
Abstract
Purpose
To explore the risk factors for central retinal vein occlusion (CRVO) by comparing a large sample of patients with healthy controls.
Materials and Methods
Multi-center case-control study. The study group includes patients affected by central retinal vein occlusion, confirmed angiographically, aged 50 years old or above (Group A). The control group includes healthy subjects without an history of retinal vein occlusion (Group B). Outcome measures: age, gender, active smoking, presence of uncontrolled arterial hypertension (uHTN), presence of the following comorbidities: diabetes mellitus type II (DMII), chronic liver disease (CLD), chronic kidney disease (CKD), thyroid disease (TD), systemic lupus erythematosus (SLE), hyperhomocystenemia (HHcy), dyslipidemia (DLip), carotid artery disease (CAD), glaucoma, atrial fibrillation (AF), migraine headache (MH), chronic obstructive pulmonary disease (COPD), obstructive sleep apnea syndrome (OSAS), history of myocardial infarction (MI). Odds-ratios were calculated with logistic regression analysis.
Results
A total of 203 patients (Group A) and 339 controls (Group B). Statistically-significant differences were found for the following variables: age (OR: 1.109 [1.081–1.138], p < .001), active smoking (OR: 2.048 [1.210- 3.466], p < .008), DMII (OR: 4.533 [2.097–9.803], p < .001), HHcy (OR: 4.507 [2.477–10.001 ], p < .001), DLip (OR: 2.255 [1.352–3.762], p = .002), CAD (OR: 6.632 [2.944- 14.942], p < .001), glaucoma (OR: 4.656 [2.031–10.673], < .001), OSAS (OR: 1.744 [1.023–2.975], < .041), uHTN (OR: 3.656 [2.247–5.949], < .001). No statistically-significant differences were found for the other variables.
Conclusions
Older age, active smoking, as well as presence of DMII, HHcy, DLip, CAD, glaucoma, OSAS, and uHTN, all increase the risk for CRVO. A comprehensive assessment of patients with CRVO is paramount. Adequate control of all the aforementioned risk factors is likely of great significance in reducing the incidence of CRVO among the general population, and it likely plays an important role in improving the prognosis following the occlusive event.
Introduction
Retinal vein occlusion (RVO) is a thrombotic phenomenon affecting retinal veins. Its prevalence is estimated around 0.3% - 2.1% in subjects of 40 years of age or older. Incidence increases with age. However, even young subjects can be affected. Patients generally complain of sudden, monocular vision loss. The degree of visual compromise depends on the extent of affected retinal tissue. For this reason, a distinction is made between central and branch retinal vein occlusions, abbreviated respectively as CRVO or BRVO. On clinical examination, vessel tortuosity and retinal hemorrhages are noted along the distribution of the affected vessel. 1
Numerous risk factors are associated with RVO. They include increasing age, ethnicity, smoking, as well as ocular and systemic comorbidities. These comprise open-angle glaucoma, ocular hypertension, arterial hypertension, dyslipidemia, diabetes mellitus, metabolic syndrome, systemic lupus erythematosus, and obstructive sleep apnea. Elevated fasting levels of homocysteine, low levels of vitamin B12, factor V Leiden mutation, and anticardiolipin antibodies have also been shown to increase the risk. 4
This case-control study compares subjects affected by central retinal vein occlusion (CRVO) with healthy controls to estimate the odds-ratio for each of the following variables: age, gender, active smoking, presence of uncontrolled arterial hypertension (uHTN), presence of the following comorbidities: diabetes mellitus type II (DMII), chronic liver disease (CLD), chronic kidney disease (CKD), thyroid disease (TD), systemic lupus erythematosus (SLE), hyperhomocystenemia (HHcy), dyslipidemia (DLip), carotid artery disease (CAD), glaucoma, atrial fibrillation (AF), migraine, chronic obstructive pulmonary disease (COPD), obstructive sleep apnea syndrome (OSAS), history of myocardial infarction (MI).
Materials and methods
This is a multi-center retrospective case-control study that recruits patients affected by central retinal vein occlusion (Group A) and healthy controls (Group B). Subjects were recruited from two Italian hospitals, located in different areas of the peninsula: Policlinico Umberto I in Rome (central area of Italy) and Policlinico Sant’Orsola-Malpighi in Bologna (northern area of Italy). All patients signed written consent for their medical records to be used in this study. This study adheres to the tenets of Helsinki's declaration and was approved by the institutional ethics committee of La Sapienza University of Rome. Inclusion and exclusion criteria were as follows:
Inclusion criteria
− Diagnosis of central retinal vein occlusion confirmed with fluorescein angiography (FA) − Age 50 years or above − Subjects with incomplete or missing medical records were excluded
Exclusion criteria
Patients of the eye clinic without a diagnosis of retinal vein occlusion were recruited as controls. A comprehensive and detailed ocular and systemic history was obtained from each patient. Blood pressure was measured in all patients. Poor patient recall was moderated with the help of the patient's family physician.
Definitions
− Smoking: a patient is classified as being an active smoker if they have a recent history of 1 pack/year or more. Packs/year is calculated with the formula: number of cigarettes smoked in a day / 20 * number of years of smoking.
− Untreated blood hypertension (uHTN): a patient is classified as having uncontrolled hypertension if they have pressure values greater than 140mmHg or 90 mmHg for systolic and diastolic blood pressure respectively, on two or more different occasions, regardless of treatment.
− Type II diabetes mellitus (DMII): a patient is classified as being having diabetes mellitus type II if they have a diagnosis confirmed by an endocrinologist, regardless of their current HbA1c values, pharmacological therapy, or number of years with the condition.
− Systemic lupus erythematosus (SLE): a patient is classified as having SLE if they have a diagnosis confirmed by a rheumatologist, regardless of current disease activity or pharmacological therapy.
− Hyperhomocystenemia: a patient is classified as having hyperhomocystenemia if they have serum homocysteine values of 14 μmol/L or higher.
− Dyslipidemia: a patient is classified as having dyslipidemia if they have a total cholesterol of 240 mg/dL or greater, or LDL-C of 160 mg/dL or greater, or HDL-C of 40 mg/dL or lower, triglycerides of 200 mg/dL or greater, or if they are taking lipid-lowering medications, regardless of the etiology.
− Carotid artery disease (CAD): a patient is classified as having CAD if they have a carotid stenosis of 50% or greater in either carotid confirmed by ultrasonography.
− Chronic kidney disease (CKD): a patient is classified as having CKD if they have either kidney damage or a glomerular filtration rate (GFR) of 60 mL/min/1.73m2 or less for at least 3 months. Kidney damage is defined as pathologic abnormalities or markers of damage, including abnormalities in blood or urine tests or imaging studies.
