
Abstract
Purpose
25-hydroxyvitamin D
Study Design
Prospective, single-center, clinical study.
Methods
The study included 82 eyes of 82 patients with 25(OH)D deficiency (Group I) and 50 eyes of 50 healthy subjects (Group II). All participants underwent OCTA examinations. The foveal avascular zone (FAZ) and superficial capillary plexus (SCP) and deep capillary plexus (DCP) vessel density (VD) measurements of the participants were statistically compared between the patients and healthy subjects.
Results
The mean 25(OH)D levels measured from the venous blood samples of the participants were 7.61 ± 3.27 ng/mL in Group I and 25.39 ± 4.16 ng/mL in Group II, and the difference between these values was statistically significant (p
Conclusion
The results showed that the FAZ area was significantly higher and the VDs of SCP and DCP were significantly lower in the patients with 25(OH)D deficiency. We found that 25(OH)D deficiency affected macular microvascular architecture.
Keywords
Introduction
25-hydroxyvitamin D [25(OH)D] is a secosteroid hormone that has receptors in various tissues and is synthesized from cholesterol in the skin. It is important for the skeletal structure of the body. 1 The best parameter indicating the body's 25(OH)D level is the serum 25(OH)D level. A serum 25(OH)D level of <20 ng/mL is defined as 25(OH)D deficiency. 2 25(OH)D has a regulatory effect on the immune system, and its deficiency has been associated with various chronic diseases. 3 In addition, 25(OH)D deficiency has been associated with decreased visual acuity and age-related macular degeneration (ARMD).4,5
Optical coherence tomography (OCT) and optical coherence tomography angiography (OCTA) are non-invasive examinations that are commonly used in the diagnosis and follow-up of retinal diseases. By examining erythrocyte motions in a certain retinal area, OCTA allows for the evaluation of microvasculature architecture in different layers of the retina with rapid OCT scans. 6
Although there are several studies on the association between the levels of 25(OH)D and macular structure, the data in this regard are limited. To the best of our knowledge, there is no previous study on OCTA measurements in patients with 25(OH)D deficiency. The current study mainly aimed to investigate macular microvasculature in 25(OH)D deficiency using OCTA. It was also aimed to obtain detailed information concerning the clinical manifestations of this condition by analyzing the extent of retinal effects in the presence of 25(OH)D deficiency.
Materials and methods
This study was prospectively conducted in line with the principles of the Declaration of Helsinki 2008 by including 132 eyes of 132 patients that presented to our hospital. Ethical approval was obtained from the local ethics committee (Date: 12.02.2019 No: 33216249-604.01.02-E.9060). Written informed consent was obtained from all participants.
Study population
The study included patients aged 18-65 years with serum 25(OH)D levels below 20 ng/mL without any comorbid systemic and ocular disease. A control group was formed with healthy individuals presenting to the ophthalmology clinic for a routine ophthalmologic examination. The inclusion criteria were as follows: refractive error ≤ ± 1 D or axial length between 22 and 24 mm, visual acuity LogMAR ≤ 0, and intraocular pressure (IOP) ≤ 21 mmHg. Patients with systemic pathologies, such as coronary artery disease, diabetes mellitus, hypertension, obesity, kidney or renal failure, acute or chronic infection, anemia, and thyroid pathologies that could affect measurements were excluded from the study. An extensive biochemical evaluation and parathormone measurements were performed by taking fasting venous blood samples from all participants. Patients reported to have any pathology were excluded from the study. Other exclusion criteria were pregnancy, alcohol consumption or smoking, presence of any ocular problem (such as ectatic corneal diseases, chorioretinal diseases, cataract, glaucoma etc.), history of contact lens use, history of ocular surgery, and poor quality of OCTA measurements. Patients with a history of any medication administration were excluded from the study.
All participants underwent detailed ophthalmologic examinations, in which refraction measurement (Tonoref III, Nidec Co. Ltd, Aichi, Japan), best corrected visual acuity analysis, slit lamp biomicroscopy, indirect ophthalmoscopy, non-contact biometry (AL-SCAN, Nidek Co. Ltd, Aichi, Japan), and IOP measurement (Tonoref III, Nidec Co. Ltd, Aichi, Japan) were carried out. The central macular thickness (CMT), central macular volume (CMV), and retinal nerve fiber layer thickness (RNFLT) were measured using SD-OCT, and the foveal avascular zone (FAZ) and vessel density (VD) measurements were obtained with an OCTA device (RS-3000 Advance AngioScan (Nidek Co. Ltd, Gamagori, Japan). The right eyes of the participants were included in the study.
