
Abstract
Purpose
Clinical phenotypes in Immunoglobulin G4-related disease (IgG4-RD) according to the patterns of affecting organs have different risks of malignancies. We attempt to determine the association of malignancies with IgG4-related ophthalmic disease (IgG4-ROD).
Design
Retrospective cohort study.
Methods
Review of medical records, orbital images and histopathology reports in a territory-wide cohort of biopsy proven IgG4-ROD patients from 2005–2019.
Findings
Among 122 patients who had biopsies taken from adnexal lesions including lacrimal glands (n = 108), orbital mass (n = 30), infiltrated orbital fat (n = 10), conjunctiva (n = 2) or extraocular muscles (n = 3), 13% (16/122) developed malignancies over 73 ± 48months’ follow-up. There were 9 cases of ocular adnexal lymphoma (OAL) and 7 extra-orbital malignancies. Compared with the general population, the incidence of OAL was significantly higher (standardized incidence ratios, SIRs = 10.0, 95%CI = 4.5–17.6) while that of extra-orbital malignancies was similar. The SIRs was highest within the first year (SIR = 46.7, 95%CI = 18.5–87.6) when 7 OAL were concomitantly diagnosed. Patients who developed OAL or extra-orbital malignancies were older than other patients at IgG4-ROD diagnosis (64.9 ± 7.1, 68.3 ± 8.5 versus 55.2 ± 15.0 years, P < 0.05). Asymmetric lacrimal gland enlargement (78% versus 13%), lack of frontal (0% versus 12%) or infraorbital nerve enlargement (0% versus 36%) were associated with OAL (all P < 0.05). Pre-treatment serum IgG4 level or extra-orbital IgG4-RD involvement was similar among patients with or without malignancies.
Conclusion
In this biopsy-proven IgG4-ROD cohort, 7% developed OAL which was 10 times higher than the general population. Patients with asymmetric lacrimal gland enlargement or without trigeminal nerves involvement radiologically were associated with OAL.
Keywords
Introduction
Immunoglobulin G4-related disease (IgG4-RD) is an immune-mediated fibroinflammatory disease characterized by tumefactive lesions with noticeable IgG4 + plasma cells infiltrating 1 into different organs including the hepatobiliary tree, pancreas, exocrine glands, kidneys, lungs, lymph nodes, meninges, aortas and prostates.2,5 IgG4-RD was first recognized as a single disease entity, but recent studies suggested several clinical phenotypes according to the patterns of affecting organs.6,8 While Lanzillotta et al. 6 did not show any difference of incidence in solid or hematological cancers among IgG4-RD phenotypes,, Niwamoto et al. 7 reported an association between malignancies and those with IgG4-related autoimmune pancreatitis.
In IgG4-related ophthalmic disease (IgG4-ROD), infiltration, fibrosis and dysfunction of the lacrimal glands, extraocular muscles, periorbital and optic nerves, the eyelid and orbital soft tissues have been reported. 9 Cheuk et al. 10 first reported 6 patients with ocular adnexal lymphoma (OAL) associated with IgG4-ROD. The Japanese study group of IgG4-ROD showed that 9.8% of mucosa associated lymphoid tissue (MALT) orbital lymphoma in their multi-center cohort were IgG4-positive. 11 IgG4-ROD appeared to have a strong association with lymphoma, compared to other organ-specific phenotypes of IgG4-RD. 12 In this study, we compare the incidence of malignancies in a well-characterized and biopsy-proven IgG4-ROD cohort with the local population, and we compare the clinical, serological and radiological features of patients who developed cancer at the time of or after the diagnosis of IgG4-ROD to those who did not.
Methods
We conducted a retrospective study of all consecutive patients of biopsy-proven IgG4-ROD diagnosed from 2005 to 2019. Patients were managed by all 7 Hospital Authority clusters covering the territory-wide, publicly funded ophthalmology service in Hong Kong and the Hong Kong Sanatorium & Hospital. Medical records including orbital images and histological slides were reviewed. This study followed the Declaration of Helsinki and ethical approval was obtained from the Institutional Review Board (IRD) of each participating hospital. Orbital adnexal specimens including the lacrimal glands (n = 108), discrete masses (n = 30), infiltrated fat (n = 10), conjunctiva (n = 2) and extraocular muscles (n = 3) were obtained by open surgical biopsies. Diagnosis of IgG4-ROD required histological evidence of lymphoplasmacytic infiltrates of >50 IgG4 + cells per high power field (PHF) × 400 and an IgG4 + /IgG + ratio of >40% in the biopsied orbital tissue. 13
Histological specimens reported before 2005 were retrospectively reviewed and stained, and the diagnosis of IgG4-ROD was only confirmed if fulfilling the mentioned criteria. An independent consultant histopathologist with over 30 years’ experience reviewed slides of all available malignant lesions to evaluate the presence and degree of IgG4-positive plasma cell infiltrations. The first biopsied specimen of IgG4-ROD patients who subsequently developed OAL in the second biopsy would be validated by the corresponding pathologist to confirm the absence of OAL in the first. An independent nuclear medicine physician reviewed the positron emission tomography-computed tomography (PET-CT) scan of a patient with radiologically diagnosed lung cancer.
Numerical results were presented as mean ± standard deviation (SD) and range unless otherwise stated. The incidence rate of malignancies was compared to the general population using the standardized incidence ratios (SIRs) and 95% confidence interval (95%CI). 14 The incidence of malignancies in the general population of Hong Kong was obtained from the Hong Kong Cancer Registry, 15 which included patients of all types of malignancies diagnosed in both public and private healthcare sectors. Information was also obtained from the Deaths Registry, Pediatric Hematology and Oncology study group, and voluntary notifications in Hong Kong up to 2017. The SIRs were further adjusted according to age as stratified by the Hong Kong Cancer Registry based on gender and the types of malignancies. Clinical, serological, and radiological risk factors were compared using the Fisher's exact test and chi-square test taking P < 0.05 as significant. All statistical analyses were performed using SPSS statistical software package (Window version 24.0; IBM Corp., Armonk, NY).
