
Abstract
Background
The use of atropine during dobutamine stress echocardiography (DSE) is contraindicated in persons with narrow angle glaucoma though there is limited evidence that low doses of intravenous atropine do not cause pupillary dilation.
Objective
The aim of this study is to investigate whether atropine when administered in persons without glaucoma during dobutamine stress echocardiography causes pupillary dilation.
Methods and Results
Out of 144 patients without a history of glaucoma referred for DSE for clinical indications, 105 patients received intravenous atropine doses ranging from 0.1 mg to 1.25 mg (most patients received 0.25–0.75 mg). Pupil diameter of both eyes was measured under the same light conditions before and after the DSE using a CP-30 Optical Digital PD Ruler. For the total of 210 examined eyes pupil diameter remained unaltered after each DSE test (3.65 ± 0.799 mm before vs 3.63 ± 0.766 mm after, p = .737). Similarly, pupil diameter remained unchanged when left and right eyes were assessed separately (right eye: 3.770 ± 0.812 before vs 3.752 ± 0.745 mm after, p = .821 and left eye: 3.521 ± 0.770 before vs 3.499 ± 0.770 mm after, p = .806). Diameter of right and left pupil were also unaltered after grouping patients by sex and iris pigmentation. Age, weight, atropine dose and propranolol dose were not correlated with changes in pupil diameter.
Conclusion
Intravenous atropine in usual doses administered in DSE does not cause mydriasis in adults without glaucoma. Future studies need to confirm our findings and expand the investigation regarding safety of atropine use during DSE in patients with narrow angle glaucoma.
Highlights
Atropine in dobutamine stress echocardiography reduces number of inconclusive tests.
In patients with narrow angle glaucoma intravenous atropine is contraindicated.
Some studies suggest that intravenous atropine is safe in narrow angle glaucoma.
In this study it is shown that IV atropine at usual doses does not cause mydriasis.
Introduction
Atropine is commonly used intravenously in selected patients during dobutamine stress echocardiography (DSE). The addition of atropine in DSE has many advantages: atropine enhances sensitivity for ischemia detection 1 being especially useful in patients with single vessel disease, 2 and is particularly helpful in reducing the number of inconclusive tests in patients receiving β-blockers. 3 Early administration of atropine reduces test time, 4 and results in lower incidence of minor adverse effects compared with the conventional protocol in the elderly, which presented adequate cardiac chronotropic responsiveness to early injections of atropine, requiring lower doses of drugs to reach test end points. 5 Also, a non-standard protocol where 1 mg of atropine is administered before the infusion of dobutamine has been proposed as safer in older people than the conventional protocol. 6
According to current guidelines, dobutamine is usually delivered at a starting dose of 5 mcg/kg/min and up-titrated at 3-min intervals to 10, 20, 30 and 40 mcg/kg/min. 7 Atropine can be either added to the latter stage of 40 mcg/kg/min in case of failure to achieve target heart rate, 7 or co-administered with dobutamine doses of 20 or 30 mcg/kg/min, particularly if heart rate does not increase accordingly. 7 Specifically, the American Society of Echocardiography (ASE) Guidelines, recommend 0.25 to 0.50 mg of atropine at 1 min intervals as needed to achieve target heart rate, to a total of 1.0 to 2.0 mg, 7 while the British Society of Echocardiography (BSE) recommend doses of 0.3 mg of atropine up to a total of 1.2 mg as needed. 8
As an anticholinergic agent, atropine causes mydriasis, and in patients with predisposing factors it can cause drug-induced acute angle closure glaucoma. 9 Therefore, according to the European Association of Echocardiography (EAE) and BSE guidelines atropine is contraindicated for stress echocardiography in patients with closed-angle glaucoma patients. 10
However, evidence suggests that atropine administered intravenously in doses of 0.4 to 0.6 mg does not affect pupil size, 11 and therefore it is not contraindicated in patients with glaucoma. 12 Furthermore, conventional doses of atropine during cardiac arrest in children have been shown to cause minimal pupillary dilation. 13 Moreover, intramuscular dose of atropine up to 0.6 mg administered preoperatively has been found to be safe even in patients with glaucoma, and that eye drops of miotic agents, such as pilocarpine or physostigmine should be used to counteract the potential mydriatic effect of atropine. 14
Though atropine is very well known for its mydriatic effect in the form of eye drops, the published evidence regarding the effect of intravenous atropine in pupil diameter is limited and based in small populations.
Given the discrepancies between the guidelines and reported studies, the aim of the present study was to investigate the effect of atropine on pupillary dilation when administered in persons without glaucoma during DSE.
Methods
This observational study includes patients who were referred to a medical diagnostic center (“Kosmoiatriki”) from 01/2020 until 02/2021 for DSE. All participants signed an informed consent permitting the use of their data for research purposes. Furthermore, all data processed in the study were anonymized. The study protocol was approved by the medical diagnostic center ethics committee (decision date 12–12–2019, decision number 2019/3).