Scan protocol
The SD-OCT and OCTA images were evaluated using the Nidek RS-3000 Advance OCT system. The light source of this device has a wavelength of 880 nm, its optical resolution in tissue is 7 microns on the Z axis and 20 microns on the XY axis, and it a speed of 53,000 A-scans per second. The fovea is focused on using an OCTA prototype internal fixation lamp, and 3 × 3 mm macula cubes, each consisting of 256 B-scans, are generated. In addition to FAZ, the device can automatically measure macular and peripapillary VDs.
Automated segmentation performed by the device is defined as the superficial retinal layer extending from the internal limiting membrane to 13 μm below the inner nuclear layer and the deep retinal layer extending from 8 μm below the inner nuclear layer to 13 μm below the outer nuclear layer.
For all cases, OCTA images were obtained by a single physician from a 3*3 mm macular area. The scanning was repeated if the SSI quality was <7/10. Participants with poor image quality in repetitive measurements were excluded from the study. With this device, FAZ and retinal VD measurements were performed from the superficial capillary plexus (SCP) (Figure 1). VD was defined as the percentage of vascularized tissue within the surrounding area. The quantitative analysis of VD was performed with the colored VD maps of the macula (ETDRS chart). The VDs of the global SCP and global deep capillary plexus (DCP) were evaluated by the macular OCTA scans.
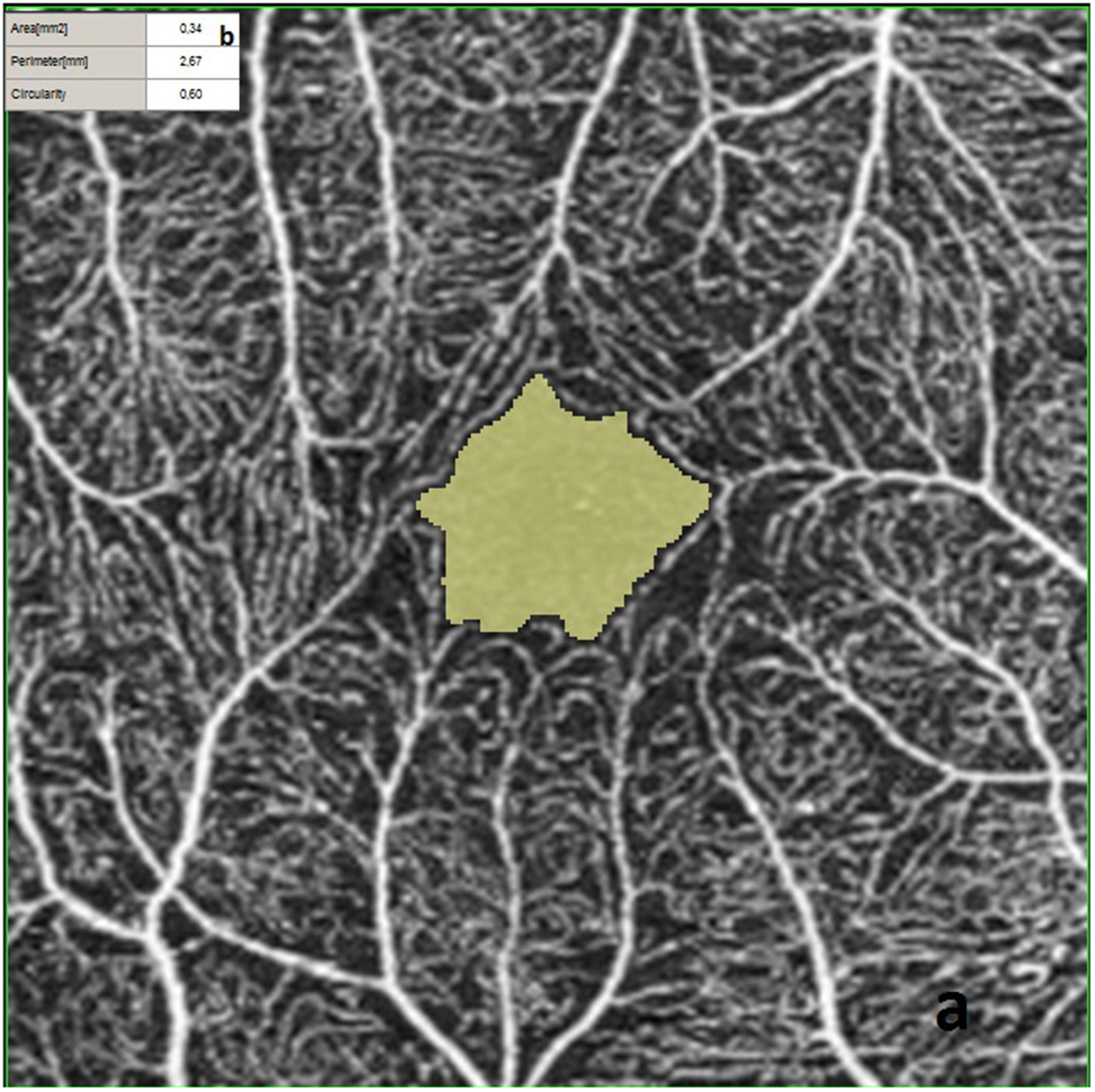
SCP FAZ metrics of a healthy 54-year-old male. a: FAZ area. b: FAZ metrics. The participant's 25(OH)D level was 33.1 ng/mL.
OCTA images showing the VDs of the SCP layer are presented in Figures 2 and 4, and the VDs of the DCP layer images are given in Figures 3 and 5. The participants were divided into two groups as those with 25(OH)D deficiency (Group I) and healthy controls (Group II). Blood samples were collected after eight hours of fasting in all participants. 25(OH)D levels were studied on the venous blood samples. All measurements were undertaken in the same season to minimize the effect of sun exposure. Biochemical analyses were performed using the Olympus AU2700 plus (Beckman Coulter, Tokyo, Japan) device.