Results
Records of 122 patients over a follow-up period of 73 ± 48 (12 to 260) months were reviewed. Three patients were diagnosed with cancer (breast cancer, prostate adenocarcinoma, and diffuse large B cell lymphoma (DLBCL) of the ipsilateral cervical lymph node) 85 ± 27 (60 to 123) months before the diagnosis of IgG4-ROD. The patient with breast cancer was subsequently diagnosed with endometrial adenocarcinoma at the time of IgG4-ROD diagnosis. 13% (16/122) of patients, including 12 males were diagnosed with malignancies at the time of or after the diagnosis of IgG4-ROD over 38 ± 25 (7 to 84) months. Ocular adnexal lymphoma (OAL) and extra-orbital malignancies were found in 9 and 7 patients respectively (Table 1 and 2). 69% (84/122) of the cohort underwent radiological investigations for extra-orbital involvement after the IgG4-ROD diagnosis, including computed tomography (CT) (abdomen = 56, thorax = 50, brain = 46 and pelvic = 46), magnetic resonance imaging (MRI) (brain = 20, abdomen = 7, thorax = 6, and pelvic = 6), ultrasound scan (thyroid = 6 and neck = 4) and PET-CT (whole body = 13). The extra-ophthalmic involvement is summarized in Table 3.
Patients who developed ocular adnexal lesions (OAL) concomitantly with or after the diagnosis of IgG4-ROD.
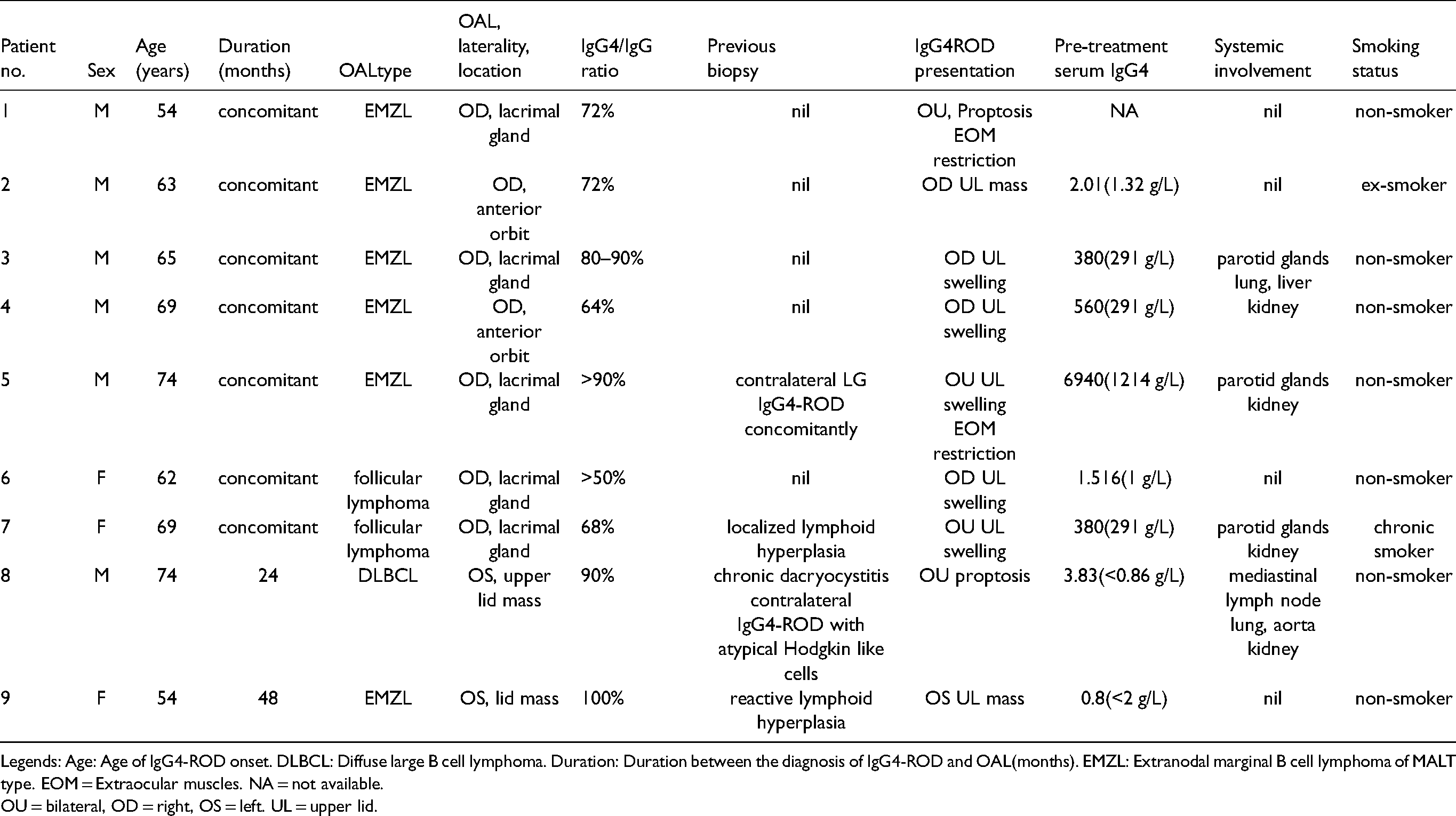
Legends: Age: Age of IgG4-ROD onset. DLBCL: Diffuse large B cell lymphoma. Duration: Duration between the diagnosis of IgG4-ROD and OAL(months). EMZL: Extranodal marginal B cell lymphoma of MALT type. EOM = Extraocular muscles. NA = not available.
OU = bilateral, OD = right, OS = left. UL = upper lid.
Patients who developed extra-orbital malignancies concomitantly with or after IgG4-ROD diagnosis.
