
Abstract
Purpose
To report the bacillary layer detachment on optical coherence tomography in exudative age-related macular degeneration.
Methods
Retrospective, observational cases
Case descriptions
Two cases of exudative age-related macular degeneration, one diagnosed as polypoidal choroidal vasculopathy following exudative age-related macular degeneration and other as wet age-related macular degeneration with choroidal neovascular membrane showed separation of myoid and ellipsoid zones of photoreceptor layer on optical coherence tomography. This is termed as BALAD. Other associated features noted were the presence of subretinal hyperreflective material, submacular hemorrhage and subretinal fluid. Both cases were treated with monthly intravitreal injections of Inj. Ranibizumab (0.5 mg/0.05 ml). Following 3 intravitreal injections at monthly intervals, reattachment of the bacillary layer detachment were noted in case 1 while the bacillary layer detachment persisted in case 2.
Conclusion
Multimodal imaging using optical coherence tomography in these cases revealed the separation of the bacillary layer following exudative age-related macular degeneration; a finding which is not routinely described in literature.
Introduction
The use of spectral-domain optical coherence tomography (OCT) has dramatically improved our understanding of the morphological changes in the retina and choroid following exudative age-related macular degeneration (eAMD). 1 The utility of OCT lies in identifying the location of the choroidal neovascular membrane (CNVM) as well as signs of activity like intraretinal fluid, subretinal fluid, pigment epithelial detachment and subretinal hyperreflective material (SHRM).1,2 The term bacillary layer was first reported in literature by Polyak in 1941. 3 Bacillary layer detachment (BALAD) was described as a separation of the retinal photoreceptor layer into the myoid inner layer and ellipsoid outer layer on OCT. This was first reported by Mehta et al. 4 in a case of toxoplasma retinochoroiditis. Similar occurrences of BALAD on OCT have been noted in a variety of choroidal inflammatory, infiltrative and vascular diseases.5–11 To the best of our knowledge, there is only one recent series of 14 patients with type 2 macular neovascularisation and BALAD on OCT. 12 In this paper, the authors describe two cases of eAMD showing BALAD on OCT; one due to polypoidal choroidal vasculopathy (PCV) and other due to wet AMD. This report of two new cases adds to a very small number of published cases of BALAD in eAMD.
Case descriptions
Case 1
A 58-year-old male, diagnosed with left eye PCV elsewhere visited the retina clinic for the second consultation. He complained of blurring of vision in the left eye for the past 7 days. He was being treated for type 2 diabetes mellitus, hypertension and hyperlipidemia. His past ocular history was unremarkable. His best-corrected visual acuity (BCVA) in the right eye was 6/6P, 6/6RS ( + 0.25 DS/ − 0.50 × 90) and left eye was 6/9P, 6/9RS ( + 0.25 DS/ − 1.25 × 100). Anterior segment examination of both eyes was within normal limits. Dilated fundus examination of the right eye showed a few extrafoveal drusens. The left eye fundus examination showed multiple pockets of serosanguinous pigment epithelial detachment (PED) along with a subretinal pigment epithelium (RPE) haemorrhage temporal to the macula. Fluorescein and indocyanine green angiography was done 5 days back at the previous consultation showed the polyp nasal to the fovea along with an abnormal branching vascular network. Spectral-domain OCT was performed using Spectralis OCT machine (Heidelberg Engineering, Heidelberg, Germany). Right eye OCT revealed a few extrafoveal drusens. The left eye OCT showed multi-lobulated PED with a type 1 choroidal neovascular membrane (CNV) with subretinal fluid and sub-RPE haemorrhage at the posterior pole. BALAD was identified as a separation of myoid and ellipsoid zones of the photoreceptor layer. A hyperreflective material with no back-shadowing, suggestive of SHRM was noted within the bacillary layer (Figure 1(A) and (B)). The choroidal thickness measured at the fovea was 392 µm. Based on the clinical and imaging findings, a clinical diagnosis of PCV following type 1 eAMD and BALAD was made. He was treated with 3-monthly doses of intravitreal Ranibizumab 0.5 mg/0.05 ml (Accentrix®, Novartis) in the left eye. After three doses of Inj. Ranibizumab, his BCVA in the left eye was 6/9, 6/9RS, respectively. OCT of the left eye showed a reduced height of the haemorrhagic PED and overlying SHRM and minimal subretinal fluid. Complete reattachment of the BALAD was noted (Figure 1(C) and (D)). The choroidal thickness measured at this visit was reduced to 305 µm. The patient was continued on treatment with monthly dosing of intravitreal Ranibizumab injections.