− Chronic liver disease (CLD): a patient is defined as having CLD if they have liver failure lasting greater than 26 weeks, as confirmed by an hepatologist by a combination of lab tests (elevated AST/ALT, elevated bilirubin, or low platelet count <150 K), imaging studies, and biopsy.
− Glaucoma: a patient is classified as having glaucoma if they have a diagnosis of glaucomatous optic neuropathy confirmed by an ophthalmologist, regardless of glaucoma type, etiology, pharmacological therapy, or intraocular pressure values.
− Atrial fibrillation (AF): a patient is classified as having AF if they have a diagnosis confirmed by a cardiologist, regardless of treatment.
− History of migraine headache (MH): a patient is classified as suffering from MH if they experience at least 2 episodes a month.
− History of myocardial infarction (MI): a patient is classified as having a positive history for MI if they had at least one episode in their lifetime, regardless of MI type or severity.
− Chronic obstructive pulmonary disease (COPD): a patient is classified as having a COPD if they have a diagnosis confirmed by a pulmonologist, regardless of etiology, disease duration, pharmacological therapy, and severity.
− Thyroid disease: a patient is classified as having thyroid disease if they have an history for any chronic condition or state affecting thyroid function, regardless of therapy. Examples include Grave's disease, toxic multinodular goiter, toxic adenoma, Hashimoto's thyroiditis, or post-thyroidectomy or post-ablation state.
− Obstructive sleep apnea syndrome (OSAS): a patient is defined as having OSAS if they have an apnea-hypopnea index (AHI) >5 on polysomnography, along with excessive daytime somnolence. Alternatively, if they record at least 15 apneas or hypopneas lasting more than 10 s per hour on polysomnography.
Statistical analysis
Logistic regression analysis was used to estimate odds-ratio for each variable. Statistical significance was set at p < 0.05 and was tested using the Wald test. The statistical analysis and charts were generated with JASP v. 0.14.1.
Results
The total number of recruited subjects is 542. The study group (Group A) includes 203 patients (47.29% males and 52.71% females), while the control group (Group B) includes 339 subjects (51.03% males and 48.97% females).
Mean age was compared between the two groups (Figure 1). It was found that the study group had a statistically-significant higher mean age, as compared to the control group (68.16 ± 9.013 years in Group A vs 55.64 ± 11.77 in Group B) (p < .001 Welch's t-test).
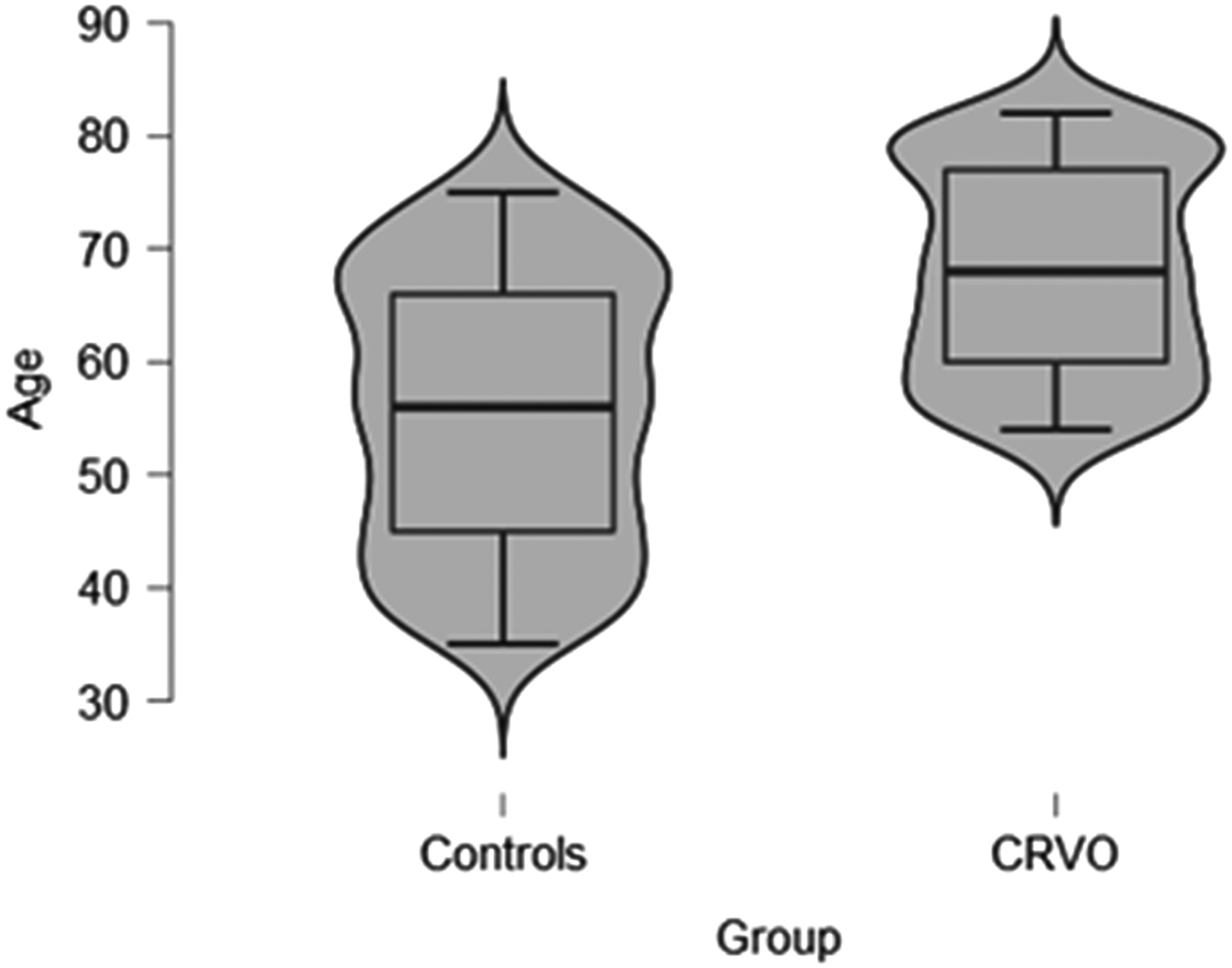
Age distribution in both groups.
Figure 2 shows no statistically-significant differences between groups in terms of gender composition (p = 0.399, Chi-square test).
