
Abstract
Purpose
To evaluate the microvascular changes in the macular and peripapillary area after intravitreal dexamethasone implant in diabetic macular edema (DME)
Material and Methods
We included 31 eyes of 31 patients treated with a single dose dexamethasone implant for DME. All subjects underwent swept-source optical coherence tomography (OCT) and OCT angiography imaging before (T0), and one month (T1), two months (T2), and four months (T4) after dexamethasone injection. The foveal avascular zone (FAZ) area of superficial and deep capillary plexus (SCP and DCP) was calculated by delineating the FAZ border using the measurement tool of the device. The vessel density (VD) of SCP and DCP and choriocapillaris (CC) in the macular and peripapillary area were automatically calculated.
Results
There was an insignificant reduction in FAZ area measurements of SCP after dexamethasone injection in DME patients (p = 0.846). The FAZ area of DCP were significantly smaller compared to T0 measurements at T1, T2, and T4 (p = 0.013, p = 0.031, and p = 0.029, respectively). The mean average parafoveal VD measurements were significantly decreased after dexamethasone injection in SCP and DCP (p = 0.004, p = 0.005). The peripapillary VD in retinal capillary plexuses and choriocapillaris showed no significant difference after dexamethasone injection.
Conclusion
Intravitreal dexamethasone leads to a significant FAZ area decrease in DCP with a reduction in parafoveal VD measurements. In addition, no significant VD changes were observed in the peripapillary area after dexamethasone. These findings indicate that dexamethasone may improve macular ischemia with no significant effects on peripapillary microvasculature in DME patients.
Keywords
Introduction
Diabetic macular edema (DME) is a common complication of diabetes and the main cause of blindness in the working-age population worldwide.1,2 DME has multifactorial and complex pathophysiology that includes mechanical and biochemical pathways triggered by hyperglycemia. The activation of pathways leads to oxidative stress and inflammatory cytokine release that disrupts the blood-retinal barrier. 3
Corticosteroids provide therapeutic benefits in DME with anti-inflammatory and anti-angiogenic properties. Steroids can stabilize the blood-retinal barrier and reduce vascular leakage in diabetic retinopathy. 4 Recent studies revealed that intravitreal dexamethasone improves peripheral retinal perfusion in DME patients using ultrawide-field fluorescein angiography (FA).
FA is the gold standard method to evaluate retinal vascular diseases in clinical practice, nevertheless, optical coherence tomography (OCT) angiography has emerged as a novel rapid imaging technique of retinal microvasculature. Vessel density (VD) and foveal avascular zone (FAZ) measurements are the commonly investigated OCT angiography parameters in diabetic retinopathy.5,6 There is also a wide-spreading interest in the role of OCT angiography in the disease course and treatment response.7,8
Several investigators have examined the macular microvascular changes after intravitreal injections in DME. Despite this interest, the studies have conflicting results and there is no agreement on the effect of intravitreal injections on macular microvasculature. A previous study demonstrated no significant macular microvascular changes after anti-vascular endothelial growth factor (VEGF) injections in DME. 9 On the contrary, a significant increase was shown in deep plexus VD measurements after both ranibizumab and dexamethasone. 10 Interestingly, another study demonstrated reduced perfusion density in the dexamethasone-treated group, whereas it did not change after ranibizumab treatment. 11
OCT angiography allows us to examine the microvascular structures of the peripapillary area as well as the macula. Previous work determined a significant decrease in VD measurements of the peripapillary area with increased diabetic retinopathy severity. 12 To the best of our knowledge, no study has yet addressed the peripapillary VD changes in the retinal capillary plexuses and choriocapillaris after dexamethasone treatment for DME. In this study, we aimed to assess and broaden current knowledge of the macular and peripapillary microvascular changes after dexamethasone injection for DME.
Material and methods
Subjects
This cross-sectional study was approved by the Hamidiye Ethics Committee of the University of Health Sciences and adhered to the tenets of the Declaration of Helsinki. All subjects were recruited from a tertiary referral center for retinal diseases. DME patients treated with a single dose 0.7 mg dexamethasone implant between February and November 2020 and who had macular and peripapillary OCT angiography imaging were enrolled in this retrospective study.
