
Abstract
Purpose:
To report a case of neurotrophic keratopathy (NK) in a patient affected by primary congenital glaucoma (PCG) who undergone glaucoma drainage implant surgery. NK was successfully treated with human recombinant Nerve Growth Factor (Cenegermin) eye drops.
Case report description:
A 46-years-old patient affected by primary congenital glaucoma underwent Ahmed glaucoma valve implantation in the right eye, after several unsuccessful surgeries to control intraocular pressure (IOP) since the age of three. Surgical intervention was performed without complications, and IOP was well-controlled post-operatively. However, 1 month after surgery, he developed NK with stromal ulceration, initially treated with a topical combination of preservative-free artificial tears and antibiotic ointment. As NK did not resolve, a new treatment with Cenegermin 20 µg/ml eye drops, 6 times daily, was started.
Outcome:
NK completely resolved after 8 weeks of Cenegermin treatment, with complete restoration of corneal integrity and improvement of corneal sensitivity and transparency. Visual acuity in the operated eye reverted to the pre-operative value.
Conclusion:
Cenegermin was extremely effective in restoring corneal integrity in this PCG patient with NK.
Keywords
Introduction
Neurotrophic keratopathy (NK) is a pathological condition caused by trigeminal nerve impairment, with consequent corneal sensitivity deficiency, non-healing epithelial defects, and possible stromal ulceration. Several ocular conditions have been associated with NK, namely drug toxicity, abuse of topical anesthetics, chronic ocular surface inflammation, and ocular surgery. The treatment aims to restore the corneal integrity and to stimulate nerve regeneration and epithelial turnover. 1
Medical therapy involves the use of preservative-free artificial tears, antibiotic ointment, and serum/plasma eye drops. Further therapeutic strategies include contact lens use, amniotic membrane transplantation, conjunctival flap transposition, tarsorrhaphy, and corneal surgery. 1 When conventional therapies fail to restore corneal integrity, the topical human recombinant Nerve Growth Factor (Cenegermin, Oxervate, Dompè Farmaceutici S.p.A., Milan, Italy) may be a treatment option.
We report a case of a 46-year-old patient affected by primary congenital glaucoma (PCG), who developed NK after the implantation of an Ahmed glaucoma valve in the right eye. As standard medical treatment failed, a therapy with Cenegermin eye drops was administered, which resulted in corneal integrity restoration.
Case description
A 46-years-old male patient affected by bilateral PCG referred to our clinic for uncontrolled intraocular pressure (IOP) in the right eye, despite a maximum medical therapy of a preserved prostaglandin analog (once a day) and a fixed combination of β-blocker and carbonic anhydrase inhibitor (twice a day). Ocular history included goniotomy and trabeculotomy at the age of 3 in both eyes, and a combined surgery of cataract extraction and trabeculectomy at the age of 38, in both eyes, due to uncontrolled IOP.
At first examination, best-corrected visual acuity was 0.1 and 0.3 (Snellen chart) in the right and in the left eye, respectively. Corneal diameters appeared to be increased (buphthalmos, 13.7 mm and 13.9 mm, for the right and the left eye, respectively), and central corneal thickness was 480 µm in both eyes (ultrasound pachymetry). Slit lamp examination revealed central corneal opacification, at the stroma level, more pronounced in the right eye. No deficit of corneal sensitivity was found and the blink reflex was within normal limits. IOP was 26 mmHg in the right eye and 12 mmHg in the left eye. Fundus examination revealed advanced glaucomatous optic neuropathy (vertical cup/disc ratio: 0.9, in both eyes). A superior flat bleb was evident in the right eye, while a polycystic and well-formed bleb was present in the left eye.
