
Abstract
Purpose
To evaluate postoperative safety of femtosecond laser deep anterior lamellar keratoplasty performed with an innovative anvil profile in keratoconus patients.
Methods
This is a single-center, retrospective cohort study. We reviewed medical records of 89 keratoconus patients that underwent femtosecond laser deep anterior lamellar keratoplasty surgery (46 eyes) and manual deep anterior lamellar keratoplasty (47 eyes). Inclusion criteria required: age > 18 years old, best-corrected visual acuity < 0.3 LogMAR, continuous suture of the graft, postoperative immunomodulant regimen with dexamethasone 0.1% for 6 months and at least 12 months follow-up. Previous eye surgery, hydrops, and other ocular disease were excluded. The main outcome measures were postoperative events: rejections, persistent epithelial defects, and graft failures.
Results
During the follow-up (20 ± 6 months) graft rejection was diagnosed in 0 of femtosecond laser deep anterior lamellar keratoplasty versus 6 (17%) of manual deep anterior lamellar keratoplasty [p 0.027], persistent epithelial defect in 0 of femtosecond laser deep anterior lamellar keratoplasty versus in 4 (11%) of manual deep anterior lamellar keratoplasty [p 0.048] and graft failure occurred in 4 (11%) of manual deep anterior lamellar keratoplasty. The best-corrected visual acuity, after removal of sutures, was better in the femtosecond laser deep anterior lamellar keratoplasty group 0.09 ± 0.08 LogMAR versus 0.16 ± 0.13 LogMAR in manual deep anterior lamellar keratoplasty [p 0.035] group although refractive spherical equivalent and cylinder, topographic average keratometry and cylinder were similar.
Conclusions
Anvil-shaped femtosecond laser deep anterior lamellar keratoplasty in keratoconus surgery increases safety and readiness of recovery, decreasing the incidence of corneal rejection, epithelial defects, graft failures, and producing better best-corrected visual acuity after removal of sutures.
Keywords
Introduction
Keratoconus (KC) is a degenerative corneal ectasia causing corneal thinning and irregular astigmatism leading to critical visual impairment. Classically, KC has its onset during puberty, although childhood and adulthood cases have been described.1–3 Wide ranges are reported for incidence and prevalence, respectively, from 1 : 3,000 to 1 : 80,000 and from 1 : 375 to 1 : 2000, according to ethnic groups and setting of the studies.1,3–5 Although visual acuity can be frequently corrected by glasses or rigid/scleral customized contact lenses, corneal transplantation is the latest option in 10%–20% of KC patients suffering from corneal opacities or non-correctable visual acuity.6–8 Penetrating keratoplasty (PKP) shows promising visual outcomes even though there are several possible serious complications, essentially graft rejection and failure events, intraocular infections, and postoperative high astigmatism.9,10 Deep anterior lamellar keratoplasty (DALK) overcomes the sight-threatening endothelial complications, by preserving the patient's own endothelium, and offers a safer and less invasive extraocular procedure. 11
Newer Femtosecond laser technology increases keratoplasty surgery safety and reproducibility by performing adjustable and complementary shapes for donor and recipient corneal cuts. 12 Multiple corneal cut profiles have been described, such as top-hat, mushroom, Christmas tree, and zigzag, with the aim of achieving a more stable and predictable wound configuration.12–14 Recently, the anvil-shaped profile allowed a wide donor/host interface and a reduced volume of transplanted tissue compared to the manual procedure of the same diameter,13,14 sparing a wider part of host endothelium in the event of penetrating keratoplasty performed in a patient with healthy endothelial cells.
Few studies approximately compare femtosecond laser-assisted DALK (F-DALK) and manual trephination DALK (M-DALK) outcomes in KC surgery, therefore the purpose of the present study was to unveil the safety and, subsequently, the efficacy of anvil profiled F-DALK in KC patients.
Methods
This was a retrospective cohort study. We reviewed medical charts of KC patients who underwent DALK surgery at hospital “Dell’Angelo” (Mestre, Italy) from 1 January 2016 to 1 November 2019. Detailed informed consent was obtained from all patients, and all cases were treated according to the tenets of the Declaration of Helsinki.
