
Abstract
Purpose
To investigate the prevalence of dry eye symptoms after successful dacryocystorhinostomy and explore the potential risk factors.
Methods
This cross-sectional study included 565 patients with lacrimal passage obstruction (LPO) who underwent external dacryocystorhinostomy. Ocular Surface Disease Index (OSDI) total score of 13 or more was regarded as presence of dry eye symptoms. OSDI total score greater than 22 combined with self-reported dry eye was defined as symptomatic dry eye. Logistic regression and linear regression were used to examine the associations between OSDI scores and its potentially predictive factors.
Results
Of the 565 patients, 344 completed the questionnaire, among which 101(29.4%) patients presented with dry eye symptoms, including 53(15.4%) mild, 14(4.1%) moderate and 34(9.9%) severe, and 48(14.0%) patients can be defined as symptomatic dry eye. Univariate logistic regression revealed that age, educational levels, income levels, and hypertension were significantly correlated with the presence of dry eye symptoms (P < 0.05). After multivariate adjustment, lower income levels were found significantly associated with dry eye symptoms (P < 0.05). Univariate linear regression demonstrated that age, lower educational levels, surgery history, and hypertension were significantly associated with OSDI total score (P = 0.037, 0.012, 0.022, 0.029 respectively). Multivariate stepwise linear regression manifested that educational levels and the surgery history influenced the OSDI total score mostly (P = 0.021, 0.036 respectively).
Conclusions
Dry eye problem of LPO patients after successful dacryocystorhinostomy cannot be ignored. In the preoperative evaluation, we should pay special attention to the elderly patients with lower educational levels, lower income levels or systemic diseases.
Keywords
Introduction
Dry eye disease (DED) is a chronic, multifactorial disorder of the ocular surface due to the loss of the tear film homeostasis, accompanied by varying degrees of ocular discomfort. 1 Dry eye symptoms comprise dryness, ocular pain, burning, visual disturbance, eye fatigue, grittiness, photophobia, tearing, and others. 2 The diagnosis of dry eye disease is heavily dependent on dry eye symptoms in clinical practice. 3 This implies that dry eye symptom assessment, such as a symptom questionnaire, is arguably the most repeatable diagnostic tests for DED. 4
Punctal occlusion is a kind of mechanical intervention for DED, which occludes the puncta to block tear drainage and preserve natural tears, thus improving the quantity and quality of tear. 5 Therefore, for some DED patients, lacrimal passage occlusion may be a protective factor of dry eye symptoms. Lacrimal passage obstruction (LPO) is a common disorder in ophthalmology clinic, with epiphora as the main manifestation. In general, dacryocystorhinostomy (DCR) or lacrimal passage intubation can significantly improve the visual function, visual quality and life quality of patients with LPO.6–8 However, we can often see dry eye symptoms worsened in some LPO patients after DCR in clinical practice. There have been previous reports of the occurrence of dry eye after Jones tube insertion or DCR in LPO patients.9,10 DCR may lead to the occurrence of DED or aggravate the original DED, affecting the life quality of patients. On the other hand, while relieving the symptoms of DED, punctal occlusion can also bring the side effects of epiphora to some patients.11,12 How to balance the relationship between LPO and DED to help patients benefit more from the treatment is worth thinking.
Kamao et al. compared the life quality of patients with and without DED after dacryoendoscopic probing and sheath-guided bicanalicular intubation treatment of nasolacrimal duct obstruction (NLDO), and pointed out that those with DED may not be able to improve life quality after treatment. 13 Thus, it will be meaningful to evaluate the patients’ condition and predict the possibility of DED before treatment of LPO. Kamao et al. discovered that 12mm of the preoperative Schirmer I test can be used as the cutoff value to predict postoperative dry eye, 13 but did not provide more analysis of predictors. Currently, relevant research on the prevalence and risk factors of DED in patients with LPO treatment is insufficient.
External DCR (ex-DCR) is a traditional and effective treatment for NLDO. 14 This study aims to investigate the prevalence of dry eye symptoms after successful ex-DCR surgery and explore the potential risk factors, to provide help for preoperative prediction of the possibility of postoperative DED.
