
Abstract
Purpose
To report on the outcome of surgical submacular choroidal neovascular membrane (CNV) removal in children and to perform a comprehensive review of literature concerning this intervention in children.
Methods
In this retrospective, noncomparative, interventional case series, we included 8 eyes of 7 consecutive children with subfoveal choroidal neovascularization treated by pars plana vitrectomy (PPV) and CNV removal. Main outcome measures were visual acuity and complications.
Results
Mean age at surgery was 8.6 ± 5.2 years (range: 2–16). Two out of 8 eyes were idiopathic. Corrected-distance visual acuity (CDVA) improved from 1.01 ± 0.45logMAR (range:0.3–1.5) at presentation to 0.60 ± 0.37 (range:0–1) at last follow-up (p = 0.03). Mean follow-up was 3.9 ± 3.9 years. Six eyes received at least one intravitreal injection of bevacizumab prior to surgery. Recurrence occurred in one eye with Best's disease.
Literature review revealed a total of 42 cases with the most frequent etiologies being Presumed ocular histoplasmosis syndrome (POHS) and idiopathic CNV. Considering all cases together, mean CDVA improved from 1.00 ± 0.37logMAR to 0.52 ± 0.42 (p < 0.01). CNV recurrence occurred in 11 eyes (22.0%), 7 of which had an inflammatory etiology. Other complications included pigment epithelium tear, atrophy and retinal tear.
Conclusion
Surgical removal of CNV is a viable, effective and safe option in children with persistent submacular neovascular membranes.
Introduction
Choroidal neovascularization (CNV) is characterized by the development of abnormal choroidal vessels that breach the Bruch's membrane. They can develop to enter the space under the retinal pigment epithelium (type 1 CNV) or under the neurosensory retina (type 2 CNV). 1 Although most commonly reported in adults and elderly, mainly secondary to age-related macular degeneration (AMD) and high myopia, it has also been reported to occur in children. 2 In the latter, however, etiologies are often different than in adults and include inflammatory or infectious diseases and hereditary maculopathies, such as Best dystrophy and Stargardt disease.1,3 A common subtype is the idiopathic one. It is unilateral in most cases. 4
CNV is usually associated with a significant decrease in visual acuity (VA) both in adults and in children, especially if the macula is involved. However, the burden of visual loss and blindness is greater in children than in adults, due to more significant disability-adjusted life years (DALY). 5
Goshorn et al. have shown in a cohort of 25 children (27 eyes) that more than half of the untreated CNVs regressed with time (11 out of 19 eyes) and that 82% of the cases that regressed (9 out 11 eyes) achieved a final VA of 20/50 or better. The remaining cases had a final visual acuity of 20/200 or worse. Furthermore, most of the children with an initial VA of 20/200 or less maintained a similarly low final VA, suggesting that initial VA predicted final VA.6,7
CNV in children usually presents with less associated fundus anomalies and grows within the subsensory retina on a solitary in-growth site.8–10 In adults, CNV is usually associated with macular degeneration or pigment epithelium anomalies and grows through multiple entry sites into the sub-pigment epithelium space. Due to these differences, treatment and prognosis differs between adults and children and makes a surgical excision of the CNV in children a more appealing surgical option than in AMD or myopia. 11
Only a few studies have reported on the outcome of surgical management of submacular CNV in children and none since the development of treatment by anti-vascular endothelial growth factor (VEGF) intravitreal injection.7,11–18 With 16 eyes, Uemura and Thomas reported the largest series in young patients with an age ranging from 7 to 17. 12 The youngest case reported in literature was a 21-month old boy. 18
The aim of the present study is to report on the authors’ clinical experience with subretinal CNV excision in the pediatric population and to review the literature.
Methods
In this retrospective consecutive case series all children that underwent pars plana vitrectomy (PPV) for the excision of a subfoveal CNV at the Fondation Ophtalmologique Adolphe de Rothschild (FOR) between the 1st of January 2005 and the 30th of September 2018 were enrolled. All patients were operated by the same surgeon (GC). The parents of all children signed an informed consent prior to the surgery. Retrospective analysis of data was approved by the institutional review board of the FOR and the study adhered to the tenets of the Declaration of Helsinki.