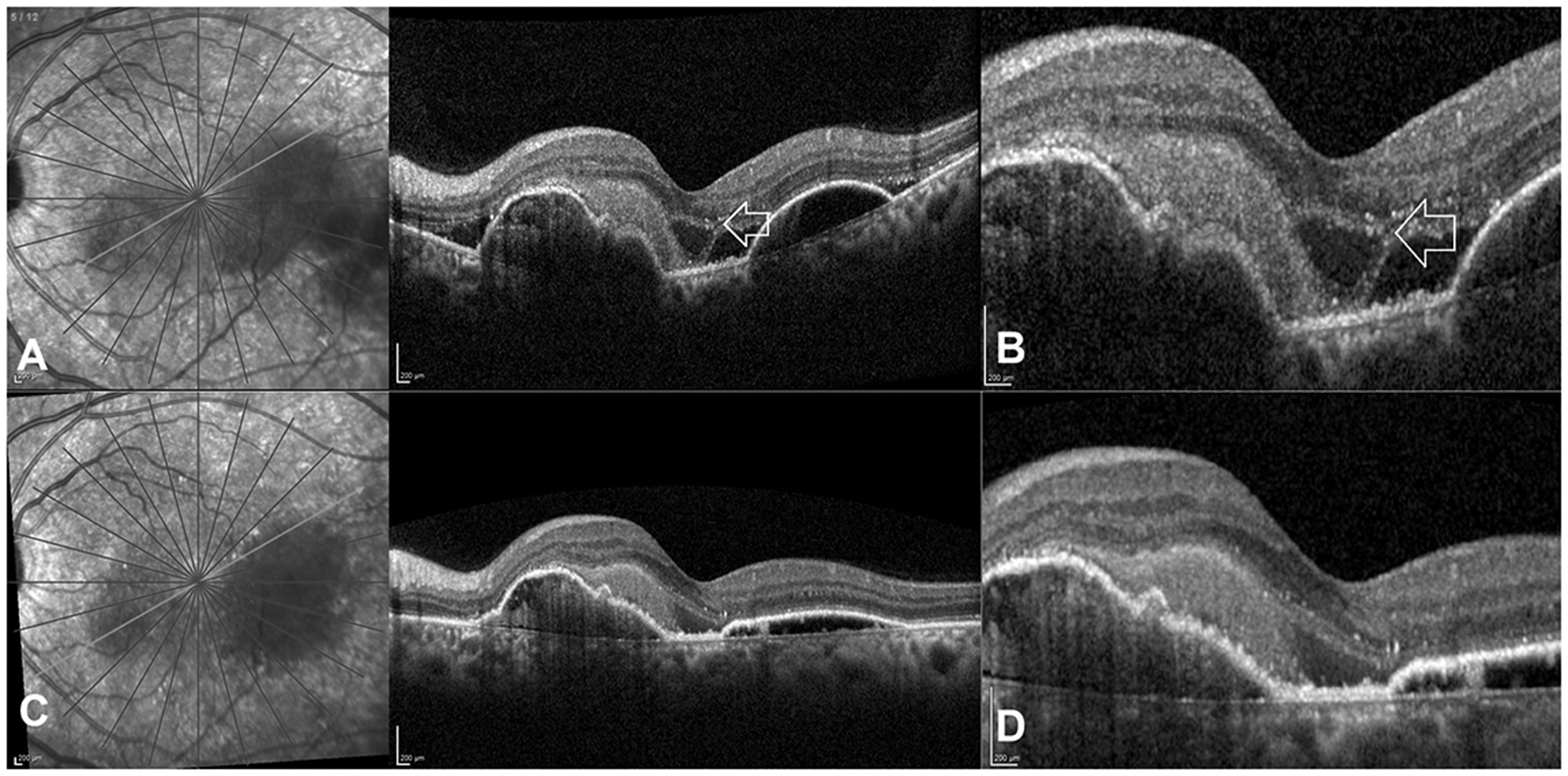
Pre and post-treatment optical coherence tomography imaging findings in case 1: (A), (B) Spectral-domain OCT of the left eye shows multi-lobulated pigment epithelial detachment with subretinal fluid and subretinal pigment epithelium haemorrhage at the posterior pole. Bacillary layer detachment (BALAD) was identified as a separation of myoid and ellipsoid zones of the photoreceptor layer (white arrow). A hyperreflective material with no back-shadowing, suggestive of subretinal hyperreflective material (SHRM) was noted within the bacillary layer. Zoomed-in image shows the BALAD. (C), (D) After three doses of Inj. Ranibizumab, OCT of the left eye showed a reduced height of the haemorrhagic pigment epithelial detachment and overlying SHRM and minimal subretinal fluid. Complete reattachment of the BALAD was noted.
Case 2
A 59-year-old diabetic male was referred to our retina clinic by a general ophthalmologist with a diagnosis of eAMD in his right eye. He complained about blurred vision and a central black spot in the right eye for the last 3 weeks. On examination, his best-corrected visual acuity in the right eye was 6/24P, 6/60RS and his left eye was 6/6, 6/6RS. He had the clear phakic lens in both eyes and his anterior segment findings were within normal limits. The right eye fundus examination showed few drusens and subretinal haemorrhage at the posterior pole. The left eye fundus showed a few deep yellow-coloured deposits suggestive of drusens. Spectral-domain OCT was done with spectralis machine which showed a flat irregular PED with a double-layer sign (type 1 CNV) and associated sub RPE haemorrhage and subretinal fluid. In addition, BALAD was identified as a separation of myoid and ellipsoid zones of the photoreceptor layer with an