
Abstract
Purpose
To describe a previously unreported posterior pseudo-lenticonus sign in a patient with nipple cone keratoconus (KC).
Case report
A 32-year-old female presented with complaints of right eye visual acuity loss. Although she was initially diagnosed with posterior lenticonus, the additional clinical evaluation revealed no true lenticonus. The corneal topography revealed a central nipple cone KC, and the crystalline lend finding was consistent with a pseudo-lenticonus.
Conclusion
Due to inadvertent visual effects, nipple cone KC may resemble posterior lenticonus.
Introduction
Keratoconus (KC) can be diagnosed through clinical findings along with direct and indirect imaging technologies. 1 However, when KC is not advanced and the cornea is clear, this abnormality may be mistaken for another before topographic imaging reveals the actual abnormality. 1
A novel posterior pseudo-lenticonus sign in a patient with nipple cone KC is introduced in this article, not previously stated in any related literature. The pseudo conditions are distinct from the original diseases in terms of etiology, treatment, and prognosis, but similar conditions occur in the exact location due to unrelated conditions.
The purpose of this report is to describe a novel diagnostic sign that may be used in cases of apparent posterior lenticonus protrusion.
Case presentation
A 32-year-old female presented with complaints of right eye visual acuity loss in a gradual pattern. On examination, the patient's uncorrected distance visual acuity (VA) was 20/80 and was not corrected. A signed statement of informed consent was obtained from the patient to publish her personal data.
