
Abstract
Purpose
To evaluate the follow up and treatment outcome of central serous chorioretinopathy (CSCR) based on the new multimodal imaging-based classification and identify the predictors for anatomic and visual outcome.
Methods
Retrospective, multicentric study on 95 eyes diagnosed with CSCR and a follow up of at least 12 months were included. Eyes with macular neovascularization, atypical CSCR or any other disease were excluded.
Results
At the baseline, observation was advised to 70% eyes with simple CSCR whereas photodynamic therapy (PDT) was performed in 49% eyes with complex CSCR. Over the follow up, decrease in CMT was significantly higher in simple CSCR as compared to complex CSCR (P = 0.008) and the recurrences were significantly more in eyes with lower CMT at baseline (P = 0.0002). Median time of resolution of SRF was 3 months and 6 months in simple and complex CSCR respectively (P = 0.09). For the 12 months follow up, the median fluid free period was greater (P = 0.03) while number of interventions performed was lesser in eyes with simple CSCR as compared to complex CSCR (P = 0.006). Multiple regression analysis showed baseline best corrected visual acuity (BCVA) and baseline persistent SRF to be significantly predictive of BCVA and persistent SRF at 12 months (P < 0.0001, 0.04) respectively.
Conclusions
Complex CSCR more often required PDT, was associated with shorter fluid free interval and longer time for SRF resolution. Baseline BCVA and persistent SRF were predictive of final visual and anatomical outcome. The new multimodal imaging based classification is helpful in establishing objective criteria for planning treatment approaches for CSCR.
Keywords
Introduction
Central serous chorioretinopathy (CSCR) is characterized by neurosensory detachment (NSD) at the posterior pole that may be associated with pigment epithelial detachment (PED) due to choroidal permeability and dysfunctional retinal pigment epithelium (RPE).1,2 Despite being a very commonly encountered disease seen by the retina specialists, the discrepancies in the terminology and classification are well known.2–4 Evaluations and conclusions on relative efficacy and safety of various treatment modalities in CSCR are thus unreliable because of variability in duration threshold in acute versus chronic CSCR (ranging from 6 weeks to 6 months), subjectivity in reporting symptoms by the patients, variability in case selection for inclusion in various studies and non-consensus for the conventional classification amongst retinal experts.3–6 A new multimodal imaging based classification system of CSCR was proposed by the CSCR international group to overcome the existing pitfalls and eventually aid in formulation of objective treatment guidelines of CSCR. 7 According to this classification, each case is classified as (i) simple versus complex [2-disc diameters (DD) of RPE abnormality]; (ii) primary versus recurrent versus resolved CSCR; (iii) Persistent [subretinal fluid (SRF) >6 months] or not; (iv) outer retinal atrophy (ORA) present or absent; (v) foveal involvement present or absent; and (vi) macular neovascularization (MNV) present or absent. Evaluation of treatment outcomes using this objective and validated multimodal imaging based classification will be useful to establish standardized recommendations in CSCR management. 8
The purpose of this study was to evaluate the follow up and treatment outcome of CSCR based on the new multimodal imaging based classification and identify the predictors for anatomic and visual outcome.
Materials and methods
This was a retrospective study in which data of patients with a known diagnosis of CSCR at multiple centers (USA, Russia, Italy, India) was evaluated between 2013 to 2020. The study adhered to the tenets of the Declaration of Helsinki and ethical clearance was obtained by the institutional review board. Patients consent for inclusion of their retrospective data in the study was obtained.
Inclusion criteria included (i) availability of demographic details, history, comprehensive eye examination and treatment details at baseline, 3 months, 6 months and 12 months (longer follow up was included when available) (ii) good quality multimodal imaging available at baseline and all follow up visits. Exclusion criteria included follow up of less than 12 months; evidence of MNV; atypical CSCR; any other retinal disease or any intraocular surgery other than an uncomplicated cataract surgery. Inclusion and exclusion criteria were satisfied by 95 eyes of 93 patients.
Multimodal imaging included fundus autofluorescence (FAF), spectral domain optical coherence tomography (SD OCT)(B scan) and optical coherence tomography angiography (OCTA) or fundus fluorescein angiography (FFA) with indocyanine angiography (ICGA, if available). FAF, fundus photographs, FFA and ICGA were obtained from Spectralis HRA + OCT (Heidelberg Engineering, Heidelberg, Germany) or F-10 scanning laser ophthalmoscope (NIDEK, Gamagori, Japan). OCTA examinations including a 6 × 6 mm (2 orthogonal volumes with 400 × 400 A scans) pattern centered at the fovea was performed with the RTVue-XR Avanti (Optovue, Fremont, CA) or Spectralis HRA + OCT. For each eye, volumetric scans (49 scans) through the macula were obtained. Central macular thickness (CMT) was measured using in-built callipers as a distance between the internal limiting membrane (ILM) and the hyperreflective line of RPE using the scan passing through fovea. Subfoveal choroidal thickness (SFCT) was measured manually as the subfoveal vertical distance between the Bruch membrane interface and the sclerochoroidal junction on the OCT B scan. Only the eyes in which the entire choroid (from Bruch membrane to sclerochoroidal interface) was clearly visible were selected for the analysis.