accumulation of SHRM within the detachment (Figure 2). The choroidal thickness measured at this visit was 295 µm. Fluorescein and indocyanine angiography were performed (Figure 3). The fluorescein angiography showed blocked choroidal fluorescence above the fovea suggestive of haemorrhage in the submacular area. A small area of neovascularization was noted above the fovea showing abnormal early hyper fluorescence with a lacy filling of the membrane and extensive fluorescein leakage in the later stage suggestive of an active classic pattern of CNV in the right eye. Transmitted hyper fluorescence was noted inferiorly due to window defects in the RPE. Indocyanine green angiography in the right eye showed a hypocyanescent area superior to the macula corresponding to the haemorrhage and a hot plaque type of hyper cyanescence clearly identifying a network of vessels in the neovascular tissue suggestive of a CNV. Based on the clinical, angiography and OCT imaging findings, a clinical diagnosis of an active classic CNV with submacular haemorrhage and BALAD was made in the right eye. He was treated with 3-monthly doses of intravitreal Ranibizumab 0.5 mg/0.05 ml (Accentrix®, Novartis) in the right eye. After three doses of Inj. Ranibizumab, his BCVA improved to 6/9, 6/6RS in the right eye, At the fourth and final follow-up visit, 3 months post-presentation, irregularity of PED was noted, with a reduction in the height of the subretinal haemorrhage and subretinal fluid. BALAD still persisted at this visit. The choroidal thickness measured at this visit reduced marginally to 277 µm. Poor anatomic response and persistence of BALAD were due to the presence of SHRM within the BALAD. The patient was advised to continue injections with intravitreal Ranibizumab; however, he was lost to further follow-up.