Due to the extensive conjunctival scarring in the right eye, the patient underwent an Ahmed glaucoma valve implantation (supero-temporal quadrant) to control IOP and prevent further progression of the disease. Intervention was performed without complications, and a regimen of a fixed combination of preservative-free betamethasone and netilmicin eye drops, 4 times daily, was prescribed (Netildex, SIFI S.p.A, Lavinaio (CT), Italy). At 1-day and 1-week follow-up examinations, IOP was 9 mmHg and 12 mmHg, respectively. Cornea epithelium was intact, and the anterior chamber was deep. The drainage tube was clearly visible within the anterior chamber, and well-positioned tangent to the iris plane.
After 1 month, the patient started to complain about ocular discomfort and blurry vision in the operated eye. BCVA progressively reduced to hand movement. Slit lamp examination revealed conjunctival hyperemia, corneal edema, and a central corneal ulcer with stromal melting, in the presence of a well-controlled IOP, digitally assessed. (Figure 1(a)) Corneal esthesiometry, performed by means of a cotton-tipped applicator, revealed complete anesthesia at the center of the ulcer, and in all the corneal and conjunctival quadrants. Therefore, a diagnosis of NK stage III was made, in accordance with the Mackie’s classification system. 1
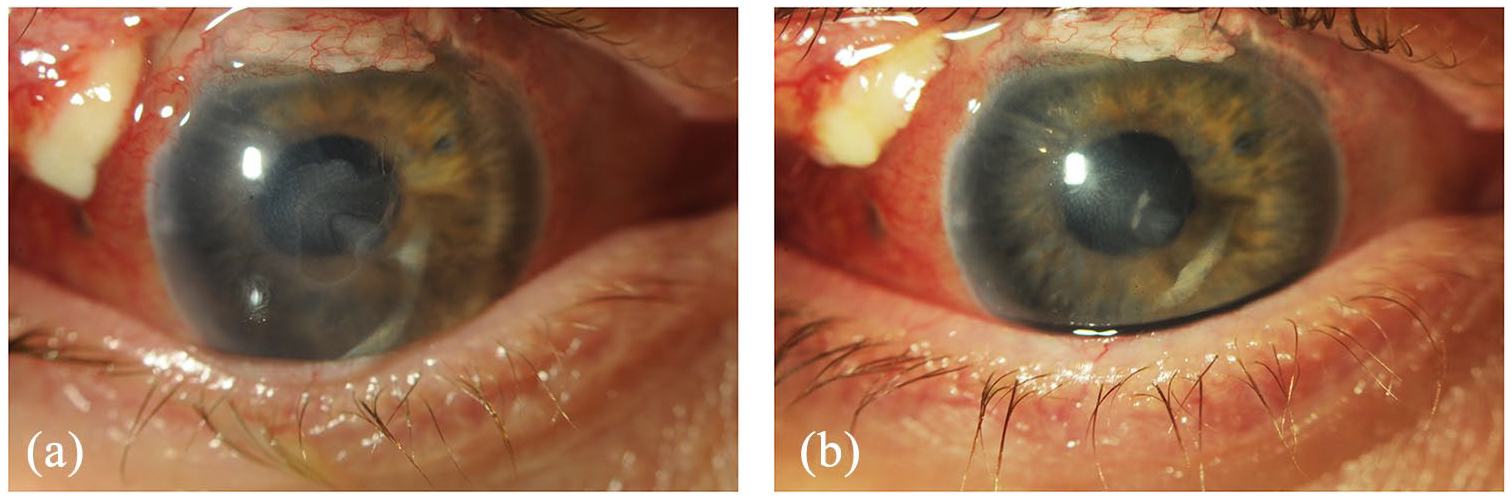
Slit-lamp photography of the patient’s right eye depicting a large corneal opacification in the interpalpebral zone before (a) and after Cenegermin eye drop therapy (b).
A topical therapy with moxifloxacin (Vigamox, Alcon, Ft. Worth TX, USA) and preservative-free lubricating eye drops was started, 6 times daily, stopping the previously prescribed therapy of a fixed combination of betamethasone and netilmicin. One week later, the clinical picture improved, with partial healing of the epithelial defect, although esthesiometry still showed a complete corneal anesthesia. However, the monthly follow-up revealed a worsening of the corneal ulcer, with deepening of the stromal involvement. Taking into account the severity of the case, and the loss of anatomic integrity, a treatment of Cenegermin eye-drops was administered, 6 times daily, for 8 weeks. The patient was monitored weekly and no side effects were reported during the follow-up period.