Colored SCP vessel density map of the participant referred to in Figure 1. Nidek's RS-3000 Advance and Navis Ex. Ver. 1.1.5 software was used to obtain and analyze SD-OCT and OCTA images. This image also shows the vessel distribution charts.

Colored DCP vessel density map of the participant referred to in Figure 1 and vessel density distribution charts.

Colored SCP vessel density map of a 50-years-old female patient with 25(OH)D deficiency and vessel distribution tables. The participant's 25(OH)D level was 3.6 ng/mL.

Colored DCP vessel density map of the patient referred to in Figure 4 and vessel distribution charts.
Statistical analysis
Statistical analyses were performed using SPSS statistical software package, for Windows (version 21.0, SPSS, Inc., Chicago, IL). Numerical data were presented as mean ± standard deviation. The comparison of the numerical data of two groups was performed with the independent-samples t-test In both groups, the data were compared according to gender with the chi-square test After checking the collinearity diagnostics, an age- and gender-corrected multivariate regression analysis was used to determine the associations between the serum 25(OH)D concentration as an dependent variable and the VDs of SCP and DCP, FAZ area, CMT, CMV and RNFLT parameters as independent variables. The results were expressed at the 95% confidence interval and regression coefficients (B) were obtained from the regression analysis. A value of P < 0.05 was accepted statistically significant.
Results
The study included 82 eyes of 82 patients with 25(OH)D deficiency (Group I) and 50 eyes of 50 healthy controls (Group II). The mean age was 37.29 ± 12.76 years in Group I and 39.1 ± 11.59 years in Group II. There was no statistically significant difference between the two groups in terms of age (p = 0.498) or gender (p = 0.548).