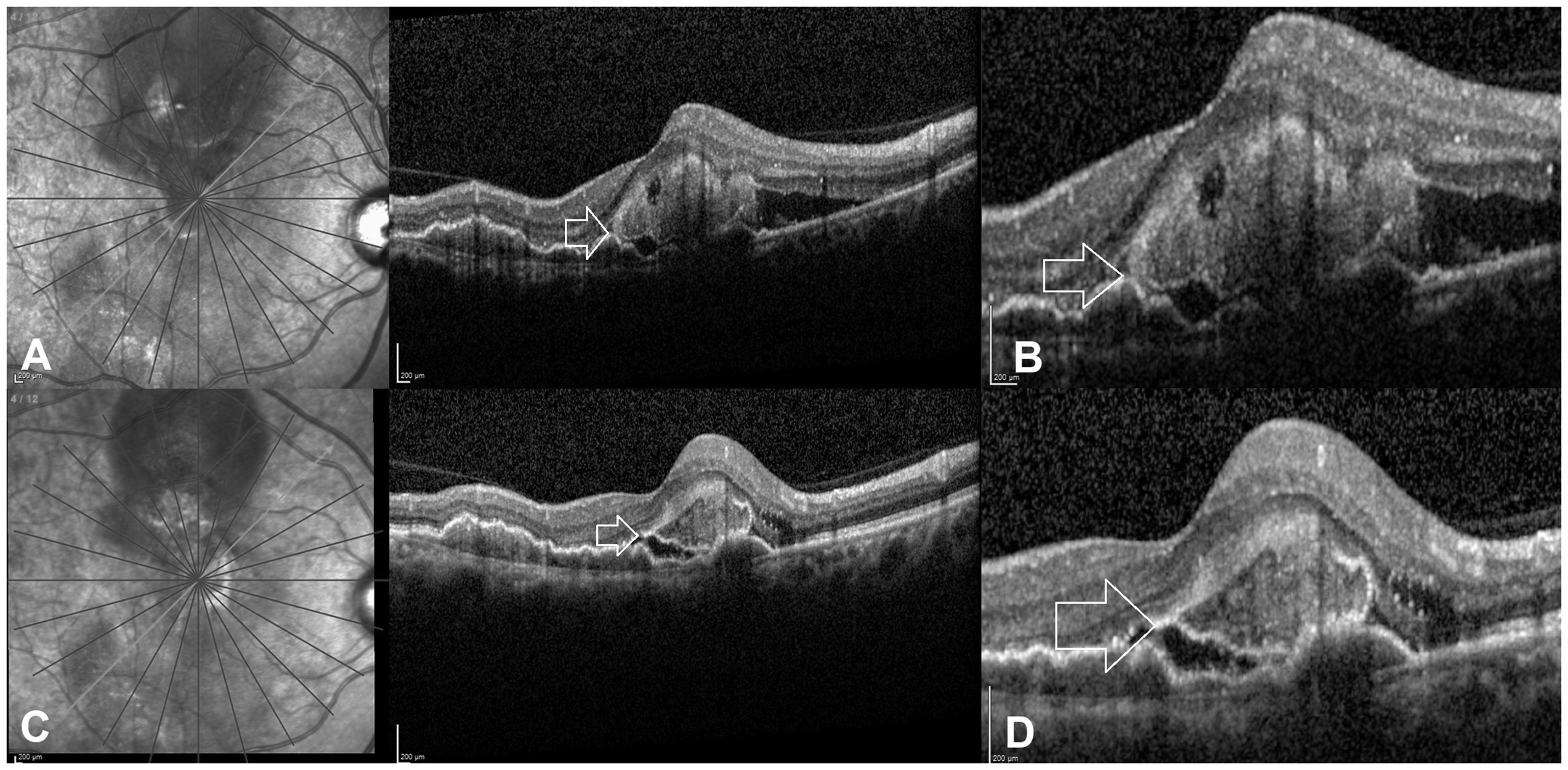
Pre- and post-treatment optical coherence tomography imaging findings in case 2: (A), (B) Spectral-domain OCT with spectralis machine shows a flat irregular pigment epithelial detachment (PED) with a double-layer sign and subretinal fluid. In addition, bacillary layer detachment (BALAD) was identified as a separation of myoid and ellipsoid zones of the photoreceptor layer with an accumulation of subretinal hyperreflective material (SHRM) within the detachment (white arrow). Zoomed-in image shows the BALAD. (C), (D) At the fourth and final follow-up visit, 3 months post-presentation, following three doses of intravitreal Inj. Ranibizumab, irregularity of PED was noted, with a reduction in the height of the intrabacillary SHRM and subretinal fluid. BALAD persisted at this visit (white arrow).