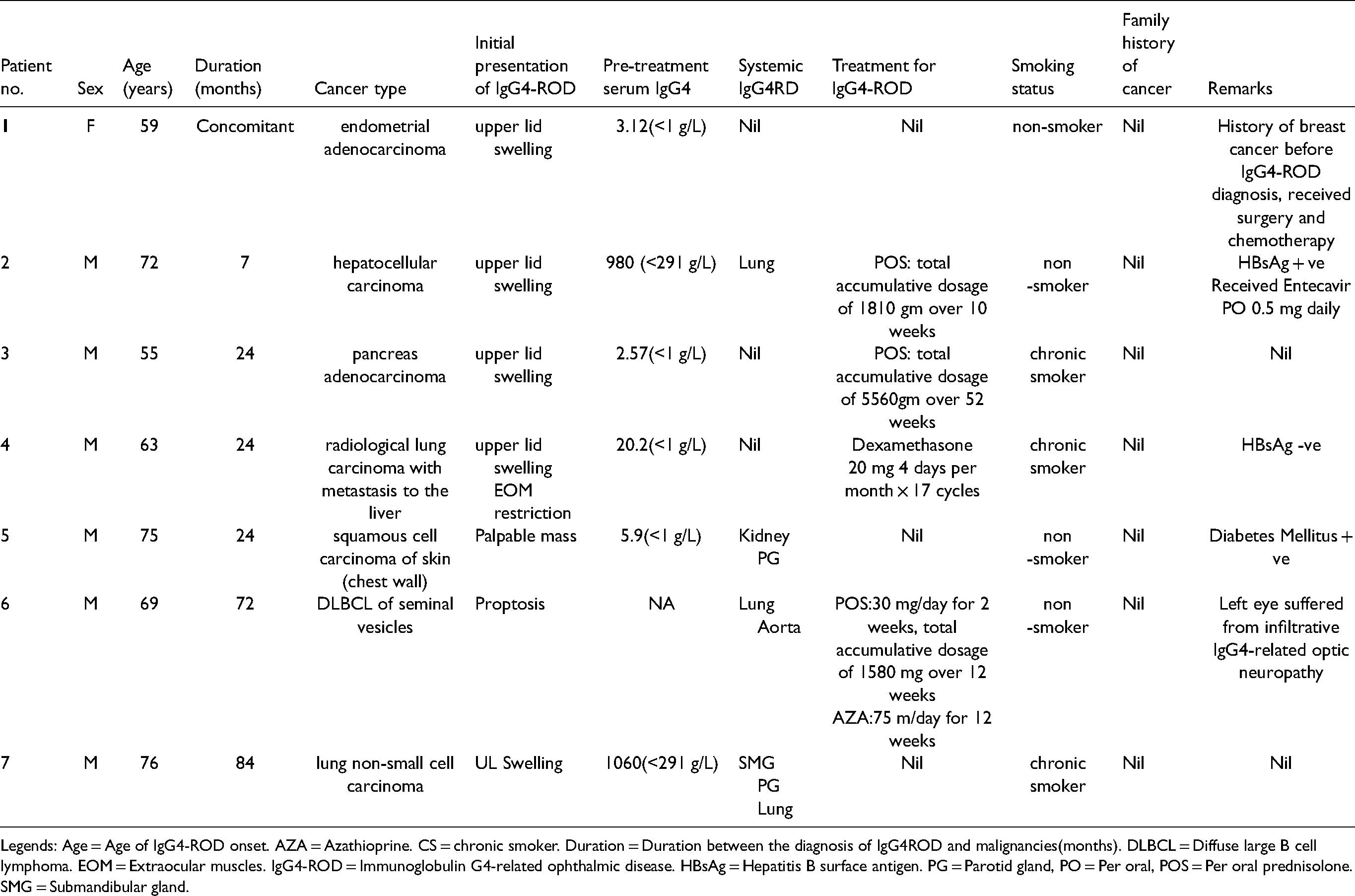
Legends: Age = Age of IgG4-ROD onset. AZA = Azathioprine. CS = chronic smoker. Duration = Duration between the diagnosis of IgG4ROD and malignancies(months). DLBCL = Diffuse large B cell lymphoma. EOM = Extraocular muscles. IgG4-ROD = Immunoglobulin G4-related ophthalmic disease. HBsAg = Hepatitis B surface antigen. PG = Parotid gland, PO = Per oral, POS = Per oral prednisolone. SMG = Submandibular gland.
Extra-ophthalmic involvement of IgG4-RD in this IgG4-ROD cohort (n = 122).
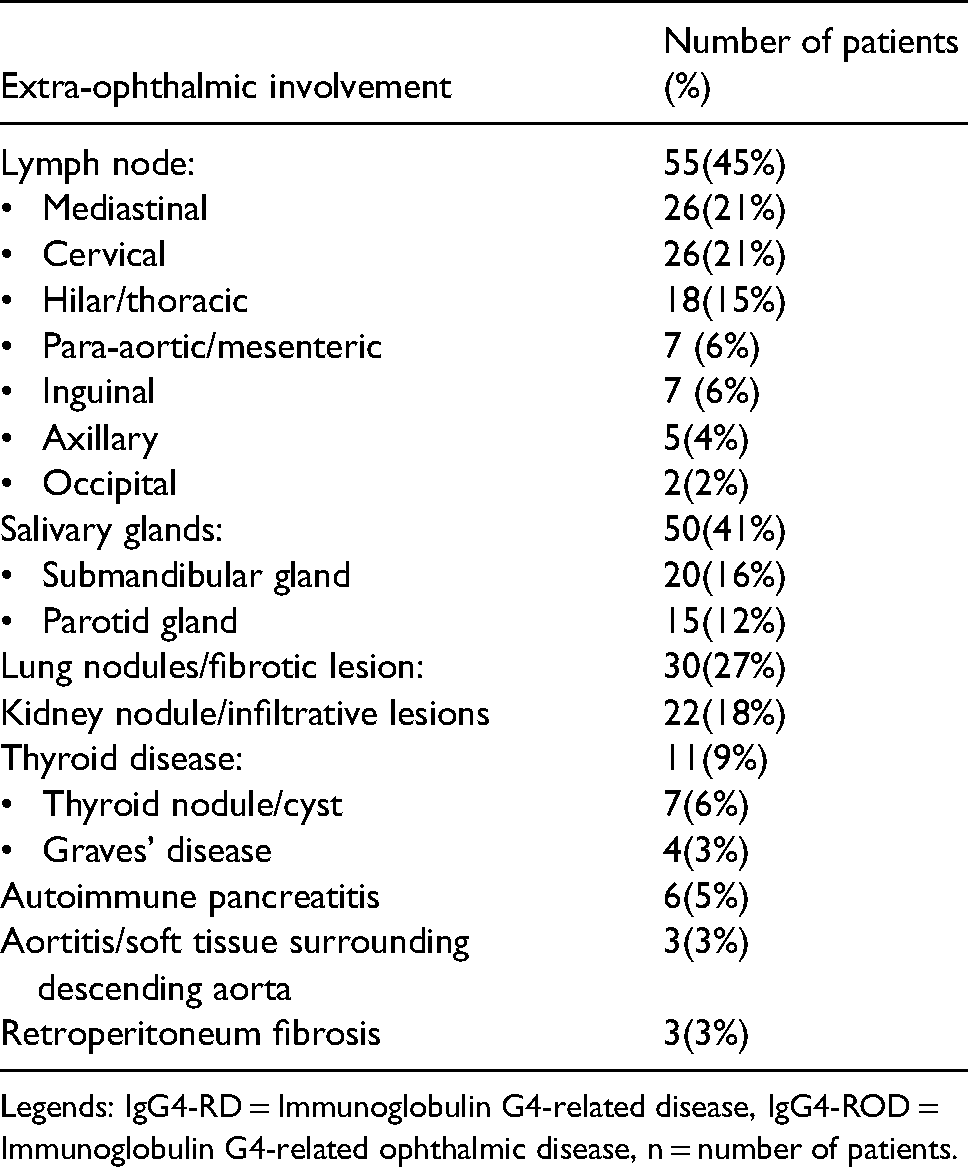
Legends: IgG4-RD = Immunoglobulin G4-related disease, IgG4-ROD = Immunoglobulin G4-related ophthalmic disease, n = number of patients.