Patients were examined preoperatively and postoperatively at week 1, month 1, 3, 6 and every 6 months thereafter. In case of postoperative complications, visits were adjusted individually. Demographic, ophthalmic, systemic data, and family history were recorded for every patient. Preoperatively and at every postoperative visit, all patients underwent a complete ophthalmological exam including corrected distance visual acuity (CDVA), anterior and posterior segment evaluation with the slit-lamp and the indirect ophthalmolscopy, with an emphasis on the status of the lens, the macula and the optic nerve. CDVA was measured using a Snellen chart and then converted to logMAR. A spectral domain optical coherence tomography (SD-OCT; Heidelberg Spectralis, Heidelberg, Germany) was obtained preoperatively and at every post-operative follow-up visit. Two children were unable to receive an OCT examination preoperatively, because the machine was not available. A fluorescein angiography was obtained preoperatively for all children, and postoperatively only when a recurrence was suspected. Angiography was performed using a Heidelberg angiograph (Heidelberg Spectralis, Heidelberg, Germany). Figure 1 shows an exemplary fundus photograph, fluorescein and indocyanine green angiogram of patient 5. Figure 2 shows the pre- and postoperative OCTs of patients 1–5. Investigations were performed to search for the etiology of the CNV. Children with family history and ophthalmological examination in favour of Best disease were considered to have the disease without the need to undergo a genetic examination. The remaining cases underwent a genetic examination before considering the CNV as idiopathic.
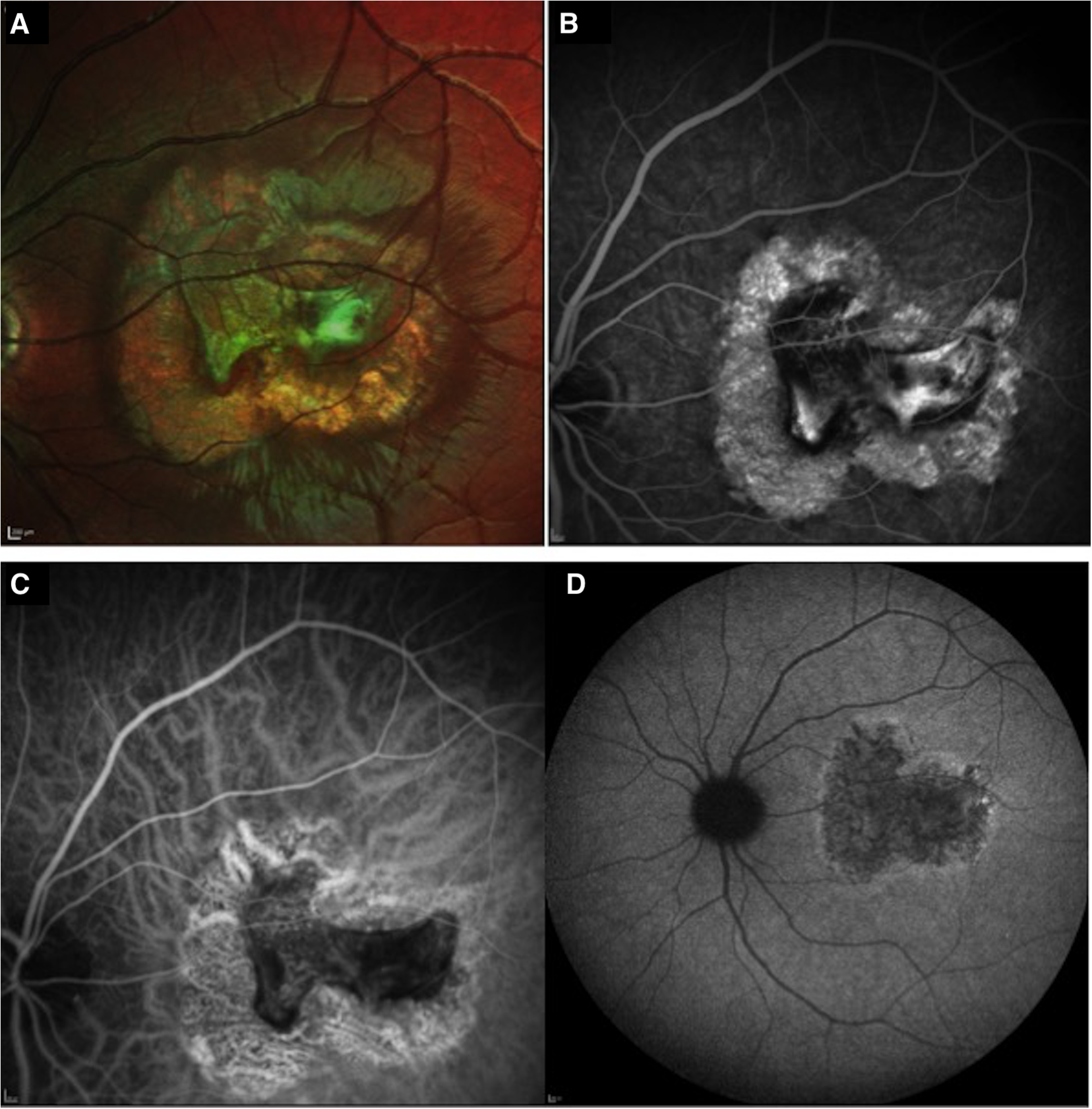
Preoperative fundus photograph (A), early fluorescein angiography phase (B), early (C) and late (D) indocyanine green angiography (ICGA) of patient five shows a classic subfoveal choroidal neovascular (CNV) membrane with atrophy surrounding the CNV.