Inclusion criteria required were the following: age < 18 years; availability of at least 12 months postoperative follow-up with complete recorded data; DALK surgery performed with the anvil-shaped profile or with manual trephination procedure, low best-corrected visual acuity (BCVA) < 0.3 logMar, visual impairing corneal opacity, continuous suture of the graft and prescribed postoperative immunomodulant therapy with topical dexamethasone 0.1% for 6 months. Eyes with histories of previous surgery or ocular diseases and corneal hydrops were excluded. A comprehensive ocular examination, best spectacle-corrected visual acuity, corneal topography, and endothelial cell count were performed at each visit. The main outcomes measures were incidence of rejections, epithelial defects, and graft failures. Secondary outcomes were rate of conversion to penetrating keratoplasty, suture revisions, need for intraocular pressure (IOP) lowering with medications, percentage of sutures removed at 1 year and at the last follow-up. For patients that had sutures removed within the follow-up, we analyzed BCVA, mean subjective spherical equivalent (SE)/cylinder, and mean topographic average (Avg) keratometry (K)/cylinder.
Surgical procedure
A single experienced anterior segment surgeon (CM) performed all the procedures with the intention of performing an Anwar big-bubble technique for stomal dissection. 15 When the big bubble was achieved, the procedure was recorded as a descemetic dissection (D-DALK); if the big bubble was not achieved, a manual deep lamellar dissection, recorded as predescemetic (PD-DALK), was performed. The donor cornea was sutured with a 16-running 10-0 nylon suture, subconjunctival cefuroxime (125 mg/mL), and betamethasone (4 mg/mL) were injected at the end of surgery.
Femtosecond laser trephination procedure
Donor preparation
The corneoscleral rim of the donor graft was secured to the artificial anterior chamber (Coronet, Network Medical Products Ltd.; Coronet House, Ripon, North Yorkshire, UK), and the intracameral pressure was maintained by a 10-mL syringe connected to the artificial chamber through a 3-way connector and was filled with BSS solution. The pressure was tested manually by the surgeon. The center of the cornea was localized with the aid of an eye ophthalmic gauge and marked with a surgical marking pen. After the applanation of the donor cornea, a graft cut was performed using a 150-kHz femtosecond laser (iFS150, Intralase FS Laser; Abbott Medical Optics, Santa Ana, CA, USA). An anvil cut profile was drawn on both the donor and the recipient's eyes. The anvil profile is a modification of the mushroom profile, in which the anterior side cut has a 135°-angle instead of 90°. This profile allows a wider area of graft-host junction contact, the inclination of the angle at 135° fits better and contrasts the internal ocular pressure that spontaneously tends to pull the graft out. This choice differs also from the zig-zag profile, where the angle of the sidecut is 30°, the amount of tissue involved in the donor-host scar is less and the suture is more inquisitive.
In the donor graft, the anterior diameter was 8.7 mm; the side cut started with an angle of 135° and reached the depth of 330 µm, intersecting the ring lamellar cut (energy 1.00). The ring lamellar cut was set at 300 µm in depth. The straight posterior-side cut diameter was 6.2 mm and posterior depth was set at 900 µm, to perform a full-depth cut.
Recipient preparation
The cuts were designed to be equal to the donor's cut diameters. The patient's corneal thickness was measured by anterior segment optical coherence tomography (OCT) (Visante, Carl Zeiss Meditec) pachymetry mapping. The posterior-side cut depth stopped 60 µm from the thinnest point measured at the 6.2 mm recipient diameter. After the laser-cut, a manual lamellar stromal dissection was performed with a crescent knife, followed by a 27-gauge air dissection cannula introduction into the deep stroma starting at the bottom of the trephination groove and advancing toward the center of the cornea. Air was injected progressively into the stroma, with the aim of achieving the formation of a big bubble. A peripheral paracentesis was performed to lower the IOP. Blunt-tipped scissors were used to divide the anterior stroma into four sections, which were then removed, exposing the Descemet layer.
Manual trephination procedure
The donor corneoscleral rim was prepared for the femtosecond laser procedure, but trephination was performed with Moira One Threpine of 8.50 mm diameter. In the recipient’s eye, the surgeon performed a partial-thickness trephination (350 – 450 mm, depending on the corneal thickness) of 8.50 mm diameter using a suction trephine. After the trephination, the first portion of the stroma was removed with a crescent knife. A 27G cannula mounted on a 5-mm syringe filled with air was used to achieve the bubble to separate Descemet's membrane from the stroma. Then an anterior chamber paracentesis was done to reduce the IOP. The bubble was opened with a diamond knife and a dispersive viscoelastic was introduced to separate the Descemet membrane from the stroma and to easily remove the stroma to bare the Descemet membrane with scissors.