The inclusion criteria were, age 18 years or older with type 1 or 2 diabetes, diagnosis of non-proliferative diabetic retinopathy and DME, best-corrected visual acuity (BCVA) between 20/200 and 20/25, and central retinal thickness (CRT) between 300 to 600 µm. The exclusion criteria were as follows, proliferative diabetic retinopathy, history of panretinal photocoagulation (PRP), focal laser treatment and intravitreal corticosteroid injection, uncontrolled diabetes and hypertension, history of intravitreal anti-VEGF injection three months before dexamethasone injection, history of any intraocular surgery within the last six months, presence of glaucoma or ocular hypertension (intraocular pressure>25 mmHg) before and after dexamethasone injection, intraocular inflammation, coexisting retinal pathologies other than diabetic retinopathy, and optic nerve pathology, patients with a history of neurodegenerative diseases, eyes with ocular media opacities and poor quality images (signal strength (SS) <40).
Ocular examinations
All subjects underwent a comprehensive ophthalmologic examination at baseline (T0), and one month (T1), two months (T2), and four months (T4) after dexamethasone injection. This included assessment of BCVA using a Snellen chart, slit-lamp biomicroscopic evaluation, intraocular pressure measurement using Goldmann applanation tonometer, dilated fundus examination, OCT, and OCT angiography imaging using Topcon DRI Triton (Topcon Inc., Japan) swept-source OCT angiography.
SS-OCT angiography imaging
Central retinal thickness was assessed using the 3D (H) Macula + 5 LineCross protocol (Wide protocol) of the device. Macular and peripapillary microvasculature was evaluated using a 6 × 6 mm and 4.5 × 4.5 mm volume scan pattern centered on the fovea and optic disc, respectively. Superficial capillary plexus (SCP), deep capillary plexus (DCP), and choriocapillaris (CC) slabs were segmented automatically using the built-in software (IMAGEnet6, v1.23.15008, Basic License 10). All scans were reviewed to provide accurate segmentation and adequate image quality. The foveal avascular zone (FAZ) area of SCP and DCP were manually calculated by delineating the FAZ border using the measurement tool of the device by two independent, masked observers. The average of the readings of two observers’ measurements was used for FAZ area analysis. The interobserver intraclass correlation coefficient (ICC) was calculated using 30 randomly selected images to determine the reliability of the FAZ area measurements of SCP and DCP.
The VD of SCP, DCP, and CC was evaluated based on a modified ETDRS grid with a 1 mm diameter inner ring and 3 mm diameter outer ring in foveal (central) and parafoveal sectors (superior, temporal, inferior, nasal). Parafoveal vascular densities of each sector were averaged to obtain an average parafoveal VD. The peripapillary VD of each slab was also automatically analyzed in four peripapillary quadrants (superior, temporal, inferior, nasal).
Statistical analysis
Statistical analysis was done using the SPSS version 22.0 (SPSS Inc. Chicago, IL). The distribution and normality of the data were assessed using the Kolmogorov-Smirnov test Continuous variables were expressed as means and standard deviation (SD). The Snellen BCVA values were converted into the logarithm of the minimum angle of resolution (logMAR) for statistical analysis. The reliability of the FAZ measurements was evaluated by analyzing the interobserver intraclass correlation coefficient (ICC). The comparison of the swept-source OCT angiography measurements from baseline and T1, T2, and T4 was done using the Repeated measures analysis of variance with post hoc pairwise comparisons corrected by the Bonferroni method. The Greenhouse-Geisser correction was used in case of a lack of sphericity. A p-value <0.05 was considered statistically significant.
Results
Study population
Thirty-one eyes of 31 DME patients were included in the study group. There were 19 (61.3%) male and 12 (38.7%) female patients with a mean age of 60.87 ± 7.90 years. The demographic and clinical characteristics of the patients are presented in Table 1.
Baseline characteristics of DME patients treated with intravitreal dexamethasone implant.
BCVA and CRT changes
The mean BCVA was significantly improved after dexamethasone injection in DME patients (p < 0.001). The pairwise comparison with Bonferroni adjustment revealed that the mean BCVA improved from 0.63 ± 2.61 logMAR at T0 to 0.55 ± 2.98 logMAR at T1 (p = 0.271). The mean BCVA was significantly improved to 0.45 ± 0.25 logMAR and 4.99 ± 2.83 logMAR at T2 and T4 (p = 0.06, p = 0.03 respectively) compared to T0.
The mean CRT was 461.19 ± 119.70 µm at baseline. The CRT was significantly decreased to 279.55 ± 74.75 µm, 264.10 ± 72.66 µm and 296.58 ± 59.18 µm at T1, T2, and T4 compared to T0 respectively (p < 0.001). The pairwise comparison with Bonferroni adjustment revealed significant differences in CRT measurements between T0 and T2, T3, T4 (p < 0.001 for all comparisons).