Patients with known glaucoma – either open or closed angle – and those taking a1-adrenergic receptor antagonists, finasteride, benzodiazepines or antipsychotics were excluded from the study. Because of the fact that narrow angle can be asymptomatic, patients were subjected to slit-lamp examination and gonioscopy before being included in the study population. Regarding slit-lamp examination Van Herick system was used to estimate the width of the angle, patients with grades 3 and 4 were used in the study. Additionally, gonioscopy using Spaeth grading system was performed and patients with anterior or posterior synechiae and plateau iris configuration were excluded from the study.
Pupil measurements were performed with all patients in the same position in the examination room before and after DSE under mesopic illumination conditions. The illumination provided in the examination room was only from artificial light (no windows or open doors). Additionally, in order to verify mesopic illumination conditions, a light meter (Mastech MS6612) was used at the position of the patient's eyes and a measurement of 29 Lux was obtained.
It is noteworthy that the pupil measurements were conducted at least 15 min after the DSE to ensure the elimination of dobutamine in bloodstream (half-life of intravenous dobutamine is 2 min. 15 ) In both measurements (before and after DSE test) each patient remained in the same lighting conditions at least 10 min. Pupil diameter was measured in both eyes using a CP-30 Optical Digital PD Ruler. To enhance measurement accuracy, the image of each eye and the instrument marker was magnified using a mobile phone camera. This allowed for accurate identification of the pupil border, which was not always clearly distinguishable in mesopic illumination conditions, especially in cases of dark colored eyes. In case of inaccurate result, for example if head or eye movement occurred, the measurement was repeated.
Iris pigmentation was classified into three categories: “Dark”, “Intermediate” and “Light” defined as follows:
Dark: Black-Brown iris, Dark brown iris, Brown iris. Intermediate: Light brown iris, Hazel Iris, Green brown iris, Green iris. Light: Dark gray iris, Light gray Iris, Blue iris, Light blue iris.
Atropine dose during DSE was individualized according to heart rate progression in each patient. In the recovery phase, individualized dose of intravenous propranolol was administered in all patients to restore heart rate to levels <90 beats/min.
Patient selection and methodology are being summarized in Figure 1.
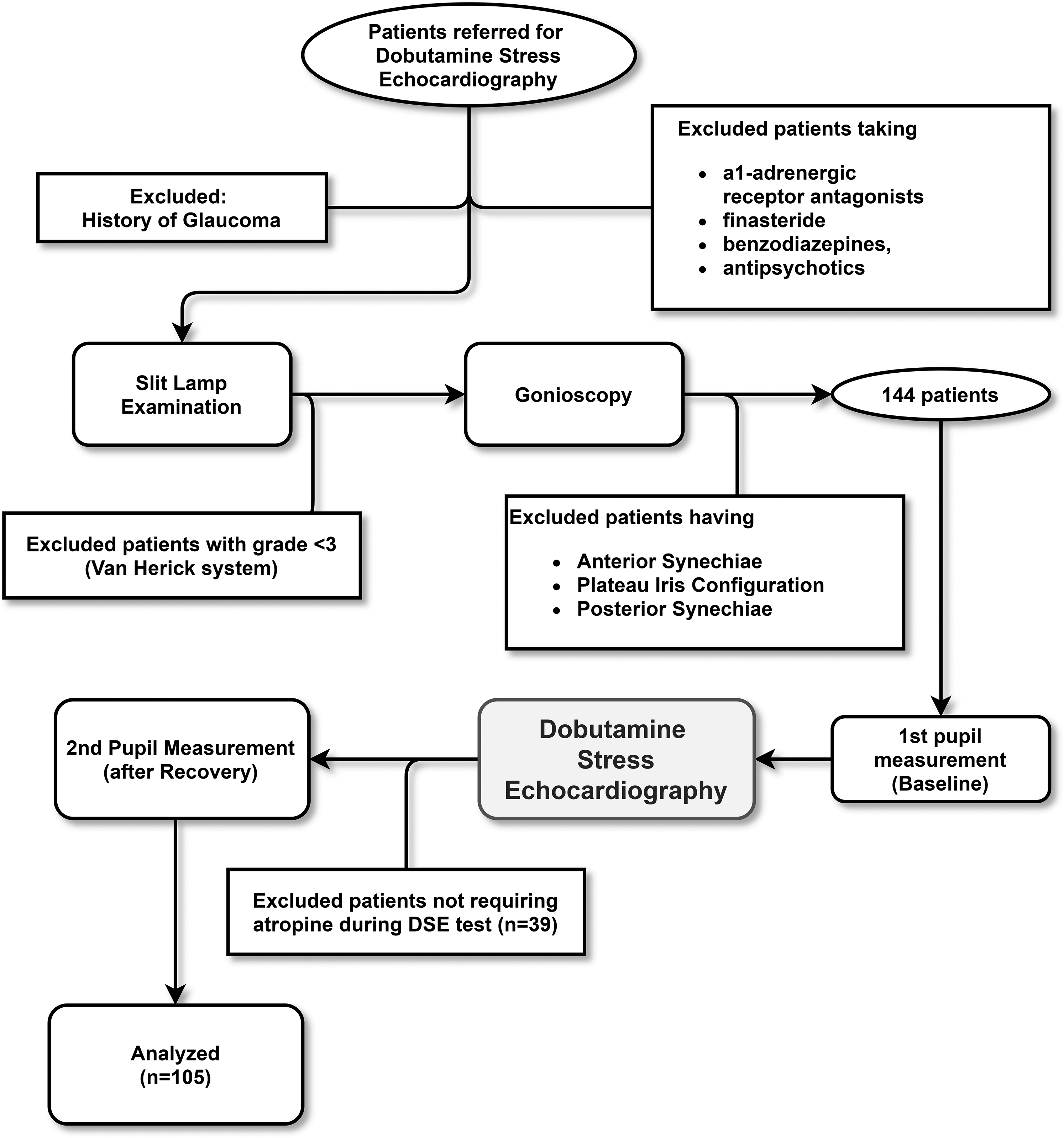
Methodology flowchart.