Postoperative regimen
Postoperative medication included an association of netilmicin 0.3% and dexamethasone 0.1% eye drops 6 times daily for 15 days, followed by 4 times daily for 15 days. It continued during the second month with dexamethasone 0.1% 4 times daily. Dexamethasone 0.1% was tapered to 3 times daily during the third month and 2 times daily from the fourth to the sixth month. All patients were reviewed on postoperative days 1, 7, and 30. Follow-up visits were then scheduled every 3 months until sutures were removed.
Statistical analysis
Continuous data are shown as the mean ± standard deviation (SD). Categorical data are shown as n (%), where n is the number of available cases and the percentage denominator is the total number of available data points in that category. Visual acuities are expressed in LogMAR values. Normality in data was confirmed using the D’Agostino Pearson test. Two-tailed analyses were used throughout. Fisher's exact test was used to compare categorical data and t-test for continuous data. D’Agostino Pearson test, Fisher's exact test, and t-test were performed using GraphPad Prism version 7.00 for Windows, GraphPad Software, La Jolla CA, USA, www.graphpad.com.
Results
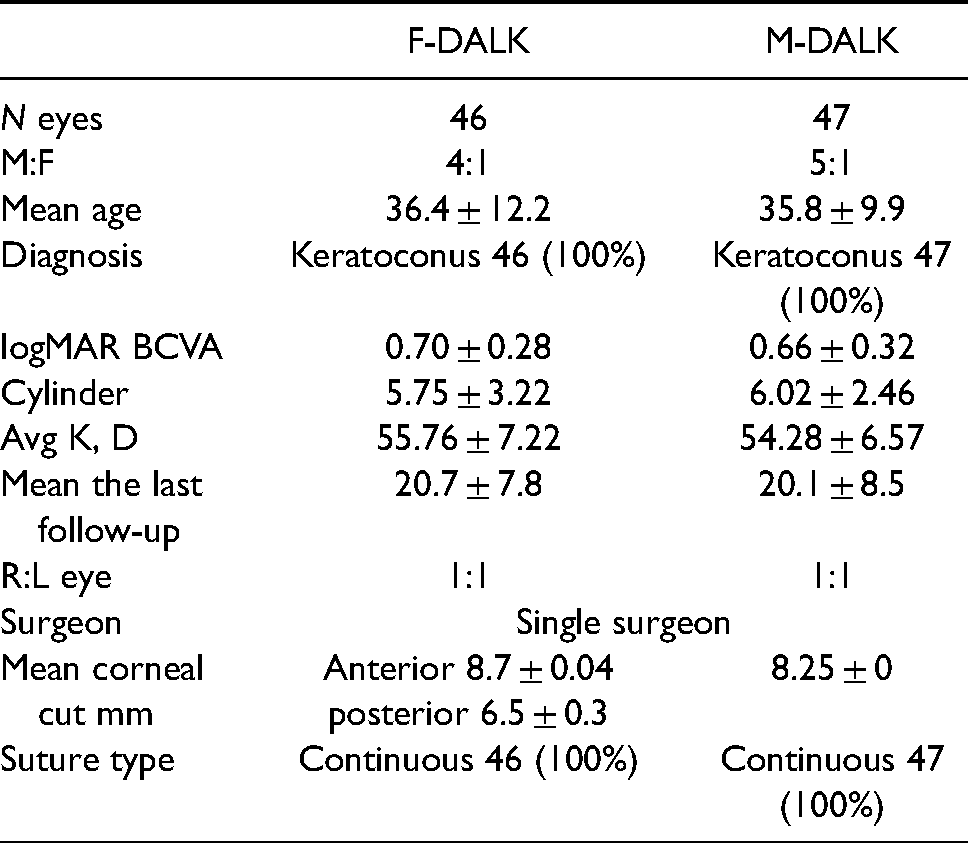
A total of 93 eyes of 89 patients were enrolled, (46 eyes anvil F-DALK; 47 eyes M-DALK). The mean follow-up period for the F-DALK group was 20.9
Demographics and preoperative data. ± Standard deviation; BCVA: best-corrected visual acuity; D: Diopters; DALK: deep anterior lamellar keratoplasty; A.F.: anvil profile femtosecond laser-assisted; M: manual; K: keratometry; M: male; F: female.
Graft rejection and failure rate
Graft stromal rejections were assessed in 6 (17%) patients in the M-DALK group while no patients had any rejection episode in the F-DALK group (p 0.027). Graft stromal rejections occurred after 6 months from surgery (exactly at 6th, 7th, 8th, 9th, 11th, 12th month after surgery). Endothelial cell count at last follow-up was not different among the two groups (2194
Persistent epithelial defect
Persistent epithelial defects during follow-up were assessed in 4 (11%) patients in the M-DALK group, while no events in F-DALK transplants were reported (p 0.048).