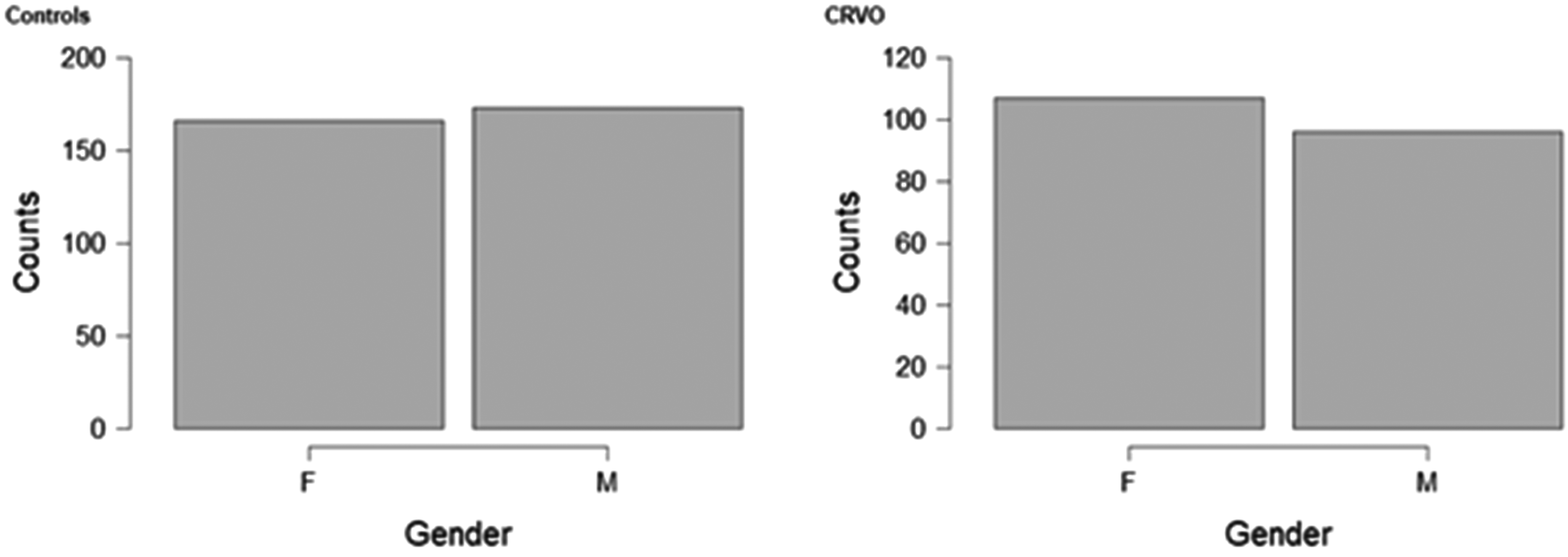
Gender distribution in both groups.
The percentage of smokers in both groups was significantly different (Figure 3). In fact, 41.37% of subjects in Group A were active smokers, as compared to 21.24% in Group B (p < .001 Chi-square test).
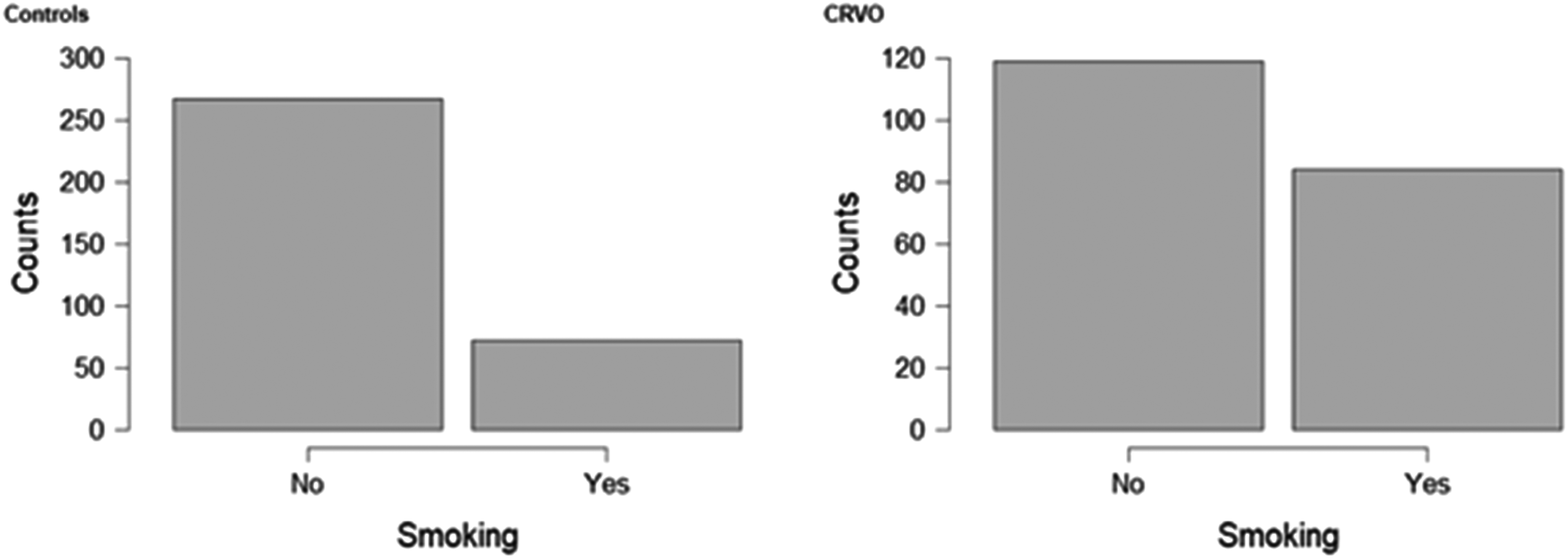
Distribution of active smokers.
The percentage of subjects with uncontrolled blood hypertension (uHTN) was different between groups (Figure 4). In Group A, 65.02% of subjects had blood pressure values (either systolic or diastolic) above the recommended values. This is in contrast with 28.02% of subjects in Group B (p < .001 with the Chi-square test).