Statistics
Normal distribution of continuous variables was assessed graphically by histograms, and statistically using Kolmogorov-Smirnov test Correlations between continuous variables were examined by Pearson correlation coefficients. Differences in pupil diameters before and after DSE were evaluated by paired-samples Student t-test Statistical significance was defined as p < .05. Statistical analysis was performed using IBM SPSS Statistics software version 25 (IBM Corp., Armonk, NY, USA).
Results
Out of 144 consecutive patients who underwent DSE, 39 did not require atropine during the test, and they were excluded from the study. The characteristics of the 105 participants are reported in Table 1.
Characteristics of population included in the study.
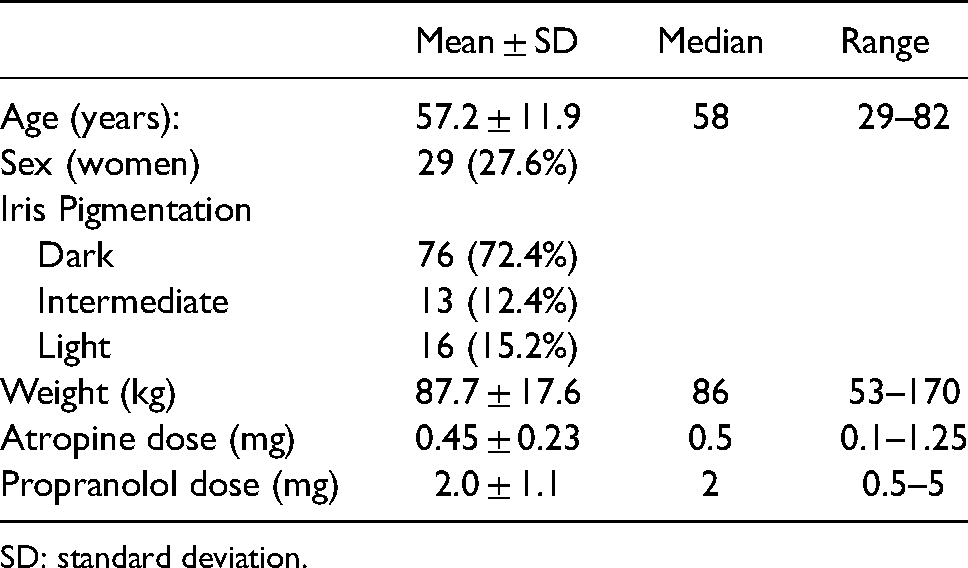
SD: standard deviation.
The pupil diameters of the 210 eyes examined were normally distributed (Figure 2), with a test value of 0.066 (p = .313, Kolmogorov-Smirnov test). The baseline diameter of the pupils remained unaltered after the DSE in all examined eyes (n = 210): 3.65 ± 0.799 mm before vs 3.63 ± 0.766 mm after DSE (p = .737) (Figure 3). This observation was also consistent when the pupil diameter of each eye was considered separately; right eye: 3.770 ± 0.812 before vs 3.752 ± 0.745 mm after the DSE (p = .821) and Left eye: 3.521 ± 0.770 before vs 3.499 ± 0.770 mm after the DSE (p = .806) (Figure 3).