Suture management
Sutures required revision in 6 (16%) F-DALK and 5 (14%) M-DALK group cases, respectively. Sutures were removed within 12 months in 13 (34%) of F-DALK compared to 4 (11%) of M-DALK (p 0.027), hence at last follow-up, 24 (69%) of F-DALK patients were free from suture compared to 16 (50%) of M-DALK patients.
Conversion rate into PKP
Intraoperative perforation of Descemet membrane with PKP conversion occurred in 8 (17%) of F-DALK cases compared to 12 (25%) of M-DALK. Complications are summarized in Table 2.
Intraoperative and postoperative complications. In postoperative complication percentages, cases converted to PK are excluded. Statistical significance * is reported if p < 0.05 and was calculated with two-tailed Fischer’s exact test.
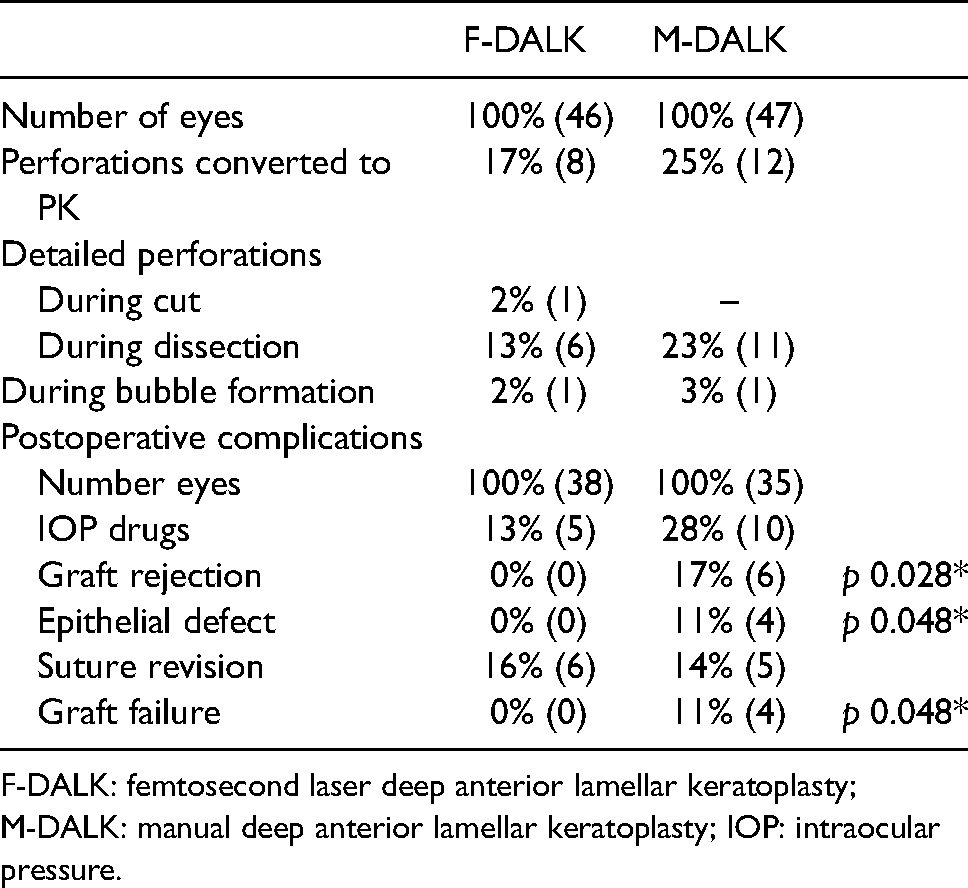
F-DALK: femtosecond laser deep anterior lamellar keratoplasty; M-DALK: manual deep anterior lamellar keratoplasty; IOP: intraocular pressure.
Visual outcomes
Patients free from sutures at the last follow-up presented not significantly different topographic and subjective refractive outcomes (Table 3), although BCVA in logMAR was 0.09 ± 0.08 in the F-DALK group and 0.16 ± 0.13 in the M-DALK group (p 0.035).
Outcomes of successful F-DALK and M-DALK: refraction, topography, and endothelial cell count shown are from patients that had sutures removed within the last follow-up. Fisher's exact test two-tailed was used for categorical data, unpaired t-test was used for continuous data, continuous data are presented as mean ± SD, statistical significance * is reported if p <0.05.
