
Abstract
Introduction
To report a late onset, deep stromal and endothelial corneal scar in a keratoconus patient after corneal collagen cross-linking (CXL).
Case description
Observational case report. A 29-year-old man with bilateral keratoconus received an accelerated (A-CXL 10*9) epithelium-off CXL procedure in the left eye.
6-months postoperatively, a 2.2 × 1.2 mm inferocentral corneal scar was detected, which was located in the posterior stroma ranging from approximately 350 µm until the endothelium, therefore was situated below the demarcation line. A topical corticosteroid treatment did not influence the magnitude or configuration of the scar. Visual acuity was never affected, which includes the examination 12 months postoperatively.
Conclusions
We report a case of a late onset deep stromal and endothelial corneal scar 6 months after accelerated CXL as postoperative complication without affecting visual acuity.
Keywords
Introduction
Over the course of the Last decades, corneal collagen crosslinking (CXL) with the application of riboflavin and the exposure to ultraviolet-A light has become the gold standard for treating progressive keratoconus. 1 This treatment is safe and highly efficient, when complied with safety standards. Nevertheless, there have been reported a few complications in the literature such as sterile corneal infiltrates, 2 corneal haze and scars, 3 keratitis and perforation, herpetic keratitis or corneal ulceration with melting.4,5
Transient corneal haze is a very common complication, while persistent scars are rare and only few cases are reported in the literature. Usually they are located in the anterior stroma and appear within the early postoperative period. 5
