
Abstract
Purpose:
To describe the natural history of acquired vitelliform lesions (AVLs) associated with different types of pigment epithelial detachments (PEDs) in dry age-related macular degeneration.
Methods:
A retrospective review of clinical examination and multimodal imaging data of patients with AVLs associated with PED(s) was performed.
Results:
This study included 25 eyes of 17 patients. The mean age of patients was 67.2 ± 9.7 (47–83) years. The mean follow-up time was 32.6 ± 16.2 (12–66) months, excluding four patients (five eyes) that were lost to follow-up. The mean logMAR BCVA was 0.21 ± 0.16 at baseline and 0.38 ± 0.28 at final visit (p = 0.016). At the end of the follow-up period, PEDs enlarged in eight eyes (40%) and were unchanged in two eyes (10%). Spontaneous resolution of the central PED(s) with AVLs was seen in four (20%) eyes. Rupture of the PED(s) occurred in four eyes (20%), with two developing central foveolar atrophy afterwards. Overall, central foveolar atrophy was seen ultimately in four eyes (20%).
Conclusion:
It seems that high PED size may be a risk factor for PED rupture during follow-up. 1/3 of the eyes ended up with unfavorable anatomical outcome.
Keywords
Introduction
Acquired vitelliform lesions (AVLs) may occur in many different clinical entities and their characteristic imaging finding is the accumulation of yellowish and presumably subretinal material. The exact pathophysiology of the AVL formation and the effect of this material on natural courses of these diseases remain unknown. It has been proposed that an unknown insult leading to stress response in retinal pigment epithelium may cause the formation of this material through ineffective phagocytosis of shed outer segments, resulting in pigment-laden macrophages. 1 Other possible mechanisms include the presence of a subretinal fluid separating the retinal pigment epithelium (RPE) from the photoreceptor outer segments leading to dysfunction, abnormally increased lipofuscin content causing reduced phagocytosis, and the loss of specialization with aging.2–4
Dry (non-neovascular) age-related macular degeneration (AMD) and its associated pigment epithelial detachments (PEDs) is one of the possible causes of AVL. In a case series (90 eyes) evaluating all causes of AVLs, non-neovascular AMD was seen in 19 eyes (21.1%), and PED(s) were seen in 7 eyes (7.7%). 1 Different types of drusen, including cuticular drusen, subretinal drusenoid deposits, and large drusen, were also reported to be accompanied by AVLs.2,5,6
The natural course of AVLs starts with an initial period of accumulation, followed by resorption. However, the literature specifically evaluating the natural course of dry AMD in the setting of AVLs is limited. Herein, we present long-term follow-up and prognosis data about AVLs in a pure dry AMD group with different types of PED(s).
Methods
The eyes of patients presenting with AVLs associated with dry-AMD were retrospectively analyzed in this observational consecutive case series. The study was conducted at the Department of Ophthalmology, Ankara University School of Medicine, Ankara, Turkey, in accordance with the Declaration of Helsinki. This study was approved by the Institutional Review Board Committee of Ankara University.
The multimodal imaging definition of AVL was used in this study. 1 The diagnosis of vitelliform material depended on the presence of yellowish deposits in the subretinal space in fundoscopy and hyperreflective material above the RPE layer on Spectral-domain optical coherence tomography (SD-OCT) (Spectralis, Heidelberg Engineering, Inc., Heidelberg, Germany). Fundus autofluorescence (FAF) (Heidelberg Retina Angiograph 2; Heidelberg Engineering, Heidelberg, Germany) imaging defined the vitelliform material as hyperautofluorescent areas that correlated with the regions where vitelliform material was observed on color fundus and OCT images. The diagnosis of AMD depended on the revised clinical classification of AMD. 7 Cuticular drusen with RPE abnormalities were also included. 8 The participants underwent a full ophthalmic assessment that included best corrected visual acuity (BCVA) with the Early Treatment Diabetic Retinopathy Study (ETDRS) chart, slit lamp biomicroscopy, and a dilated funduscopic examination. SD-OCT and FAF scans were performed for all participants. Fluorescein angiography (FA), indocyanine green angiography (ICGA; Heidelberg Retina Angiograph 2), and/or optical coherence tomography angiography (OCTA; Avanti RT Vue XR® with AngioVue software; Optovue Inc., Fremont, CA, USA) was performed to exclude choroidal neovascularization. Greatest basal diameter and maximum height of the largest PED on SD-OCT were measured using the caliper tool at all visits. Greatest basal diameter was defined as the greatest PED base diameter on the plane of Bruch membrane as the reference. Maximum height was defined as the greatest distance between Bruch membrane and the outer boundary of the RPE. Enlargement of the PED was defined as > 10% increase in the greatest basal diameter and/or >10% increase in the maximum height.
Primary outcome measures of the study were the change in the characteristics of AVLs over time and the final outcome so that we may make a prediction about the effects of these lesions on the final prognosis.