Definitions
As per the new classification, 7 CSCR was classified into simple and complex subtypes based on the area of RPE alterations identified on FAF imaging. Eyes with total area (cumulative) of RPE alteration >2 DD or multifocal area of involvement were classified as complex CSCR, while eyes with ≤2 DD of RPE abnormality were classified as simple CSCR. For categorizing the cases as per the episode; an eye was noted to have a primary episode of CSCR if there was no history or signs of a previous episode; recurrent CSCR was noted if there was a history or signs of a previous episode and CSCR was noted to be resolved if there was no SRF on SD OCT. Eyes were categorized into persistent CSCR if SRF was noted on SD OCT along with a history of the current episode for > 6 months. ORA was documented on SD OCT if there was outer nuclear layer (ONL) thinning or ellipsoid zone (EZ) and external limiting membrane(ELM) disruption. Fovea was noted to be involved (Fovea+) if there was SRF or PED or ORA at the fovea on SD OCT. All eyes were classified by two masked retinal experts (SA and DM) as mentioned above. In cases of non-consensus, a senior investigator (JC) was consulted.
Classification of all the eyes was done at the baseline, 3 months, 6 months, 12 months and at a longer follow up (if available). Comparison of baseline characteristics was done between simple and complex CSCR and follow up of simple and complex CSCR was evaluated. Changes of various parameters over the follow up as well as at final follow up were assessed. Treatment prescribed at the baseline as well as that performed subsequently along with eventual outcome (anatomic resolution and final visual acuity) was compared between simple and complex CSCR. Treatment options included observation, focal laser, micropulse laser, photodynamic therapy (PDT) and eplerenone. The settings for focal laser were 70–110 mW, 100 µm, 100 ms; and for micropulse laser were 5% duty cycle, 200 ms, 100 µm contiguous spots. Half fluence PDT was performed with a 689 nm laser with a standard dose of verteporfin (6 mg/m2) and energy of 25 mJ/cm2. Eplerenone was started with a dose of 25 mg once a day for 1 week and then increased to 50 mg once a day.
Finally, time of resolution of SRF, fluid free period, number of interventions and recurrences during follow up were evaluated in simple and complex CSCR. For counting the number of interventions in an eye, if an eye was observed over 12 months then the number of interventions was noted to be zero. If a single intervention was done (PDT/ micropulse laser/focal laser/eplerenone), the number of interventions was noted to be 1. In case of non resolution with the first intervention, if a second intervention was done then the number of interventions was noted to be 2. If an additional treatment was performed, the number of interventions was noted to be 3. Total number of interventions performed in the 12 months period was documented for each eye.
Statistical analysis
Statistical analysis was performed using MedCalc 18.4.1(MedCalc Software, Ostend, Belgium). The data was tested for normality distribution using the Kolmogorov–Smirnov test and did not fit a normal distribution. All data is presented as the median and 95% confidence interval (CI). Correlation coefficient was calculated between final BCVA and baseline BCVA, subfoveal choroidal thickness (SCT), and central macular thickness (CMT). The Mann–Whitney and chi-squared tests were used to compare the difference between the CSCR classes in continuous and categorical variables, respectively. Multiple regression models, including baseline BCVA, SCT, CMT, CSCR class (simple versus complex), persistence of SRF at baseline, and baseline prevalence of ORA, were constructed to find the variables independently associated with final BCVA and persistence of SRF at final follow up. The Wilcoxon test was used to evaluate statistical significance of changes in BCVA, SCT, CMT over follow-up. P-values <0.05 were considered statistically significant. The 12-month cumulative persistence probability was calculated using the Kaplan–Meier method for the cases that were only observed in the two CSCR classes (simple and complex) and for different treatment options.
Results
The dataset consisted of 95 eyes of 93 patients, consisting of 80 males and 13 females. Median age of patients was 47 years and there was bilateral involvement in 2 patients. History of steroid use was noted in 21 patients. Median duration of complaints was 4 months (range:0.1–144 months, mean:10.2 ± 22.5 months).
Baseline characteristics
At the baseline, 46 eyes had simple CSCR, 49 eyes had complex CSCR, 73 eyes had a primary episode, 20 eyes had a recurrent episode and 2 eyes had resolved CSCR. Persistent SRF was documented in 27 eyes, ORA in 30 eyes and foveal involvement in 89 eyes. All the eyes had a follow up of at least 12 months, 48 eyes (50.5%) had a longer follow up (13–84 months) and the mean follow up of all eyes was 23 ± 17.3 months.
The baseline characteristics of simple versus complex CSCR have been tabulated in Table 1. Median duration of complaints was 1 month in eyes with simple CSCR and 8 months for complex CSCR (P < 0.0001). There was no significant difference between simple and complex CSCR in regards to the age of the patients, BCVA, SCT and foveal involvement. The risk for a complex CSCR was lesser in females [odds ratio (OR) = 0.14, P = 0.014 (95% CI: 0.03–0.67). CMT was higher in simple CSCR (P = 0.04); while recurrent episodes, persistent SRF and ORA were higher in complex CSCR (P = 0.001, <0.0001 and <0.0001).(Table 1)
Baseline characteristics and their comparison between simple and complex central serous chorioretinopathy (CSCR).