This case report describes a late onset deep stromal and endothelial scar as a rare postoperative complication after CXL.
Case description
A 29-year-old man was referred to our clinic on August 2019 with progressive bilateral keratoconus. The patient specified neither ocular diseases nor injuries in the past nor medical history of systemic diseases. In the slit-lamp examination we observed bilateral Fleischer rings on the cornea, but otherwise no corneal pathologies. Further ocular examination was inconspicuous in both eyes. The corneal topography using Scheimpflug imaging (Pentacam ® , Oculus, Germany) showed an inferior steepening and asymmetric bow-tie sign in the left eye (Figure 1). The patient was classified as stage 2 keratoconus according to the Amsler-Krumeich classification, 6 which includes the absence of central corneal scars, astigmatism of 5.2 diopters, an average K value of 49.2 diopters and a minimal apical corneal thickness of 423 µm. Numerical parameters are shown in Table 1.
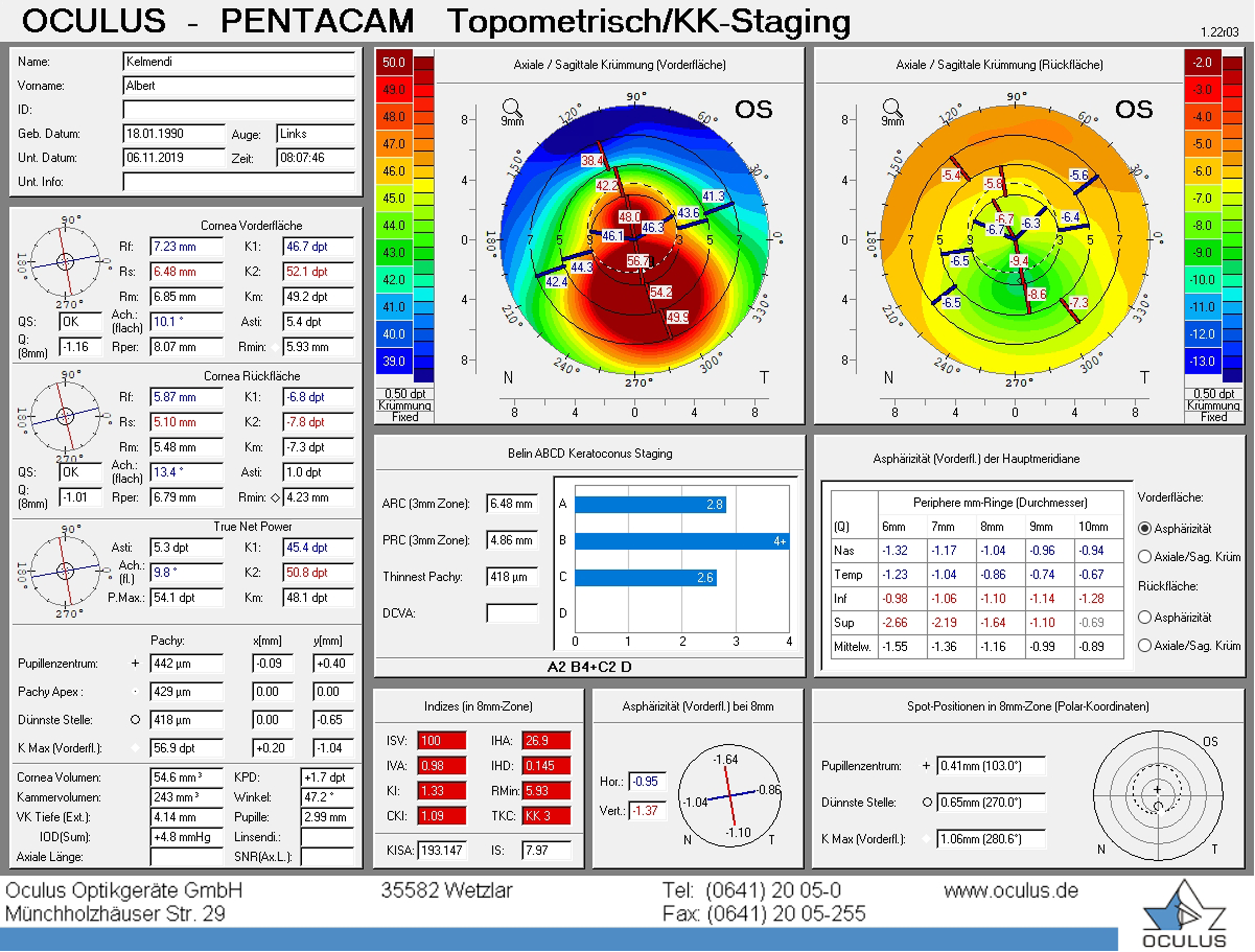
Preoperative corneal topography using Scheimpflug imaging (Pentacam ® , Oculus, Germany) showed an inferior steepening and asymmetric bow-tie sign.
Corneal topography in the left eye using Scheimpflug imaging (Pentacam®, Oculus, Germany) at each time of investigation.
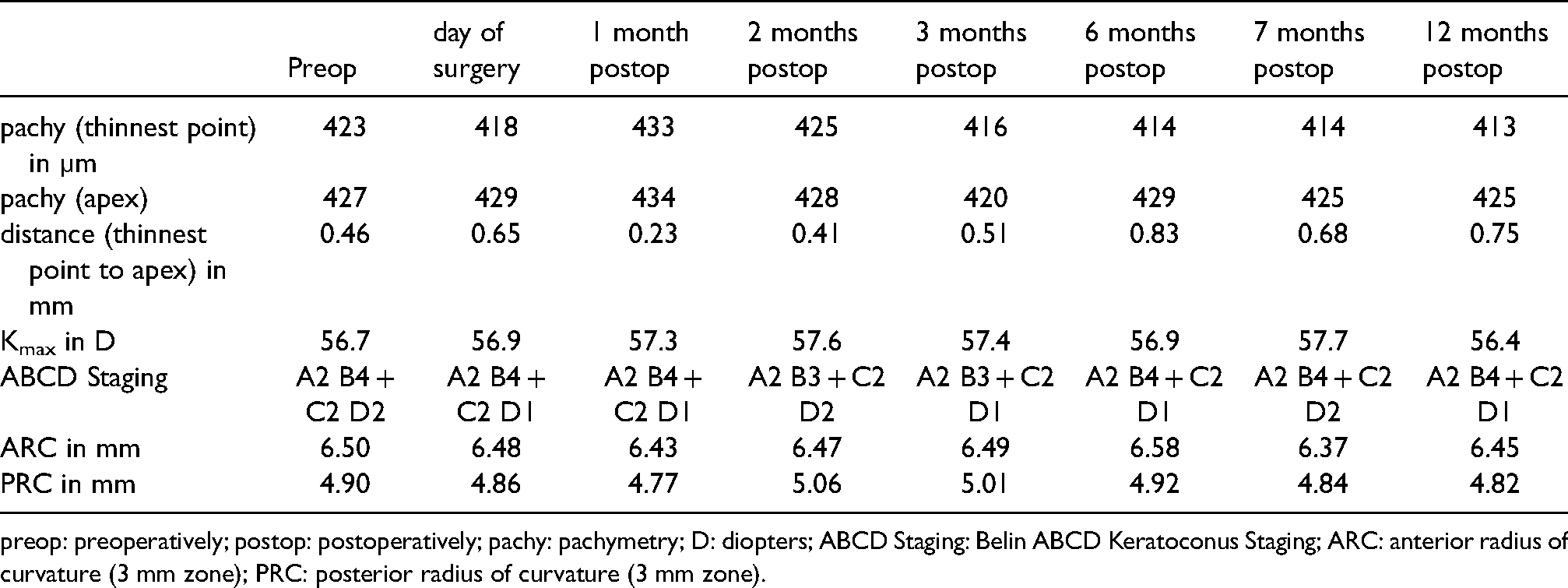
preop: preoperatively; postop: postoperatively; pachy: pachymetry; D: diopters; ABCD Staging: Belin ABCD Keratoconus Staging; ARC: anterior radius of curvature (3 mm zone); PRC: posterior radius of curvature (3 mm zone).