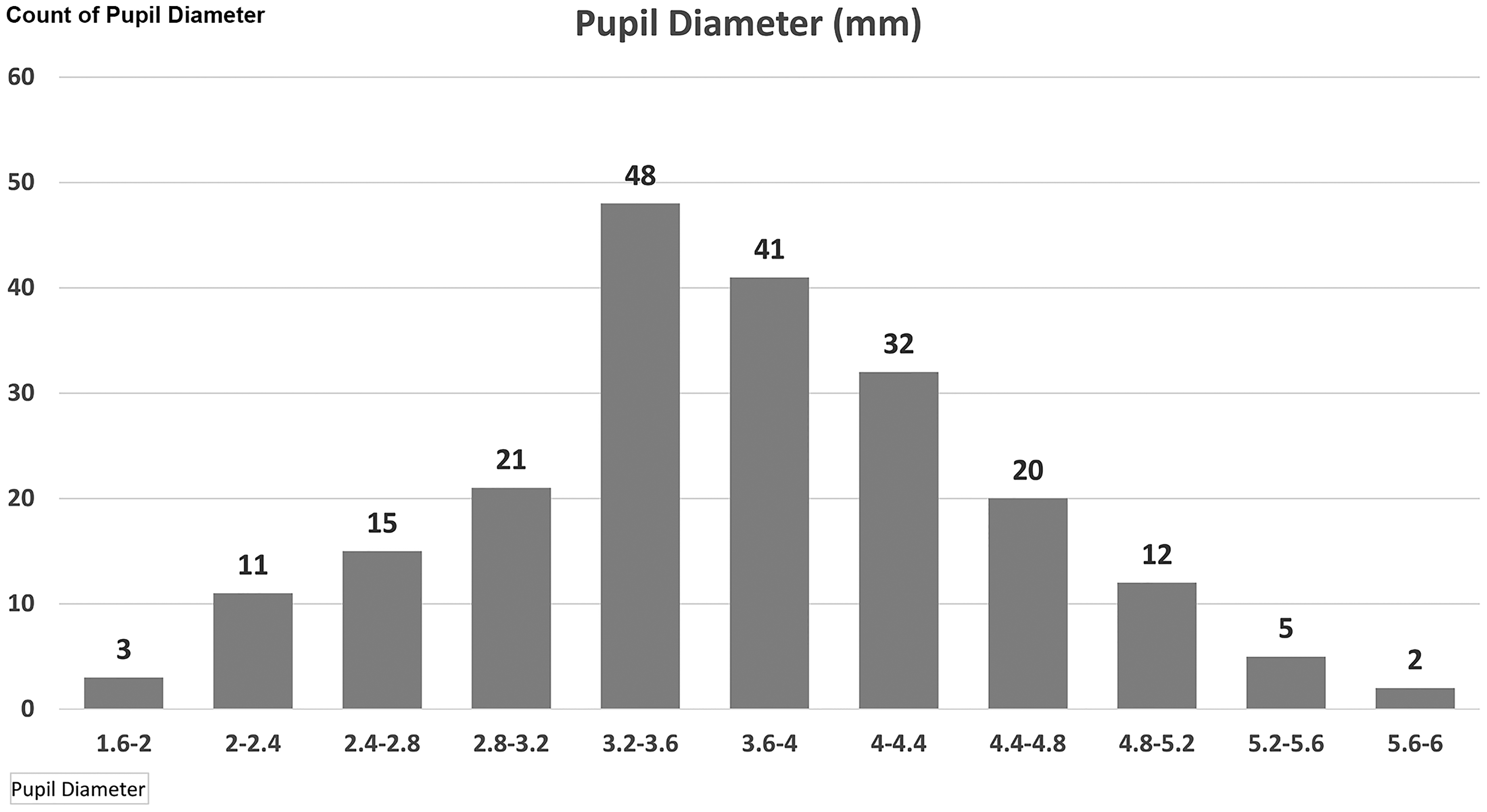
Pupil diameter in millimeters.
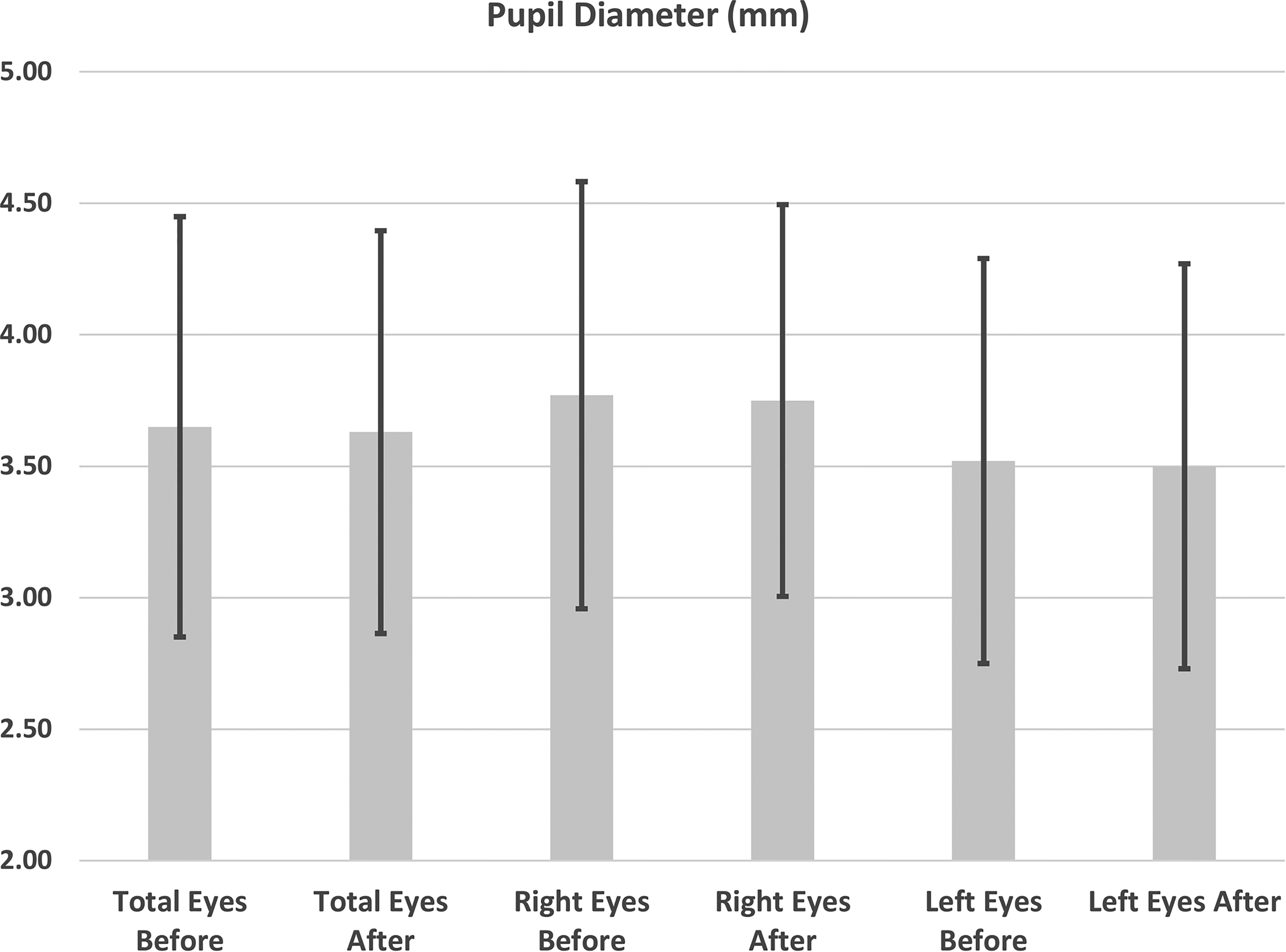
Pupil diameter before and after the DSE examination.
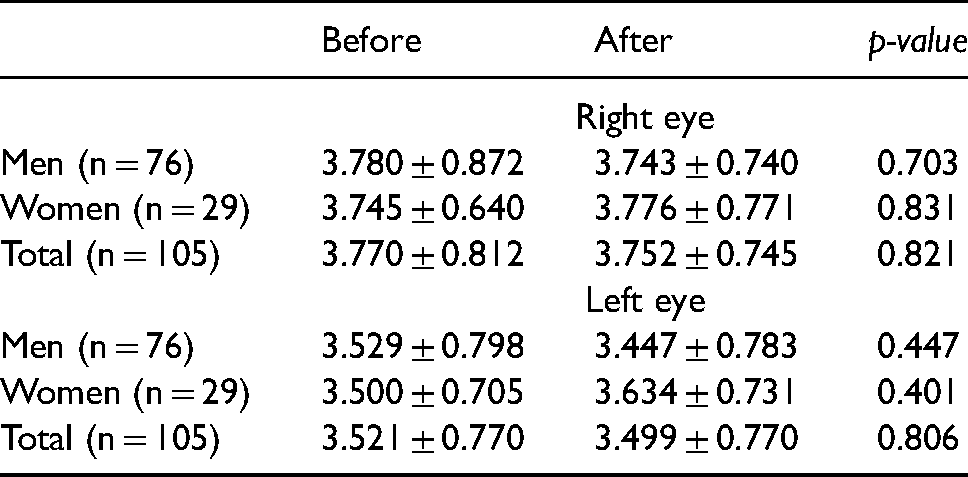
The results were consistent when men and women were considered separately (Table 2 and Figure 4), and regardless of the category of iris pigmentation (dark, intermediate, light), as shown in Table 3 and Figure 5.