The mean 25 (OH) D levels measured from the venous blood samples of the participants were 7.61 ± 3.27 ng/mL (3.30-14.50) in Group I and 25.39 ± 4.16 ng/mL (20.90-33.1) in Group II (p < 0.0001). The mean axial length (AL) measurements were 23.44 ± 0.77 mm (range 22.04-23.98) in Group I and 23.52 ± 0.83 mm (range 22.09-24.00) in Group II, indicating no statistically significant difference (p = 0.754). The mean refractive error measurements were −0.07 ± 0.15 diopters (D) (range: −0.75–0.50) in Group I and 0.15 ± 0.19 D (range: −0.25–0.25) in Group II (p = 0.485).
The OCT and OCTA measurements of the participants are summarized in Table 1. The FAZ measurements were significantly higher in Group I (p = 0.014) while the VDs of SCP and DCP were significantly higher in Group II (p < 0.0001 and p < 0.0001, respectively). It was observed that retinal vascular density values were lower in the group with low 25(OH)D levels, and on the contrary, FAZ values increased in this group. When the CMT values of the participants were compared, Group II had a significantly higher value (p = 0.023), but there was no significant difference between the two groups in relation to CMV and RNFLT (p = 0.442, and p = 0.184, respectively).
SD-OCT and OCTA findings of the study groups.
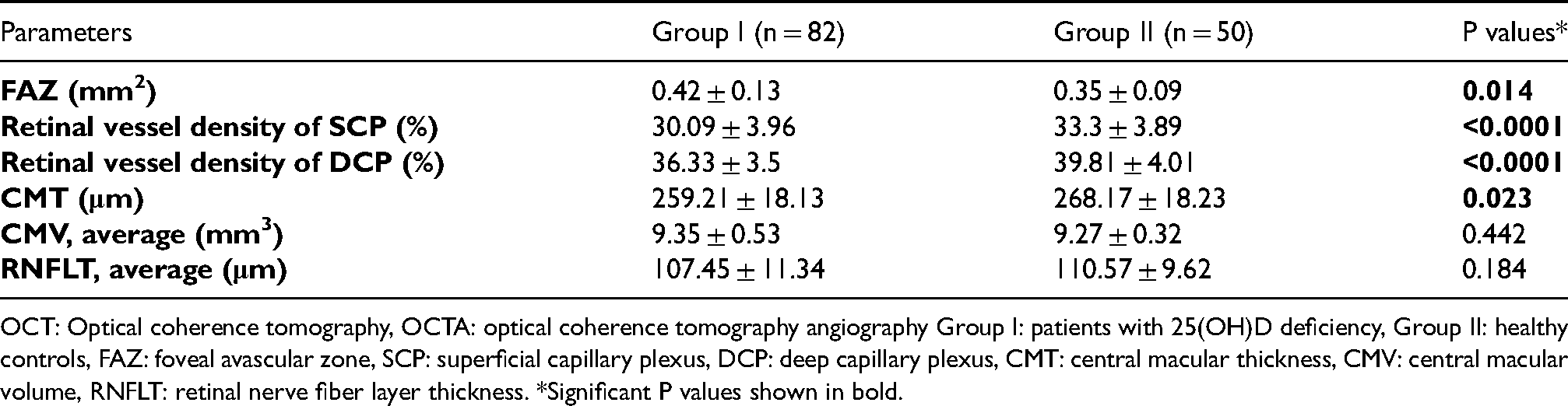
OCT: Optical coherence tomography, OCTA: optical coherence tomography angiography Group I: patients with 25(OH)D deficiency, Group II: healthy controls, FAZ: foveal avascular zone, SCP: superficial capillary plexus, DCP: deep capillary plexus, CMT: central macular thickness, CMV: central macular volume, RNFLT: retinal nerve fiber layer thickness. *Significant P values shown in bold.
In the multivariate regression analysis, there was a significant positive correlation between serum 25(OH)D and the VDs of the global SCP and DCP and a significant negative correlation between 25(OH)D and serum the FAZ measurements of SCP and DCP (p < 0.001). Thus, it was determined that at lower 25(OH)D levels, SCP and DCP VD decreased and FAZ measurements increased. However, no correlation was observed between serum 25(OH)D and CMT, CMV or RNFLT (p = 0.254, p = 0.318, and p = 0.524, respectively) (Table 2).
Associations of the VD and FAZ values with the serum 25(OH)D concentrations of the study groups.