Accelerated CXL was conducted in November 2019 on the left eye. A rigid contact lens was worn until the day of the surgery. After topical anesthesia using 0,4% oxybuprocain (Novesine®, OmniVision GmbH, Germany) the epithelium was removed mechanically over the central 9 mm of the cornea. Riboflavin (0.1%) solved in hydroxypropyl methylcellulose (HPMC) (VibeX Rapid™, Avedro Inc., USA) was instilled to the cornea every minute for 10 min before ultraviolet-A light irradiation. The corneal thickness was measured with the handheld iPac® pachymeter (Reichert Inc., USA) after epithelium removal and application of riboflavin to ensure a thickness greater than 400 μm. Then, the cornea was exposed to ultraviolet-A light (KXL® system, Avedro Inc., USA) with an irridiance of 9 mW/cm2 for 10 min (A-CXL 10*9) resulting in a total energy of 5.4 J/cm2. During the irradiance, riboflavin drops were continued every 2 min. Postoperatively, a bandage contact lens was placed on the eye until complete re-epithelialization 5 days postoperatively. The patient was instructed to use 0.3% topical ofloxacin (6 times a day) (Floxal® eye drops, Bausch & Lomb GmbH, Berlin) for one week and 0.1% topical dexamethasone (4 times a day) (Monodex® eye drops, Laboratoires Thea, France), which was tapered off over 4 weeks. In addition, preservative free artificial tears (hourly) (Vismed® eye drops, TRB Chemedica AG, Swiss) and 400 mg dexibuprofen pills (up to 3 times a day if required) (Seractil forte 400mg® film-coated tablets, Gebro Pharma GmbH, Austria) were recommended. After the uneventful CXL and initial postoperative investigation, follow-up examinations were arranged 1, 2, 3, 6 and 12 months after surgery.
1 week after CXL on the left eye, the patient was free of pain and postoperative findings showed a subtle ciliary congestion. At the 1, 2 and 3 months follow-up, slit-lamp examination of the left eye showed no signs of infection, inflammation or scarring and corneal topography reveals a stop for the disease's progression as can be seen in Table 1.
6 months postoperatively, a deep teardrop shaped corneal scar of 2.2 × 1.2 mm, corneal guttae and vogt's striae were observed, which were localized inferocentral adjacent to the apex of the cone (Figure 2).

Slit-lamp image unveiled a corneal scar of 2.2 × 1.2 mm 6 months postoperatively, which was localized inferocentral.
The anterior segment optical coherence tomography (OCT) (Spectralis®, Heidelberg Engineering, Germany) showed a faint demarcation line at a depth of approximately 250 µm and a stromal scar ranging from 350 µm until the endothelium (Figure 3).