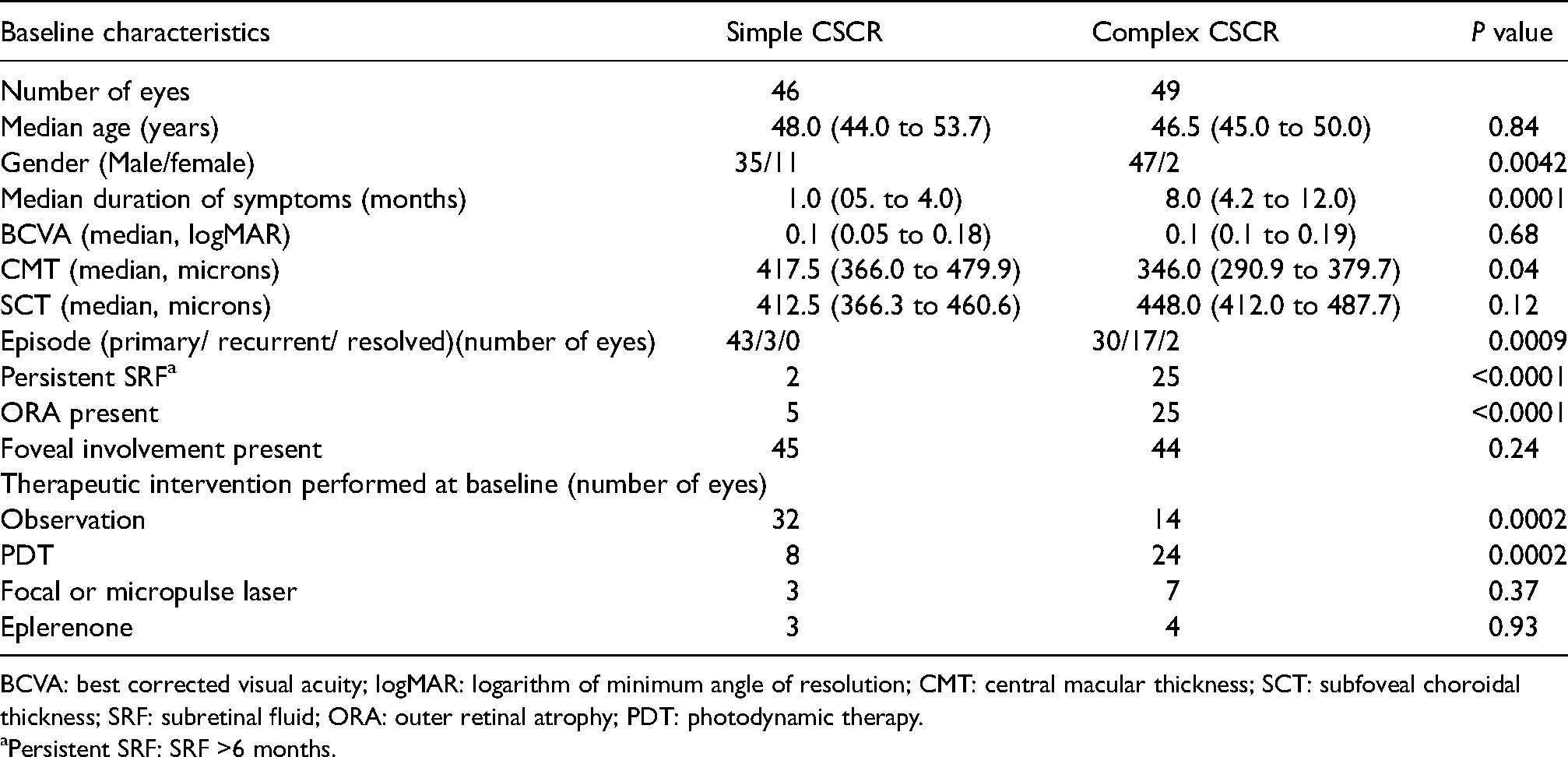
BCVA: best corrected visual acuity; logMAR: logarithm of minimum angle of resolution; CMT: central macular thickness; SCT: subfoveal choroidal thickness; SRF: subretinal fluid; ORA: outer retinal atrophy; PDT: photodynamic therapy.
Persistent SRF: SRF >6 months.
Therapeutic intervention
At the baseline, observation was advised in 32 eyes of simple CSCR versus 14 eyes in complex CSCR (P = 0.0002); while PDT was performed in 8 eyes of simple CSCR versus 24 eyes of complex CSCR (P = 0.0002).(Table 1) Median number of interventions performed over the 12 months follow up period was zero for simple CSCR (95% CI: 0.0 to 1; range 0 to 2) and one for complex CSCR (95% CI: 1.0 to 1.0; range: 0 to 3) (P = 0.006).
Follow up characteristics
Over 12 months follow up, in simple CSCR group, there was a significant decrease in CMT, SCT and number of cases with foveal involvement (P = <0.0001, 0.011 and 0.003) along with significant improvement in BCVA (P = 0.01). The number of resolved cases, persistent SRF and ORA (P < 0.0001, 0.0003 and 0.0003) increased over 12 months follow up. In complex CSCR, CMT and number of cases with foveal involvement decreased significantly (P < 0.0001 and 0.004); number of resolved cases and BCVA improved significantly (P < 0.0001, 0.04) and there was no significant change in SCT and in the number of eyes with persistent SRF and ORA (P = 0.11, 0.68 and 0.22) over 12 months follow up. Over the follow up period, decrease in CMT was significantly higher in simple CSCR as compared to complex CSCR (P = 0.008). Eight eyes with simple CSCR and 7 eyes with complex CSCR experienced a recurrence during the follow up period (P = 0.96) but the recurrences were significantly more in eyes with lower CMT at baseline (P = 0.0002). The final BCVA, CMT, SCT, type of episode, persistence, ORA and foveal involvement were not significantly different between simple and complex CSCR (P = 0.49, 0.9, 0.12, 0.13, 0.59, 0.12 and 0.94) (Table 2).