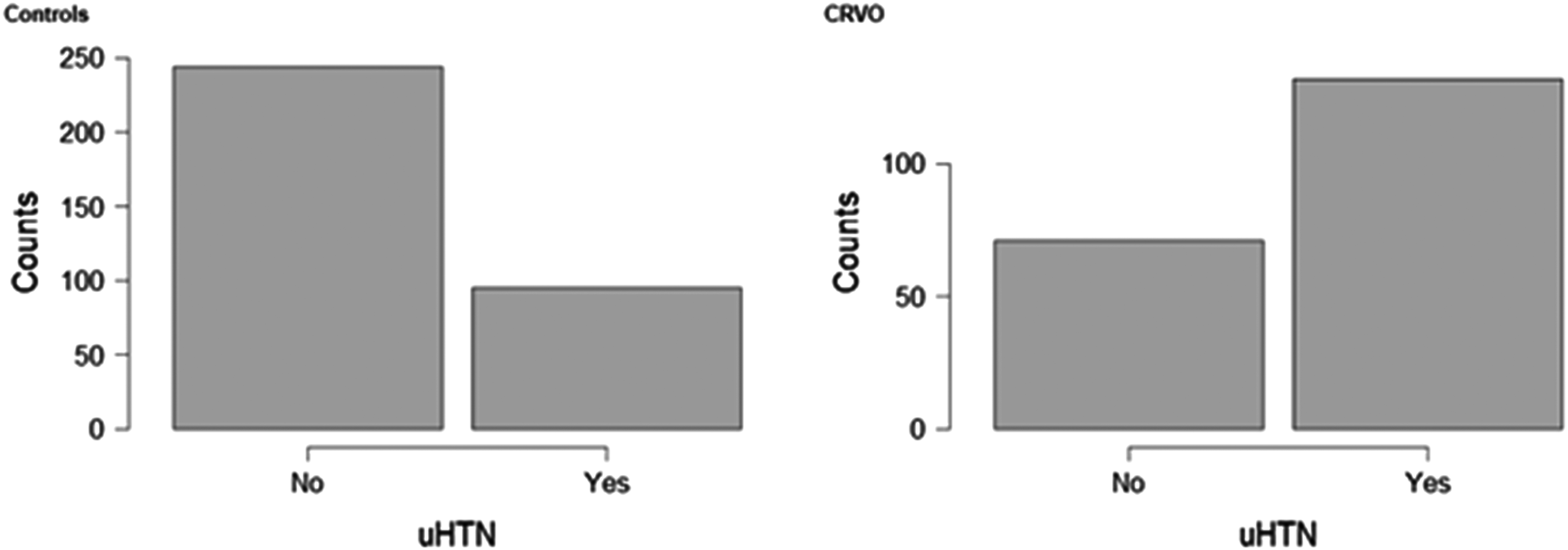
Distribution of subjects with uncontrolled arterial hypertension (uHTN) in both groups.
The comparison of the percentage of subjects with glaucoma yielded statistically-significant results (Figure 5). In fact, 19.21% of subjects in Group A had a diagnosis of glaucoma (any type), as compared to 6.19% of subjects in Group B (p < .001 with the Chi-square test).
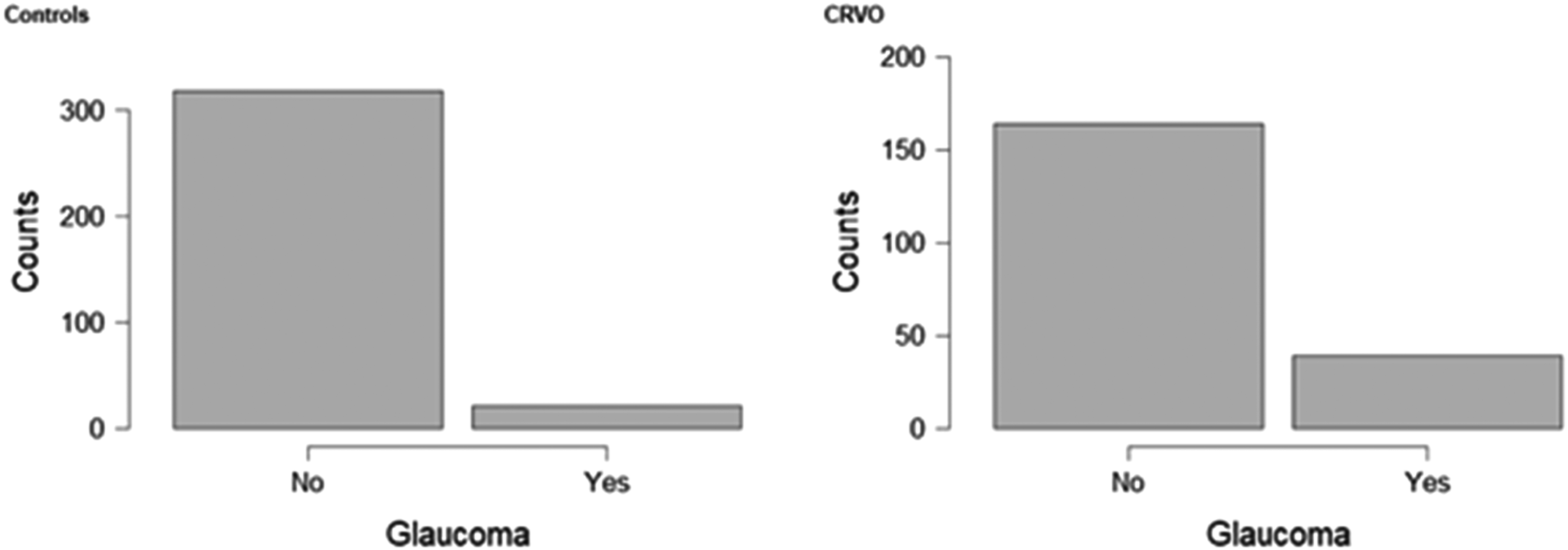
Distribution of subjects with glaucoma in both groups.
In the study group, 43.35% of subjects had a diagnosis of dyslipidemia (DLip), as compared to 28.02% of subjects in the control group (Figure 6) (p < .001 with the Chi-square test).
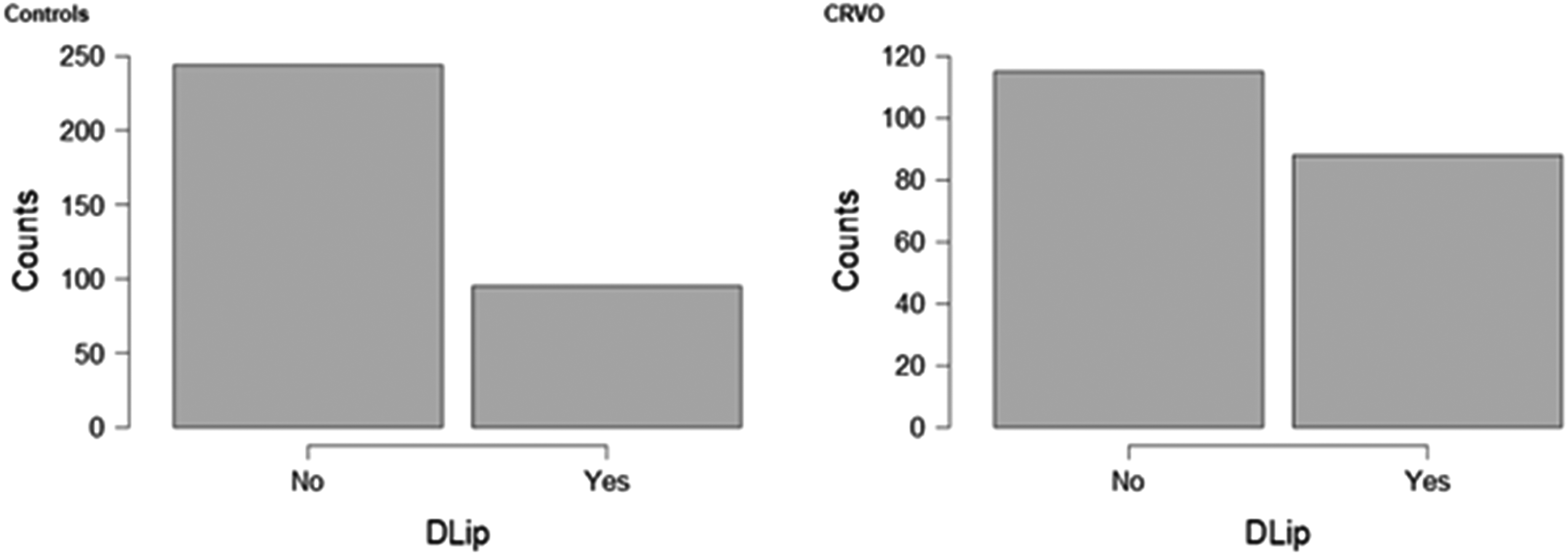
Distribution of subjects with dyslipidemia (DLip) in both groups.