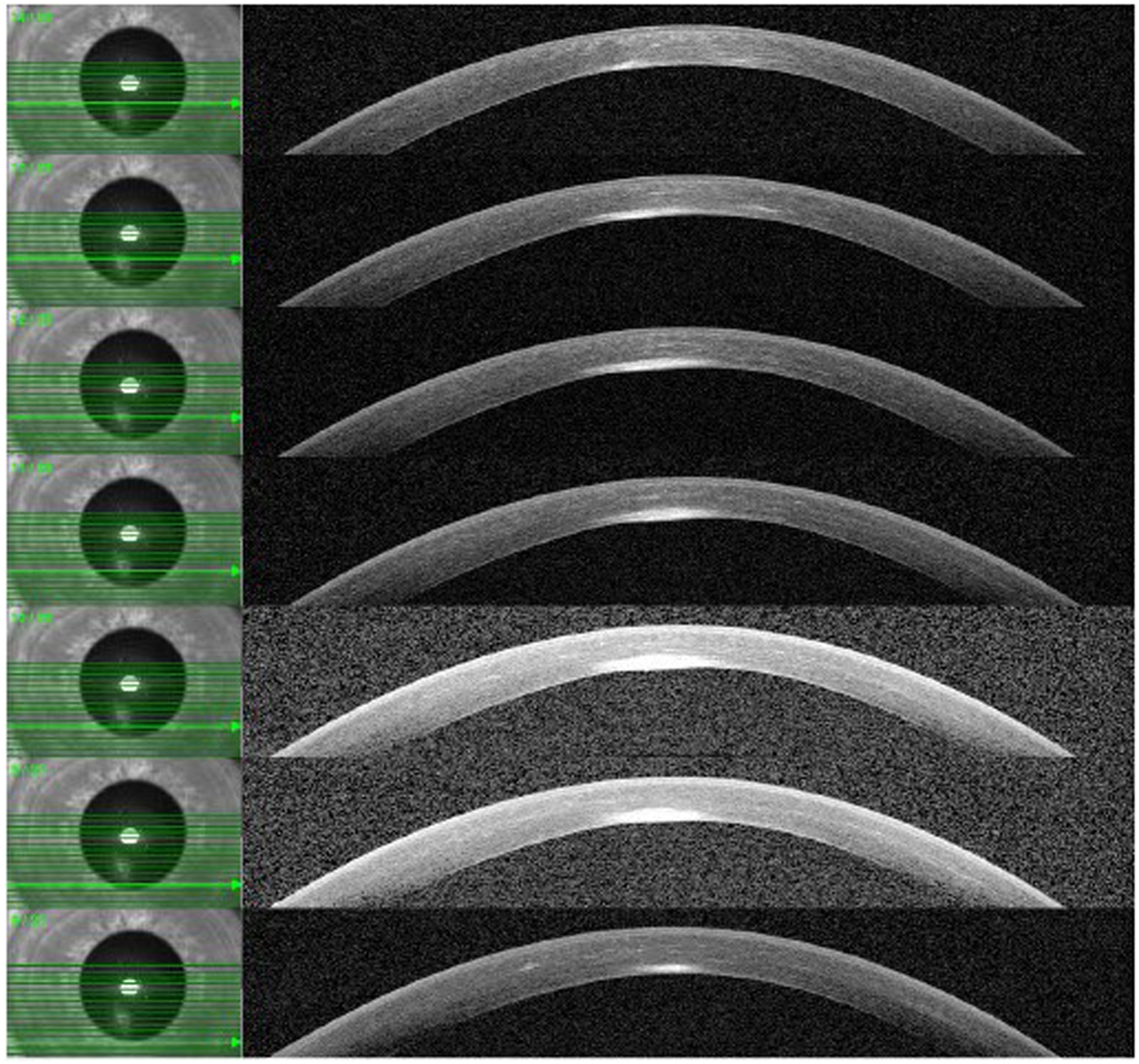
Anterior segment OCT revealed multiple anterior-segment morphologic alterations in single acquisition images.
Corneal endothelial cell density revealed comparable values in both eyes (right eye = 2816 cells/cm2; left eye = 2745 cells/cm2). Scheimpflug parameters such as pachymetry, Kmax and the ABCD Staging remained stable over the whole postoperative period (Table 1). Neither was the visual acuity affected at any time. A topical corticosteroid treatment (5 times per day tapered off over 5 weeks) (Softacort® eye drops, Laboratoires Thea, France) was started in addition to preservative free artificial tears up to 6 times a day.
During the subsequent examinations one to 6 months later, no significant change in shape and density of the scar as well as in Scheimpflug parameters and endothelial cell count was detected. Further treatments with topical steroids did not show a positive influence on the course. At the latest follow-up appointment 12 months postoperatively, visual acuity was 0.2 logMAR with contact lenses, which was equal to our examinations pre- and 3 months postoperatively. No additional visual impairment such as photophobia was reported. Pachymetry was 413 µm at the thinnest point and therefore similar to the examinations previously alongside the other relevant parameters for progression of keratoconus, which is shown in Table 1. Therefore, no further treatments are planned to date.