Characteristics at the 12 month follow up, at the baseline and change over the follow up within the groups [simple and complex central serous chorioretinopathy (CSCR)] and between the groups.
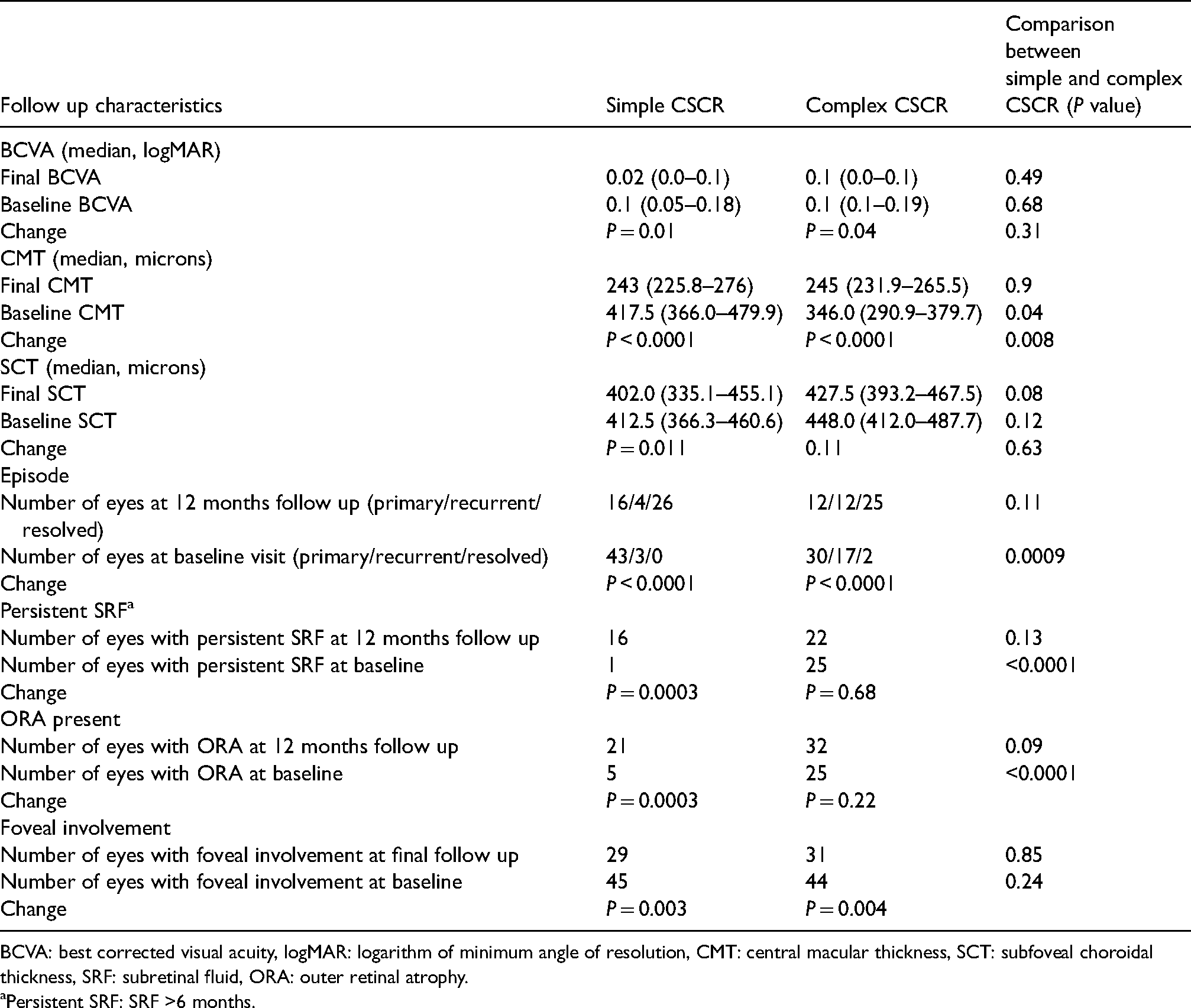
BCVA: best corrected visual acuity, logMAR: logarithm of minimum angle of resolution, CMT: central macular thickness, SCT: subfoveal choroidal thickness, SRF: subretinal fluid, ORA: outer retinal atrophy.
Persistent SRF: SRF >6 months.
The persistence probability in patients that were observed without any treatment after 12 months determined from Kaplan–Meier analysis was 50% for complex CSCR and 33% for simple CSCR (Figure 1A). Comparison of the two survival curves (persistence probability) with the log-rank test showed no statistically significant difference (P = 0.3) between two CSCR classes. The persistence probability after 12 months as determined from Kaplan-Meier analysis was 31.3%, 38.3% and 50% in the PDT, observation and focal laser treatment respectively (Figure 1B). Comparison of survival curves (persistence probability) with log-rank test showed no statistically significant difference (P = 0.68) between different treatment options.