Methods
Study population
This was a cross-sectional research. The patients with LPO who underwent ex-DCR in Peking University Third Hospital from January 2016 to January 2021 were followed up by telephone. Inclusion criteria: Patients diagnosed with NLDO and treated with ex-DCR combined with artificial lacrimal intubation set (RITLENG) implantation. The artificial lacrimal intubation set was removed two weeks after operation. Telephone survey was conducted at least one month postoperatively. Lacrimal irrigation one month postoperatively showed that the lacrimal passage was unobstructed after surgery. The cases that had a recurrence of LPO were excluded.
Data collection
Patients’ basic information including sex, age, menstrual history (for females), reproductive history, education, income level, history of other eye surgery, and past history of systemic diseases were collected from medical records or through telephone inquiry. Because income levels vary greatly in different regions, we identify income levels by asking patients’ subjective feelings. The patients were asked how do they think their income level compares with people living around. The answer is divided into four levels, including low, middle, high, and very high. Each patient was asked on a voluntary basis to fill out the Ocular Surface Disease Index (OSDI) questionnaire on dry eye symptoms, according to which the dry eye level was classified. This study followed the Declaration of Helsinki and was approved by Peking University Third Hospital Medical Science Research Ethics Committee. All personally identifiable information of subjects was treated with strict secrecy and used for research purposes only.
OSDI questionnaire
The OSDI scores consist of four parts, which are the total score and the scores for the 3 subscales, including ocular symptoms subscale, vision-related function subscale, and environmental triggers subscale. 15 Patients were divided into 4 categories according to the OSDI total score: without dry eye symptoms (scores 0–12), mild symptoms (13–22), moderate symptoms (23–32), and severe symptoms (33–100).15,16 OSDI total score of 13 or more was regarded as presence of dry eye symptoms. According to previous researches, symptomatic DED was defined as OSDI total score greater than 22 combined with self-reported dry eye.17,18
Statistical analysis
Data analysis was performed using SPSS 23.0 (IBM, Armonk, New York, United States). OSDI scores were expressed as mean ± SD. Shapiro-Wilk test was used for normality test P > 0.05 was considered to conform to the normal distribution. Nonparametric Mann–Whitney U test was used for two independent samples non-normally distributed, and nonparametric Kruskal-Wallis test was used for more than two independent samples non-normally distributed.
Odds ratios (OR) and univariate, unadjusted logistic regression models were used to describe the relationship between the presence of dry eye symptoms and the potentially predictive factors, including sex, age distribution, reproductive history, menstrual history (only females), educational levels, income levels, history of other eye surgery, and systemic diseases including hypertension, diabetes and coronary heart disease. Predictive factors significantly associated with presence of dry eye symptoms in univariate logistic regression analysis were included in multivariate logistic regression analysis.
Univariate linear regression model was established to analyze the correlation between total OSDI scores and the subscales and potentially predictive factors, including sex, age, reproductive history, menstrual history (only females), educational levels, income levels, history of other eye surgery, and systemic diseases including hypertension, diabetes and coronary heart disease. A collinearity analysis was conducted before the multivariate linear regression model was established. Age and menstrual history were found to have multicollinearity. According to clinical significance, menstrual history was excluded. Multivariate linear regression model was established to include all the factors mentioned above except menstrual history in the same model to analyze their correlation with total OSDI score. The stepwise method was used to perform the analysis. The inclusion criterion is P ≤ 0.05, and the exclusion criterion is F ≥ 0.1. P < 0.05 was considered statistically significant.
Results
Study population and procedure characteristics
A total of 565 patients were interviewed by telephone. Due to the change of telephone number, refusal of investigation, or death of patients, 221 patients were lost to follow-up. A total of 344 valid questionnaires were received, including 69 males and 275 females aged 16∼88 years old. The mean age was 59.8 ± 13.7. According to the OSDI total score, 101 (29.4%) patients presented with dry eye symptoms, including 53 (15.4%) mild, 14 (4.1%) moderate and 34 (9.9%) severe, among which 48 (14.0%) patients can be defined as symptomatic DED. The number and proportion of patients were listed in Table 1. The proportion of low educational level population is large. Patients with education below junior high school accounted for 46.8%. Of the 66 patients who experienced previous surgery on the affected eye, 49 had underwent cataract surgery, 5 had pterygium surgery, and the rest had external eye surgery, orbital surgery, or vitreoretinal surgery.