Swept-source OCT angiography findings
Interobserver ICC value for FAZ area of SCP and DCP was 0.983 (95% confidence interval, 0.935–0.979) and 0.972 (95% confidence interval, 0.966–991), respectively.
There was an insignificant reduction in FAZ area measurements of SCP after dexamethasone injection in DME patients (p = 0.846). The FAZ area of DCP was significantly smaller compared to T0 at T1, T2, and T4. The post hoc comparisons revealed a significant difference in FAZ area of DCP between T0 and T1, T2, T4 (p = 0.013, p = 0.031, and p = 0.029, respectively).
The mean average parafoveal VD measurements were significantly changed after dexamethasone injection in SCP (p = 0.004). The pairwise comparison with Bonferroni adjustment showed significant differences between T0 and T1; T1 and T2; and T0 and T4 (p < 0.001 for all comparisons). Figure 1 shows the macular VD measurements at T0, T1, T2, and T4 of a representative case.

Macular optical coherence tomography angiography imaging of a representative case before (T0) and one month (T1), two months (T2), and four months (T4) after dexamethasone injection. Fundus photographs and the B-scan images with flow overlay before and after treatment (Panel A and B). Color-coded density maps and automatized vessel density measurements of the superficial capillary plexus (Panel C), deep capillary plexus (Panel D), and choriocapillaris (Panel E) before and after dexamethasone injection.
The mean VD of SCP in the superior and inferior quadrant was significantly changed after intravitreal dexamethasone (p = 0.033 and 0.035). The pairwise comparison with Bonferroni adjustment showed significant differences between T0 and T1; T0 and T4; and T1 and T4 (p = 0.014, p = 0.031, and p = 0.031 respectively) for the superior quadrant. The difference was significant between T1 and T2; and T1 and T4 (p = 0.021 and p = 0.037) for the inferior quadrant.
The mean average parafoveal VD measurements were also significantly changed after dexamethasone injection in DCP (p = 0.005). The pairwise comparison with Bonferroni adjustment showed significant differences between T0 and T1; T0 and T4 and T1 and T4 (p = 0.004, p = 0.013 and p = 0.010 respectively).
The mean VD of DCP in the superior and inferior parafoveal quadrant was significantly changed after intravitreal dexamethasone (p = 0.018 and 0.005). The pairwise comparison with Bonferroni adjustment showed significant differences between T0 and T1; T0 and T4; and T1 and T4 (p = 0.014, p = 0.035, and p = 0.016 respectively) for the superior quadrant. The difference was significant for T0 and T1, T2, T4 (p = 0.004, p = 0.017, and p = 0.002, respectively).