Comparing the 16 patients to the rest of the cohort (106 patients), the age at IgG4-ROD diagnosis was significantly higher (66.3 ± 7.9 years versus 55.2 ± 15.0 years, P < 0.05), while the male to female ratio was higher but not reaching statistical significance (12:4 versus 53:51, P = 0.13). 56% (9/16) of the cancer patients had extra-orbital involvement of IgG4-RD, as compared to 53% in the rest of the cohort (P = 0.80). 15 of the 16 cancer patients had pre-treatment serum IgG4 tested and elevation was found in 87% (13/15) of them, compared to 90% (90/100) of the rest of the cohort (P = 0.74), mean level was 2.5 ± 1.7(1.3–5.7) times higher than the normal upper range compared to 11 ± 2.7 (1.1–22.8) times in the rest of the cohort (P > 0.05). Smoking status was similar (25% versus 24%, P = 0.47).
IgG4-related ocular adnexal lymphoma (OAL)
7.4% (9/122) of patients, 6 males, developed OAL at the time (7 patients) of or 24 and 48 months following the diagnosis of IgG4-ROD (2 patients). One patient was a chronic smoker. Comparing these 9 OAL patients with the rest of the cohort (106 patients), the mean age of IgG4-ROD diagnosis was higher (64.9 + /-7.1 vs 55.2 + /-15.0, P < 0.05), and the male to female ratio was higher but not reaching statistical significance (6:3 versus 56:50, P > 0.5). The commonest presentation was upper lid swelling (62% versus 71%, P = 0.78), followed by proptosis (25% versus 20%, P = 0.15) and palpable mass (22% versus 20%, P = 0.37). 88% (7/8) of patients with OAL had elevated pre-treatment serum IgG4 compared 90% (90/100) patients from the rest of the cohort (P > 0.05). Radiologically, 78% (7/9) of patients with OAL had asymmetric enlargement of the lacrimal gland (versus 13%, P < 0.05) (Figure 1), and 5 showed retrobulbar extension. There was no frontal or infraorbital nerve enlargement, as defined by the nerve diameter equal to or larger than that of the ipsilateral optic nerve on coronal imaging, in all 9 OAL patients (0% versus 12%, 0% versus 36%, P < 0.05). Four patients had extra-orbital involvement of IgG4-RD in the parotid glands (n = 4), kidneys (n = 4), lungs (n = 2), liver (n = 1), aorta (n = 1) and mediastinal lymph node (n = 1) (44% versus 65%, P > 0.05). Histologically, obliterative phlebitis and storiform fibrosis were found in 3 and 0 patients with OAL respectively (33% versus 7%, 0% versus 4%, P > 0.05).