The statistical analyses were performed using SPSS software for Windows version 15.0 (SPSS, Inc, Chicago, IL). A Shapiro-Wilk test was performed for all variables to detect departures from a normal distribution. Descriptive statistics were expressed as mean ± standard deviation or median (minimum–maximum) for continuous variables and as the number of observations and percentage for categorical variables. A Wilcoxon test was performed to compare the baseline and final visit parameters of related non-parametric variables. Spearman’s rho test was used for correlation analysis of non-parametric variables. A linear mixed effects model was used to estimate the longitudinal change of BCVA, greatest basal diameter of PED and maximum height of PED. The mean of scores was modeled as a linear function of time since baseline visit. A p-value of < 0.05 was considered to be statistically significant.
Results
This study included 25 eyes of 17 patients (14 females, 3 males) with AVL associated with dry AMD. The mean age of the patients was 67.2 ± 9.7 (47–83) years. The mean follow-up time was 32.6 ± 16.2 (12–66) months, excluding four patients (five eyes) that were lost to follow-up. Demographic and clinical characteristics of the cases are given in Table 1.
Demographic and clinical characteristics of the patients.
BCVA: best-corrected visual acuity; NA: not applicable; PED: pigment epithelial detachment.
All eyes had an acquired vitelliform material seen as a yellowish lesion in the central macula and proven by SD-OCT and FAF images. All eyes had associated PED(s) including different structural characteristics: multiple drusenoid in 14 eyes (56%), large single seromembranous in nine eyes (36%), and multiple seromembranous in two eyes (8%). The mean logMAR BCVA was 0.21 ± 0.16 at baseline. The mean greatest diameter of the largest PED was 1828 ± 972 µm and maximum height of the PED was 278 ± 190 µm at baseline. There was a statistically significant correlation between baseline BCVA and greatest basal diameter of PED (rho = 0.472, p = 0.017). There was also a statistically significant correlation between baseline BCVA and the maximum height of the PED (rho = 0.551, p = 0.004). Subretinal fluid was present in 13 (52%) eyes, with a mean thickness of 50.0 ± 28.6 µm. To exclude choroidal neovascularization (CNV), OCTA was performed in 16 (64%) eyes, combined FA - ICGA was performed in 9 (36%) eyes, and only FA was performed in seven (28%) eyes. On FA, accompanying basal laminar drusen was observed in two eyes.
Eight (47.1%) patients had bilateral AVL. The fellow eyes of patients with unilateral AVL had central foveolar atrophy (two eyes), drusenoid PED(s) (three eyes), seromembranous PED(s) (one eye), central retinal artery occlusion (one eye), and the remaining two were healthy.
Final prognosis of PED(s) with AVL were evaluated among patients with available follow-up data (20 eyes). PEDs were enlarged in eight eyes (40%) (Figures 1 and 2), and unchanged in two eyes (10%). Spontaneous resolution of the central PED with AVL was seen in four eyes (20%) (Figure 3). Rupture of the PED occurred in four eyes (20%) causing central foveolar atrophy in two (Figure 4). (20%). The comparison of the eyes with final PED rupture (n = 4) to the remaining eyes (n = 16) revealed that the PED rupture group had significantly higher mean greatest basal diameter of PED (2994.5 ± 1066.7 µm vs 1589.3 ± 846.0 µm, p = 0.011) and mean maximum height of PED (544.3 ± 249.8 µm vs 214.4 ±140.7 µm p = 0.016) at baseline. Central foveolar atrophy was seen in four eyes (%20) including two previously ruptured ones. Overall unfavorable anatomical outcome (rupture and/or atrophy) was seen in ultimately six eyes (30%).