After 2 weeks of treatment, visual acuity was almost unchanged and corneal opacity was still evident. IOP was within normal limits (digitally assessed) and corneal sensitivity was unchanged. However, a slight improvement of the NK was noticed, with complete recovery of the corneal epithelium by week 3 (Figure 2).
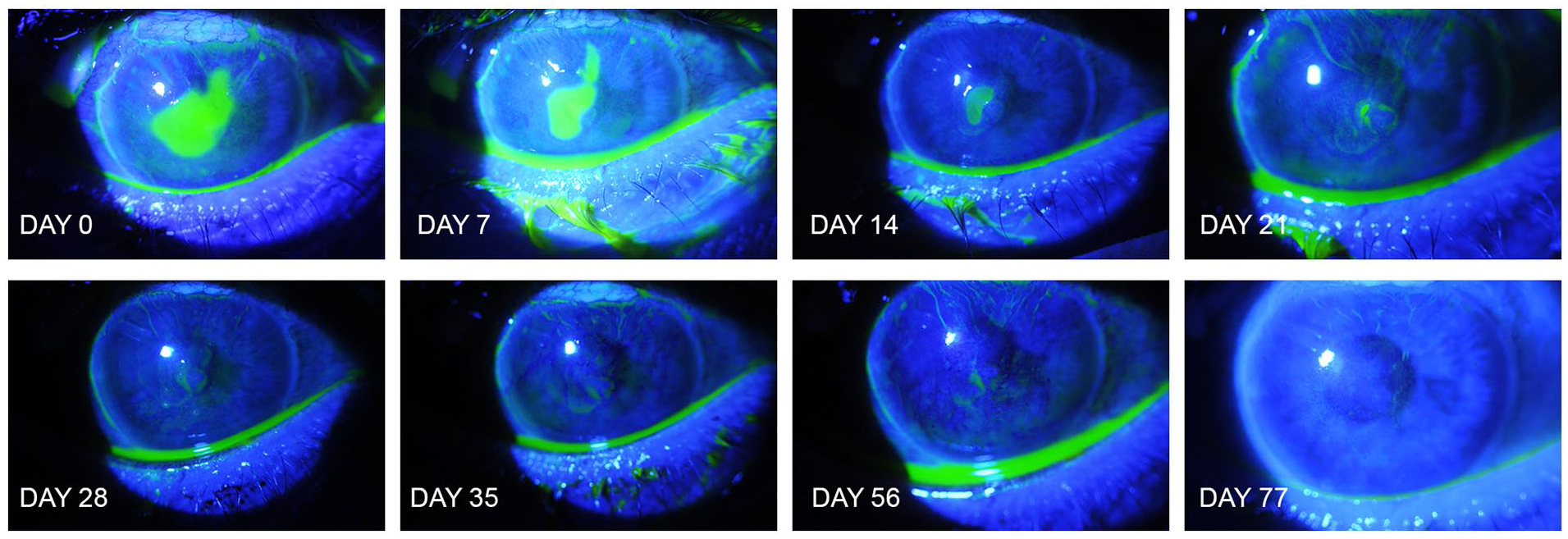
Clinical picture change over time, during the treatment with Cenegermin eye drops (fluorescein dye).
At week 6, a blink reflex was found by touching the cornea with the wisp of a cotton-tipped applicator, as the patient moved away from the examiner. Two weeks later, follow-up examination revealed an improvement of visual acuity to 0.1. The central corneal opacification previously described, linked to the glaucomatous disease, appeared less pronounced at the slit lamp (Figure 1(b)). IOP was 15 mmHg, assessed by means of Goldmann tonometry, and a blink reflex was present.