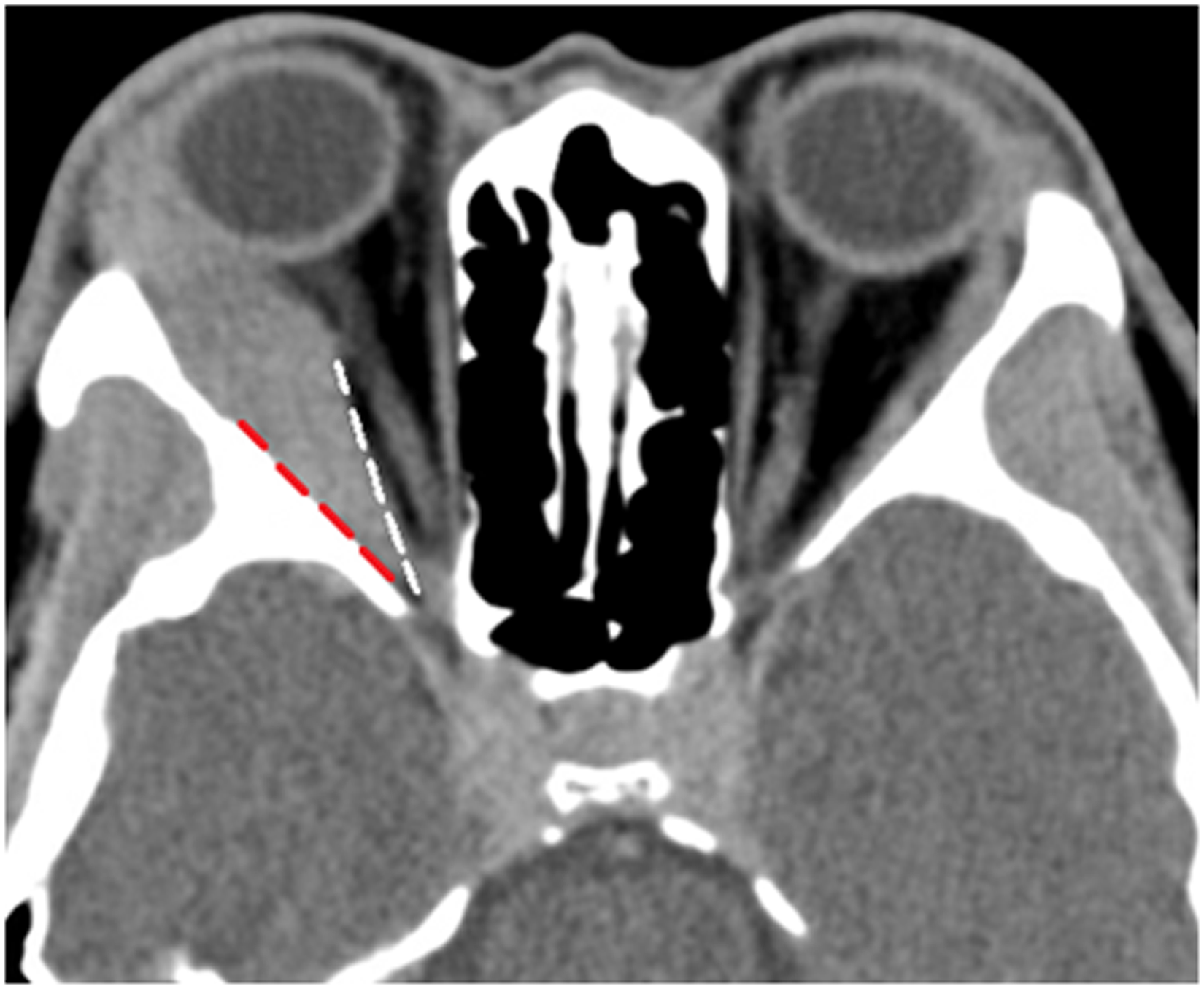
Axial image of computed tomography scan showing the enlarged right lacrimal gland extending back to the orbital apex; previously described as the wedge sign, 16 with the enlarged lacrimal gland restricted to the triangular space between the lateral rectus (white line) and the lateral orbital wall (red line).
Extra-orbital systemic malignancies
Six were diagnosed with extra-orbital malignancies at 38 ± 25 (range: 7–84) months following the diagnosis of IgG4-ROD, while 1 patient with history of breast cancer was diagnosed to have endometrial adenocarcinoma at the time of IgG4-ROD diagnosis. One patient was diagnosed to have primary lung cancer with metastasis based on radiological and serological features. In this patient, multiple hypermetabolic spiculated lesions were found in both lungs and liver with extensive lytic osseous lesions over different long bones on PET-CT scan, and there was a grossly elevated serum carcinoembryonic antigen (CEA) level of 2753ug/L (normal range < = 5). All the specimens of the extra-orbital malignant specimens were undergone additional IgG4 immunostaining, and there was an increased IgG4 + plasma cell infiltration (IgG4/IgG ratio = 49–62%) of the nearby cervix in one patient with endometrial adenocarcinoma. The other malignant lesions did not show any IgG4 + plasma cell infiltration. Comparing the 7 patients with extra-orbital malignancies to those without diagnosing cancer at or after IgG4-ROD diagnosis (106 patients), the age of IgG4-ROD diagnosis (68.3 ± 8.5 versus 55.2 ± 15.0, P < 0.05) was higher and the male to female ratio was also higher (6:1 versus 28:25, P = 0.11) but not reaching statistical significance. Otherwise, the initial clinical presentation, the level of pre-treatment serum IgG4, radiological changes and pattern of extra-orbital IgG4-RD involvement were not statistically different between the 2 groups. The number of patients who received oral corticosteroid (71% (5/7) versus 82% (87/106), P > 0.05)
and the mean cumulative dosage of oral prednisolone (5745 ± 3145 mg versus 6006 ± 4942 mg) were similar between the 2 groups. 29% (2/7) of these patients who were diagnosed with extra-orbital malignancies opted not to receive any treatment in view of their stable IgG4-ROD, compared to 18% (19/106, 17 clinical remissions, 2 against medical advice) of the rest (P > 0.5). None of the 7 (0%) patients received biologic agents, compared to 3 (3%) (2 rituximab, 1 infliximab) in the rest (P > 0.05).
Incidence of malignancies in the study cohort of IgG4-ROD
The overall incidence of OAL was higher (SIRs = 10.0, 95%CI = 4.5–17.6), especially within the first year of IgG4-ROD diagnosis (SIRs = 46.7, 95%CI = 18.5–87.6). The overall, age- and gender-adjusted incidence rates and SIRs of OAL were increased. On the contrary, the overall incidence of extra-orbital malignancies was comparable (SIRs = 0.54, 95% CI = 0.2–1.0) to the general population. The incidence was similar within the first 2 years of IgG4-ROD diagnosis (SIRs = 1.2, 95% CI = 0.4–2.5). The overall, age- and gender-adjusted incidence rate and SIRs of systemic malignancies were similar (Table 4).
Incidence of malignancies in the study cohort.