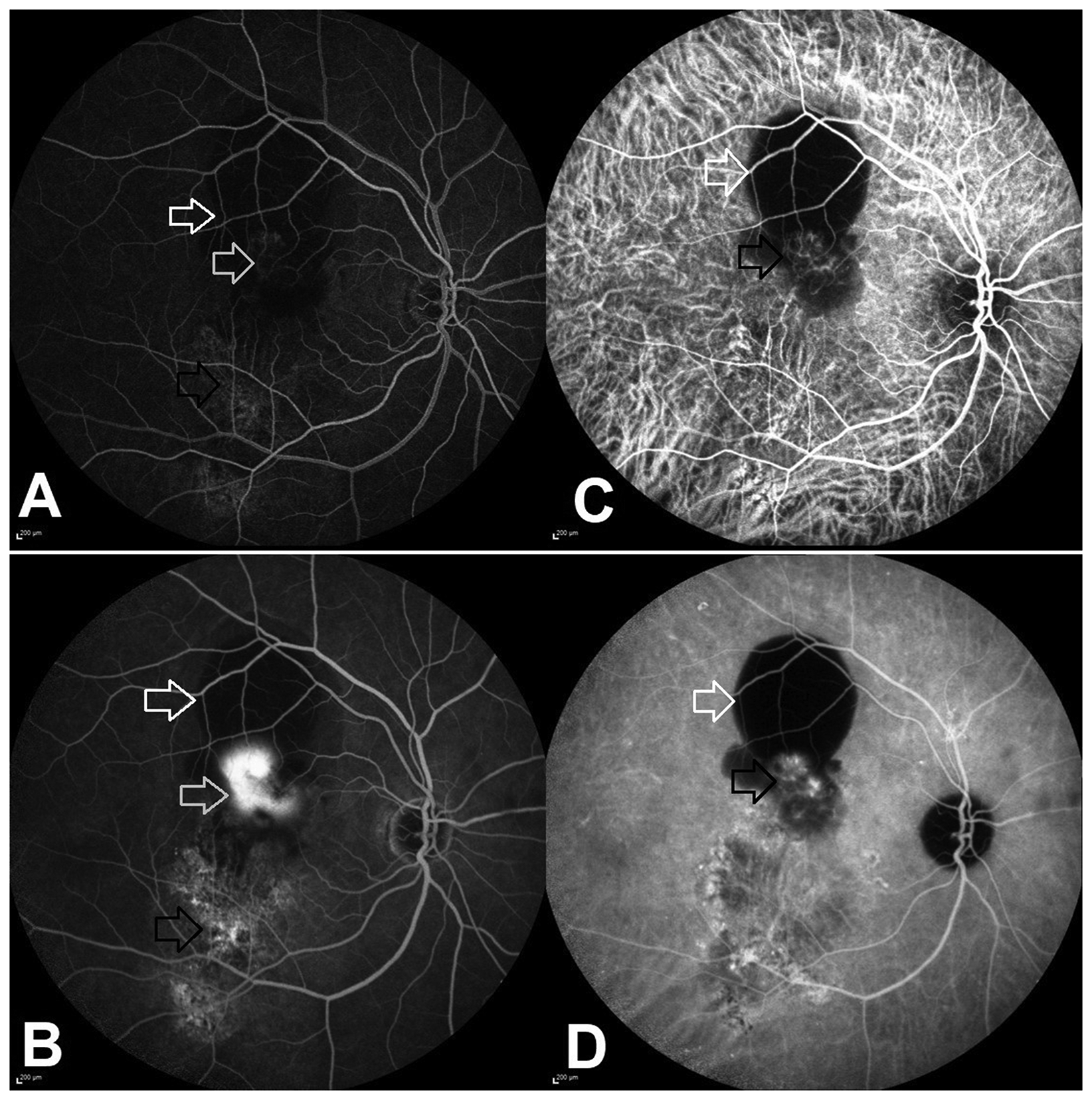
Fluorescein and indocyanine green angiography findings in case 2: (A), (B) Early and late phase fluorescein angiography images show blocked choroidal fluorescence above the fovea suggestive of haemorrhage (white arrow) in the submacular area. A small area of neovascularization is seen above the fovea showing abnormal early hyper fluorescence with a lacy filling of the membrane and extensive fluorescein leakage in the later stage suggestive of an active classic pattern of the choroidal neovascular membrane (grey arrow) in the right eye. Transmitted hyper fluorescence is noted inferiorly due to window defects in the retinal pigment epithelium (black arrow). (C), (D) Early and late phase indocyanine green angiography in the right eye show hypocyanescent area superior to the macula corresponding to the haemorrhage (white arrow) and a hot plaque type of hyper cyanescence clearly identifying a network of vessels in the neovascular tissue suggestive of a choroidal neovascular membrane (black arrow).
Discussion
The above described two cases highlight the presence of a rare finding of BALAD on OCT in patients with eAMD. These eyes with BALAD were associated with the presence of SHRM and subretinal or sub-RPE haemorrhage and an underlying type 1 CNVM.
The available literature on BALAD shows that this finding has been described in a variety of diseases like ocular toxoplasmosis and tuberculosis, Vogt-Koyanagi-Harada disease, acute posterior multifocal placoid pigment epitheliopathy, virus-induced acute idiopathic maculopathy, malignant conditions like bilateral diffuse uveal melanocytic proliferation, vascular conditions like peripapillary pachychoroid syndrome and even following blunt trauma with choroidal rupture.4–11,13 The similarity in all these diseases is the primary involvement of the choroid and RPE, either due to pachychoroid disease, choroidal inflammation, trauma or infiltration.