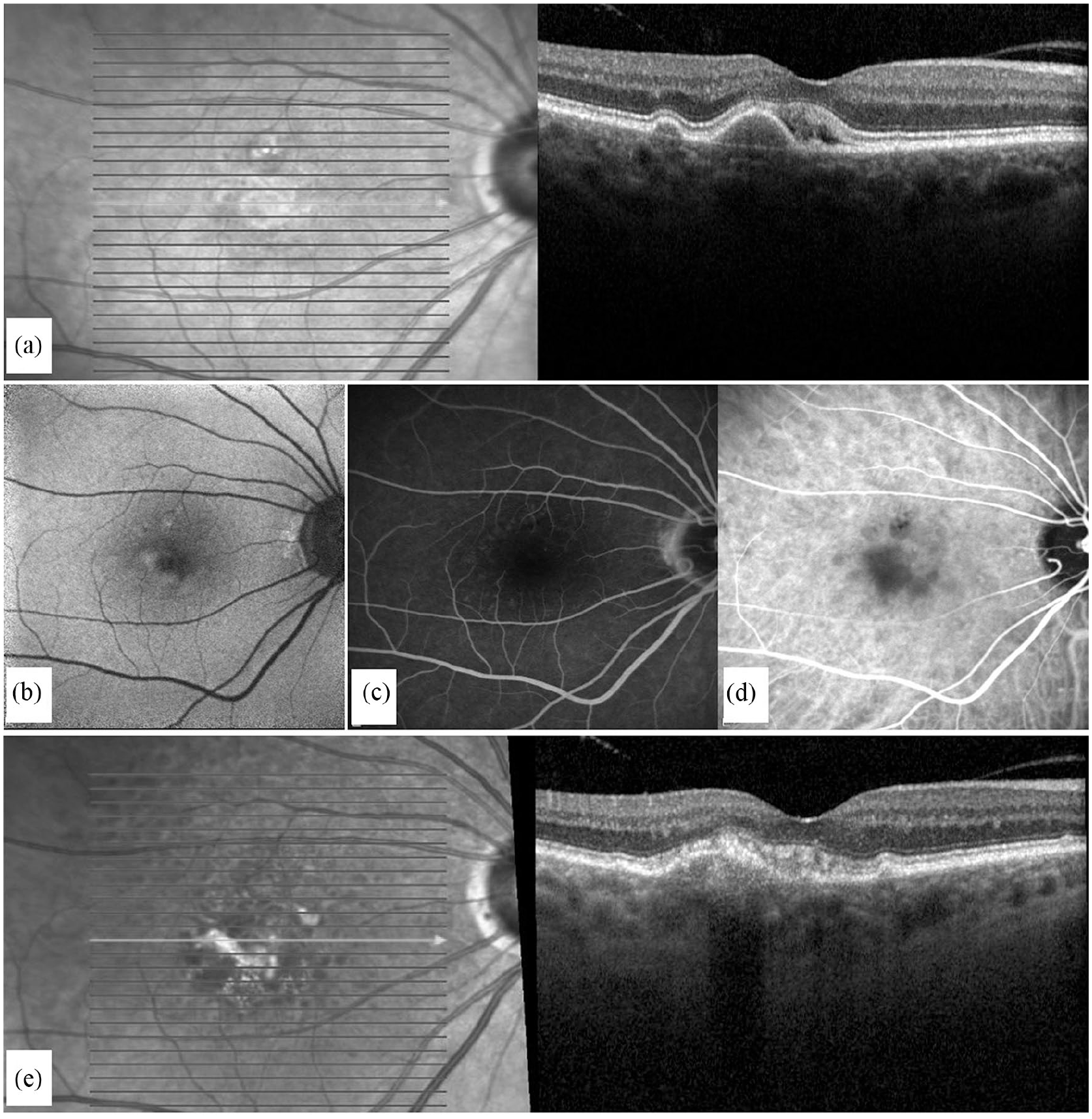
Case 2. A 69-year-old female with an acquired vitelliform lesion with multiple drusenoid pigment epithelial detachments (PEDs). At baseline, the best-corrected visual acuity was 0.1 logMAR in her right eye: (a) optical coherence tomography revealed drusenoid PEDs and hyperreflective material in the subretinal space, (b) fundus autofluorescence imaging showed hyperautofluorescence, (c) fluorescein angiography combined with (d) indocyanine green angiography did not show any signs of choroidal neovascularization and (e) at the last visit, after 66 months, the PEDs became confluent and enlarged with acquired vitelliform material in the subretinal space. Also reticular pseudodrusen formation was seen on the infrared image of OCT. Her best-corrected visual acuity decreased to 0.4 logMAR in her right eye.