Univariate and multivariate logistic regression of potential predictive factors of presentation of dry eye symptoms.
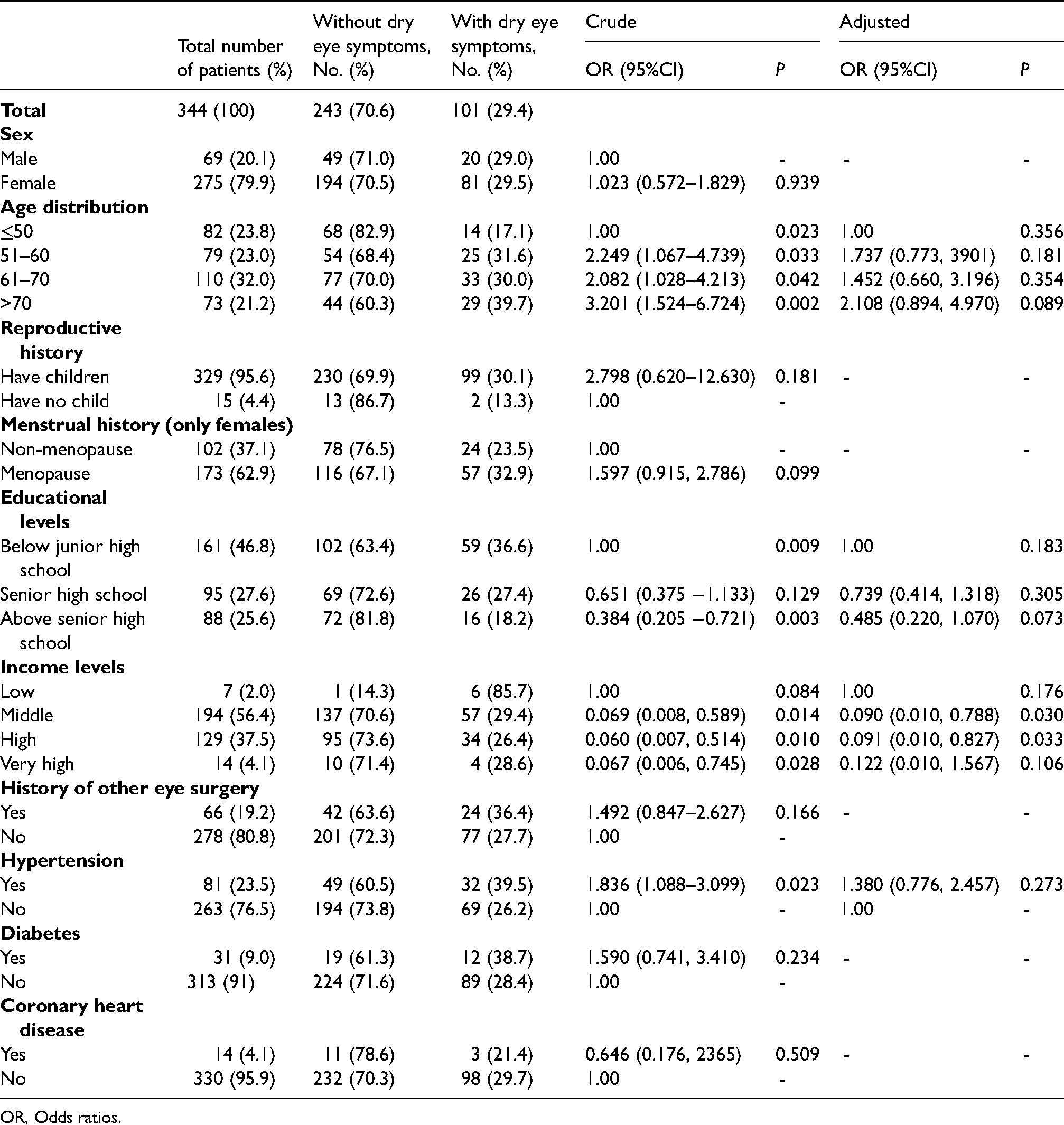
OR, Odds ratios.