The study group reported a prevalence for chronic kidney disease (CKD) of 8.37%, as compared to 3.25% in the control group (p = .009 with the Chi-square test) (Figure 7).
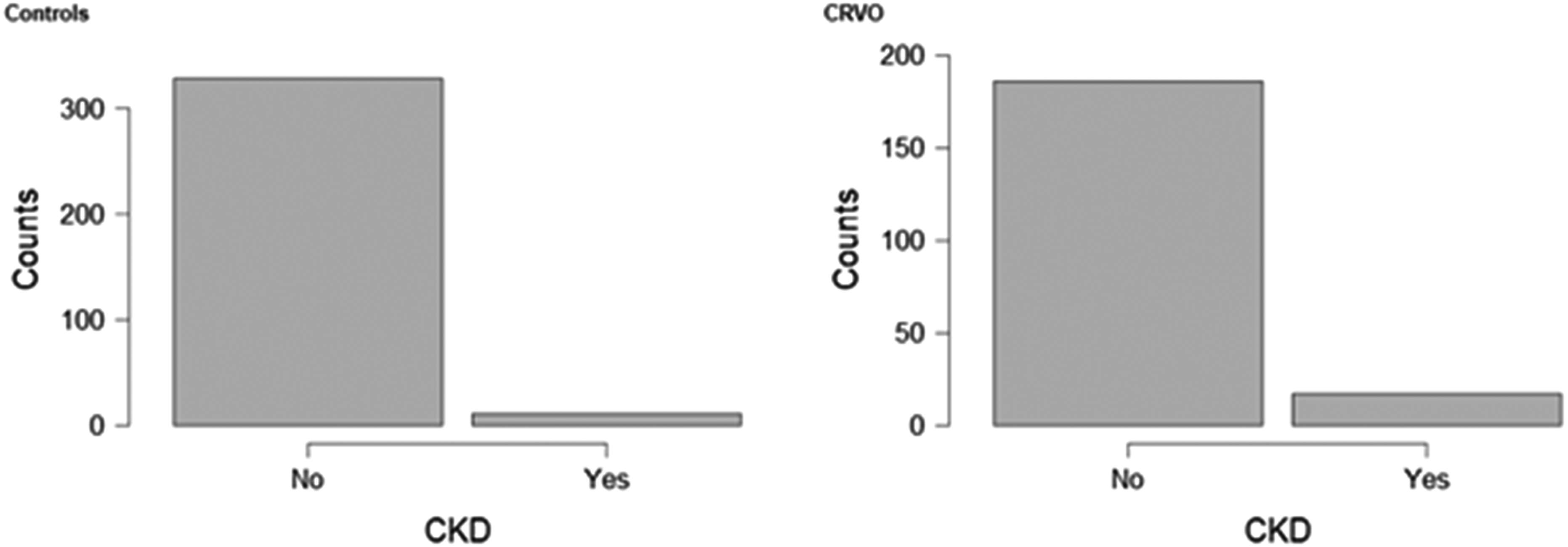
Distribution of subjects with chronic kidney disease (CKD) in both groups.
The study group reported a prevalence for carotid artery disease (CAD) of 22.16%, which significantly differs from 6.20% in the control group (p = .001 with the Chi-square test) (Figure 8).
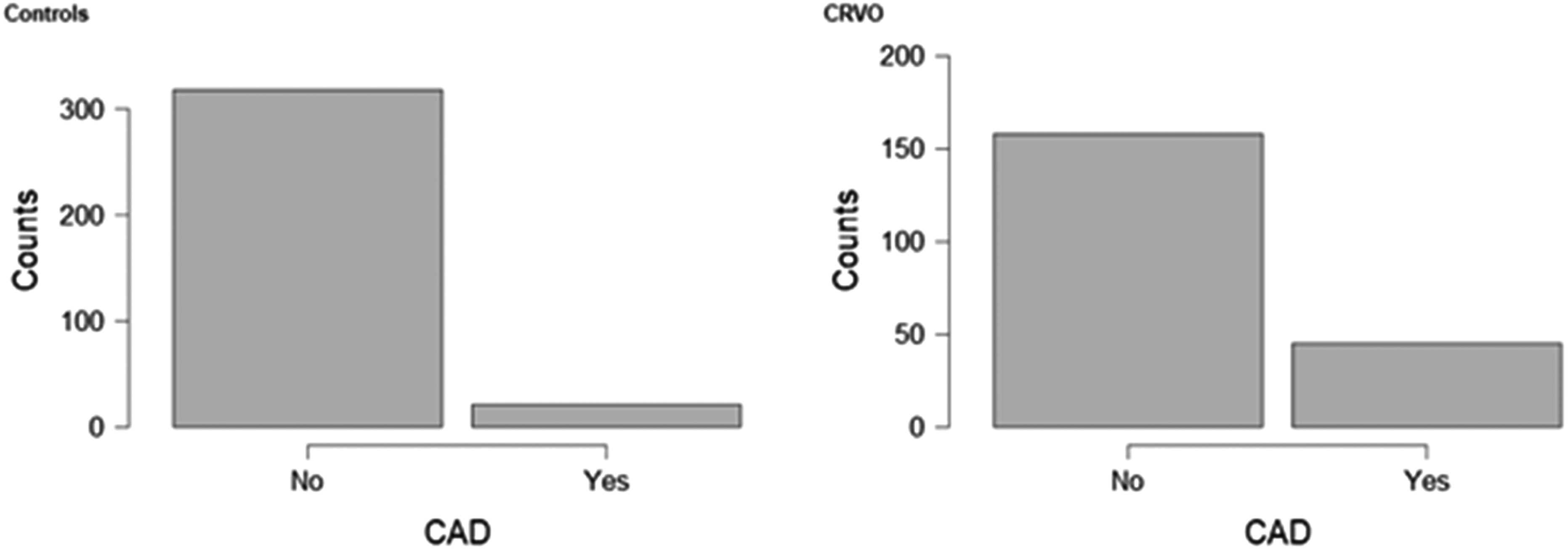
Distribution of subjects with carotid artery disease (CAD) in both groups.