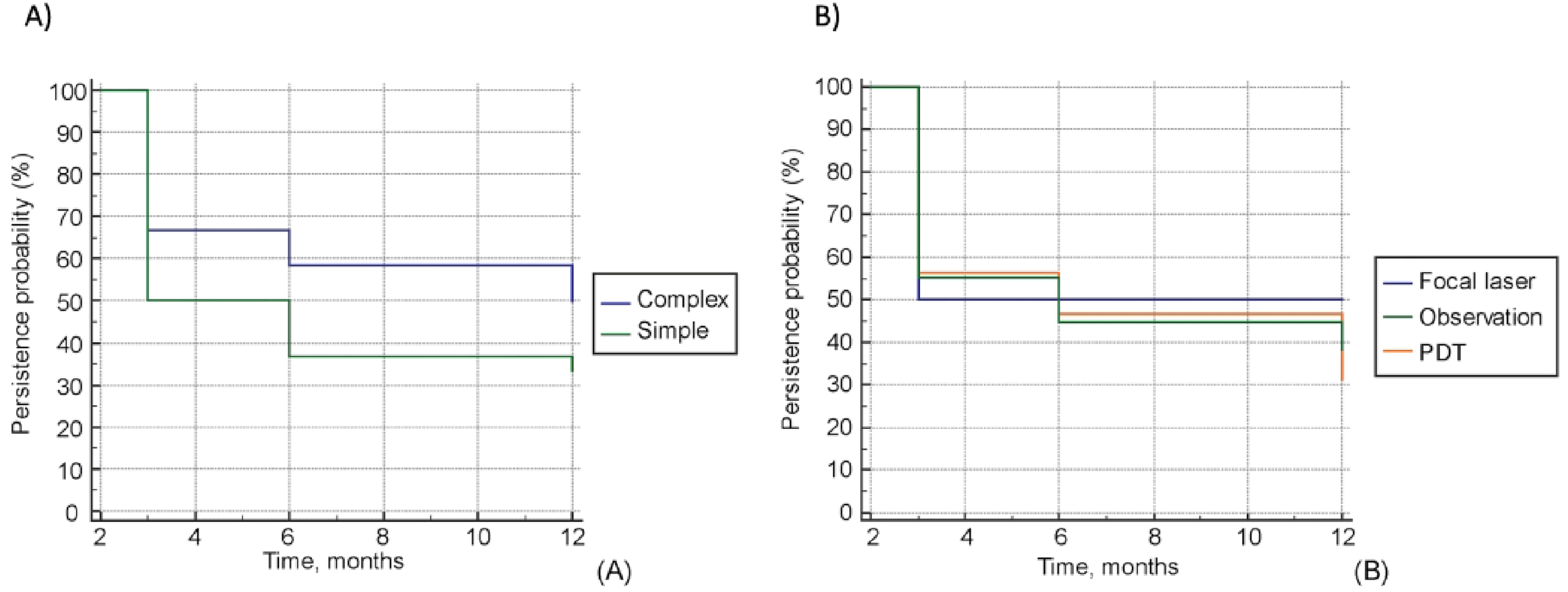
Persistence probability over 12 months depicted with a Kaplan-maier curve in (A) cases that were only observed in simple versus complex central serous chorioretinopathy (CSCR) (B) with various treatment options such as observation, focal laser and photodynamic therapy (PDT).
Anatomical outcome, time of resolution and fluid free period
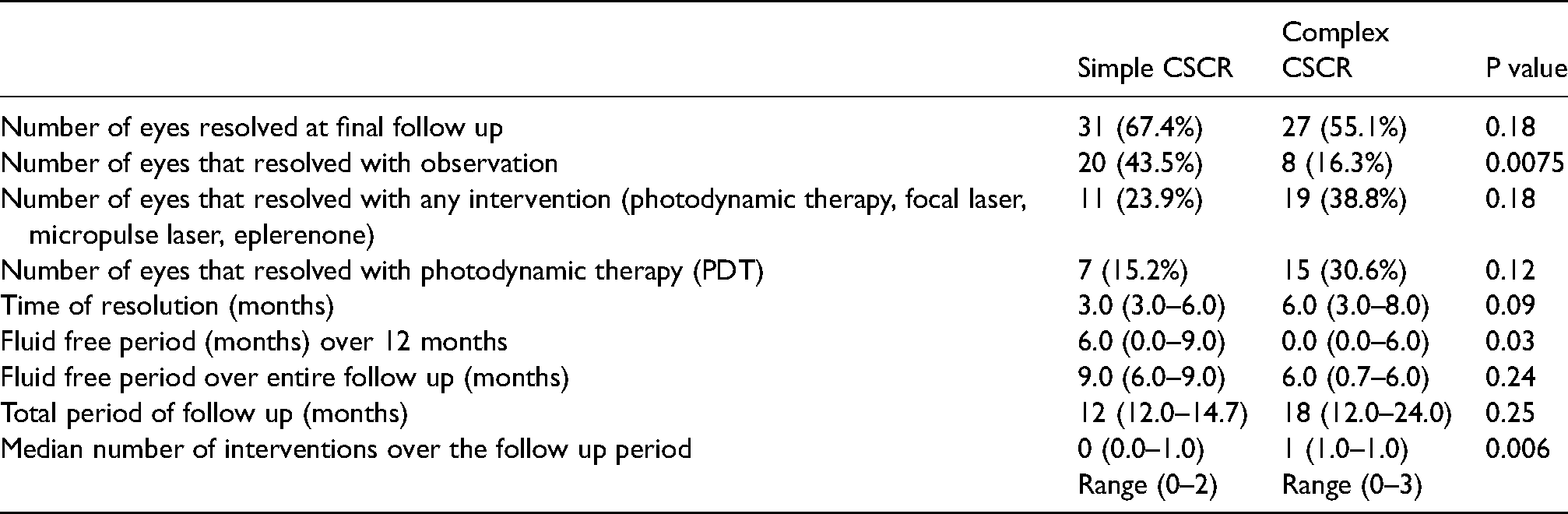
At the final follow up (mean 22.8 ± 16.6 months), complete resolution was noted in 31 out of 46 (67.4%) eyes of simple CSCR and 27 out of 49 (55.1%) eyes of complex CSCR (P = 0.18). Twenty eyes of simple CSCR versus 8 eyes of complex CSCR resolved with observation (P = 0.008). Median time of resolution of SRF was 3 (3.0–6.0) months in simple CSCR cases and 6 (3.0–8.0) months in complex CSCR cases. For the whole study group, over the 12 months follow up duration, the median fluid free period was significantly greater in eyes with simple CSCR [6 (0.0–9.0) months] as compared to complex CSCR [median fluid free interval: 0(0.0–6.0) months] (P = 0.03). During the entire follow up duration, eyes with simple CSCR had a median fluid free interval of 9 months (range: 6.0–9.0 months) out of total median follow up of 12 months (range:12.0–14.7 months) while complex CSCR eyes had a median fluid free interval of 6 months (0.7–6.0) out of the total follow up of a median of 18 months (12.0 to 24.0) (P = 0.2).(Table 3)
Comparison of anatomical outcome, time of resolution, fluid free period and number of interventions between simple and complex central serous chorioretinopathy (CSCR).