Mean OSDI scores of patients were presented in Figure 1. There were significantly differences among the scores of ocular symptoms subscale for different age groups (P = 0.007), educational levels (P = 0.027), and income levels (P = 0.026). Patients with older age, lower educational levels, and lower income tend to have higher scores. The score of ocular symptoms subscale was higher in in patients with diabetes than in those without (7.668 ± 12.640 vs 12.419 ± 14.881; P = 0.019). The scores of the vision-related function subscale were found significantly different between the hypertension group and the non-hypertension group (8.729 ± 18.793 vs 15.509 ± 26.439; P = 0.014).
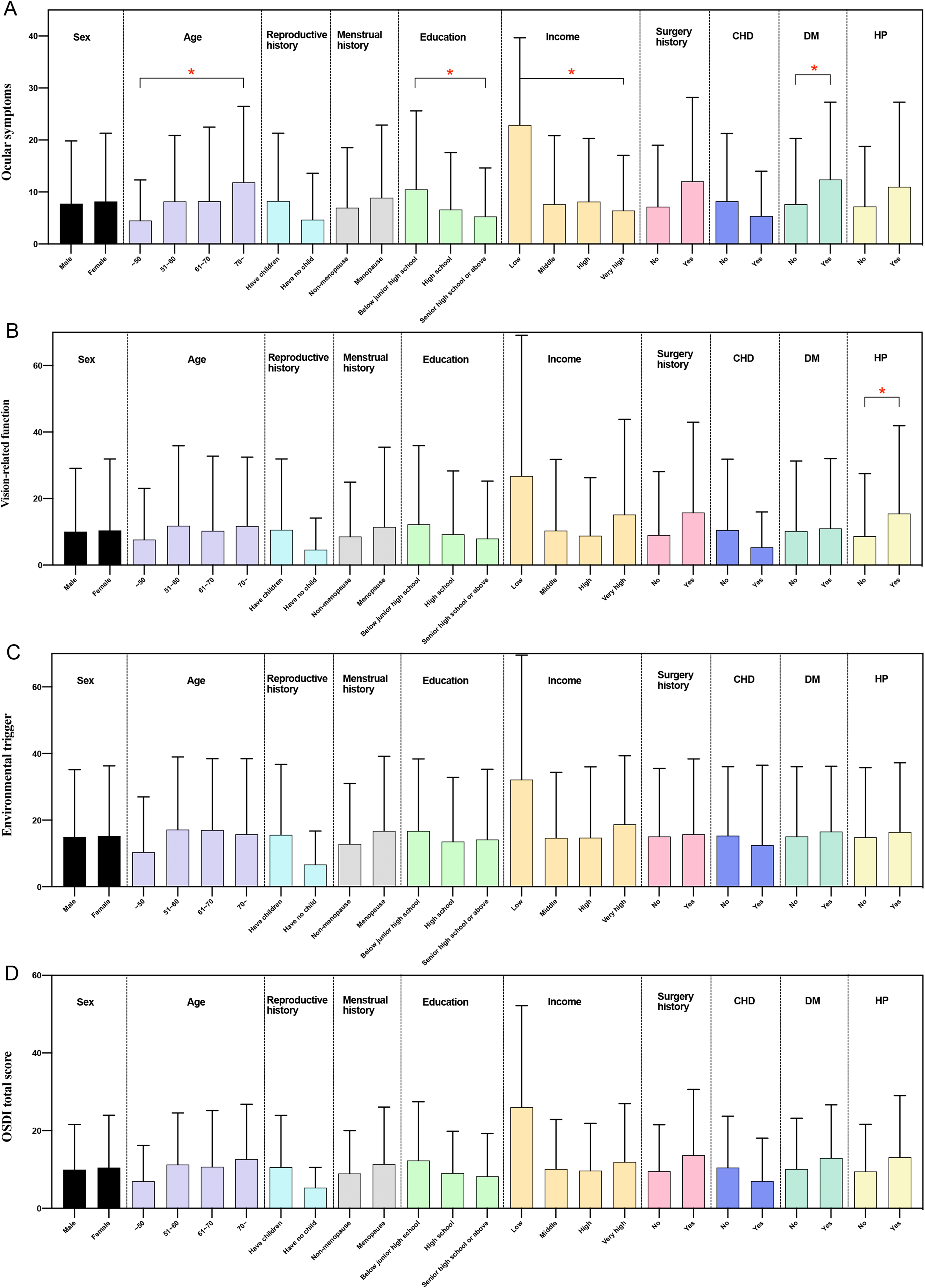
Mean OSDI scores. A. ocular symptoms subscale; B. vision-related function subscale; C. environmental triggers subscale; D. OSDI total score. CHD, coronary heart disease; DM, diabetes mellitus; HP, hypertension.