The study group reported a prevalence for hyperhomocystenemia (HHcy) of 28.08%, which significantly differs from 6.20% in the control group (p = .001 with the Chi-square test) (Figure 9).
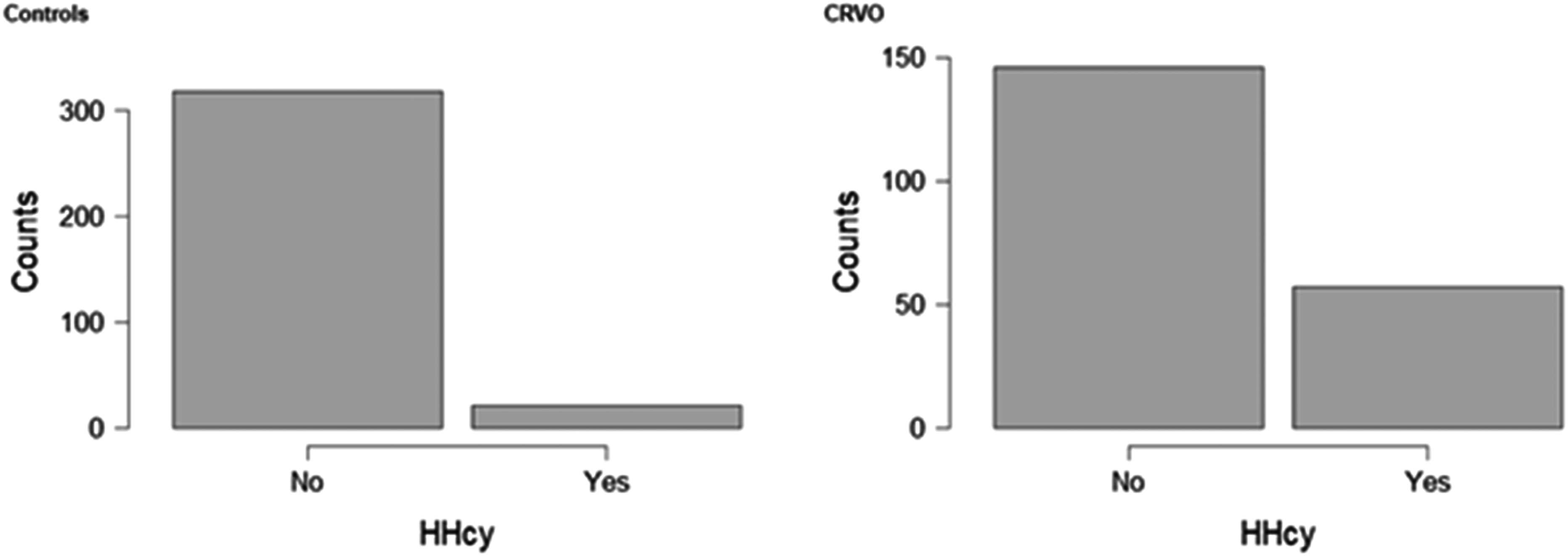
Distribution of subjects with hyperhomocystenemia (HHcy) in both groups.
In the study group, 19.21% of subjects had a diagnosis of type II diabetes mellitus (DMII), as compared to 5.05% of subjects in the control group (Figure 10) (p < .001 with the Chi-square test).
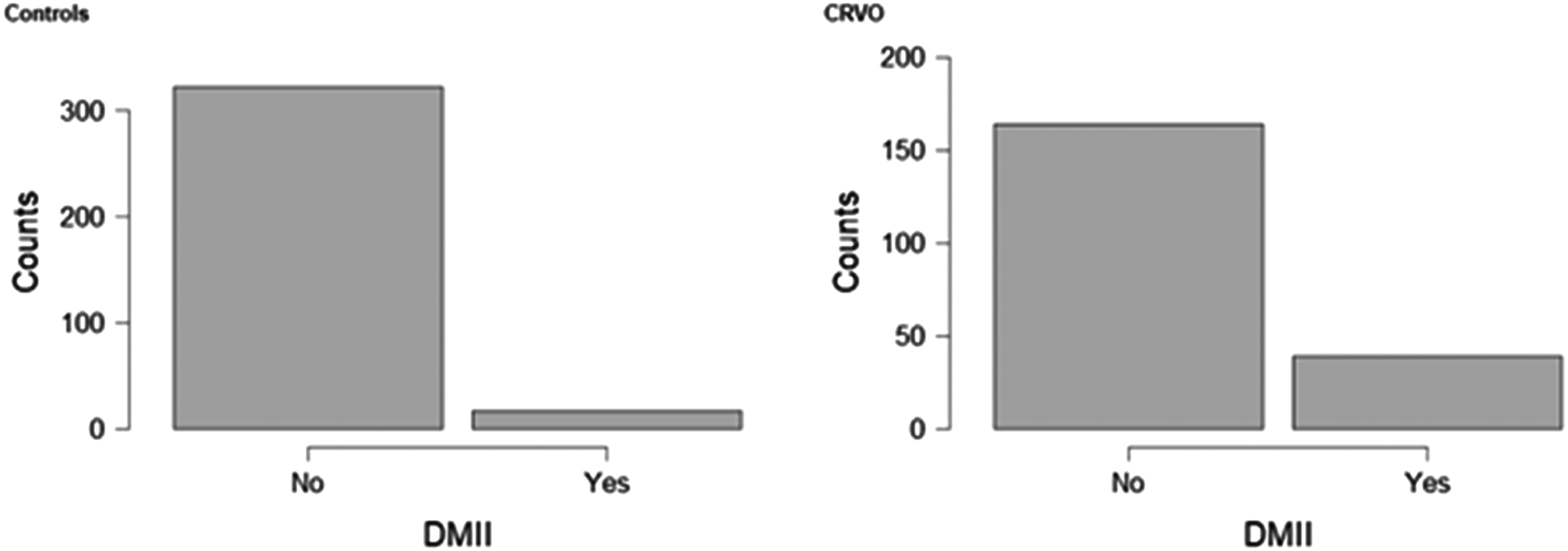
Distribution of subjects with diabetes mellitus type II (DMII) in both groups.