Predictors of visual outcome
There was a significant correlation between BCVA at 12 months and baseline BCVA (r = 0.77, P < 0.001) and baseline CMT (r = 0.32, P = 0.002). On univariate analysis, there was a significant association between baseline BCVA and baseline CMT with BCVA at 12 months (P < 0.0001 and P = 0.002 respectively). With multiple regression analysis, only baseline BCVA was significantly associated with BCVA at 12 months (P < 0.0001). The model also showed that the persistence (fluid for more than 6 months) at baseline was significantly associated with persistent SRF at 12 months (P = 0.04).
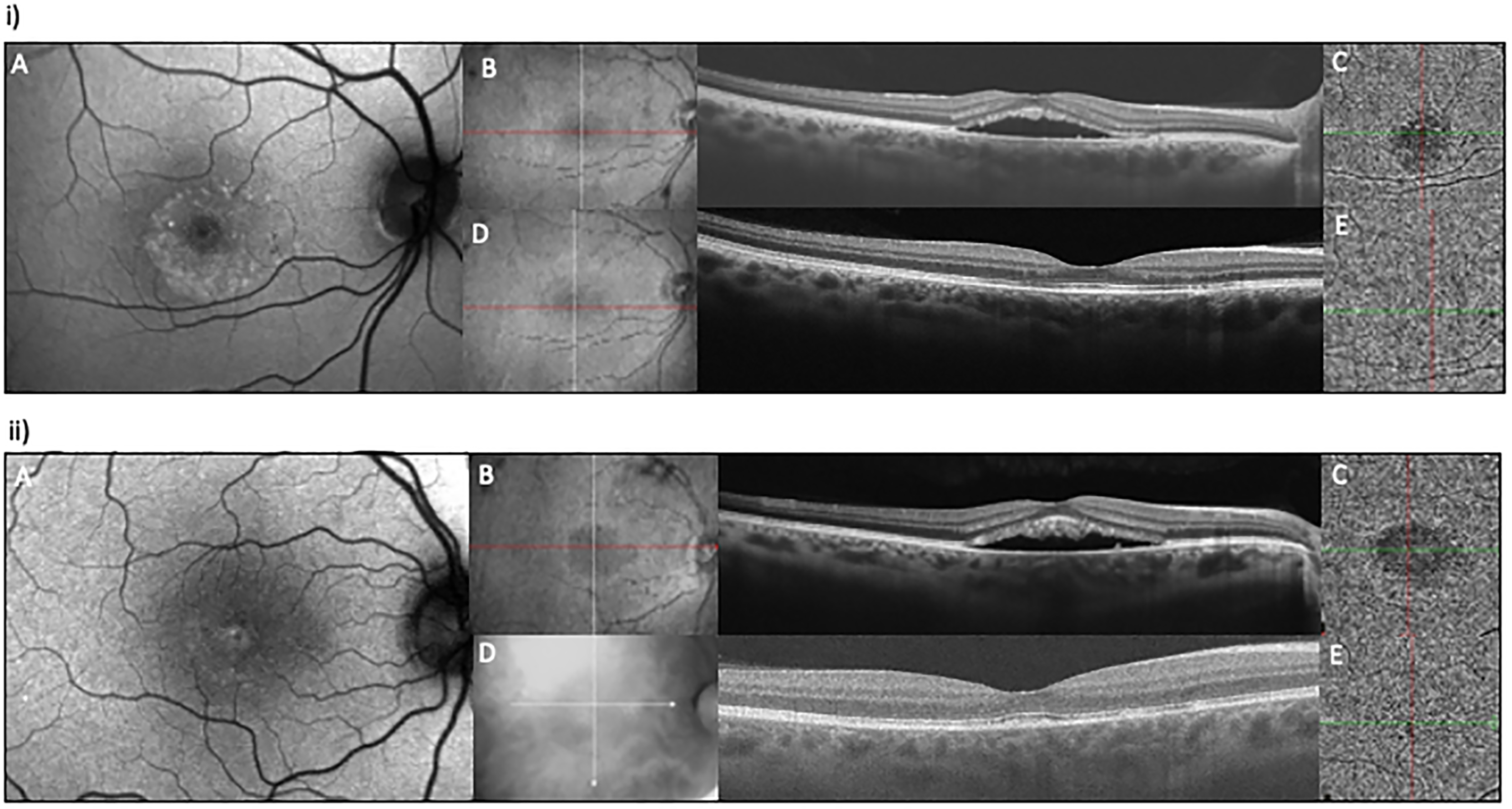
Figure 2(i) and (ii) are demonstrating two representative cases of simple CSCR and Figure 3(i) and (ii) depict two representative cases of complex CSCR.