Risk factors associated with Dry Eye symptoms after ex-DCR
Univariate and multivariate logistic regression of potential predictive factors of presence of dry eye symptoms were listed in Table 1. Univariate logistic regression revealed that the following factors were significantly correlated with the presence of dry eye symptoms: age distribution (reference: ≤50 years; 51–60 years: crude OR = 2.249 (1.067–4.739), P = 0.033; 61–70 years: crude OR = 2.082 (1.028–4.213), P = 0.042; 71–80 years: crude OR = 3.201 (1.524–6.724), P = 0.002), educational levels (reference: below junior high school; senior high school: crude OR = 0.651 (0.375–1.133), P = 0.129; above senior high school: crude OR = 0.384 (0.205–0.721), P = 0.003), income levels (reference: low; middle: crude OR = 0.069 (0.008–0.589), P = 0.014; high: crude OR = 0.060 (0.007–0.514), P = 0.010; very high: crude OR = 0.067 (0.006–0.745), P = 0.028), and hypertension (crude OR = 1.836 (1.088–3.099), P = 0.023). A final multivariate model was performed including age distribution, educational levels, income levels, and hypertension, which were statistically significant in the univariate analysis. Income levels remained in the multivariate model as independent predictors (reference: low; middle: adjusted OR = 0.090 (0.010–0.788), P = 0.030; high: adjusted OR = 0.091 (0.010–0.827), P = 0.033; very high: adjusted OR = 0.122 (0.010–1.567), P = 0.106).
Table 2 demonstrated the results of the univariate linear regression between different potential influential factors and OSDI scores. Age and lower educational levels were found significantly associated with OSDI total score (P = 0.037, 0.012, respectively) and the ocular symptoms subscale (P = 0.004, 0.001, respectively). History of other eye surgery and the presence of hypertension were found significantly associated with OSDI total score (P = 0.022, 0.029, respectively), the ocular symptoms subscale (P = 0.006, 0.021, respectively), and the vision-related function subscale (P = 0.018, 0.011, respectively).
Univariate linear regression of potential predictive factors of total OSDI scores and the subscales.
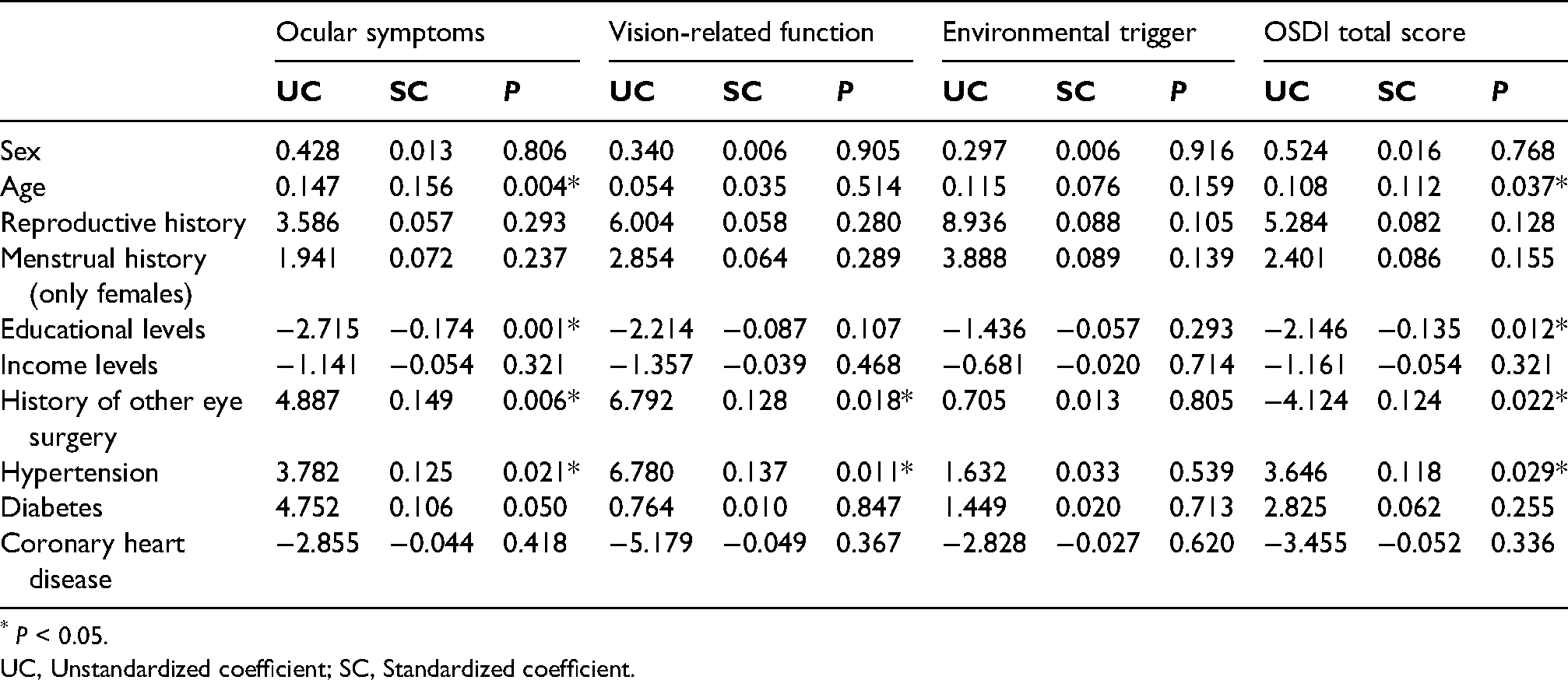
* P < 0.05.
UC, Unstandardized coefficient; SC, Standardized coefficient.
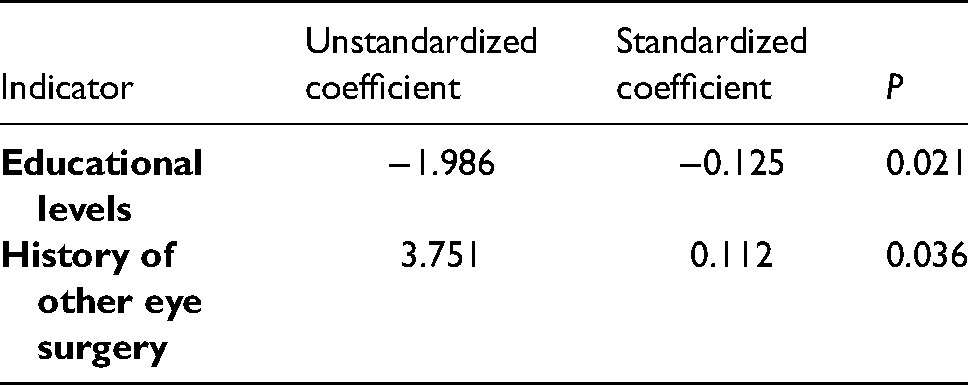
To further explore the contribution of different potential influential factors, multivariate linear regression was conducted and the results were demonstrated in Table 3. Educational levels were found having the most significant impact on OSDI total score (P = 0.021), while the history of other eye surgery was also preserved in the model (P = 0.036).