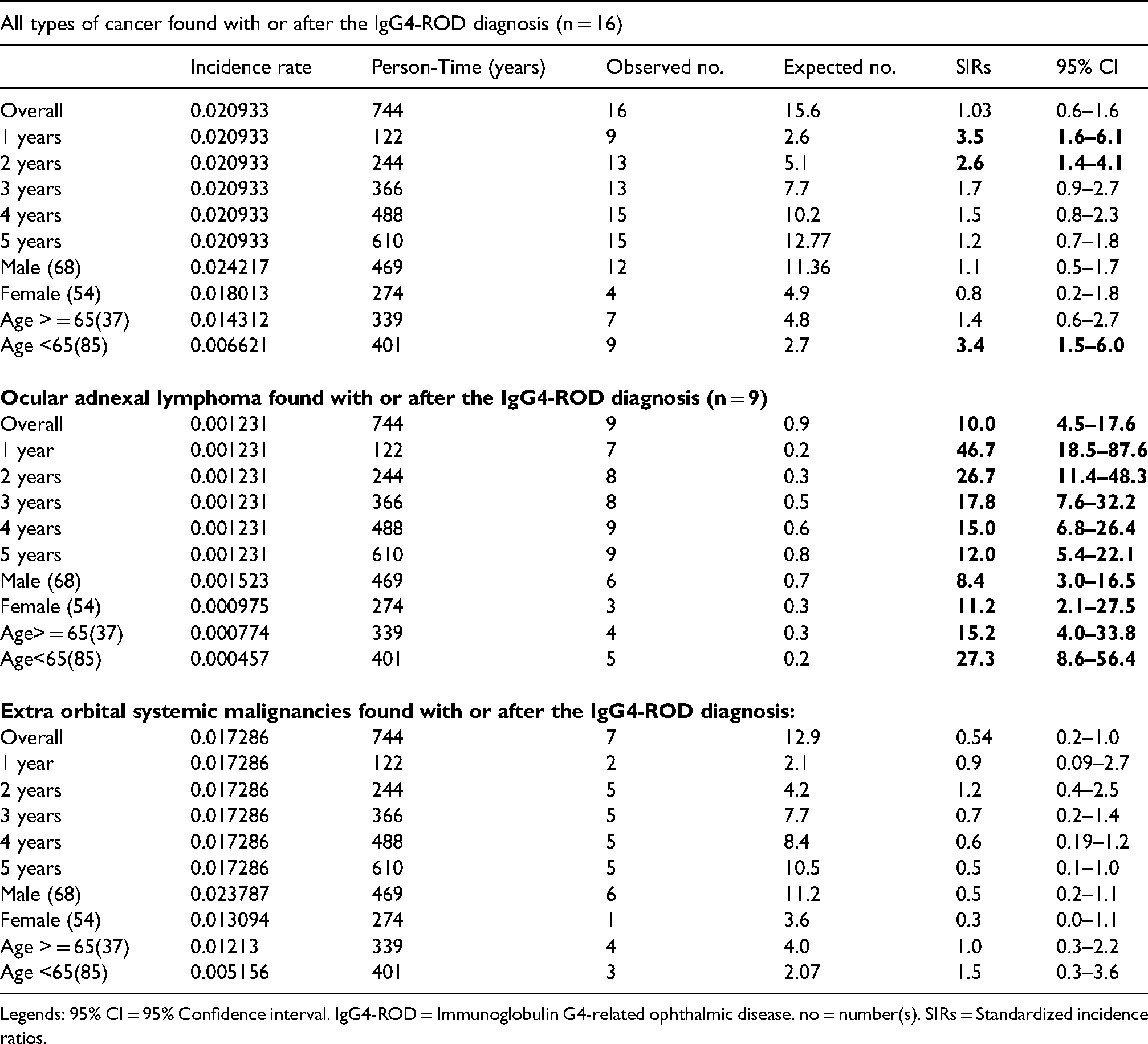
Legends: 95% CI = 95% Confidence interval. IgG4-ROD = Immunoglobulin G4-related ophthalmic disease. no = number(s). SIRs = Standardized incidence ratios.
The overall incidence of malignancies (all types) diagnosed concomitantly with or subsequently after IgG4-ROD was comparable to the general population (SIR = 1.03, 95% CI = 0.6–1.6). The incidence of malignancies (all types) was higher within the first 2 years of IgG4-ROD diagnosis (first year: SIRs = 3.5, 95% CI = 1.6–6.1, first 2 years: SIRs = 2.6, 95% CI = 1.4–4.1) and similar to the level of the general population by the end of the third year (SIR = 1.7, 95% CI = 0.9–2.7)
Discussion
In this multi-centered, territory-wide, and biopsy-proven IgG4-ROD cohort of 122 patients, 16 (13%) patients were diagnosed with cancer at the time of or after IgG4-ROD diagnosis over a follow-up period of 73 ± 48 (12 to 260) months. Nine patients were diagnosed with OAL and 7 patients extra-orbital malignancies including one case of DLBCL of seminal vesicles. Compared to the general population, the overall SIRs of OAL was 10 times higher while that of extra-orbital malignancies was similar. Increased risk of malignancies has been reported in various inflammatory disorders such as Systemic lupus erythematous, 17 Sjogren's syndrome 18 and IgG4-RD. 19 Long-term immunosuppressive therapies and chronic immune dysregulation are likely associated with tumorigenesis. Wallace et al. 9 proposed that both IgG4-RD and malignancies shared similar risk factors, and the increased risk of IgG4-RD might be resulted from the treatment of malignancies such as certain immunosuppressants which adversely affected the immune system.
Some studies reported an association between IgG4-RD and malignancies.19,21 Among epithelial malignancies, colorectal21,22 and gastric 23 cancer showed stronger associations with IgG4-RD. The overall risk of malignancies (all types) was the highest in patients during the first year of the diagnosis of IgG4-related AIP.22,24 Higher incidences of malignancies (including both pancreatic and extra pancreatic cancer) in patients with IgG4-related AIP were reported in 2 studies with comparable SIRs = 2.08 (95%CI:1.32–2.85) 25 and SIRs = 2.7 (95%CI:1.4–3.9). 23 IgG4-related AIP may develop as paraneoplastic syndrome, since non-pancreatic cancerous tissues of 6 patients in one study showed abundant IgG4-positive plasma cells infiltration. 23 In our study, all available tumor specimens from patients with extra-orbital malignancies showed no IgG4-positive plasma cell infiltration, except one patient with endometrial adenocarcinoma, where the IgG4-positive plasma cells infiltrated the nearby cervix but not the endometrial tumor itself.