The right crystallin lens had a remarkable conical protrusion that resembled a posterior lenticonus upon slit-lamp biomicroscopy examination (Figure 1). Examinations of the posterior vitreous and posterior pole fundoscopy were unremarkable. Rotating Scheimpflug imaging (Pentacam®; Oculus, Wetzlar, Germany) revealed a central ectasia, consistent with nipple KC (Figure 2). After fitting rigid gas-permeable (RGP) lenses, the conical posterior bulging was eliminated (Figure 3), and the corrected distance visual acuity improved to 20/30. The Scheimpflug image (without the RGP lens) revealed the lens's standard posterior border (Figure 4). Thus, while a lenticonus-like shape is noted on slit-lamp examination, it was possible that was not a true lenticonus; and a nipple KC as a pseudo-lenticonus sign should be considered.

Examination of biomicroscopy using a slit lamp. The right lens exhibited a conical protrusion similar to that of a posterior lenticonus.

Scheimpflug imaging revealed a central corneal cone in the right eye, consistent with nipple cone KC.
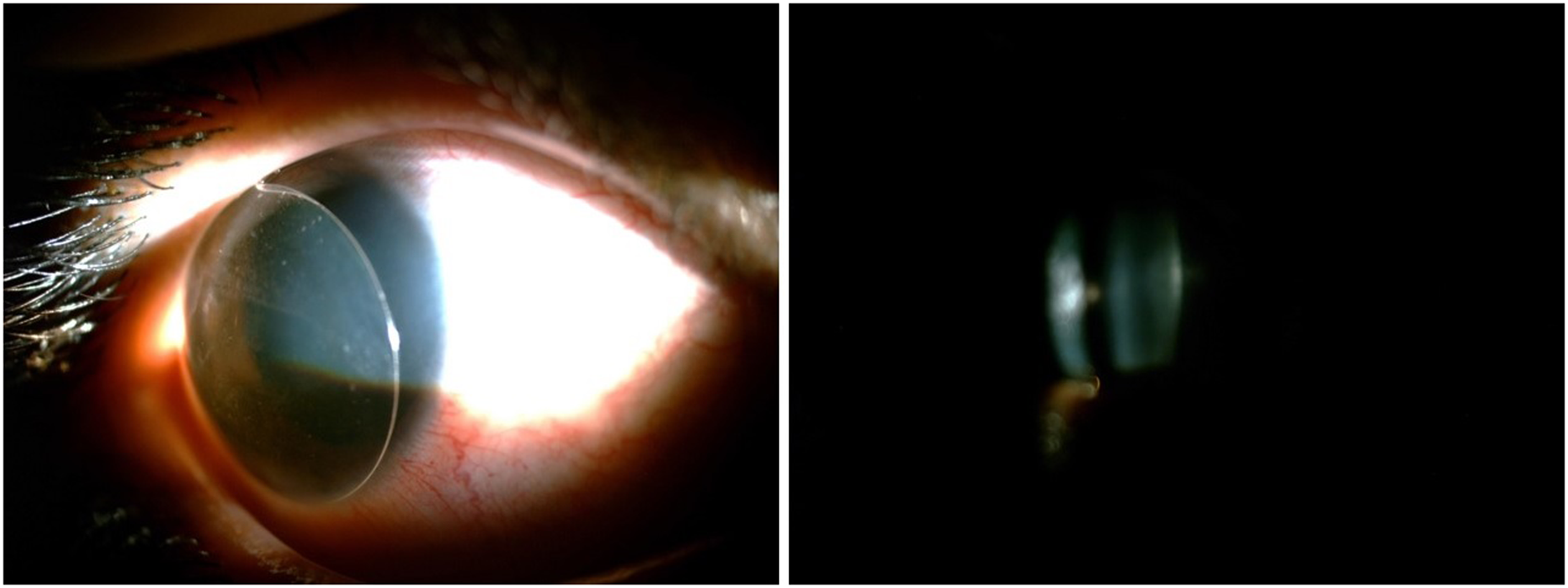
Following a rigid gas-permeable contact lens application (left), the conus bulging decreased to posterior flattening, demonstrating a sign of pseudo-lenticonus.
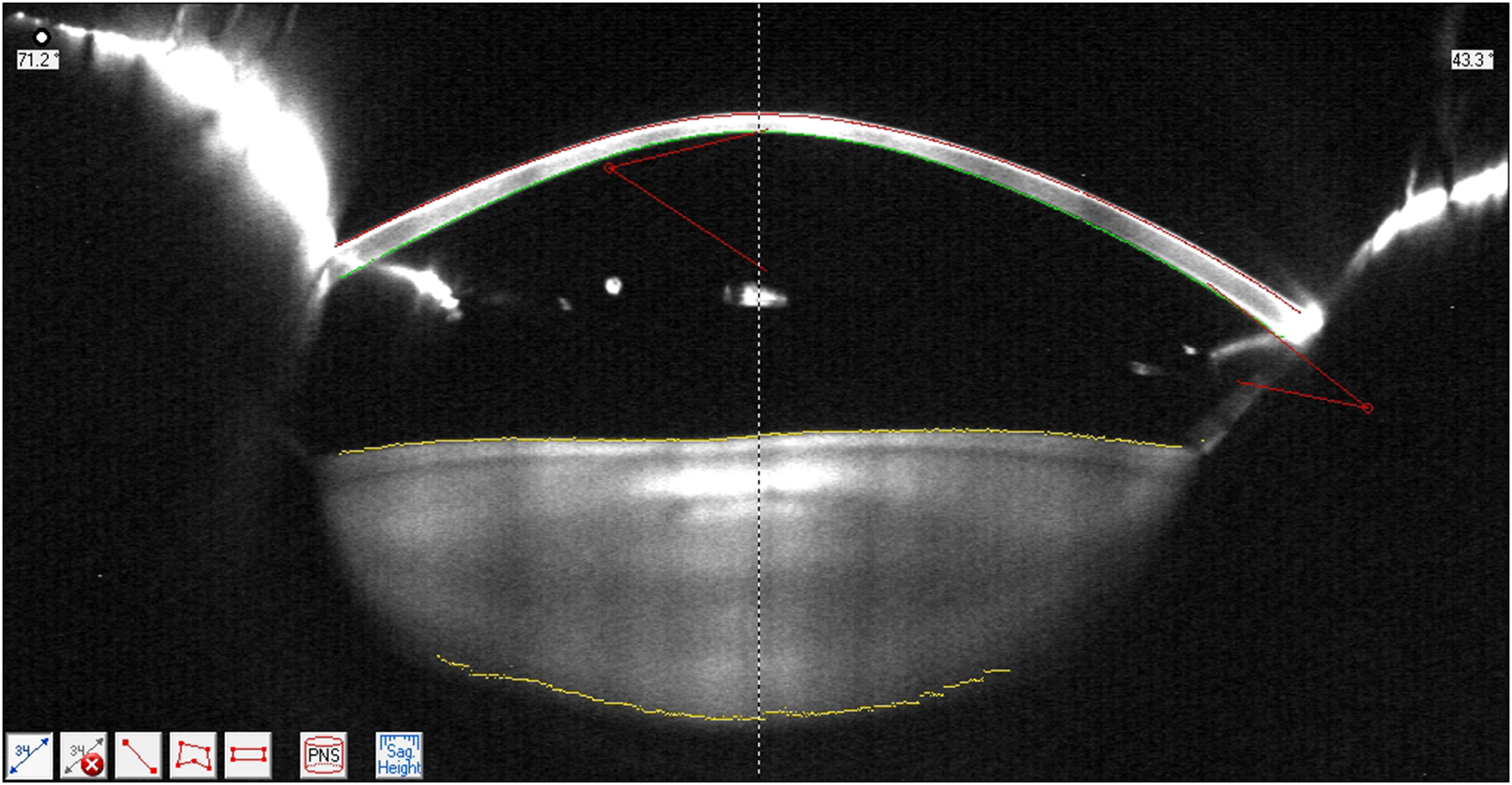
Scheimpflug image demonstrates a normal posterior crystalline lens border without posterior protrusion, indicating that posterior lenticonus secondary to a lens abnormality can be ruled out.
Discussion
The cornea or the crystalline lens can induced optical aberrations in the ocular media. 1 Keratoconus and ectatic corneal disorders are well-known corneal diseases that cause the cornea to become irregular in shape and biomechanically instable, resulting in a loss of vision. 1 Specific crystalline lens abnormalities, such as lens subluxation, anterior, and posterior lenticonus, 2 can also cause optical irregularities. The treatment of the disorders mentioned above is different from addressing the pathologic component of KC.
Due to the shortage of imaging methods for confirming a lenticonus diagnosis, the slit lamp examination remains the gold standard for diagnosis. Before proceeding with lens surgery and intraocular lens implantation to treat lenticonus, it is critical to make an exact distinction and diagnosis between true, false, pseudo conditions.