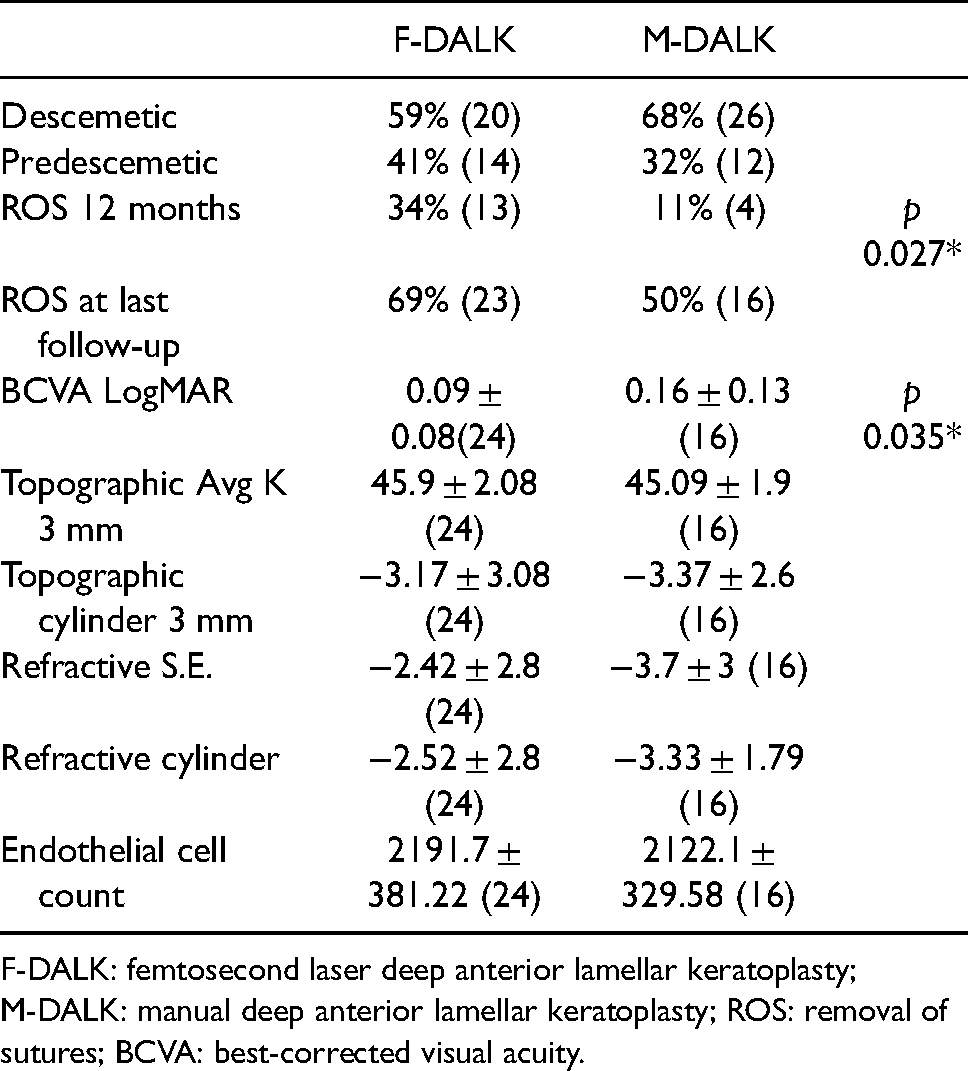
F-DALK: femtosecond laser deep anterior lamellar keratoplasty; M-DALK: manual deep anterior lamellar keratoplasty; ROS: removal of sutures; BCVA: best-corrected visual acuity.
Miscellaneous complications
IOP lowering medications were prescribed in 28% of M-DALK and 13% of F-DALK patients. There were no cases of Urrets Zavala Syndrome, double anterior chamber, infections nor need for air injection and glaucoma surgery.
Discussion
Anvil-shaped F-DALK is a safer and more effective procedure in KC patients compared to M-DAK. In fact, a critical reduction of graft rejection and failure, as well as a reduction in intra- and post-operative complications, have been shown in our patients. This safety advantage is also associated with a relatively better BCVA, with faster removal and easier management of sutures.