The mean VD did not show significant changes after dexamethasone injection in the CC layer (p > 0.05, for all comparisons). Table 2 summarizes the microvascular changes after dexamethasone injection in the macular area.
Foveal avascular zone (FAZ) area and macular vessel density measurements in the superficial capillary plexus (SCP), deep capillary plexus (DCP) and choriocapillaris (CC) at baseline (T0) and one month (T1), two months (T2), and four months (T4) after injection. .
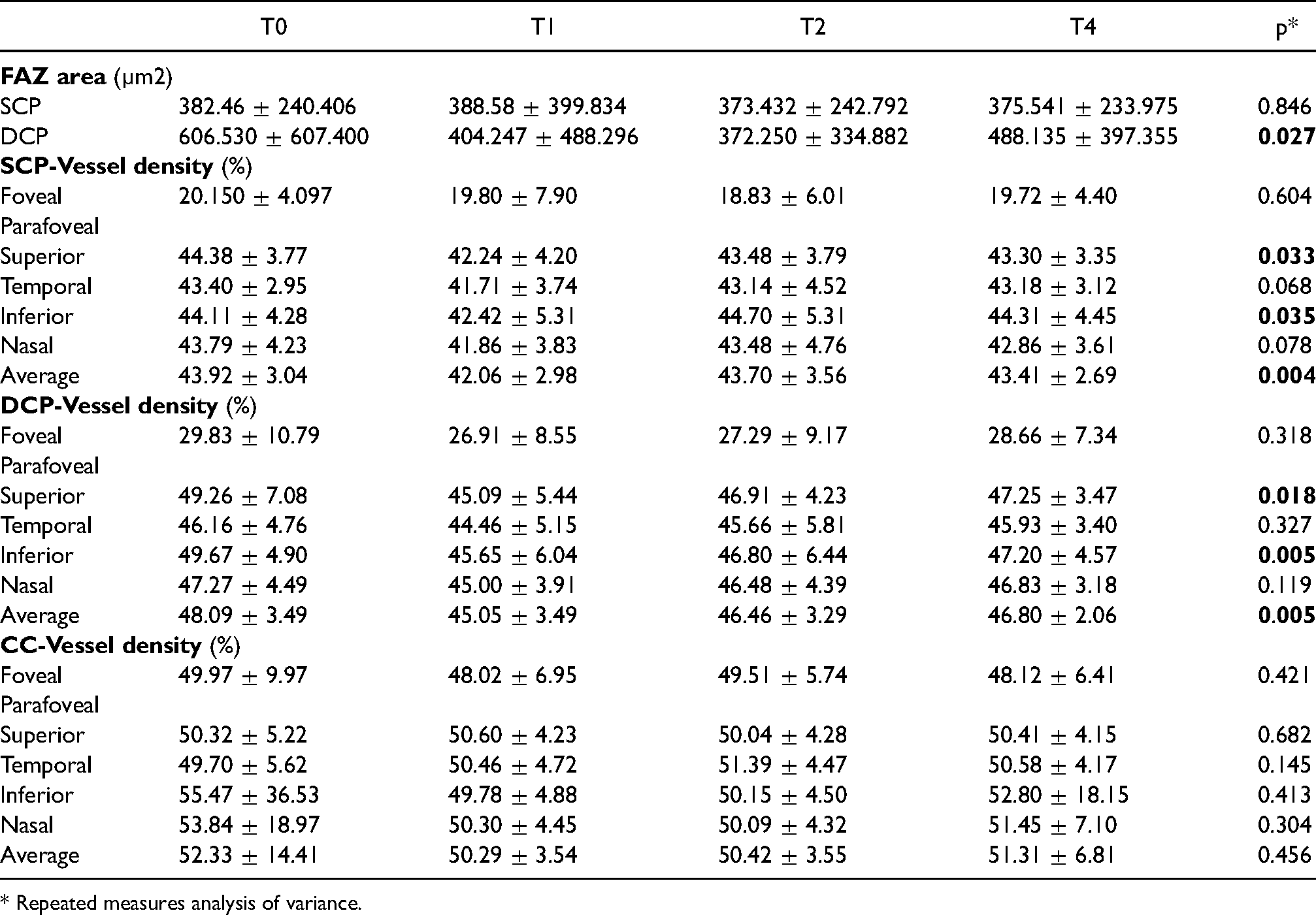
* Repeated measures analysis of variance.
The VD of retinal capillary plexuses and choriocapillaris in the peripapillary area showed no significant difference after dexamethasone injection (p > 0.05, for all comparisons). Table 3 illustrates the VD analysis of the SCP, DCP, and CC in four peripapillary quadrants.
The peripapillary vessel density (VD) analysis in the superficial capillary plexus (SCP), deep capillary plexus (DCP) and choriocapillaris (CC) before (T0) and one month (T1), two months (T2), and four months (T4) after dexamethasone injection.
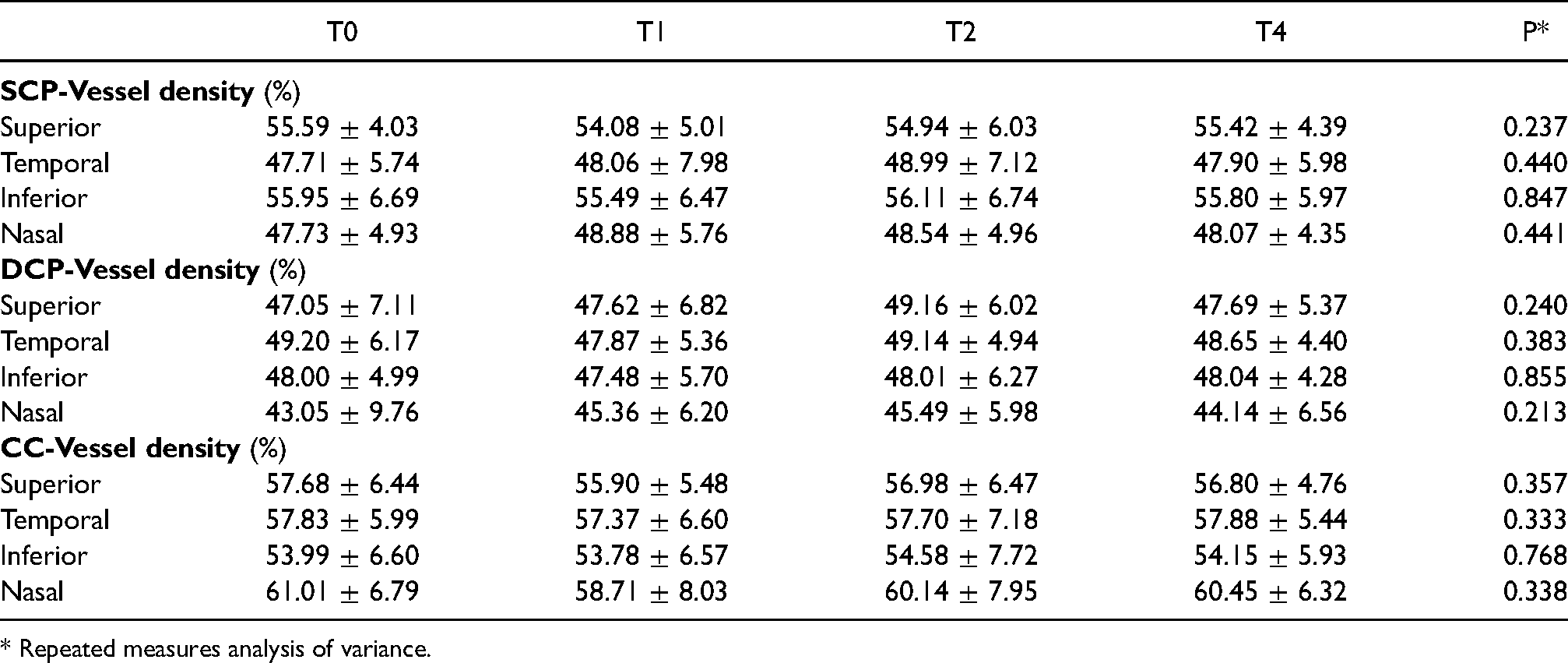
* Repeated measures analysis of variance.
Discussion
This study demonstrated a significant reduction in FAZ area of DCP and parafoveal VD measurements after dexamethasone injection compared to baseline. A significant visual and anatomic improvement was also achieved after a single dose of dexamethasone. In addition, no significant changes were found in peripapillary retinal and choroidal microvasculature after intravitreal dexamethasone. These findings indicate that dexamethasone may improve macular ischemia with no significant effects on peripapillary microvasculature in DME patients.
OCT angiography is attracting widespread interest in assessing retinal microvasculature due to its feasibility and non-invasiveness. It also allows accurate measurement of FAZ area and quantitative assessment of retinal and choroidal microcirculation in retinal vascular diseases. FAZ enlargement is regarded as an indicator for ischemia and may play a role in DME.13,14 Some authors suggested that the FAZ measurements could be a biomarker in the evolution of visual acuity and monitoring treatment response.15,16 In this study, we revealed smaller FAZ area measurements of retinal capillary plexuses after dexamethasone injection at any time point compared to baseline. The improvement in macular ischemia after dexamethasone was significant for DCP. In addition, the FAZ changes were accompanied by a decrease in macular thickness and visual recovery. Similar to our findings, Dastiridou et al. found smaller FAZ measurements after treatment in DME and implied that ischemia decreases with aflibercept treatment. 17 On the contrary, Busch, and co-workers did not demonstrate any significant changes in the retinal capillary plexuses and FAZ area after aflibercept despite an anatomic and visual improvement. 18