At the end of the eight-week Cenegermin treatment, a maintenance therapy with preservative-free artificial tears (4–5 times per day) was prescribed. Three months later, the corneal epithelium was still intact and IOP was 16 mmHg. (Figures 1(b) and 2)
Conclusions
Primary congenital glaucoma is a sight-threatening disease characterized by an idiopathic increase of IOP in the first years of life, resulting in optic disc damage, and impaired visual function. 2 High IOP is responsible of children’s eye elongation (buphthalmos), corneal thinning and ruptures of the corneal Descemet’s membrane (Haab’s striae), leading to progressive corneal opacification and haze.2,3
Few studies have investigated the bio-mechanical properties of a buphthalmic cornea and the histological characteristics of its anatomical layers.2–4 Mastropasqua et al., 3 using in vivo confocal microscopy, demonstrated an abnormal, convolute, “coil-shaped” morphology of corneal stromal nerves in two patients affected by PCG. Gatzioufas et al. 5 demonstrated that the corneal sub-basal nerve plexus density and the total number of nerve fibers are decreased in the cornea of young patients affected by PCG. However, corneal sensitivity of PCG patients was within normal limits in this study, likely because the decrease of corneal sensitivity appears only in the presence of a very compromised sub-basal nerve density (<835 µm per frame). 5
It has been shown that the relationship between corneal sensitivity and corneal sub-basal nerve morphology is influenced by the status of the entire ocular surface system (OSS). 6 Both medical and surgical glaucoma interventions have a detrimental effect on the OSS.1,7 However, surgically treated eyes seem to have minor OSS impairment, including the corneal sub-basal nerve stratum, when compared to medically treated eyes. Indeed, the toxic effect of preserved glaucoma medications may play a central role in corneal homeostasis modification.7,8
In our patient several factors may have contributed to the onset of NK: 1. The corneal sub-basal nerve dysfunction related to the underlying ocular disease; 2. The long-term effect of preserved glaucoma medications; 3. The impact of several intraocular surgery interventions, that is, trabeculectomy, phacoemulsification and drainage valve implant. All these factors may have had a role in the impairment of the corneal sub-basal nerve stratum, with consequent sensory deficiency.
Human recombinant Nerve Growth Factor (Cenegermin, Oxervate, Dompè Farmaceutici S.p.A, Milan, Italy) is the only treatment approved for NK, targeting the sensory nerve level of the disease. 1 Indeed, previous studies have shown that Cenegermin plays a fundamental role in corneal epithelium proliferation and has a positive effect on corneal sensory functions. Safety and efficacy of Cenegermin have been evaluated in two double-masked studies, involving 151 patients with NK, restoring corneal integrity in 70% of subjects affected by moderate/severe NK.9,10 In 11 eyes affected with NK stage II or III, Zwingelberg et al. 11 reported complete epithelial closure within 12 weeks of Cenegermin treatment, with long-term improvements in vision and corneal sensitivity.
In our patient, complete and persistent corneal epithelium healing was achieved 3 weeks after the beginning of treatment, with significant improvements of corneal sensitivity. Interestingly, a mild clearing of the previous congenital corneal opacity was also noticed, that contributed to the improved final visual acuity. As previously suggested, 12 loss of corneal transparency and modifications of corneal tissue homeostasis in buphthalmic eyes may be related, at least partly, to a reduced corneal sub-basal innervation. It is less likely, although it cannot be ruled out, that the corneal clearing was due to the IOP decrease after surgery, in a not completely competent cornea.
To the best of our knowledge, this is the first report of NK in a patient affected by PCG and treated with Cenegermin. Cenegermin was extremely effective in restoring the corneal anatomy and the epithelium integrity. Further studies are needed to better investigate the effects of human recombinant Nerve Growth Factor on the corneal nerves, and to understand its role in the epithelium proliferation and the keratocyte homeostasis, often compromised in eyes affected by PCG.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.