Although DALK spares a patient's endothelium, it is not free from epithelial and stromal rejection risk and the duration of postoperative immunomodulant therapy is crucial. For reference, 7 weeks of postoperative corticosteroid eye drop regimen used by Gonzalez et al., 16 who performed DALK in a group of 251 patients, presented rejection episodes within the first year of 20.2% in the M-DALK group versus 9.3% of F-DALK. The risk or relative risk (RR) of rejection was 2.7-fold greater with trephines. Instead, Salouti et al., 17 prescribing immunomodulant therapy for 12 months, had a 3% of rejection rate both in the M-DALK group and F-DALK group. In our study population, 6 months of tapered corticosteroid therapy was sufficient to prevent rejection in F-DALK but not in the M-DALK group, which had episodes of stromal rejection between the sixth and 12th postoperative month. The rejection rate of M-DALK (17%) was consistent with other studies with a similar postoperative regimen. 18 The absence of corneal graft rejection episodes in the F-DALK group may be partially explained by the reduced amount of rejectable tissue transplanted. In support of this hypothesis, it has been demonstrated that mushroom PKP decreases the rejection rate in high-risk corneal transplants. 19 Such lower rejection and failure rate also reduces the need and timing of immunomodulant therapy. Although rejection after DALK is easy to control, epithelial and stromal graft rejections can severely worsen visual outcomes in association with corneal graft neovascularization (CoNV) and lipids exudation. 20 In F-DALK, CoNV followed a specific pattern along with the anterior cup without penetrating the posterior side cut interface (Figure 1). Such neovessels completely regressed after suture removal, once inflammatory stimuli ceased.21,22 Contrarily, in M-DALK, CoNV easily overcomes host-graft junction leading to a central graft involvement. Since CoNV directly causes graft rejection, such neovessels behavior can further contribute to the different rejection incidence. 23
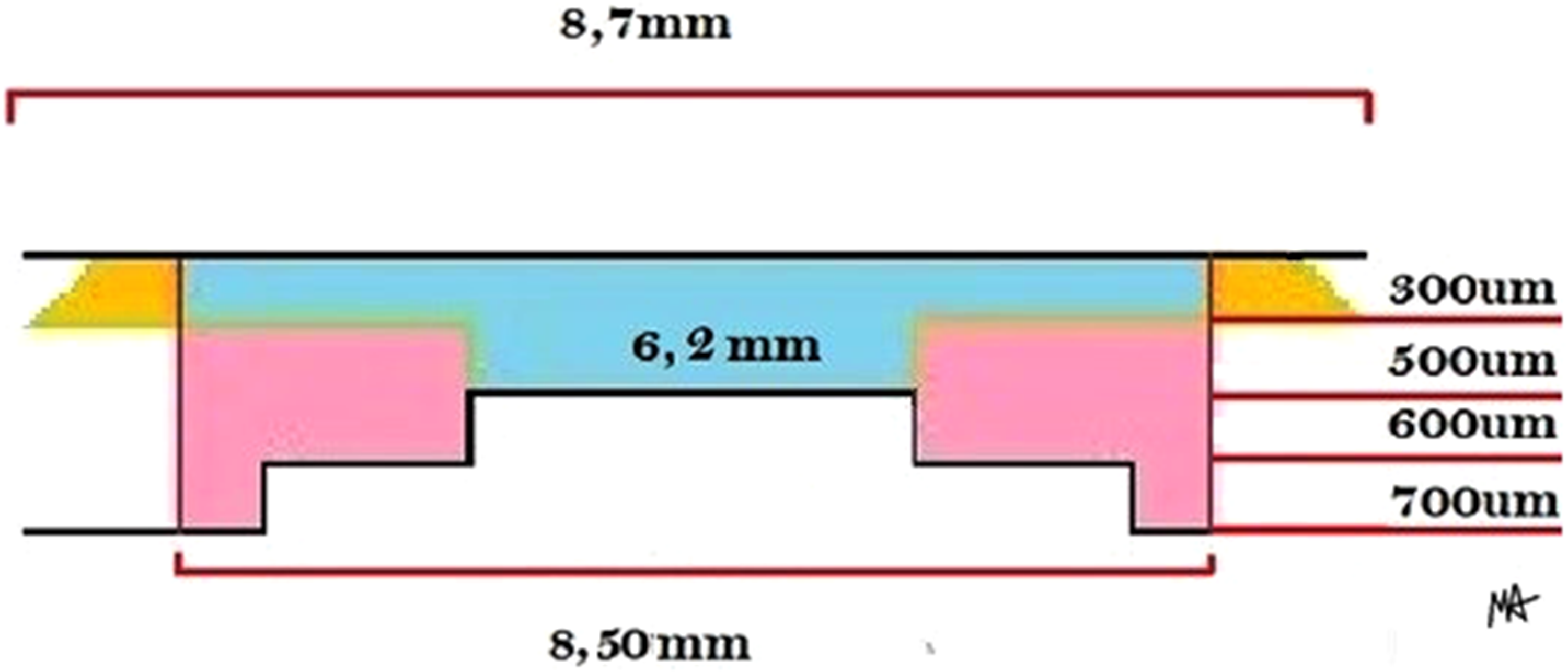
Donor cornea: F-DALK and M-DALK cut comparison. In azure stromal tissue was harvested both in A. F-DALK and M-DALK; in yellow tissue exclusive of A. F-DALK.In pink tissue exclusive of M-DALK. It shows how the tissue volume harvested in anvil-shaped F-DALK is consistently inferior to the M-DALK procedure.