(i
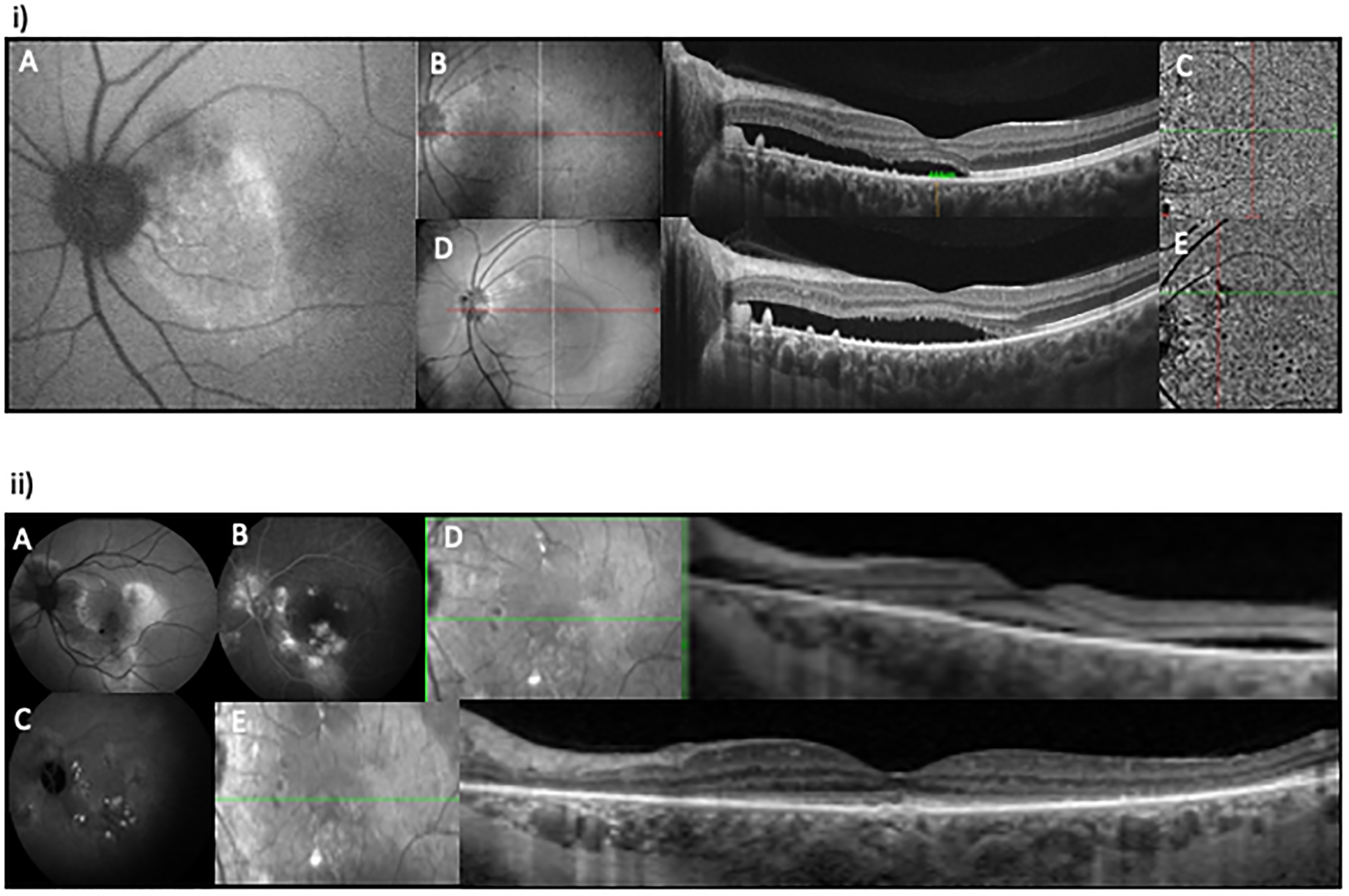
(i). A 54-years-old male presented with blurred vision in left eye for 8 months, BCVA of 20/40 and there was no history of recurrence. (A) FAF image at baseline depicted >2 DD of RPE abnormality (complex CSCR), (B) OCT (B scan) at the baseline demonstrated SRF involving the fovea with ORA and (C) OCTA at baseline ruled out MNV. Eye was classified as complex, primary, persistent CSCR, ORA+, fovea+. Patient denied treatment and therefore he was observed. There was no resolution until his last follow up at 18 months, (D) OCT (B scan) shows persistent SRF involving fovea with ORA and (E) OCTA at 18 months ruled out MNV. Fluid free interval was noted to be zero out of a total follow up of 18 months and number of interventions was also zero. (ii
Discussion
This retrospective study demonstrated that observation was advised to 70% eyes with simple CSCR whereas PDT was offered to 49% eyes with complex CSCR at the baseline. In terms of eventual resolution of fluid, a significantly higher number of simple CSCR cases resolved with observation as compared to complex CSCR (43.5% and 16.3%). Number of interventions performed over the 12 months study period was significantly higher for complex CSCR as compared to simple CSCR. Time of SRF resolution was significantly shorter and fluid free period significantly longer in simple CSCR as compared to complex CSCR. Number of resolved cases was 67.4% in simple CSCR and 55.1% in complex CSCR at the final follow up. Visual acuity at the final follow up was better in simple CSCR as compared to complex CSCR [median 0.02 logarithm of minimum angle of resolution (logMAR) in simple CSCR and 0.1 logMAR in complex CSCR], but it did not reach statistical significance because of the ceiling effect. Similarly, SCT, CMT, number of persistent cases, number of cases with ORA and foveal involvement was not significantly higher in complex CSCR compared to simple CSCR at the final follow up. This demonstrates that the appropriate interventions for complex CSCR may lead to almost similar outcomes as simple CSCR.