In addition to FAZ changes, a number of studies revealed that microvascular changes were observed even before the presence of any characteristic sign of diabetic retinal disease. 19 Dimitrova et al. showed reduced VD on SCP and DCP in diabetic patients without retinopathy compared to healthy eyes. 20 Aschauer et al. demonstrated a parallel change between capillary perfusion and inner retinal layer thickness in patients with type 2 diabetes. 21 Furthermore, a recent study showed progressive VD decrease with increasing DR severity. 22
Although VD reduction in diabetic patients has previously been well established, vascular density changes after DME and diabetic retinopathy treatment are still controversial. Mastropasqua et al. demonstrated a significant increase in parafoveal SCP and DCP density with no significant changes in CC density after aflibercept. 23 In another study, aflibercept was found to significantly reduce the central macular VD in DME. 17 Similar to their findings, we observed a reduction in parafoveal VD measurements of SCP and DCP after dexamethasone injection. Glacet-Bernard et al. analyzed the OCT angiography changes in retinal vein occlusion patients treated with dexamethasone. In that study, they also demonstrated that the mean VDs slightly decreased in the SCP and DCP after injection. 24 On the contrary, Toto et al. showed an insignificant increase in VD of SCP one month after dexamethasone injection with a decrease of retinal capillary non-perfused areas.25,26 The discrepancy between study outcomes could be attributed to the difference in intravitreal agents, treatment protocols, OCT angiography platforms, and lack of automatized data. In the present study, the macular VD changes in retinal capillary plexuses were prominent in superior and inferior parafoveal quadrants. In a previous study, Gadde et al. quantified the VD in circular and sectoral zones around the fovea and demonstrated sectoral differences. They claimed that VD analyses in the SCP and DCP need to be regional rather than an average of the whole image. 27 The VD differences in horizontal sectors might be related to the vascular anatomy of the retina and the topographic distribution of vessels.