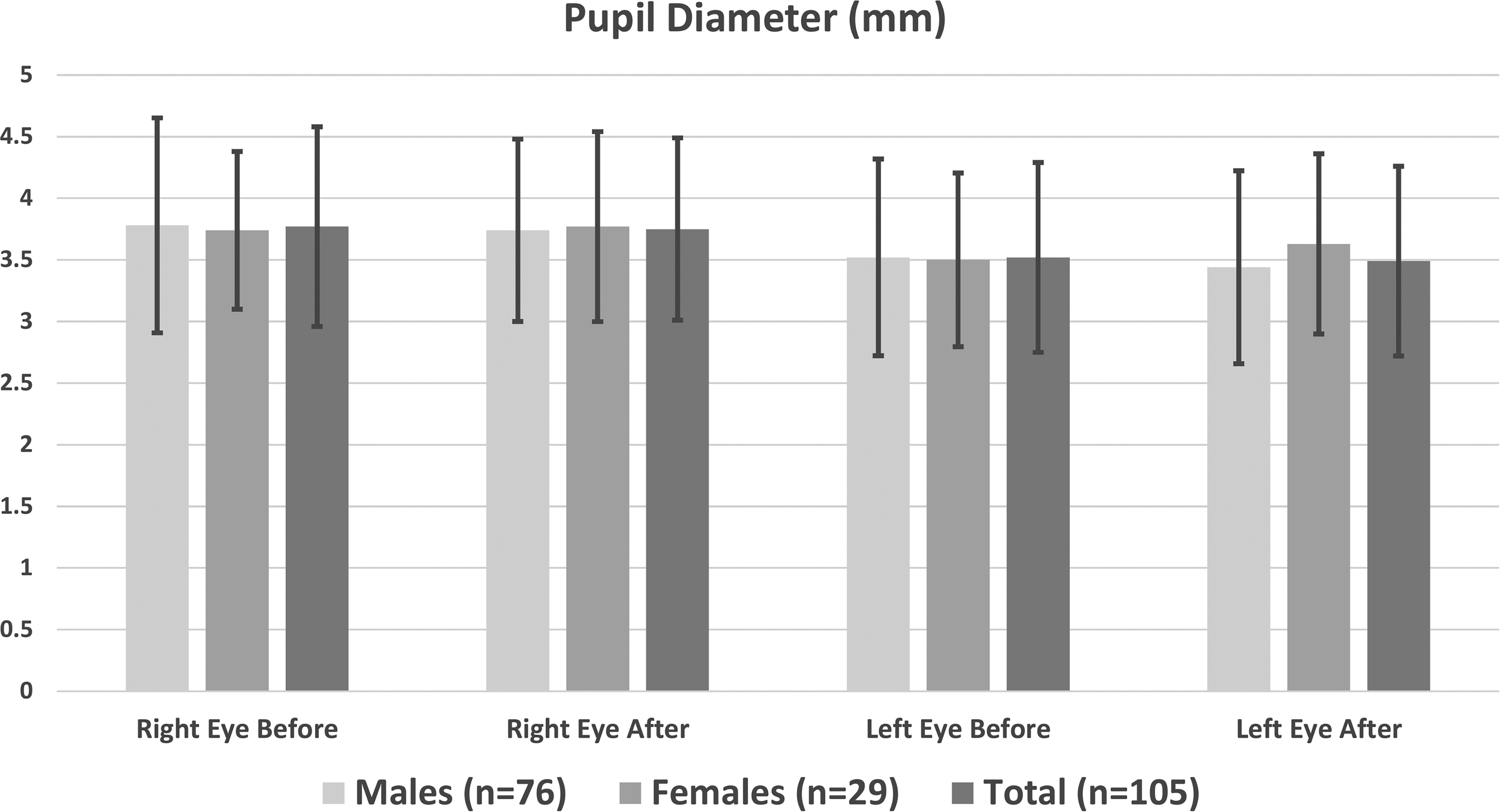
Pupil diameter of left and right eyes before and after the DSE examination in men and women separately.
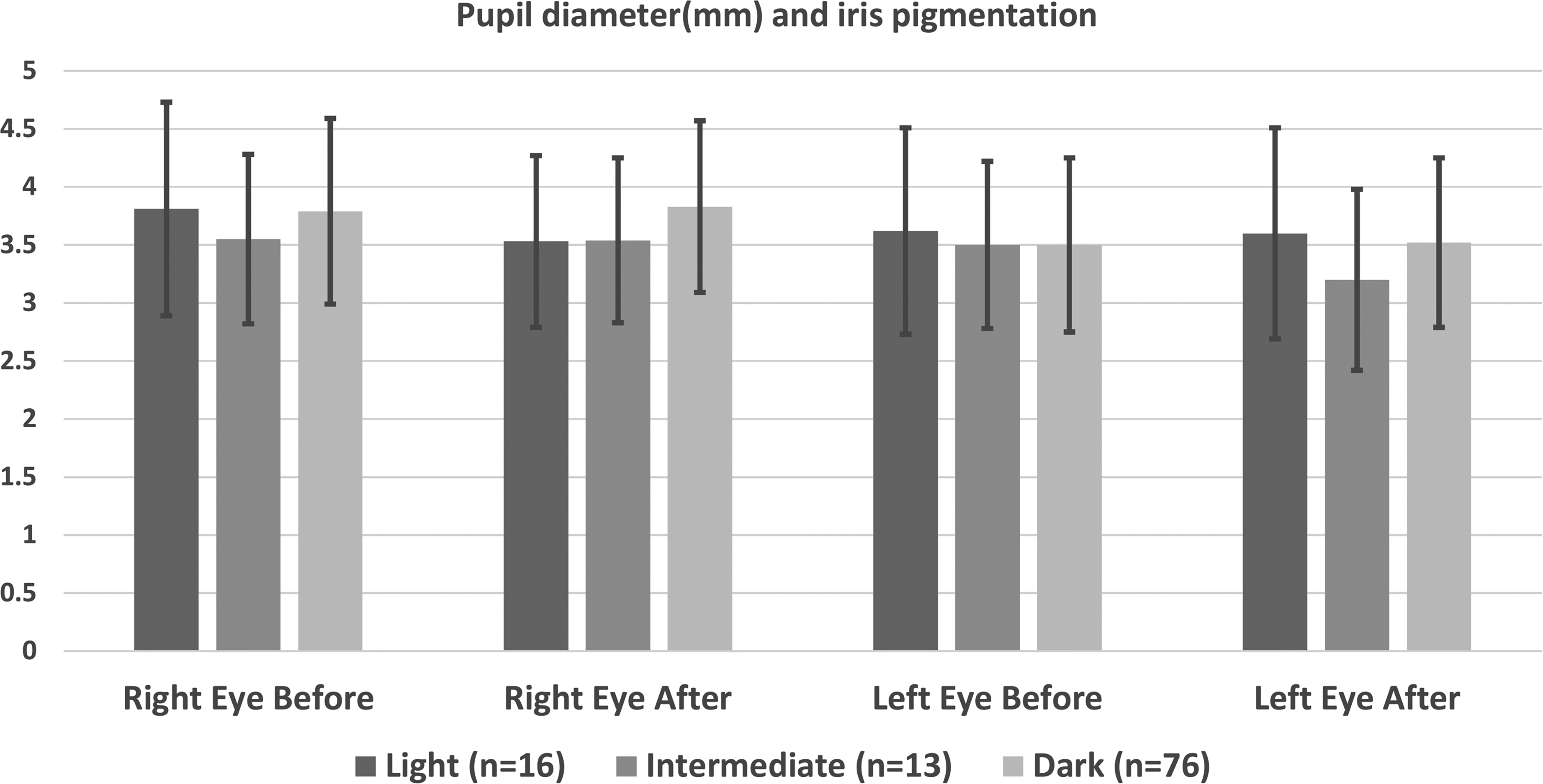
Pupil diameter of left and right eyes before and after the DSE examination in the three iris pigmentation categories.
Right eye and left eye pupil diameter comparison in men and women before and after the DSE examination.