Graft failure can be broadly defined as an irreversible change in the graft that prevents useful vision. 24 In this study, considering the high potential improvement in visual acuity of KC patients, we defined as graft failure every patient with a final BCVA value worse than 0.4 LogMAR due to pathological changes in the graft. In the M-DALK group, four graft failures occurred, two resulting from a persistent epithelial defect (diagnosed at fourth and at 20th month) and two due to persistent loss of stromal transparency 12 months after resolution of rejection.
F-DALK group shows a lower perforation rate, as reported for other similar cut patterns, such as mushroom, because of smaller bared Descemet membrane. Anvil profile harvests a large disc of the anterior corneal stroma, merging increased rigidity, structural stability, better refractive curvature, with decreased transplanted tissue volume, if compared to M-DALK (Figure 2). In our cases, one single perforation occurred during laser-cut, underling that peculiar caution should be paid during recipient cornea posterior side cut depth setting. Anterior segment optical coherence tomography (OCT) scan reveals high reflectivity of graft host interface wound in F-DALK anvil profiled laser-cut compared to M-DALK (Figure 3). Improved quality graft/host junction may be associated with decreased epithelial defects and stronger wound, as well as better visual and refractive outcomes.
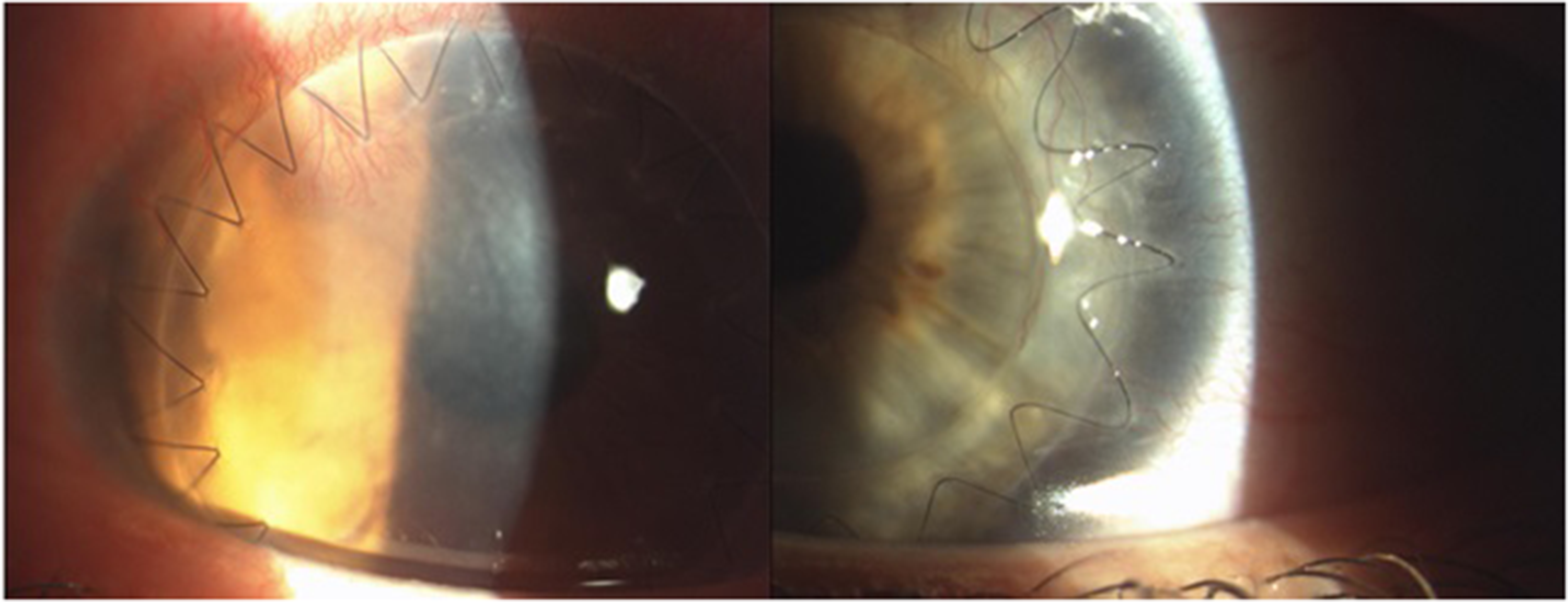
Corneal neovascularization: on the left, neovascularization in M-DALK penetrates in graft stroma contrary to F-DALK, on the right, with neovascularization limited to the host stroma below the anterior cup.