Multivariate linear regression of potential predictive factors of total OSDI scores.
Discussion
For LPO patients, DCR or lacrimal passage intubation may bring many benefits, such as relieving the epiphora symptom, and improving visual function, visual quality and life quality.6–8 However, this approach can be complicated by aggravation of dry eye symptoms. 13 The OSDI is a validated and reliable questionnaire designed to assess the ocular symptoms consistent with DED and their impact on vision-related function.15,19 In our study, the incidence of dry eye symptoms was 29.4%, and the incidence of symptomatic DED was 14%. It is lower than that obtained in a large meta-analysis which demonstrated the pooled prevalence of symptomatic DED was 38.89% among Chinese population. 20 A study in South Korea showed that 27.3% of patients presented with dry eye after successful endoscopic DCR, which is close to our results. 21 A study in UK showed 17% patients caught dry eye symptoms after Lester Jones tube insertion, 9 but it is similar to the rate in the normal population. 22 After DCR, the tear volume decreased, but the incidence of symptomatic DED did not increase, indicating that the quality of tear film may play a more important role in the presence of dry eye symptoms than the quantity of tear film. Tear film is the first barrier of ocular surface and an important refractive medium, with the functions to protect, lubricate, and nourish the ocular surface, and maintain visual quality.23,24 Epiphora and DED are both manifestations of tear film homeostasis lost, which can cause decreased visual quality and ocular discomfort. 23 After DCR, tear film may be more stable for most patients than preoperatively. DCR in patients with epiphora is to make the excessive tears get better drainage and increase the stability of tear film, which does not conflict with punctal occlusion in the treatment of DED, whose principle is to increase the quantity of tear and improve the stability of tear film for people with tear volume insufficiency. 5 The final outcome of both is better protection of the tear film homeostasis. This may be the reason why the incidence of symptomatic DED did not increase after DCR. It is still very important to identify susceptible people before surgery, so as to make a better evaluation preoperatively and help patients benefit more from the treatment.