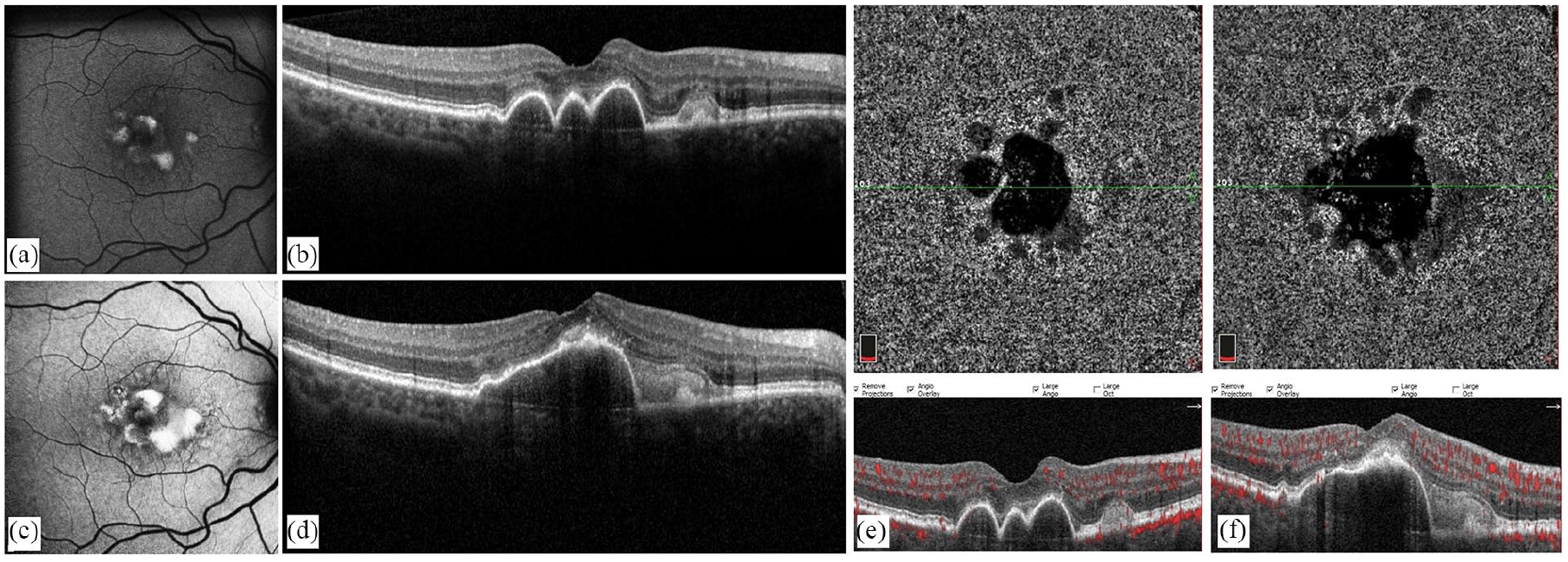
Case 6. A 67-year-old woman with an acquired vitelliform lesion (AVL) with multiple drusenoid pigment epithelial detachments (PEDs). At baseline, the best-corrected visual acuity (BCVA) was 0.1 logMAR in her right eye: (a) fundus autofluorescence (FAF) showed hyperautofluorescent areas on the posterior pole, (b) optical coherence tomography revealed centrally located multiple drusenoid PEDs and hyperreflective material in the subretinal space, (c) at the last visit, after 28 months, hyperautofluorescent areas on FAF image markedly increased, (d) the centrally located drusenoid PEDs became confluent and enlarged and the amount of the vitelliform material increased considerably on OCT and (e and f) on OCT-angiography, choriocapillaris slabs and corresponding B-scans with flow overlay did not show any sign of choroidal neovascularization at baseline and final visits. Her BCVA remained same throughout the follow-up period (0.1 logMAR).
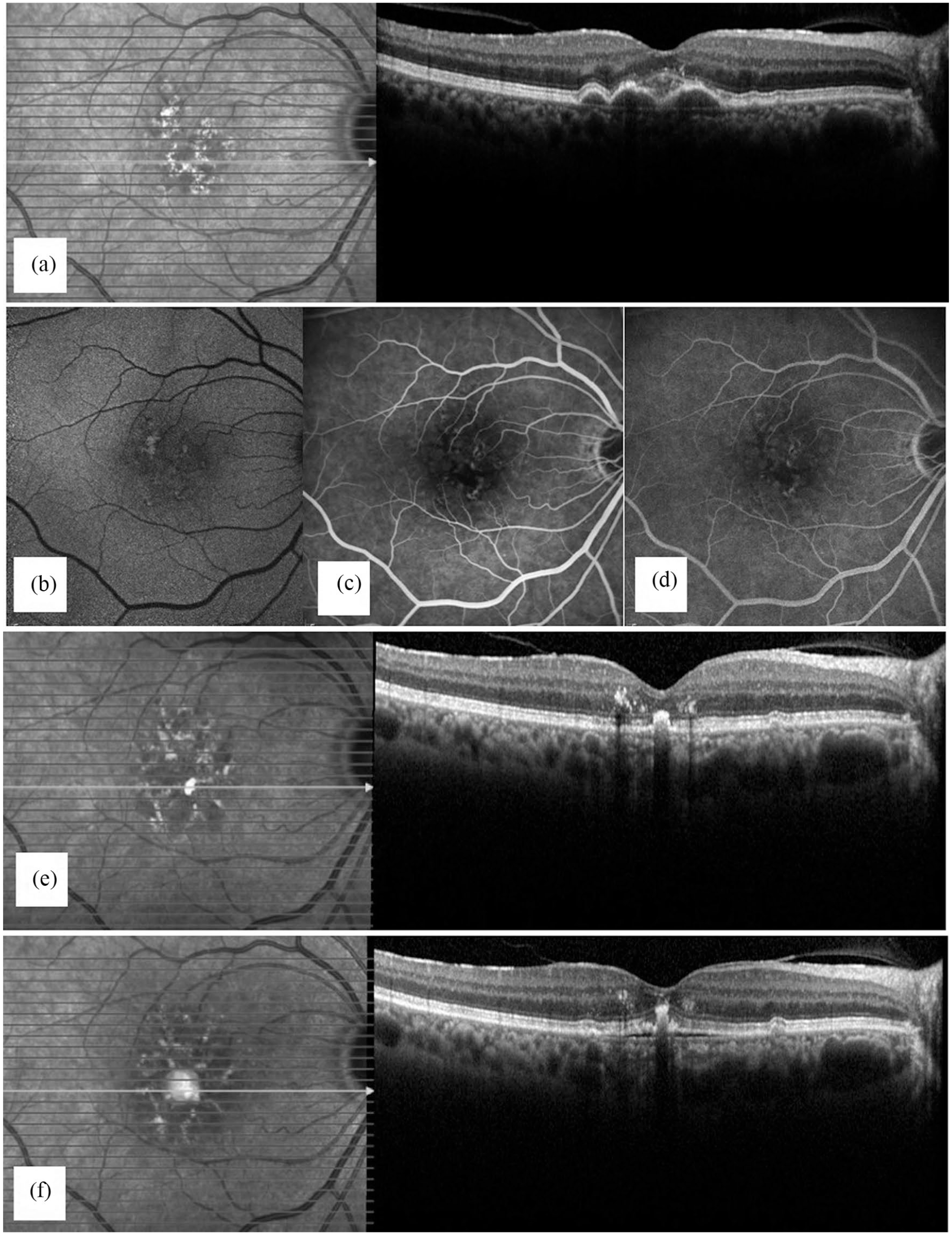