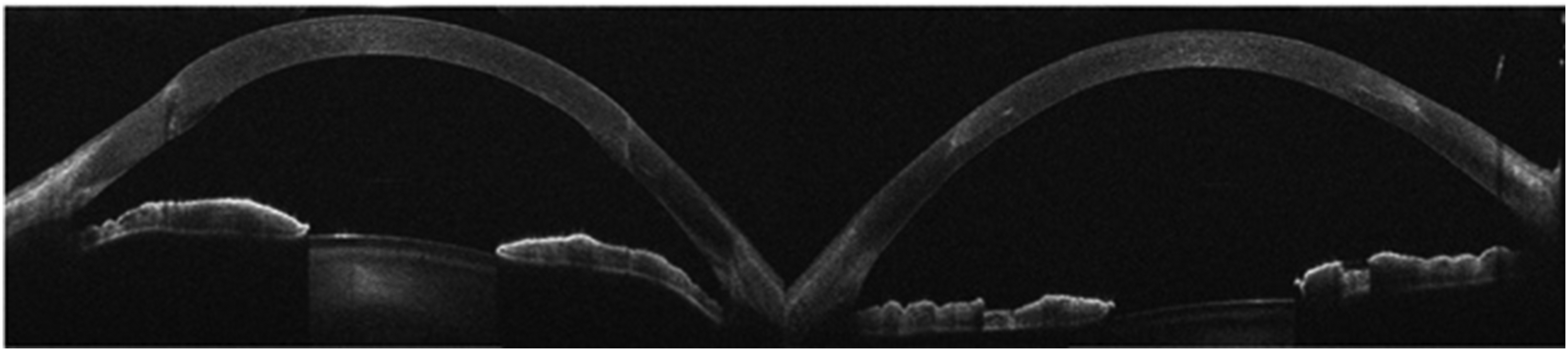
Anterior OCT scans after ROS: on the left anterior OCT scan from the M-DALK patient shows the inferior quality of donor/host junction compared to the F-DALK patient. Notice the smooth anterior junction and high reflectivity of the graft/host interface.
Time for removal of suture (ROS) is not strictly bound to the readiness of wound healing, but it was performed sooner in the F-DALK group, and this is commonly confirmed in literature. It must be considered that all the rejections occurred before ROS, thus, the earlier suture removal in F-DALK is a further hypothetical factor influencing the rejection rate. Not unexpectedly, the rate of suture revision was similar in both groups given that grafts were sutured in the same fashion by the same surgeon, and it was similar to literature values. 25 Once sutures were removed, the topographic and refractive analysis does not show any significant difference between laser-assisted and manual procedures, but BCVA was evidently increased in F-DALK. Central 6.2 mm graft clarity, without any CoNV or persistent epithelial defect episode, can explain such difference.
IOP medications were prescribed in case of higher IOP or in prophylactic association following the increase of corticosteroid postoperative regimen. Therefore, our M-DALK group has a slightly higher frequency of IOP lowering medications compared to literature.10,25
Our study has some limitations, as it has a retrospective design and relatively small sample sizes, as well as postoperative and intraoperative changes according to KC stages, were not evaluated.
Surely, further studies are required to better understand the role of such high technology in corneal surgery, but we may conclude that femtosecond laser-assisted DALK, with anvil-shaped corneal cuts, provide consistent improvements to safety, and partially efficacy, in corneal transplantation of KC patients.
Footnotes
Authors’ contribution
Conceived and designed the study: CM and MA. Analyzed the data: CM, ADZ, LC, and MA. Wrote the paper: CM, MA, ADZ, DG, LC, MC, and ER.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.