Pupil diameter comparison before and after the DSE examination according to the iris pigmentation category.
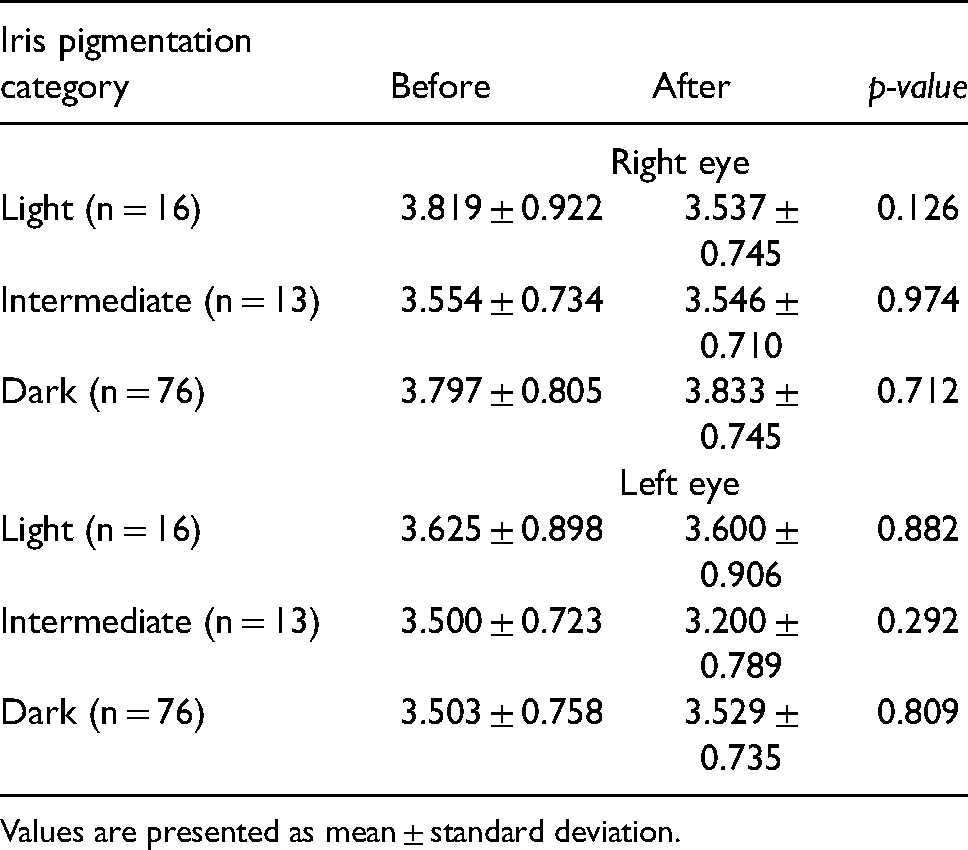
Values are presented as mean ± standard deviation.
Furthermore, no significant correlations were noted between changes in pupil diameter and age, weight, atropine dose, and propranolol dose, as shown in Table 4.
Pearson correlation between absolute pupil diameter change and age, weight, dose of atropine, and dose of propranolol.