Case 4. A 68-year-old woman with an acquired vitelliform lesion with multiple drusenoid pigment epithelial detachments (PED). At baseline, the best-corrected visual acuity was 0.0 logMAR in her right eye: (a) Optical coherence tomography images revealed drusenoid PEDs and hyperreflective material in the subretinal space, (b) fundus autofluorescence showed hyperautofluorescence, (c) early, (d) late phase images of fluorescein angiography did not show any signs of choroidal neovascularization, (e) 26 months later, drusenoid PEDs disappeared and a centrally located hyperreflective focus formed on OCT and (f) at the last visit, after 32 months, a new serous PED developed under the hyperreflective focus. Her best-corrected visual acuity decreased to 0.2 logMAR in her right eye.
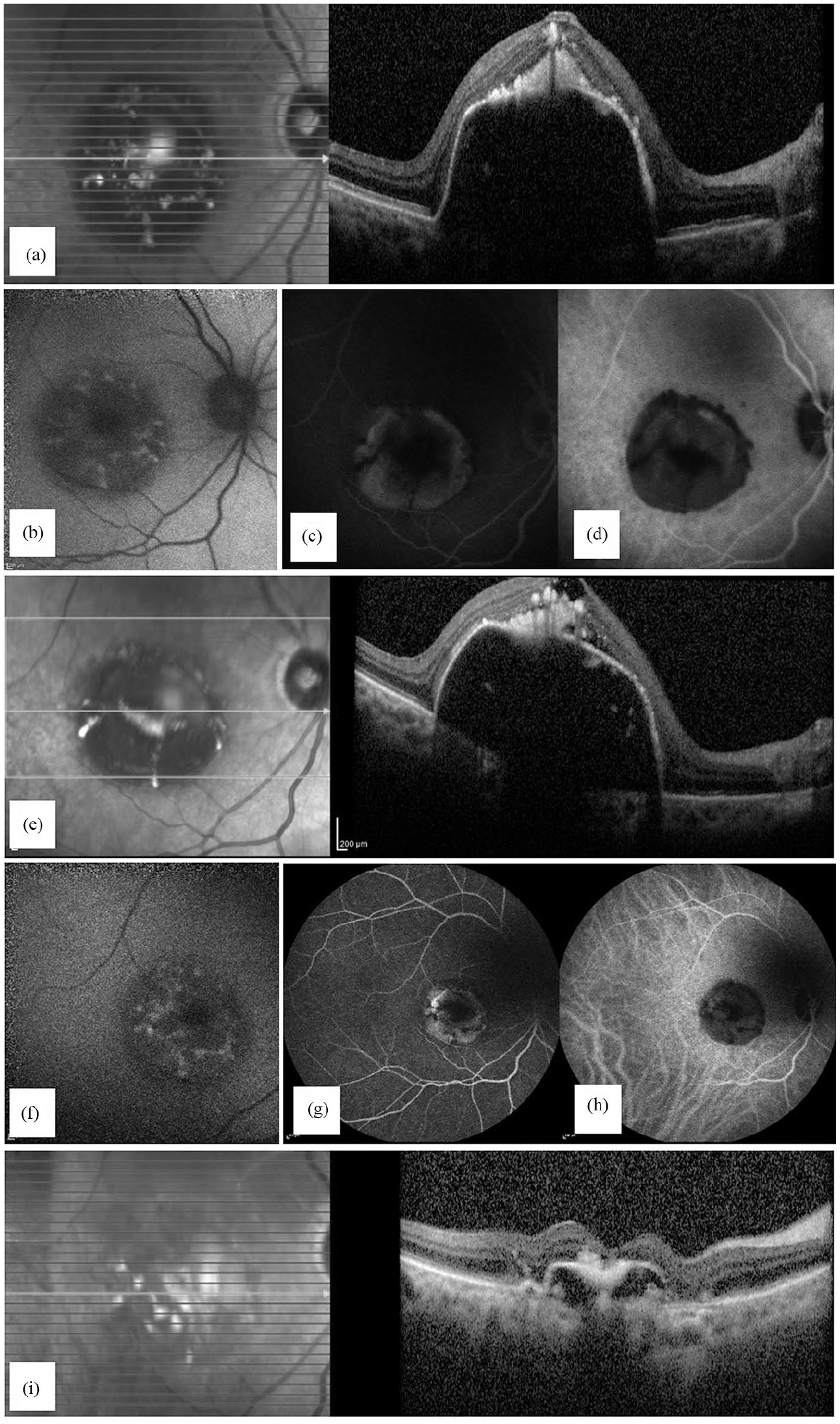
Case 3. A 61-year-old woman with an acquired vitelliform lesion with a large single seromembranous pigment epithelial detachment (PED). At baseline visit, the best-corrected visual acuity was 0.52 logMAR in her right eye: (a) optical coherence tomography (OCT) images showed hyperreflective material in the subretinal space above the large PED, (b) fundus autofluorescence (FAF) revealed a ground of hypoautofluorescence corresponding to the blockage of large PED and mottled