No statistically-significant differences were found in the number of subjects with an history of myocardial infarction (p = .898 with the Chi-square test), COPD (p = .898 with the Chi-square test), chronic liver disease (p = .865 with the Chi-square test), migraine-type headache (p = .411 with the Chi-square test), SLE (p < .766 with the Chi-square test), OSAS (p < .114 with the Chi-square test), or thyroid disease (p = .697 with the Chi-square test).
Logistic regression analysis was conducted to calculate the odds (and their respective confidence intervals) for each variable (Figure 11).
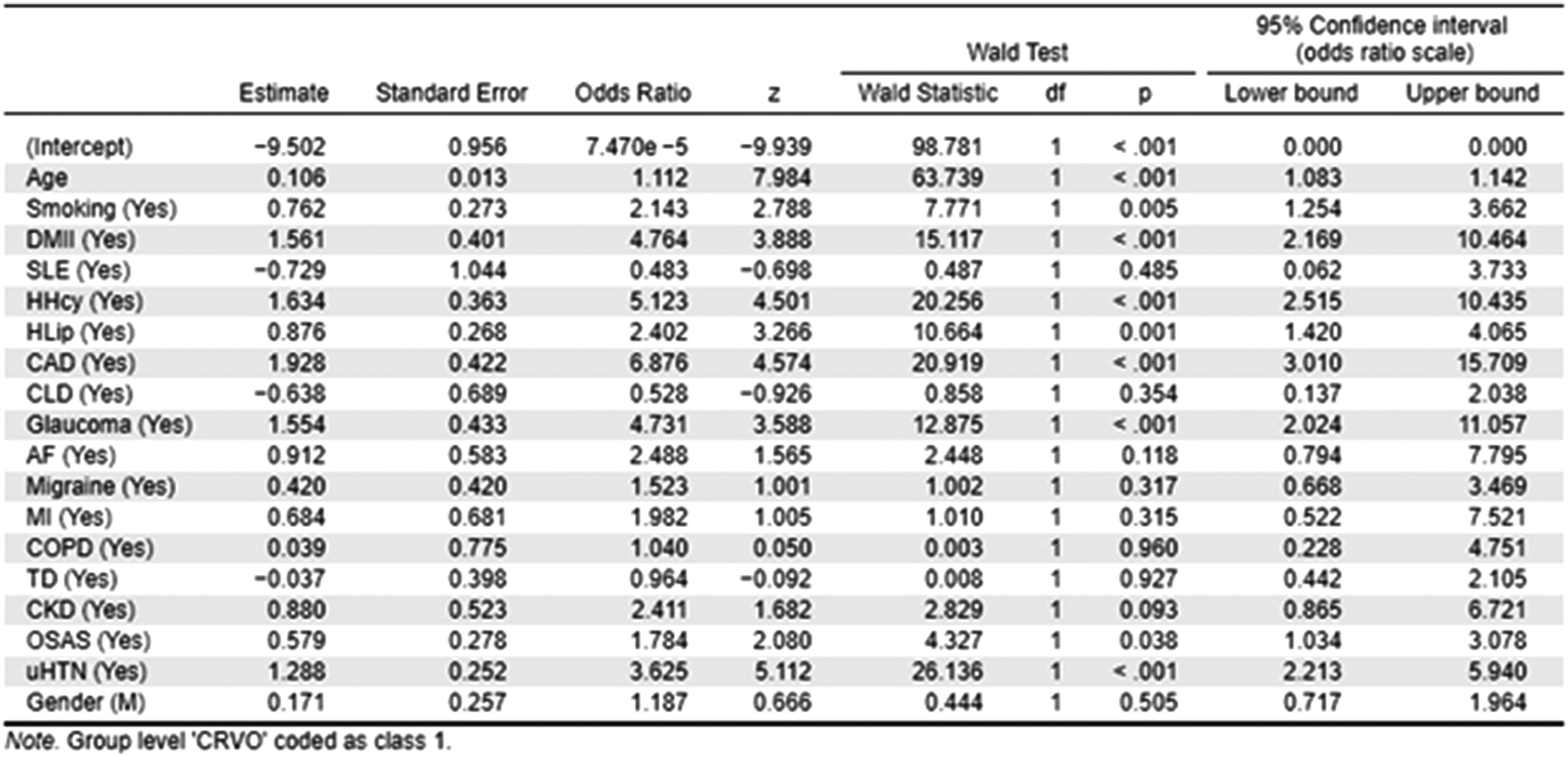
Results of the logistic regression analysis.
Discussion
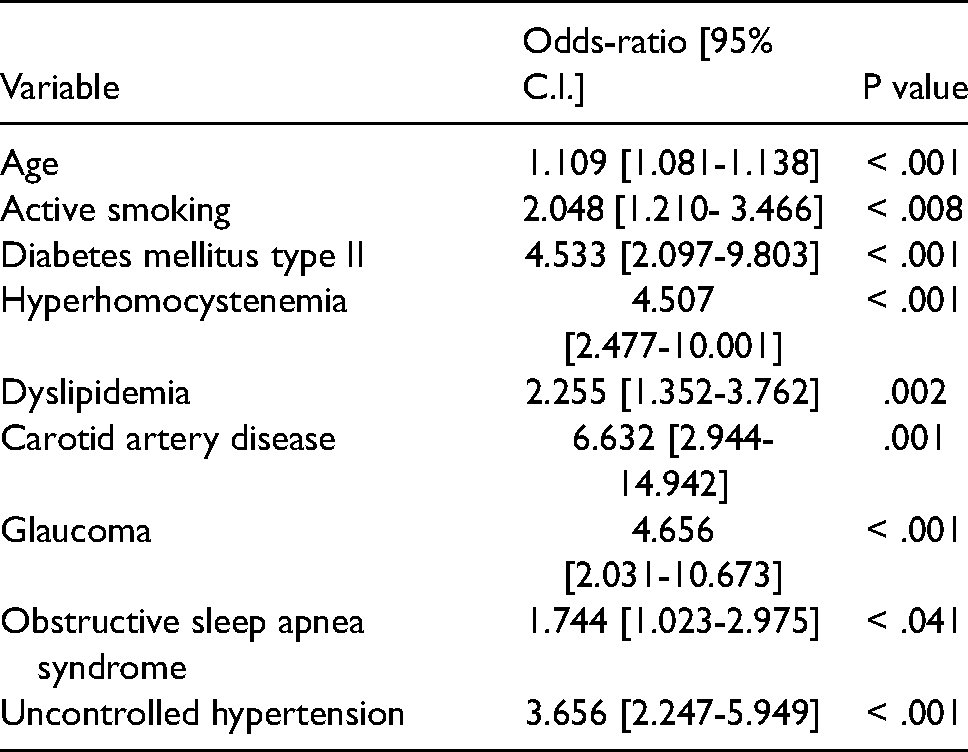
This epidemiological study has explored the role of demographic factors and systemic comorbidities in increasing the incidence of central retinal vein occlusion. This was accomplished by comparing a large group of patients affected by CRVO with healthy controls. Authors found that age, diabetes mellitus type 2, active smoking, hyperhomocystenemia, dyslipidemia, presence of carotid artery disease, glaucoma, obstructive sleep apnea syndrome, uncontrolled blood hypertension can all increase the risk for this occlusive event in the retinal venous system (Table 1). Previous studies had already identified some of these risk factors, yet on samples of smaller size or different ethnicity. The current study is probably one of the largest conducted on the Italian population. The logistic regression analysis was used to estimate the effect size for each variable (Tab 1). Of note, these variables probably exert a synergistic effect when present simultaneously in the same patient.
