
Abstract
Introduction
This report described a rare case of corneal perforation secondary to orbital cellulitis caused by Streptococcus pseudoporcinus (S. pseudoporcinus) infection. To the best of our knowledge, only six cases of S. pseudoporcinus infection have been reported. This case report suggested that S. pseudoporcinus infection was contagious and potentially life threatening. The report emphasized the value of managing infections early to avoid serious consequences.
Case description
A patient with orbital cellulitis, which progressed to corneal perforation was admitted to the hospital for right facial swelling, pain, and decreased vision in his right eye. S. pseudoporcinus infection was found after bacterial culture of pus puncture. After aggressive anti-infection and surgical treatment, the infection was eliminated, and the patient was discharged. However, the patient had sustained permanent vision loss.
Conclusions
This case suggested the potential risk of corneal perforation and orbital cellulitis caused by S. pseudoporcinus infection in humans. The specific biological changes and mode of action of S. pseudoporcinus are unclear and need further investigation.
Introduction
Orbital cellulitis is an acute inflammation of the orbital soft tissue caused by pathogenic microorganisms. The disease initially presents with severe eyelid redness, edema, ptosis, conjunctival deposition, and secretions, in addition to common signs and symptoms, such as erythema of the periorbital tissue, pain around the eyes, and painful eye movement. Proptosis, displacement of the eye, decreased vision, pupillary afferent defect, impaired color vision, and limited movement could occur with disease progression. Moreover, systemic manifestations include fever, leukocytosis, headache, general malaise, and loss of appetite. In severe cases, infections can lead to vision loss and life-threatening conditions, including optic neuropathy, orbital abscess formation, corneal ulcer, endophthalmitis, meningoencephalitis, intracranial abscess, cavernous sinus thrombosis, and septicemia. 1 This disease usually occurs in children. It primarily affects the orbit and spreads to the surrounding tissue, infecting the paranasal sinus and maxillofacial region. The most common pathogens of orbital cellulitis are Staphylococcus aureus and hemolytic streptococci, particularly Haemophilus influenzae. There have been no reports of ocular infections caused by S. pseudoporcinus worldwide. To the best of our knowledge, only six cases of S. pseudoporcinus infection have been reported. These cases included a finger wound infection caused by trauma, 2 left lower thigh honeycomb tissue infection related to dermatitis, 3 pulmonary infection, 4 puerperal infection, 5 and two cases of endocarditis.4,6 Therefore, this is the first study reporting a case of orbital infection caused by S. pseudoporcinus.
Case report
A 71-year-old man with a 50-year history of chronic rhinitis had been irregularly treated with non-standard oral antibiotics. At the time of admission, he had had right-sided facial pain, right-sided eyelid swelling, and decreased vision in the right eye for a week. In addition, he had no light perception in his right eye, while the visual acuity of his left eye was 20/30. The right eyelid was swollen, and the cornea was clear. The anterior chamber and iris were normal. The vitreous humor was slightly turbid, while the retina was pale and edematous. The veins were hyperemic, but the arteries were normal. Part of the eyeball was prominent. Eye movement was limited, and the orbit was swollen. No obvious abnormalities were observed in the left eye. The white blood cell count was 13.71 × 109/L, neutrophil ratio 87.8%, and lymphocyte ratio 5.8%. The erythrocyte sedimentation rate was 51 mm/h, and the procalcitonin level 1.10. The patient had an abnormal liver function. Magnetic resonance imaging of the brain (Figure 1) showed inflammation of the right sinuses, with infection of the right periorbital region. Ceftriaxone and methylprednisolone were administered to address the infection and inflammation, respectively. At the same time, the deep orbital cavity pus fluid was taken for culture and drug sensitivity testing. Upon resolution of the infection, the patient remained stable in the hospital four days after opening of the right side of the sinus, right orbital decompression, and septoplasty. On the fifth day of hospitalization, the patient had uncontrollable “hot tears” in his right eye. He had corneal perforation. He was treated with levofloxacin and bovine alkaline fibroblast growth factor eye drops, and incision and drainage of a periocular abscess, as well as conjunctival flap coverage, were performed (Figure 2). Meanwhile, the laboratory reported that the patient's pus grew S. pseudoporcinus. Identification of the isolate as S. pseudoporcinus was performed by the BD PhoenixTM M50 system (Dickinson and Company,USA) and confirmed by molecular analysis. S. pseudoporcinus, which develops from deep orbital pus, is sensitive to cefepime, linezolid, ampicillin, cefotaxime, penicillin, and vancomycin. Ceftriaxone was replaced with cefotaxime. The relevant data were collected only after the patient was discharged from the hospital, and the cultured flora has since been destroyed. Therefore, it is regrettable that the bacterial sequencing results cannot be obtained. The patient was discharged with no light perception after the infection was controlled. Slit-lamp examination revealed corneal scarring and anterior chamber formation (Figure 3). No corneal ulcers or eye infections were found throughout the course of the disease. The patient is currently being followed up.