Baseline characteristics of our study show lesser risk of complex CSCR in females. This is supported by literature which demonstrated less chances of diffuse RPE damage in females. 9 Recurrent episodes and persistent SRF produce a wider or multifocal RPE abnormality which is the very definition of complex CSCR. Persistent SRF also leads to ORA 10 and thus, complex CSCR cases had significantly higher recurrences, persistent SRF and ORA at the baseline.
On evaluation of change in parameters during the follow up, improvement in vision and reduction in the height of NSD or CMT was significant in simple as well as complex CSCR. Reduction in CMT was more pronounced in simple CSCR as compared to complex CSCR because of lower CMT in complex CSCR at the baseline. Number of eyes which experienced a recurrence during our period of follow up, was similar for simple and complex CSCR. However, complex CSCR had a much higher incidence of recurrent episodes at the presentation. Interestingly, eyes with lower CMT at the baseline were more prone to develop a recurrence during the follow up and eyes with complex CSCR had a lower CMT at the baseline. Thus, lower CMT or shallow NSD at presentation, in addition to extensive RPE changes, warrants a definitive intervention such as PDT, instead of observation.
Visual acuity at the baseline was demonstrated to be a significant predictive factor of final visual outcome in this study, as reported previously.11–13 Higher CMT at baseline was also associated with better final visual acuity in this study. Study by Singh et al. also showed that higher SRF height and CMT at baseline is associated with better visual recovery at 12 months follow up. 14
On Kaplan-Meier analysis for persistence probability of SRF with various treatment options, the probability followed the order: PDT < observation < focal laser. Superiority of PDT over focal laser in terms of SRF absorption has been well established in literature. 15 Some authors have even questioned if laser photocoagulation is warranted in the treatment of CSCR.4,16,17 In our study cohort, observation was mostly advised in eyes with simple CSCR and they fared well.
Interestingly, there were 4 eyes of 4 patients with complex CSCR that did not undergo PDT at the baseline visit. Two patients had no intervention at the baseline, third patient was prescribed oral eplerenone and fourth patient underwent micropulse laser followed by eplerenone. None of the eyes resolved with the above mentioned measures. First and third patients underwent PDT after 3 months of presentation and the second patient at 6 months, which led to a complete resolution. Fourth patient was on oral eplerenone for 9 months after undergoing micropulse laser at the baseline. He underwent PDT at 12 months and was noted to have a resolution at 14 months. This attests the need for a definitive approach towards treating complex CSCR that can help in a speedy resolution of the disease. Overall, we did observe a more aggressive approach being practiced in cases of complex CSCR as 49% eyes with complex CSCR were advised PDT at baseline, which probably led to similar visual outcomes as simple CSCR. Kaplan-Meier analysis showed the probability of persistence of fluid to be 50% for complex CSCR and 33% for simple CSCR in eyes which were only observed during the follow up. Thus, it is essential to differentiate simple or complex at baseline to prognosticate fluid resolution without treatment.
Use of objective criteria in classification of cases and use of imaging data at every follow up visit over the entire duration of follow up, forms the strength of our study. The two graders who classified the cases were masked. Limitations of our study include its retrospective nature. There were few cases treated with micropulse laser and eplerenone, which were mostly used as an adjunct rather than primary treatment, therefore, we could not comment on its efficacy. Because of the limited number of eyes treated with each treatment modality, we could not make a comparison or study the predictors of treatment outcome with respect to specific modalities. In our study, CRT was measured between ILM to RPE, however, few studies 18 considered CRT as the measurement between ILM and ellipsoid zone (excluding SRF). Considering the retrospective nature and multicentric study, there was no specific treatment protocol followed. We excluded the eyes with MNV and atypical CSCR and thus our conclusion does not apply to those cases.
In conclusion, our study reports anatomical and visual outcome among simple and complex CSCR groups along with the number of interventions and fluid-free interval over 12-months follow up. We also report predictors for visual outcome with baseline BCVA being the most significant predictor. This study helps to establish treatment guidelines using objective multimodal imaging based CSCR classification. Future prospective studies evaluating new classification based treatment approaches are warranted.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Jay Chhablani is a consultant for Allergan, OD-OS, Novartis and Biogen.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.