hyperautofluorescent areas on it, (c) fluorescein angiography showed hyperfluorescence without leakage, (d) late-phase indocyanine green angiography revealed no sign of choroidal neovascularization, (e) one year later, the large PED and its associated hyperreflective material persisted on OCT and a new cystoid space occurred in the inner retinal layers, (f) FAF revealed blockage of the large PED and hyperautofluorescent material on it. Conventional dye angiographies were repeated, (g) fluorescein angiography demonstrated hyperfluorescence without leakage again, (h) late-phase indocyanine green angiography image did not show any sign of choroidal neovascularization and (i) at the last visit, 20 months after, the large PED ruptured and collapsed leading to central foveolar atrophy on OCT. Her best-corrected visual acuity decreased to 0.8 logMAR in her right eye.
The mean BCVA scores, greatest basal diameter, and maximum height of PED values throughout the follow-up period were given in Table 2. At the final visit, the mean BCVA decreased from 0.21 ± 0.16 logMAR to 0.38 ± 0.28 logMAR (p = 0.016). The mean greatest diameter of the largest PED changed from 1828 ± 972 µm to 1677 ± 1309 µm, and the maximum height of the PED changed from 278 ± 190 µm to 230 ± 280 µm (p = 0.911, p = 0.433, respectively). Subretinal fluid was present in six eyes (30%), with a mean thickness of 71.7 ± 56.5 µm (p = 0.285). Comparing to baseline values, the estimated rate of change per year was 0.068 logMAR for the BCVA, –52.55 µm for the greatest basal diameter of PED, and -13.04 µm for the maximum height of PED (Table 3).
The mean BCVA, greatest basal diameter of PED, and maximum height of PED values throughout the follow-up period.
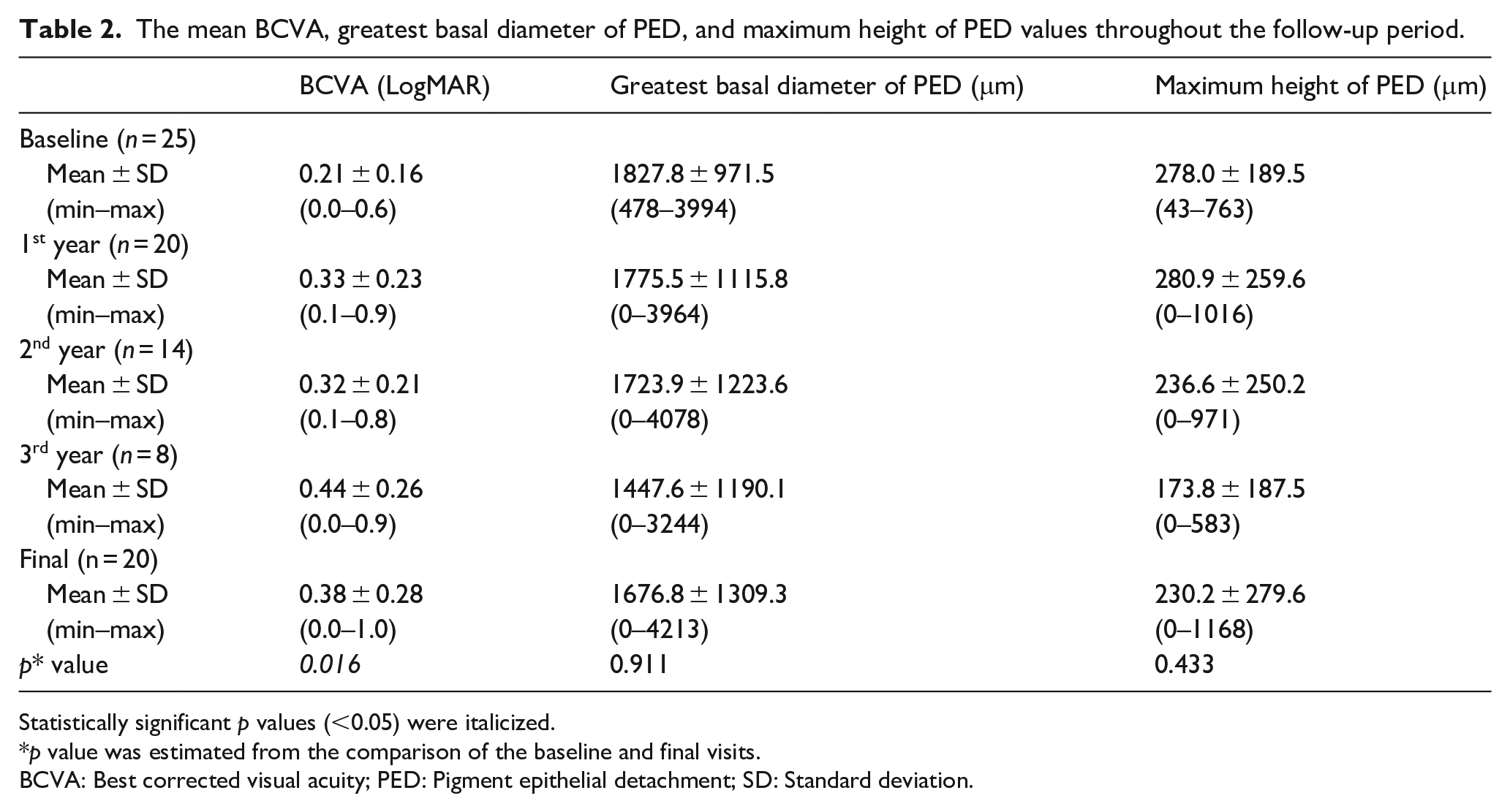
Statistically significant p values (<0.05) were italicized.
p value was estimated from the comparison of the baseline and final visits.
BCVA: Best corrected visual acuity; PED: Pigment epithelial detachment; SD: Standard deviation.
The longitudinal change rates of BCVA, greatest basal diameter of PED, and maximum height of PED measurements.
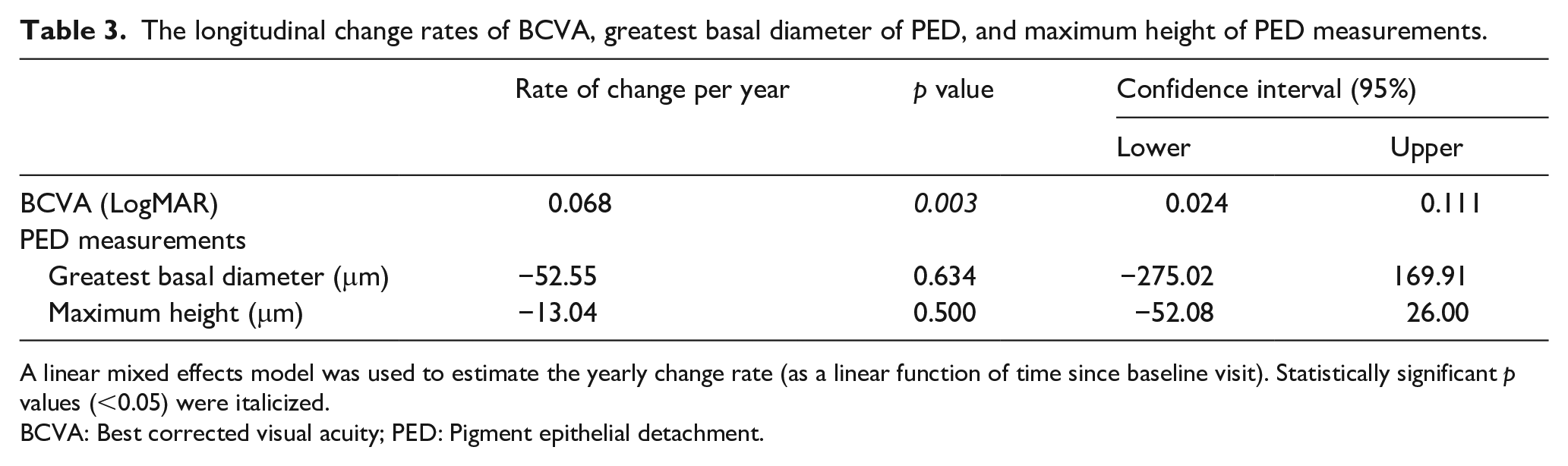
A linear mixed effects model was used to estimate the yearly change rate (as a linear function of time since baseline visit). Statistically significant p values (<0.05) were italicized.