A recent paper by Jung et al. described 14 patients of type 2 macular neovascularisation with associated subretinal haemorrhage and BALAD. 12 In all the cases, the BALAD resolved following therapy with intravitreal anti-VEGF injections. In both our cases, there was type 1 macular neovascularisation. Finally, BALAD resolution was noted in only one of the two cases (case 1). Fajnkuchen et al. 14 reported a different type of serous retinal detachment on OCT in eyes with eAMD. They defined it as the ‘bridge arch-shaped’ serous retinal detachment, seen due to the fibrotic evolution of CNVM which could look similar to BALAD.
The mechanism of BALAD in eAMD could be either due to the underlying poor choroidal perfusion which leads to the stress and splitting of the photoreceptor (bacillary) layer or due to a rapid influx of exudative fluid into the potential space between the external limiting membrane and ellipsoid zone as suggested by Jung et al. 12 The photoreceptors receive their nutrients from the choriocapillaris; hence, in the acute stages, the compromised perfusion could lead to a splitting of the bacillary layer. Another possible explanation could be the accumulation of SHRM or haemorrhage within the bacillary space. The shearing force due to SHRM or haemorrhage causes the separation of the myoid and ellipsoid portions of the photoreceptor layer leading to BALAD. The BALAD resolves once the choroidal neovascular membrane regresses following therapy (as in case 1) or sometimes depends on the resolution of the SHRM or haemorrhage within the intrabacillary space (as in case 2).
To conclude, multimodal imaging of these cases revealed the separation of the bacillary layer in eAMD; a finding which is not routinely described in literature. This report provides an additional dimension in the pathogenesis of BALAD in eyes with eAMD.
Footnotes
Authors’ contributions
RV, JC – conceptualising the study, data acquisition, analysing the data, statistics and results, interpreting the findings, writing & reviewing the manuscript. NR, SAM – Data acquisition and analysing the data. NKY, AP – critically reviewing the manuscript.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Consent for publication
Obtained from the patient.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.