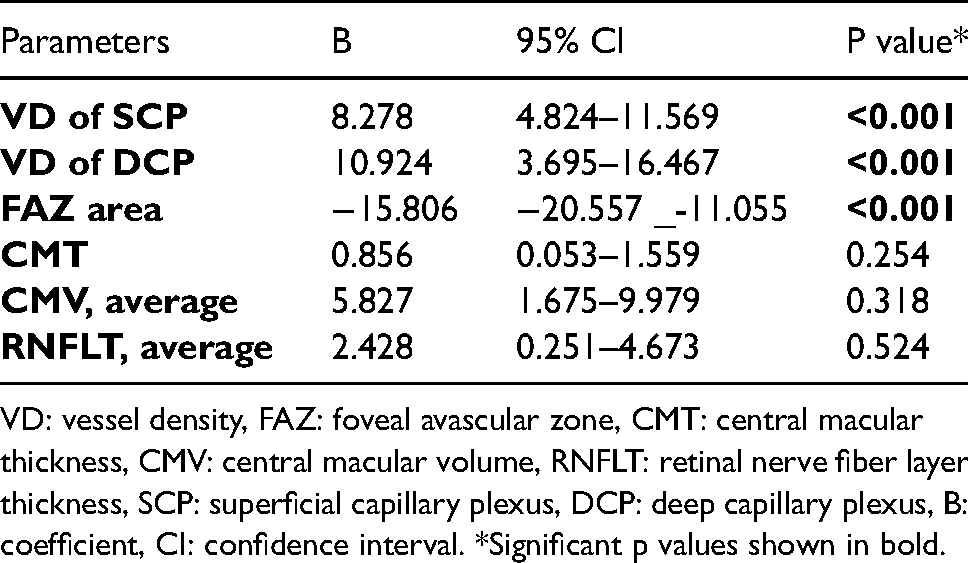
VD: vessel density, FAZ: foveal avascular zone, CMT: central macular thickness, CMV: central macular volume, RNFLT: retinal nerve fiber layer thickness, SCP: superficial capillary plexus, DCP: deep capillary plexus, B:coefficient, CI: confidence interval. *Significant p values shown in bold.
Discussion
25(OH)D Deficiency is a common health problem worldwide. 25(OH)D has critical biological importance for the body. In addition, it has been reported to have immunomodulatory effect on the natural immune system. 7 Although this vitamin can be taken through the diet, it does not occur naturally in most foods; therefore, it is necessary to be synthesized in the skin with exposure to ultraviolet B rays. 1 It then transforms into 25(OH)D in the liver, which is its essential form in circulation. 8 A short time spent in outdoor activities, wearing long clothes, intense use of sunscreen, and use of some drugs such as colchicine have been associated with 25(OH)D deficiency. 9
OCTA is a device commonly used today in the diagnosis and follow-up of retinal diseases based on the evaluation of retinal microvasculature. There are several advantages of OCTA, including its non-invasive nature, requirement of no contrast substance use, and no side effect. 10
Previous experimental animal studies have shown that 25(OH)D supplementation has a protective effect on a number of autoimmune diseases. 8 Patients with ankylosing spondylitis, Behcet's disease, Vogt-Koyanagi-Harada syndrome, and acute anterior uveitis have been shown to have low 25(OH)D levels11–14 In addition, it has been found that ocular pathologies, such as dry eye syndrome, glaucoma, age-related macular degeneration, diabetic retinopathy, and optic neuritis may coexist with 25(OH)D deficiency. 15
The target cells of 25(OH)D were first shown in the central nervous system and retina widely. 25(OH)D receptors have also been shown in the cornea, lens, ciliary body, retinal pigment epithelium, corneal epithelium, ganglion cell layer, and retinal photoreceptors.16,17 Oxidation, angiogenesis and inflammation in ocular tissues are known to cause cell dysfunction and tissue damage. Penna et al. found that 25(OH)D exhibited a protective effect by reducing the production of proinflammatory (interleukin-2 (IL-2), IL-12, interferon γ etc.) cells and promoting anti-inflammatory cell increase (IL-4, IL-10, and tumor growth factor ß). 18 25(OH)D has also been found to be very effective in providing homeostasis of vascular tissues in patients with type 2 diabetes. In diabetic patients with 25(OH)D deficiency, the risk of cardiovascular disease almost doubles compared to optimal 25(OH)D levels. 25(OH)D prevents foam cell formation and reduces the risk of vascular disease. Active 25(OH)D decreases stress in the endoplasmic reticulum in type 2 diabetes, reduces macrophage infiltration, reverses macrophage-cholesterol accumulation, and promotes cholesterol excretion. These findings suggest 25(OH)D supplementation as a potential treatment for atherosclerosis regression. 19 Based on these vascular effects of 25(OH)D, it can be concluded that the effect of 25(OH)D on vascular homeostasis is supported by the correlation of 25(OH)D levels with FAZ and VD measurements in our study.