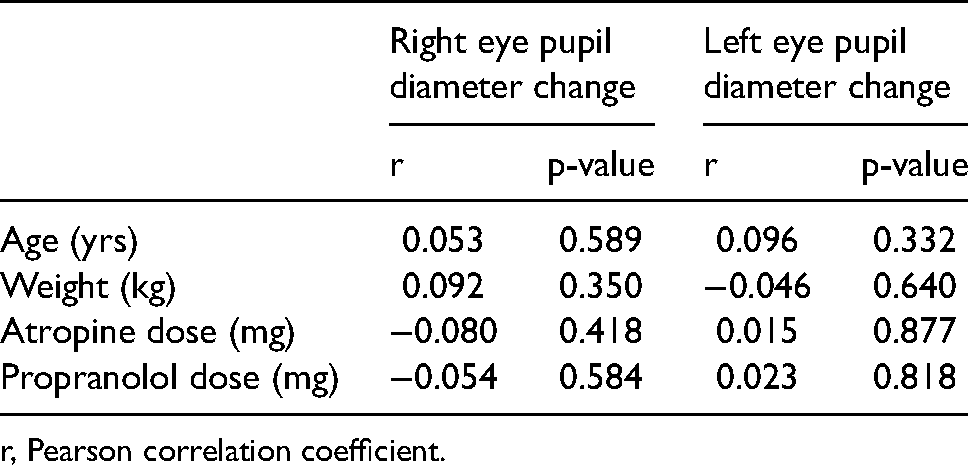
r, Pearson correlation coefficient.
Discussion
This study provides novel insight on whether atropine use in DSE can cause changes in pupil diameter in people without glaucoma.
The normal pupil size in adults varies from 2 to 4 mm in diameter in bright light to 4 to 8 mm in the dark. 16 In DSE besides dobutamine, atropine and β-blockers (propranolol in this study) are used as needed to induce appropriate heart rate increase and in the recovery phase, respectively. Pupil dilation mechanism is being mediated via α1-adrenergic receptors. 17 Dobutamine is a β1 selective agonist with minimal α-adrenergic effect, and mydriasis is being mentioned in animals in case of overdose toxicity. 18 Propranolol blocks β1 and β2 adrenergic receptors and it is considered a weak α-adrenoreceptor agonist; 19 pupil dilation has been noted only in cases of overdose. 20
Regarding atropine, it induces mydriasis by its antimuscarinic effect. Iris pigmentation influences the rate and degree of pupillary response to dilating agents. Dark eyes do not dilate as fast or as well as light-colored eyes, but the effect lasts longer. 21 The effect of atropine on pupil size is observed when eye drops are used even in low dose solutions (0.01% and 0.005%, whereas as a mydriatic is being used in concentration of 1%). 22
Evidence regarding intravenous atropine use in narrow angle glaucoma is conflicting. Stress Echocardiography guidelines recommend against atropine use in patients with glaucoma, 10 but other studies state that it is not contraindicated and can safely be used in doses up to 0.6 mg, 11 while some authors suggest prophylactic use of a miotic agent before atropine administration. 14
Typically, atropine is administered in bolus doses of 0.25 mg with a range of 0.25–0.75 mg commonly used in clinical practice. In our study the mean atropine dose used during the DSE test was 0.45 ± 0.23 mg. We have demonstrated that the drugs administered (atropine and propranolol) at each DSE test did not have any significant effect on pupil diameter (measurements were performed after the elimination of dobutamine from bloodstream). Most probable explanation is that atropine induces mydriasis in larger doses (e.g. more than 2 mg), and that during a typical DSE study the dimming of the examination room lights has a more potent effect on pupil diameter than the drugs administered.
These results need to be confirmed by future studies in order to establish safety of atropine during DSE, particularly in patients with narrow angle glaucoma. Furthermore, the preventive use of pilocarpine eye drops could be possibly assessed as a feasible safety measure (miosis starts in 10–30 min, with maximal effect within 30 min and usually persists for 4–8 h). 23
Ιt would be interesting to investigate the influences of DSE atropine use on changes in anterior segment geometry like central and peripheral anterior chamber depth by ultrasound biomicroscopy or anterior segment OCT biometry. Based on studies performed so far after topical instillation of atropine eye drops, there is an increase in the depth of the anterior chamber due to cycloplegia and relaxation of the radial muscle.24–27
Limitations
There are limitations in this study. First, eye measurements were not performed by independent observers but from a single, though trained, operator. Second, it would be preferable if pupil diameters were measured at baseline after the lights were dimmed, before the administration of the first dose of atropine, at peak stress phase (after administration of atropine), and at the recovery phase after the end of β-blocker administration. Third, accurate pupillary measurements in dark environment require an infrared pupillometer, which was not available. Furthermore, DSE requires continuous monitoring of the patient, and thus eye measurements in the middle of the procedure would be an inconvenient distraction.
Conclusions
Intravenous atropine, in usual doses administered in DSE does not cause mydriasis in adults without glaucoma. It remains to be investigated whether atropine use during DSE in patients with narrow angle glaucoma is safe; further studies are needed to investigate this topic.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.