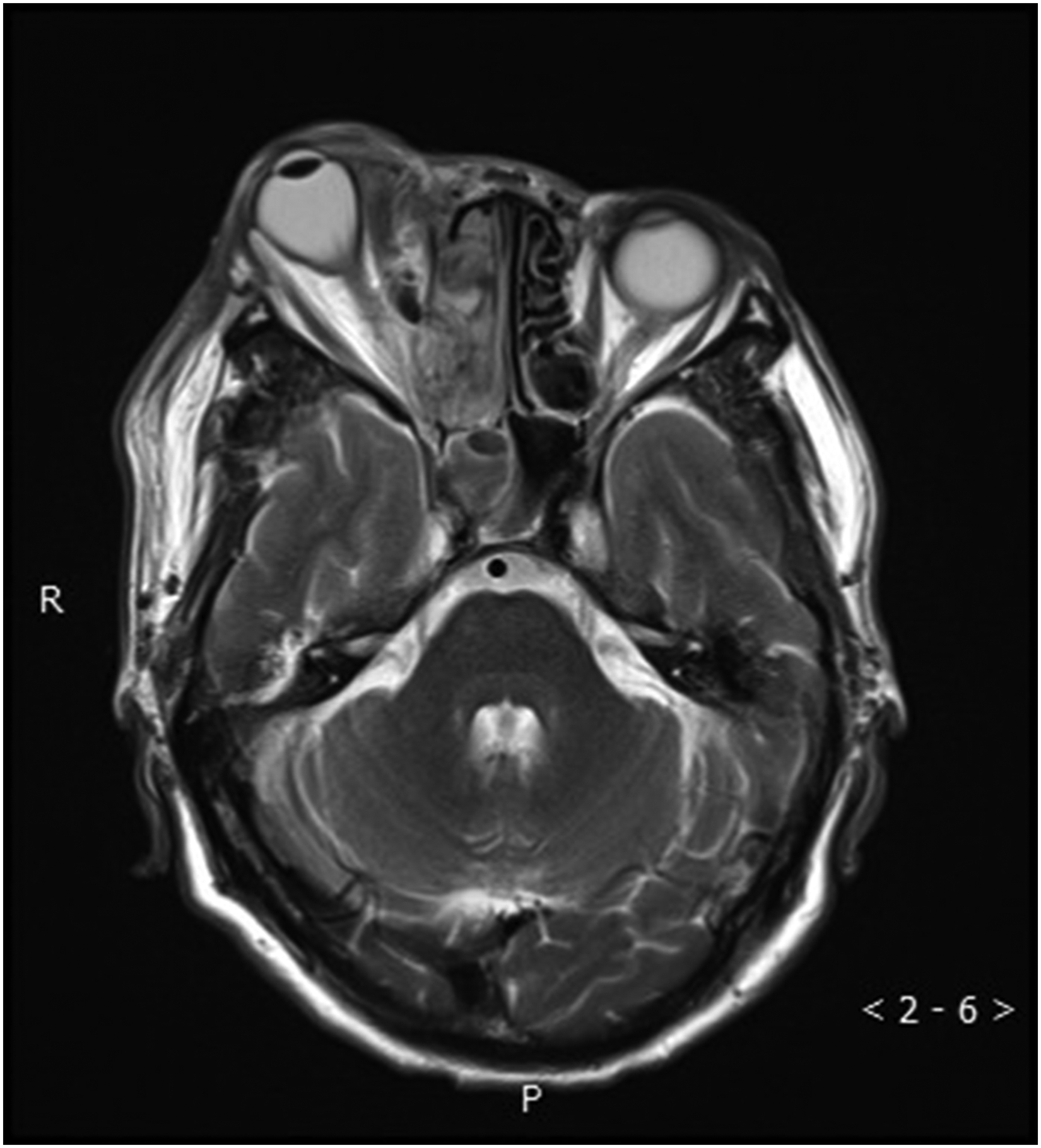
On admission, the eyeball of the right eye was prominent and deformed. The anterior chamber was normal. The periorbital and intraorbital soft tissues of the right eye were swollen.
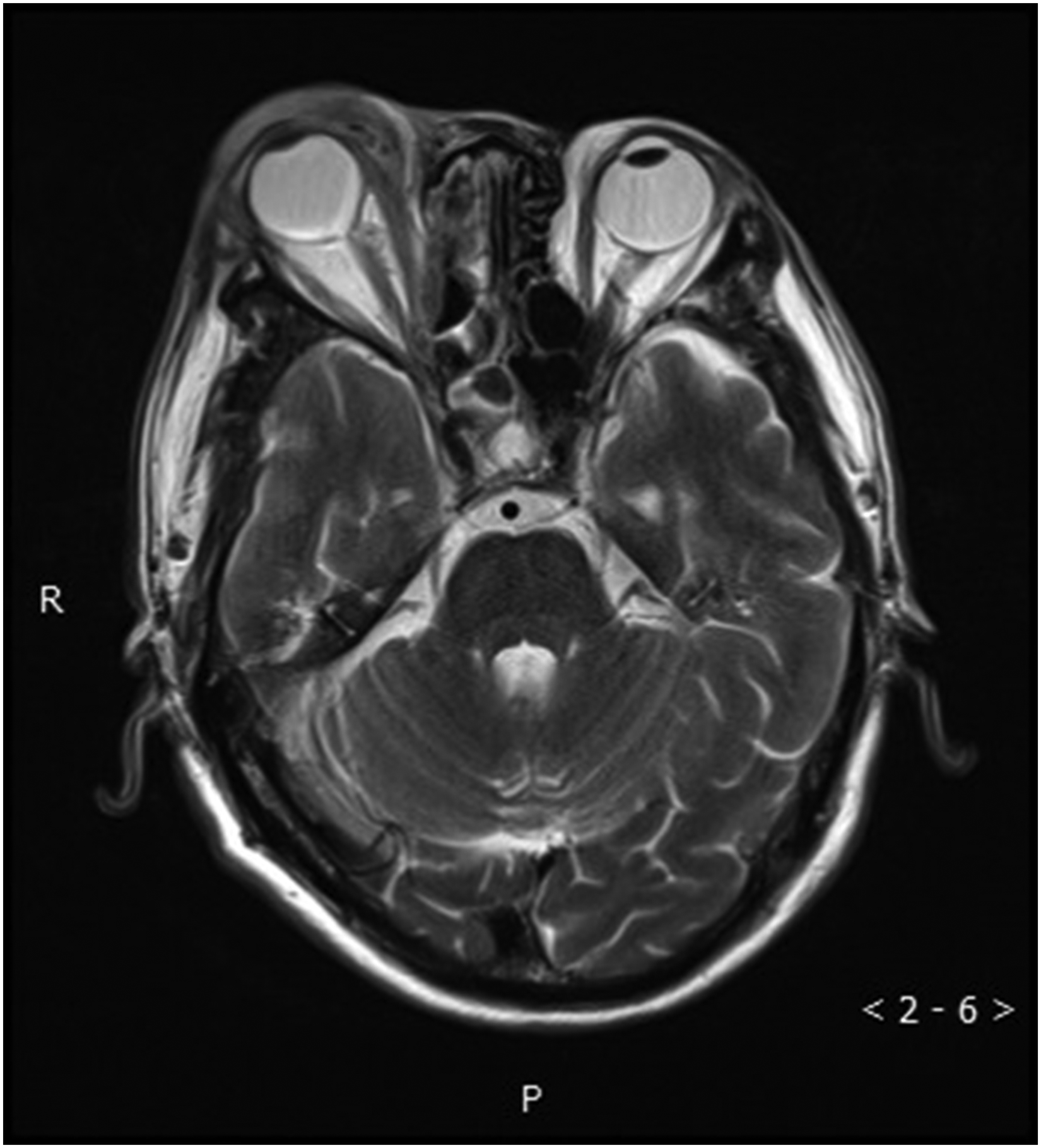
The anterior chamber disappeared four days after corneal perforation, and the swelling of the periorbital and intraorbital soft tissue of the right eye improved slightly.
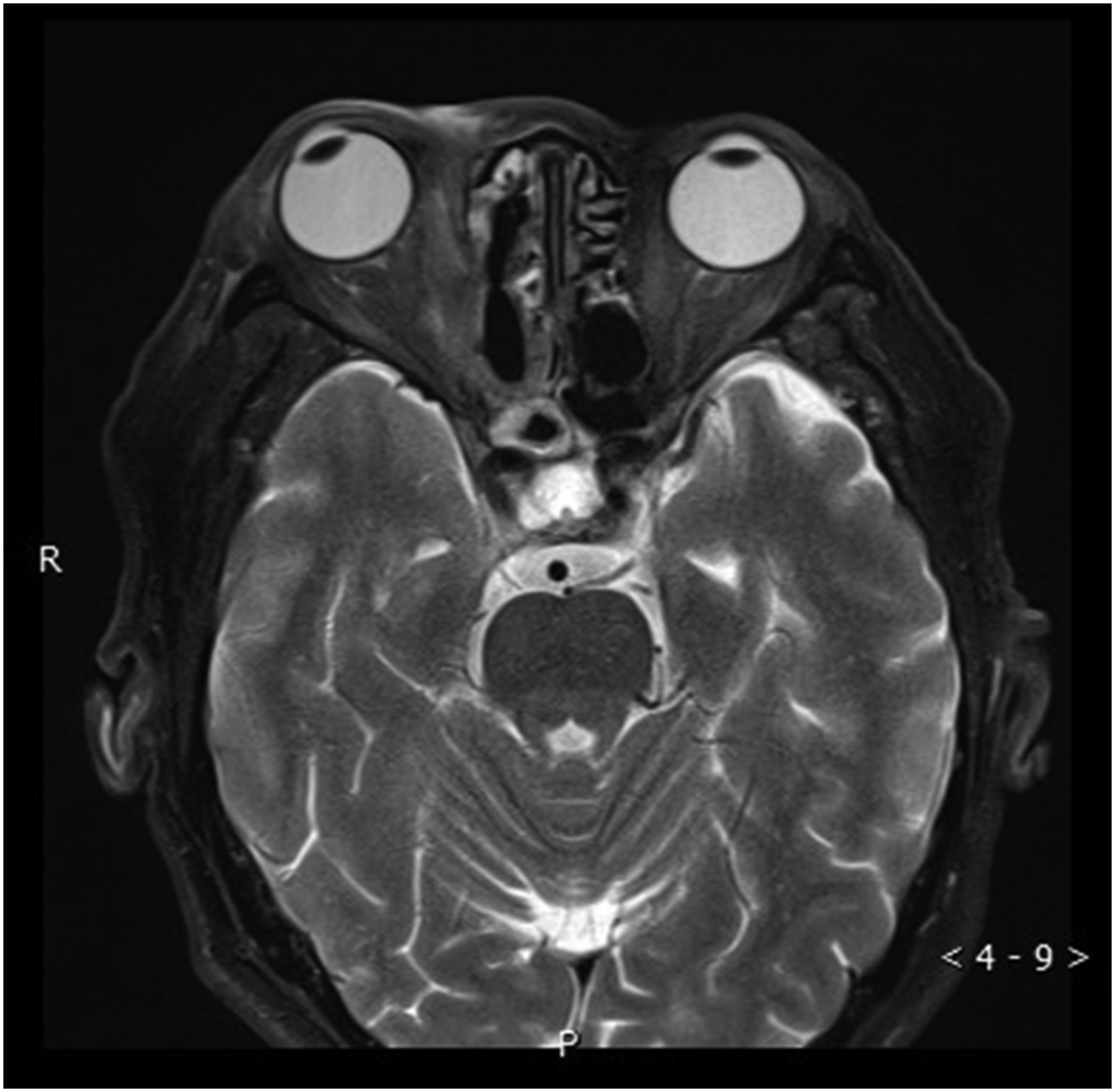
On hospital discharge, the anterior chamber returned to normal, and the periorbital and intraorbital soft tissues of the right eye were normal.
Discussion
Ocular infections are usually accompanied by loss of vision. Orbital cellulitis often causes irreversible damage to the optic nerve due to optic nerve compression by inflamed tissues. 