A study by Seddon et al. showed that adequate 25(OH)D intake could have a preventive effect on the progression of ARMD. 20 In another study, it was stated that a sufficient 25(OH)D level could protect against ARMD through its anti-inflammatory and antiangiogenic effects. 21 Graffe et al. referred to the association between 25(OH)D deficiency and reduced macular thickness in elderly patients. 22 Similarly, we found that CMT was significantly lower in the patients with 25(OH)D deficiency compared to the control group. In addition, we determined that the FAZ measurements were significantly higher in the patients with 25(OH)D deficiency than in the control group. Accordingly, the retinal VD was found to be lower in both SCP and DCP. Measurements of FAZ, CMT, SCP&DCP VD do not have serious pathological values in the cases included in Group I but there is a statistically significant difference when these values are compared with the Group II. This change can be supported by future studies that include measurements before and after 25(OH)D treatment in cases with 25(OH)D deficiency. When advanced age, additional ocular or systemic diseases affecting the retina and choroidal structure come into play, these measurements in 25(OH)D deficiency, which do not show significant numerical difference, may create pathological conditions that should be taken into account.
In the current literature, some sources specify the vitamin D reference range as 30–100 ng/ml, and vitamin D insufficiency and deficiency correspond to <30 ng/ml and <20 ng/ml levels, respectively.23–25 Most of the guidelines accept that this value above 20 ng/mL is sufficient for the human body.26,27 The mean 25(OH)D value of 25.39 ± 4.16 ng/mL and the statistically significantly higher retinal microvascularity in Group II compared to Group I may also indicate that this cut-off value is also effective in terms of retinal health. The 25(OH)D level in Group II is sufficient in many studies, but it can be said that it is a controversial issue in some sources. In our study, the statistically significant difference in OCT-A examinations in 25(OH)D levels at these levels seems to support the fact that this limit is an effective level. In the future, these findings can be supported by detailed studies to be conducted before and after treatment for 25(OH)D deficiency with more participants.
Based on these values, it can be hypothesized that 25(OH)D has a protective effect on macular health; therefore, 25(OH)D supplementation may be helpful in the prevention of macular pathologies and treatment of such pathologies. Various studies have shown the relationship between 25(OH)D levels and ocular inflammation and immunological reactions.28,29 In line with this information, it can be said that 25(OH)D deficiency leads to negative conditions in retinal microvascular structure as in diabetic retinopathy as a result of lack of anti-inflammatory effect. To the best of our knowledge, this is the first study to investigate retinal microvasculature using OCTA in patients with 25(OH)D deficiency.
Factors limiting our study were the relatively low number of participants and the absence of an evaluation of changes in OCT and OCTA measurements after the administration of 25(OH)D treatment.
In conclusion, in this study, we evaluated the OCTA findings and structural OCT parameters of patients with 25(OH)D deficiency compared to healthy controls. Based on these findings, it can be stated that macular perfusion is negatively affected by 25(OH)D deficiency. However, considering that cross-sectional studies cannot sufficiently demonstrate the microvascular effect of 25(OH)D deficiency, we are currently performing a follow-up study to better explain our findings. Thus, the data presented in this paper should be carefully interpreted and supported by further studies to be conducted with a large sample size.
Footnotes
Acknowledgements
This study was presented as a poster at the TOD 42th Spring Symposium, held from May 10-12, 2019 in İstanbul, Turkey
Statement
The manuscript has been seen by all authors. It has not been submitted in similar form for publication elsewhere.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.