DME. Additional studies would probably be useful to clarify these delays and justify – or not – a difference according to lasting time of DME.
Regarding the IOP elevation management, 4 statements were largely consensual across our participants: local pressure-lowering treatment is enough to control the IOP elevation for the vast majority of patients; IOP monitoring is mandatory between 1 and 2 months after each of the first 2 DEX-I injections ; IOP monitoring could be reduced (but still regular) when no IOP took place after injections #1 and #2; due to a high rate of false negatives, topical steroid loading test remains optional before injection. The authors would like to highlight the need to control IOP systematically after the two first DEX-I injections. In SAFODEX and SAFODEX-2 studies, the hypertonic cases were detected after the first and second injections in 87% and 80% of the cases, respectively.59,60 However, only 63% of French retinal ophthalmologists - versus 86% for Spanish experts 12 - estimated that the risk of developing a cataract after two injections of dexamethasone on a clear lens was low. As the concept of cataract is questionable, surgical indication would have been probably more precise to obtain a broad consensus from the French experts.
Although the Delphi consensus is a structured procedure, this approach is not without certain limitations linked to the drafting of statements, the criteria considered to define the consensus and the profile of voting experts. 61 Our study tried to limit these potential biases as much as possible to ensure maximum objectivity. Despite their recruitment in a single country, voters were selected based on objective criteria combining experience and expertise that made it possible to obtain a sample with reassuring characteristics: 15 years of experience in DME on average and 100% with recent active participation in a research project in this disease. The high participation rate (44%) and the absence of attrition between vote 1 and vote 2 also attested to their strong involvement. Regarding the statements, prior analysis of other European Delphi methods12,34,36 allowed us to address the main questions raised in practice and often propose more precise statements, in particular on the preferential or alternative indications of DEX-I. As for the threshold used to define the consensus, our study was based on a rigorous two-criterion approach, unprecedented to our knowledge in ophthalmology: consensus rate (75% of responses ≥7) to assess the general level of adherence and the median (≥ 8) to illustrate the distribution of responses. This strict and demanding definition provides strong credibility for our results. Finally, our program was carried out with a continuous and complete separation between panellist experts and members of the SC, who neither participated in the vote nor directly interacted with the retina specialists interviewed in a completely anonymous manner. That process could be a real advantage in terms of pragmatism and applicability compared to scientific societies guidelines written by experts in a more top-down approach. The constraint inherent in this separation was the absence of direct exchanges between participants, or between participants and members of the SC. This type of debate however could have been useful for reformulating certain statements.
Conclusion
This Delphi consensus study in France showed that there was a very good level of consensus on the management of DME by dexamethasone implant injections (58% strong consensus and 18% good consensus, therefore a total consensus of 76%). Supported by a strong consensus regarding its pathophysiological rationale, its overall clinical efficacy, its frequency of injections and its known and controlled safety profile, the panellists recommended DEX-I preferential use as a first-line treatment in certain situations (patients not readily available, requiring cataract surgery or with recent cardiovascular history) and as a therapeutic alternative to first-line anti-VEGF in several others (patients with a history of vitrectomy, retinal serous detachment, hyper-reflective dots or dry exudates in OCT). Conversely, some points considered as good statement for the SC experts (stability or even prolongation of the interval between two injections over time, difficulty in carrying out in common practice the eight to nine anti-VEGF injections required in the first year) were not validated by the panel experts. Finally, certain points of uncertainty, such as the role of OCT markers in OCT and the minimal number of injections required to assess efficacy before switching treatment, would justify further studies. Overall, this Delphi study provides pragmatic recommendations that should be useful to ophthalmologists in the routine management of DME as a consensual professional agreement.
Footnotes
Acknowledgements
The authors would like to thank the following physicians for their active participation: Yacine AILEM, Jad AKESBI, Sandrine ALLIEU, Karine ANGIOÏ, Frank BECQUET, Mounir BENZERROUG, Chloé CHAMARD, Anne COUZINET, Stéphane DELAGE, Franck FAJNKUCHEN, Éric FOURMAUX, Pierre GASCON, Vincent GUALINO, Ruxandra HERA, Marie-Laure LE LEZ, Olivier LEBRETON, Amélie LECLEIRE COLLET, Laurence MAHIEU, Pascale MASSIN, Thibaud MATHIS, Cyril MEILLON, Audrey-Émilie MERCIER, Anh-Minh N’GUYEN, Hassiba OUBRAHAM-MEBROUKINE, Éric PARRAT, Loïc PINSARD, Maud RIGHINI, Thi Ha Chau TRAN, Joël UZZAN, Frédéric VILLEROY.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: LK reports fees from Abbvie, Allergan, Bayer, Novartis, Roche, Théa; all outside the submitted work. SB declared conflicts of interest from Allergan, Novartis, Bayer, Horus Pharma, Bausch et Lomb; all outside the submitted work. AC declared conflicts of interest from Abbvie, Allergan, Bayer, Novartis; all outside the submitted work. CCG declared conflicts of interest from Abbvie, Allergan, Bausch and Lomb, Bayer, Novartis, Roche, Théa, Horus Pharma; all outside the submitted work. MND declared conflicts of interest from Allergan, Bayer, Novartis, Horama, Horus Pharma, Théa; all outside the submitted work. FM declared conflicts of interest from Alcon, Allergan, Bausch & Lomb, Bayer, Horus, Novartis, Thea; all outside the submitted work. MW declared conflicts of interest from Abbvie, Allergan, Bayer, Horus, Novartis, Théa; all outside the submitted work.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Allergan (grant number Unrestricted Medical Grant).