7 We considered that the patient had permanent vision loss because of optic nerve damage caused by the infection. There have been reports of orbital cellulitis causing corneal ulcers, 8 but corneal perforation due to orbital cellulitis is rare. We report a case of orbital cellulitis with corneal perforation caused by S. pseudoporcinus infection. The destructive nature of S. pseudoporcinus causes corneal perforation.
S. pseudoporcinus is a hemolytic microorganism that colonizes the female genital tract. 9 It was previously classified as S. confusum, but in 2006, it was reported as a distinct species. 10 The cells of S. pseudoporcinus are globular to ovoid in shape. S. pseudoporcinus are gram-positive bacteria, commonly arranged in short chains, and they are hemolytic. 10 S. pseudoporcinus and S. porcinus strains might be falsely identified as group B streptococci (GBS,Because of the historical association with the bovine udder streptococci of serological group B were taxonomically classified as Streptococcus agalactiae), but the wide hemolysis zone, positive aesculin, and acid production in mannitol and sorbitol broths and proteomics method of identification(matrix-assisted laser desorption ionization time-of-flight mass spec-trometry) can distinguish the first two Streptococcus species from the latter.11,12 At present, studies have shown that S. pseudoporcinus has a certain impact on pregnant women. 13 In this case, the patient had S. pseudoporcinus infection of the right orbit. However, only corneal perforation was observed. The surface of the sclera and optic canal is more compact than that of the cornea. When bacteria secrete lysozymes into the tear film, the corneal surface barrier function is lost, and corneas with low immunity cannot heal properly. At the same time, the patient unconsciously rubbed his eye, resulting in corneal perforation.
Conclusions
This case suggested the potential risk of corneal perforation caused by S.pseudoporcinus infection in humans. The specific biological changes and mode of action of S.pseudoporcinus are unclear and need further investigation.
Footnotes
Informed consent statement
This case report was written using the clinical data of the patient in 2020. General consent was obtained in which the patient agrees with the research use of clinical records and data with anonymization.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.