Yamamoto et al. 19 reported an increased incidence of malignancies after the diagnosis of IgG4-RD over an average follow-up period of 3.1 years. Two of their patients with chronic sclerosing sialadenitis and dacryoadenitis were diagnosed with lung cancer. However, our study was the first to systematically report the risk of OAL and extra-orbital malignancies before and after the histological diagnosis of IgG4-ROD. In contrast to the reported increase in both pancreatic and extra-pancreatic malignancies (lymphoma and carcinoma) in IgG4-related AIP patients,22,23,25 our data showed an increase only in OAL but not extra-orbital malignancies in IgG4-ROD patients. Three patients were diagnosed with breast cancer, DLBCL of an ipsilateral cervical lymph node and prostate adenocarcinoma respectively at an average of 73 + /-40 (range 24–123) months before the diagnosis of IgG4-ROD in our cohort. Meanwhile they had no self-reported or recorded feature of IgG4-RD before malignancies.
Lymphoma was the commonest malignancy associated with IgG4-RD in a report by Ahn et al. 26 Among 46 published cases of IgG4-ROD associated with OAL, 2 cases previously reported by Cheuk et al. 10 were included in the current study. The mean age of diagnosis of IgG4-ROD was 62 (30–90) years (Table 5), while our mean age of diagnosis was 64 (range 54–74) years. Notably, 25 (63%) of the 46 published cases presented as unilateral or asymmetric enlargement of lacrimal glands, comparable to our finding that asymmetric enlargement of the lacrimal gland was associated with OAL (Figure 1). We also found, for the first time, “atypical” presentations of IgG4-ROD including asymmetric lacrimal gland enlargement and lack of frontal or infraorbital nerve enlargement, were associated with OAL.
Published cases of IgG4 related ocular adnexal lymphoma (OAL).
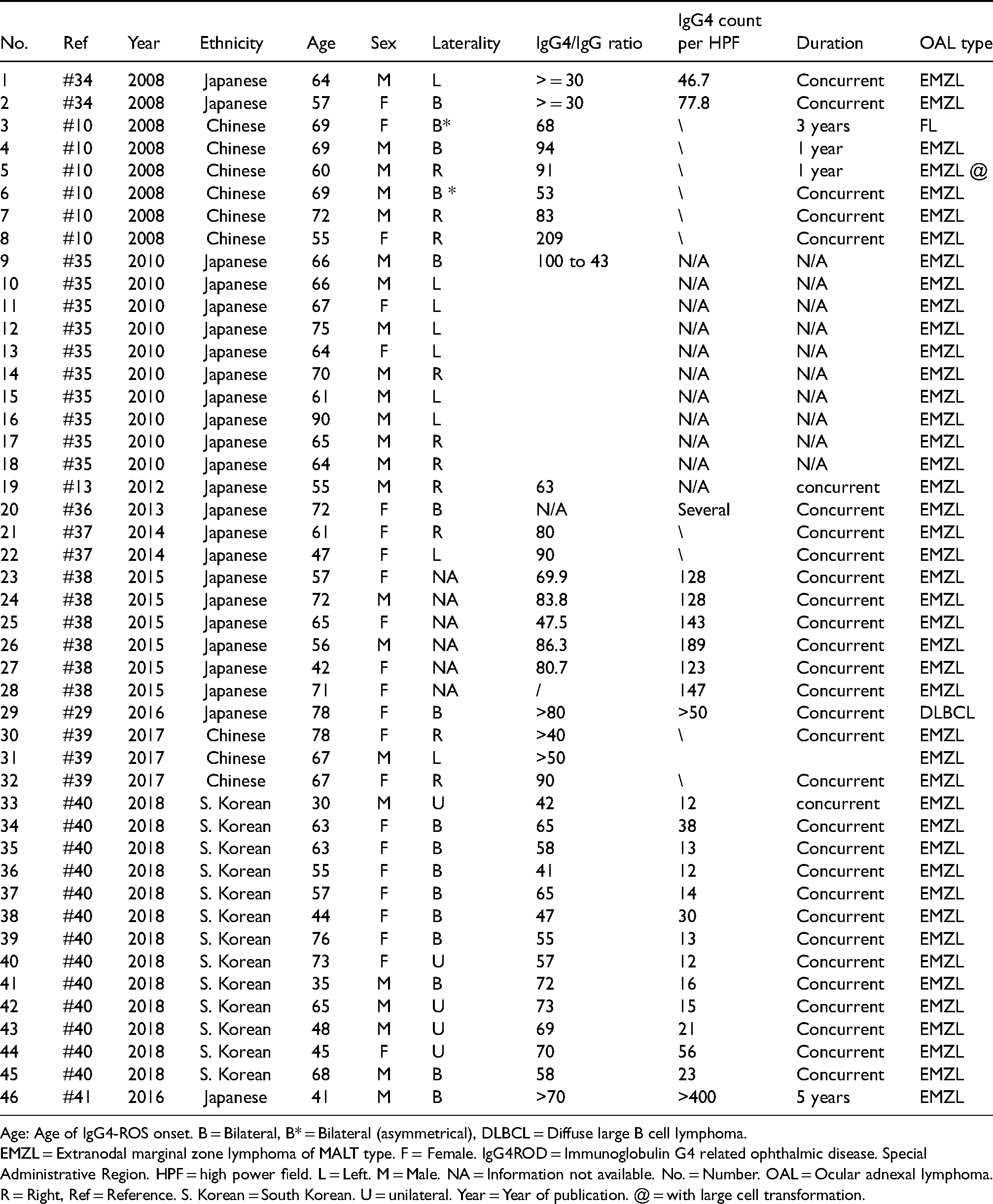
Age: Age of IgG4-ROS onset. B = Bilateral, B* = Bilateral (asymmetrical), DLBCL = Diffuse large B cell lymphoma.
EMZL = Extranodal marginal zone lymphoma of MALT type. F = Female. IgG4ROD = Immunoglobulin G4 related ophthalmic disease. Special Administrative Region. HPF = high power field. L = Left. M = Male. NA = Information not available. No. = Number. OAL = Ocular adnexal lymphoma. R = Right, Ref = Reference. S. Korean = South Korean. U = unilateral. Year = Year of publication. @ = with large cell transformation.