Grewal et al. previously described an isolated pediatric posterior lens capsule tear as a result of closed globe injury. The vitreous face was preserved during the slit-lamp examination of the affected eye. Integrity of lens was preserved, but the lens matter bulging through this posterior capsule tear created an erroneous clinical profile of posterior lenticonus; The authors refer to this as posterior pseudo-lenticonus. 3 In this instance, correcting the underlying KC pathology with a rigid contact lens restored normal visual function (Figure 4). As a result, lens pathology was ruled out as a possible cause of the visual disturbance. The purpose of this report for the first time is to demonstrate and quantify the lenticonus versus nipple cone KC using scheimpflug imaging. While neither a slit-lamp examination nor the anterior segment scheimpflug camera reveal the exact etiology of posterior capsule protrusion, the rotating Scheimpflug camera dose provides an additional, invaluable advantage in accurately diagnosing lenticonus versus nipple cone KC.
Conclusion
A nipple KC may inadvertently induce signs similar to of posterior lenticonus. When eye care professions encounter a patient with apparent posterior lenticonus during a slit-lamp examination, the possibility of KC should be considered, and the patient evaluated with other instrumentation including ultrasound, optical coherence tomography and etc.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval and consent statement
Ethics approval for this report was obtained from the Ethics Committee of Isfahan University of Medical Sciences, Isfahan, Iran (IR.MUI.MED.REC.1400.814). A signed statement of informed consent to publish patient data obtained from the patient.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.