Earlier studies demonstrated vessel caliber changes after intravitreal steroid therapy for DME. Wickremasinghe et al. found that DME-treated eyes with bevacizumab had no change in vascular diameter, while dexamethasone treated eyes had a significant decrease in venular diameter. 28 Kurt et al. stated that intravitreal and subtenon triamcinolone may lead to a significant constriction of retinal arteries and veins in DME. 29 According to a study evaluating the vascular changes in retinal vein occlusion, the deep retinal vessels become less telangiectatic after dexamethasone treatment. 30 Inflammation has been identified as a leading factor for vessel stiffness in diabetes.31,32 Dexamethasone may reduce vessel stiffness with its anti-inflammatory effect which promotes vascular remodeling as shown by histologic studies. 33 Previous evidence suggests that the VD reduction in this study might be related to steroid-induced vasoconstriction and remodeling of retinal vessels. On the other hand, the parafoveal VD decrease could be rather related to the mechanical effect of the large intraretinal cysts. We hypothesize that the retinal vascular narrowing can be a consequence of DME resolution and regression of cysts as well as vessel constriction. In addition, the resolution of edema could improve imaging and provide accurate segmentation and analysis. Further prospective studies are needed to clarify the mechanisms behind changes in macular microvasculature after dexamethasone in DME.
Contrary to parafoveal VD reduction in SCP and DCP, no significant difference was observed in peripapillary VD measurements of retinal capillary plexuses and choriocapillaris. Previous work has tended to focus on macular microvascular changes after treatment rather than the optic disc in DME. However, OCT angiography studies have revealed that both macular and peripapillary perfusion is affected in diabetic patients. Although the pathogenesis is different from diabetic retinopathy, Nicolai et al. demonstrated that intravitreal anti-VEGF may alter peripapillary VD measurements in patients with central retinal vein occlusion. 34 In accordance with our results, Toto et al. also reported no significant difference in optic disc vessel density. 26 The instrument and software were different in that study and the region of interest was thinner, not comprising the DCP. The topographic distribution of retinal capillaries makes DCP more susceptible to ischemic damage. 35 More recent evidence highlights that the DCP suffers more severe microvascular damage than the SCP with prominent vascular changes. 36 In this context, we particularly tried to evaluate both superficial and deep vascular plexus in the peripapillary area and observed that dexamethasone has no significant effect on peripapillary microvasculature.
Our study is limited by a limited number of DME patients and its retrospective design. FAZ area measurements were done manually due to the software of the device. However, the agreement between the two examiners was excellent. Segmentation artifacts may occur more frequently in eyes with retinal pathologies. 37 Automatic segmentation may not be reliable in the presence of macular edema. Therefore, we applied a manual correction to avoid image misinterpretation. Previous anti-VEGF usage is another concern, however, a recent work implied that the presence of washout period or not before enrollment does not affect VD measurements. 9 In the present study, we yet excluded the cases that underwent anti-VEGF injection preceding three months before dexamethasone injection.
In conclusion, we have presented that intravitreal dexamethasone led to a decrease in macular vascular density and a significant reduction in the FAZ area of retinal capillary plexuses. After dexamethasone injection, the VD changes in the peripapillary area were unremarkable in DME. These results suggest that dexamethasone therapy may improve macular ischemia with no inadvertent effects on peripapillary microcirculation. Larger scale longitudinal studies evaluating the microvascular changes after dexamethasone injection may aid determine the role of OCT angiography in treatment response.
Footnotes
Authors’ contribution
SO, SP, ZH: Data collection and analysis, CA, GE: Interpretation of the results, SO: Drafting manuscript, OA: Peer-review.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.