The right eye underwent an accelerated epithelium-off CXL procedure in December 2019 as well, including the same postoperative medications and follow-up appointments, but no complications, such as corneal scarring in particular did occur.
Discussion and conclusions
CXL is a successful technique for arresting progressive keratoconus. However, CXL is known to be a safe procedure, few postoperative complications are known. They can be subdivided into early postoperative complications such as sterile infiltrates, delayed epithelial healing, infections, haze and endothelial failure or late onset complications such as corneal scars, which occur typically one month postoperatively or later. Latter are very rare and only a few cases are reported in the literature.4,7 A clear differentiation from very common corneal haze has to be made. Haze occurs typically already a few days postoperative and is located in the anterior stroma ranging until the demarcation line, what is assumed to be the posterior limit of the crosslinked tissue.8,9 Haze is usually transient and can be treated with corticosteroids successfully. 10
In the literature there are few cases of postoperative scaring reported. Güell et al. 3 found a deep stromal scar but after combined PRK and CXL in a case of forme fruste keratoconus which was resistant to continuous steroid therapy over more than one year. Kato et al. 7 reported 3 cases of deep stromal scars post CXL. In two of these cases the epithelium was removed with the excimer laser, what might have a disadvantageous influence on the healing process leading to a similar reaction as described by Güell and coworkers. In PRK the haze formation is triggered differently and might play a major role in those cases. 11 Lim et al. 12 reported the appearance of two approximately 300 µm deep scars which appeared 3 months postoperatively. In contrast to our findings, the scars did not reach the endothelium, but were located in the transition zone between crosslinked tissue and the underlaying stroma linked to the demarcation line. Other reports of scars are usually limited to the anterior part of the cornea 4 and are often not clearly distinguished from early postoperative haze. 13
In the presented case normal early postoperative healing phase was observed. After 3 months, no haze or other corneal opacities was reported. No additional risk factors such as preexisting ocular diseases, far progressed keratoconus and no intra- or early postoperative complications did occur. As the scarring is not in the anterior part of the cornea, which is assumed to be crosslinked, has no connection to the demarcation line and appeared only about six months postoperatively, it does not seem to be related to intraoperative interactions. While most healing processes take place earlier, the repopulation of keratocytes of the crosslinked tissue is assumed to take place approximately 6 months postoperatively and might play a role in inducing the scar present in this case, though it was shown, that the deep stroma is not affected by CXL with in vivo confocal microscopy. 14
Due to the localization of the scar in the posterior stroma with contact to the endothelium, an endotheliitis is a considerable cause, as previously reported as a rare complication after CXL, but never with consecutive scarring so far. 15 As corneal edema is present in several patients after CXL 16 the endothelium seems to be affected to a certain point in those cases. What speaks up against this theory is the fact, that the patient didn't show any other symptom like pain, keratoprecipitates or corneal edema at any visit. In contrast to the previously reported cases this scar occurred only after an irritation free period and more than 3 months after the CXL, what was never described before. Nevertheless, an endotheliitis seems the most probable cause to us. Further investigations, such as anterior chamber-puncture to search for a viral cause of the endotheliitis were not conducted, as there was no activity seen at any visit and the symptoms did not worsen. Furthermore, a confocal microscopy could have delivered additional information about the detailed morphology of the affected stromal tissue and is be recommended in subsequent cases.
To the best of our knowledge, this is the first report of a late onset of a deep stromal scar following CXL. In this case, the presence of the deep stromal and endothelial scar had no detrimental effect on the outcome of the therapy, and no other complications were reported 12 months after surgery. However, clinicians should be aware that late onset complications after CXL are possible and continuous follow-up examinations should be conducted.
Declarations
None of the authors has a financial interest in any of products, devices or drugs mentioned in this manuscript. No funding was received for this work. This study has been reviewed by the JKU-ethics committee (Johannes Kepler University; Medical Faculty) and has therefore been performed in accordance with the ethical standards laid down in the Declaration of Helsinki 1964 with actual revisions. The person gave the informed consent prior to the inclusion in the study according to the guidelines in SOP06 V1.0. Data sharing is not applicable to this article as no datasets were generated or analysed during the current study. All authors read and approved the final manuscript. Acknowledgements: Not applicable.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.