Consistent with previous studies,19,25,26 the present study discovered that age, history of previous surgery on the same eye (such as cataract surgery), diabetes, and hypertension were risk factors of dry eye symptoms. Among them, ocular symptoms were significantly associated with age and educational achievements. Lines of evidence support the hypothesis that the incidence of DED increases with age. For example, there is an age-related decrease in the quality and lipid profiles of meibomian gland secretions possibly due to atrophy of acinar cells, 25 in keeping with the age-related decline in the function of other sebaceous glands. 27 Our study observed that people with lower income and lower educational levels were more prone to suffer from LPO, and at the same time, they were more likely to develop dry eye symptoms postoperatively, which may be attributed to the fact that people with low income and education may not have enough labour protection. Consistent with our study, a study among US women found that those with higher levels of education reported a lower prevalence of dry eye. 28 However, the conclusions of different regions are not all the same. A study in South Korea showed that people with lower educational levels are less likely to develop dry eye. 29 In their study, the majority of the participants was aged under 60, and younger people with higher levels of education tend to work at the computer and thus have a higher incidence of dry eye. 29 By contrast, our study focused on the patients with lacrimal obstruction, mainly consisting of older people. Among these people, lower levels of education were more likely to be related to harder work or a lower standard of living and a higher incidence of dry eye. Further studies are required to confirm this association.
In this study, both ocular symptoms and vision-related function were found significantly associated with hypertension and previous surgery history of the same eye. This suggests that the factors that may directly change the anatomical structure and physiological function of the ocular surface may have more influence on the vision-related function than the social factors. Eye surgery is an important cause of iatrogenic dry eye. 26 Previous studies have revealed that DED is correlated with many systemic diseases, such as hypertension, 30 diabetes,19,31 ischaemic heart disease 31 etc. Various systemic diseases may also affect the structure and physiological function of ocular surface. Therefore, for LPO patients with other eye surgery history and systemic diseases, it is important to fully evaluate their ocular surface conditions before treatment.
Several limitations exist in the present study. Firstly, this is a cross-sectional study. There is no preoperative data of patients with dry eye, so we cannot compare the pre- and postoperative status. In addition, the OSDI is a screening standard, which only evaluates the subjective feelings of patients and lacks objective indicators. Prospective studies are needed in the future.
In summary, the symptomatic dry eye problem after DCR cannot be ignored. Our study discussed the risk factors of dry eye symptoms after DCR, and provided evidence for the preoperative assessment of LPO patients. We should pay special attention to the elderly LPO patients with lower educational levels, lower income levels and systemic diseases such as hypertension and diabetes. Our study explored the importance of tear film homeostasis in improving the symptoms of both epiphora and dry eye, and open up the possibility to better predict postoperative dry eye symptoms before DCR. With the possibility of risk prediction before DCR, we may be able to help LPO patients benefit more from the treatment.
Footnotes
Authors’ contributions
Y. J., Y. G. and G. Q. collected the data. Y. L. double checked the data. Y. G. and Y. W. analyzed and interpreted the data. Y. J. and Y. G. were major contributors in writing the manuscript. Y. T. and X. L. revised the manuscript. All authors read, commented and approved the final manuscript.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request
Ethical approval
This study was approved by Peking University Third Hospital Medical Science Research Ethics Committee. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. For this type of study formal consent is not required.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Natural Science Foundation of Beijing Municipality (grant number 7202229).