Sato et al. 12 reported 7 cases of ocular extranodal marginal zone lymphoma (EMZL) associated with IgG4-ROD. The Japanese prevalence study group of orbital lymphoproliferative disease 11 reported 9.8% (n = 44) of MALT lymphoma cases being IgG4 positive, and the mean age of patients with IgG4-positive MALT lymphoma was significantly higher than those with IgG4-ROD alone. One of our patients was diagnosed with IgG4-ROD 4 years before orbital EMZL showing positive light chain restriction among the IgG4 + plasma cells, indicating the malignant transformation of lesions in IgG4-ROD over time. On the other hand, a Japanese patient developed IgG4-ROD 10 years after receiving external beam radiotherapy for orbital MALT lymphoma. 27 Meanwhile one of our patients was diagnosed with EMZL affecting the left lacrimal gland 2 months prior to the right lacrimal gland becoming clinically enlarged. The right lacrimal gland was affected by IgG4-ROD alone as confirmed by histology. While IgG4 positive MALT lymphoma may evolve secondary to the lymphomatous transformation of longstanding IG4-ROD 12 and thus the older age on presentation, it may also be originated from de novo development of IgG4-producing MALT lymphoma in older patients.
One of our patients developed diffuse orbital DLBCL, which is extremely rare in IgG4-ROD. The contralateral lacrimal gland showed atypical Hodgkin-like cells. Subsequent negative PET-CT scan and kappa light chain restriction of plasma cells excluded bilateral IgG4-related OAL. We found other reported case of DLBCL in IgG4-ROD involving the lacrimal sac. 28 One of our male patients developed DLBCL of the seminal vesicles 5 years after the IgG4-ROD diagnosis and also suffered from infiltrative IgG4-related optic neuropathy as previously reported. 29
Hiwatashi et al. 30 proposed the use of non-echo planar (NEP) diffusion-weighted imaging (DWI) to obtain the apparent diffusion coefficient (ADC) of any region of interest to differentiate OAL from IgG4-ROD. Since diagnosis of OAL requires histological confirmation, we recommend sampling the region of lowest ADC if DWI is available and repeating biopsy in previously stable IgG4-ROD patients with noticeable unusual worsening of periocular swelling or proptosis. Three of our OAL patients had prior biopsies showing lymphoid hyperplasia (n = 2) or chronic dacryocystitis (n = 1). Whether the use of MRI or NEP-DWI guided biopsy reduces sampling errors in IgG4-related OAL warrants further investigation.
Our data suggested that patients with “typical” presentations of IgG4-ROD including bilateral symmetrical lacrimal gland, frontal or infraorbital nerve involvement had a lower risk of OAL. We therefore recommend clinical surveillance every quarterly in IgG4-ROD patients presented with asymmetric lacrimal gland involvement during the first 2 years from diagnosis. If clinically suspicious, radiological workup, e.g. MRI and DWI for ADC or PET-CT, should be arranged to look for radiological evidence of OAL and to arrange image-guided biopsy as appropriate.
There are several limitations in the present study. Firstly, this was a retrospective multi-center study with inherent differences in the documentation. Secondly, our cohort consists of only ethnic Chinese patients, and the risks of malignancies in IgG4-ROD may vary among different study populations. Thirdly, one patient was diagnosed to have primary lung cancer with metastasis by the parent team based on the PET-CT findings and elevated serum CEA level. Histological confirmation was absence. Fourthly, patients were managed under divergent protocols at different collaborating centers, and patients had undergone different extents of investigations for extra-ophthalmic IgG4-RD involvement. Our data may serve as a reference for future prospective cohort studies to study the systemic involvement in IgG4-ROD. Fifthly, 17 patients did not fulfil the definite diagnosis in the comprehensive diagnostic criteria for IgG4-RD. We included also biopsy proven IgG4-ROD patients with normal serum IgG4 level because the the percentages of IgG4-RD patients with elevated serum IgG4 ranged from 50 to 90%,31,32 and importantly, no difference of the baseline serum IgG4 level was observed between patients with or without malignancies in our cohort. Sixthly, we acknowledge possible incidental occult malignancies which were developed years before and attributed to an increase in malignancy, especially during the first few years after IgG4-ROD diagnosis. Large and prospective cohorts are needed to study the long-term association of malignancies in IgG4-RD patients with different affecting organs, and understand the potential malignant transformation risks 33 of using immunosuppressive or biologic agents in IgG4-RD patients.
Conclusion
In this cohort of 122 biopsy-proven IgG4-ROD patients, the incidence of OAL was 10 times higher while the incidence of extra-orbital malignancies was similar to that of the general population. IgG4-ROD patients presenting with asymmetric lacrimal gland enlargement, lack of frontal or infraorbital nerves involvement radiologically were associated with OAL.
Footnotes
Acknowledgements
We thank the Department of Anatomical and Cellular Pathology, The Chinese University of Hong Kong, Department of Pathology, United Christian Hospital; Department of Pathology, Pamela Youde Nethersole Eastern Hospital; Department of Pathology, Queen Elizabeth Hospital for their support in terms of data retrieval. We would like to acknowledge Ms Angela Po Ling Ho, for her important contributions to data retrieval for this work.
Ethics approval
This study followed the Declaration of Helsinki and ethical approval was obtained from the Institutional Review Board (IRD) of each participating hospital as following:
Joint Chinese University of Hong Kong- New Territories East Cluster Ethics Committee: 2020.478 New Territories West Cluster Ethics Committee: NTWC/CREC/17097 Kowloon Central Kowloon East Clusters Ethics Committee: KC/KE-17-164/ER-2 Kowloon West Cluster Ethics Committee: KW/EX-17-149(117-16) Hong Kong East Cluster Ethics Committee: HKECREC-2017-75 Hong Kong West Cluster Ethics Committee: UW18-120 Hong Kong Sanatorium & hospital Ethics Committee: RC-2017-16
Consent for publication
Not applicable. The research involves no more than minimal risk to subjects, and the waiver will not adversely affect the rights and welfare of the subjects. The need for consent is deemed unnecessary according to the institutional regulations with approval to the wavier.
Abbreviations
Authors contributions
KL, JY, KW and KC analyzed and interpreted the data. CW performed the histological review of specimens. KL and KC were the major contributors in writing the manuscript. All authors read and approved the final manuscript.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.