BCVA: Best corrected visual acuity; PED: Pigment epithelial detachment.
Discussion
The natural course and pathophysiology of AVLs remain unknown. In contrast to adult-onset foveomacular vitelliform dystrophy, AVL had been reported in one study to diminish in size significantly during follow-ups; however, in that study, the AVL was accompanied by many different clinical entities. 9 The current report presents a single-center study analyzing a pure cohort of dry AMD with AVL with a mean of 33-month follow-up; which is a valuable addition to the limited data in the literature on this subject.10,11
The Age-Related Eye Disease Study (AREDS) group evaluated the natural course of drusenoid PED(s) for 5 years and estimated the rates of progression to geographic atrophy, central geographic atrophy, and neovascular AMD as 54%, 50%, and 34%, respectively. 12 However, associated AVLs were not reported in their study and their presence may alter these outcomes. Balaratnasingam et al. 11 evaluated predictors of visual outcomes in AVL and reported that foveal atrophy was present in 43.8% of the eyes with AMD-associated AVL. In our study, only 20% of the eyes progressed into central foveolar atrophy and none of the eyes developed CNV. However, should the follow-up period in our study have been even longer, the atrophy rate would have been increased because the two more eyes with PED rupture are likely to develop atrophy in time. Furthermore, at the time of the first presentation, two subjects already had central foveolar atrophy in their fellow eyes, which may have been due to a prior AMD-associated AVL which resulted in atrophy.
In the current study, spontaneous regression of the AVL associated with PED was seen in 20% of the cases. Similarly, Lima et al., 2 in a study of AVL associated with large drusen, reported spontaneous regression of material in 15% of the cases. Their study included 13 eyes of nine patients with a mean follow-up duration of 10 months. At the end of this period, the median visual acuity of the patients increased from 20/60 to 20/40. In our study, the final BCVA decreased from 0.21 ± 0.16 logMAR (approximately 20/32 Snellen line) to 0.38 ± 0.28 logMAR (approximately 20/50 Snellen line) with a mean follow-up time of 33 months. Previously, Cukras et al. 13 reported a 15-letter loss in visual acuity during the natural course of drusenoid PED associated with dry AMD at the end of a 5-year follow-up. Overall better prognosis in the presence of AVL may suggest that acquired vitelliform material or separation of RPE from the outer retina may have a protective effect on RPE preventing excessive lipofuscin deposition.
AVL may be complicated with secondary CNV.11,14 In particular, AVL associated with AMD had an increased risk for CNV development that was reported to be 12.5% in one study. 11 Because of the presence of subretinal fluid in some of the cases, particular attention should be given to the differential diagnosis. In the current study, 52.0% of eyes had subretinal fluid at the first evaluation; however, none of them had CNV. This is in line with Lima et al. 2 observing subretinal fluid in 31% of study eyes with AVL associated with large drusen. In fact, the subretinal fluid that develops in AVL may depend mostly on the effect of the vitelliruptive material or may develop depending on the RPE pump dysfunction at that side. These cases should not be misdiagnosed as neovascular AMD. Anti-vascular endothelial growth factor injections for serous PEDs associated with AVL was reported to be ineffective because the PEDs did not resolve and the visual acuity was not maintained. 10 Therefore, wasted treatments could be prevented by excluding CNV. The diagnosis of CNV associated with AVLs using FA alone can be challenging. Vitelliform material may demonstrate hyperfluorescence during the late phases due to staining of the material, and it may be misinterpreted as occult CNV. 1 For this reason, ICGA is an important imaging modality, providing visualization of the area under PEDs and AVLs. In these cases, the use of OCTA may also be limited because of the blockage effect of large PEDs. In a study evaluating the ability of OCTA to detect CNV in adult-onset foveomacular vitelliform dystrophy, the sensitivity of the OCTA was reported to be 80%. 15 Therefore, in the present study, combined FA-ICGA was needed in 36% of the eyes to exclude CNV.
We acknowledge several limitations of this retrospective study. Although the follow-up period of this study was relatively long, in some cases, definitive conclusions could not be provided for the final outcomes of the lesions that remained the same (10%) or enlarged (40%). Perhaps an even longer follow-up period would be possible, in these cases, the final version of the lesion could be changed. Also, the limited size of the study did not allow for subgroup analysis of different PEDs types associated with AVL. Further biochemical and histopathological studies are needed to explain why some of these materials disappear spontaneously, while some result in central atrophy.
In conclusion, AVL may develop on dry AMD-related PEDs. High PED size may be a potential risk factor for PED rupture during follow-up. Finally, almost 1/3 of the eyes resulted in unfavorable anatomical outcomes (rupture and/or central foveolar atrophy).
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.