– variables found to increase the risk for CRVO in the current study and their respective odds ratios.
Advancing age and the presence of systemic arteriosclerotic vascular disease are known risk factor for CRVO. 12 CRVO rarely occurs in subjects younger than 50 years of age. In addition, arterial hypertension, dyslipidemia, and diabetes mellitus are frequently encountered in these patients. Logistic regression analysis has estimated the OR for advancing age around 1.109. In other words, advancing age increases the risk for CRVO by 10%, as compared to younger controls. Previous studies conducted on a multiethnic population had found ORs between 1.34 and 1.70..2,9,17 This could be explained by the fact that non-Caucasian ethnicities carry an increased risk for CRVO.18,19 The current study primarily consisted of individuals of Caucasian ethnicity. Arterial hypertension is another well-known risk factor. Its OR was calculated at 3.656. This means that hypertensive subjects are 3.5 times more likely to suffer from CRVO. For the purpose of this analysis, subjects with higher-than-recommended blood pressure values were categorized as a single group. No subgroup analysis was conducted based on hypertension severity. Furthermore, no distinction was made between systolic or diastolic hypertension. In 2011, Satoshi Arakawa et al. were able to estimate the OR for each 10-mmHg increase in diastolic blood pressure around 1.51. This suggests some sort of linear relationship between diastolic hypertension and risk for CRVO: the higher the pressure, the greater the likelihood to suffer from CRVO.
Active smoking, hyperhomocystenemia, dyslipidemia, and diabetes mellitus type II are important modifiable risk factors for major cardiovascular accidents. Their association with CRVO has been confirmed in the current study. Active smokers and subjects with dyslipidemia have about twice the risk for major retinal venous thrombotic events. Subjects with hyperhomocystenemia or DMII are about 4.5 times more likely to suffer from CRVO. Carotid artery disease increases the risk by a factor of 6.5. In addition, comorbid internal carotid artery disease also correlates with a poor visual prognosis, as found in a Japanese study conducted by Daisuke Nagasato et al. in 2020. 20 Obstructive sleep apnea syndrome was estimated to increase the risk by a factor of 1.744. The possible higher prevalence of OSAS among patients with RVO was detected in recent studies, but the current analysis is the first to quantify its actual impact in terms of odds-ratios. 21 The mechanism for increased risk for CRVO is probably explained by the microvascular changes found in the retinal vessels of subjects with OSAS. 24
No statistically-significant differences were found for the other variables: thyroid disease, systemic lupus erythematosus, migraine headache, chronic kidney disease, chronic liver disease, chronic obstructive pulmonary disease, history of myocardial infarction, or gender. Gender has not been associated with an increased risk in previous studies either. 25 However, a Chinese study found an association between retinal vein occlusion and chronic kidney disease, which was not confirmed in the current study.. 27
Other parameters have been identified as risk factors for retinal vein occlusions. These were not included in the current study but are listed below: systemic lupus erythematosus (adjusted HR = 3.883, 95% CI 2.299 to 6.558), high hematocrit (OR, 3.09; 95% CI, 1.10–1.22), high hematocrit and arterial hypertension (age- and sex-adjusted OR, 36.0; 95% CI, 4.43–292), presence of anticardiolipin antibodies (OR: 3.9, 95% CI 2.3–6.7), MTHFR mutation (OR: 1.2, 95% CI 0.9–1.6), factor V Leiden mutation (1.5 (95% CI 1.0–2.2)), prothrombin gene mutation (1.6 (95% CI 0.8–3.2)), plasma fibrinogen (OR, 3.29; 95% CI, 1.08–10.02; highest quartile vs. lowest), history of barbiturate use (OR, 5.30; 95% CI, 2.28–12.31), presence of retinal arteriovenous nicking (OR, 4.01; 95% CI, 2.06–7.81), focal arteriolar narrowing (OR, 2.45; 95% CI, 1.29–4.66 by Ronald Klein et al. or OR, 4.38; 95% CI, 1.44–13.34 by Ning Cheung et al. or OR, 5.17; 95% CI, 2.59–10.29 by Tien Yin Wong et al.), serum ionized calcium level (OR per 0.4 mg/dL, 0.43; 95% CI, 0.23–0.79), serum phosphorus level (OR per 0.3 mg/dL, 1.15; 95% CI, 1.01–1.30), and serum creatinine level (OR for > or = 1.4 vs < 1.4 mg/dL, 1.61; 95% CI, 1.00–2.59)..4,12 In addition, some factors have been found to increase the risk selectively in either BRVO or CRVO. For BRVO: pulse pressure (OR 1.24 for 10 mm Hg, 95% CI 1.03, 1.48), ocular perfusion pressure (OR 2.09 for 10 mm Hg, 95% CI 1.45, 3.01), arteriovenous nicking (OR 16.75, 95% CI 7.33, 38.24), and focal arteriolar narrowing (OR 22.86, 95% CI 8.43, 62.03), atrial fibrillation (3.37, 1.24–9.12), peripheral artery disease (OR 1.83, 95% confidence interval 1.14 to 2.95), and history of migraine headache (OR, 1.99; 95% CI, 1.08–3.67). For CRVO, a family history of stroke (4.64, 1.18–18.25).2,28
The current study has concluded that age, active smoking, diabetes mellitus type II, hyperhomocystenemia, dyslipidemia, coronary artery disease, glaucoma, obstructive sleep apnea syndrome, and uncontrolled arterial hypertension are important risk factors for CRVO. In agreement with the literature, authors of this study emphasize the importance of primary prevention. A balanced diet and an active lifestyle are recommended to reduce the risk for vascular thromboembolic phenomena. Retinal vein occlusions almost always have a systemic correlation. For this reason, a closer cooperation with primary care physicians is encouraged.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.