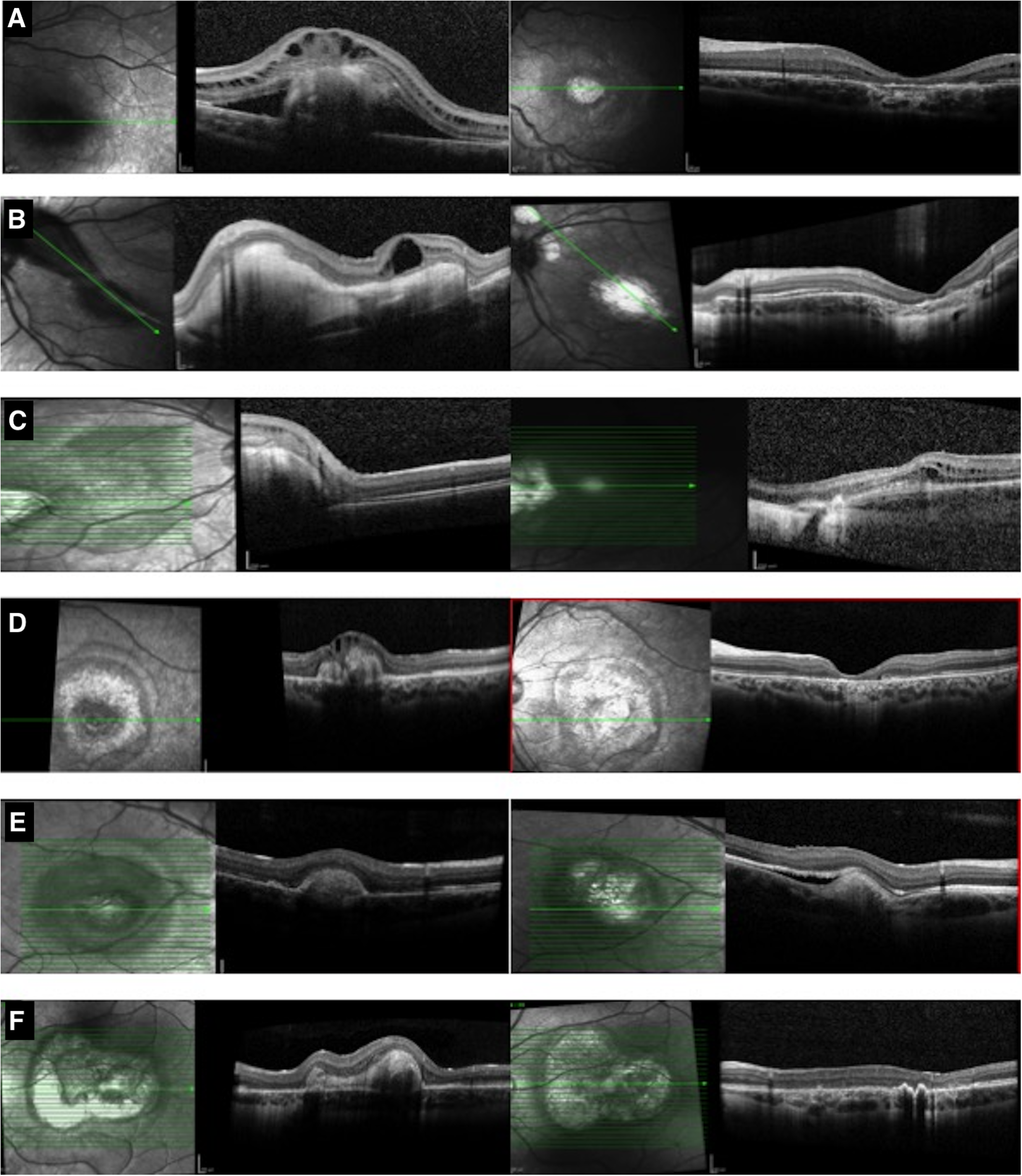
Shows on the left the preoperative OCTs and on the right the postoperative OCTs at last follow-up of children cited in Table 1. A is for child 1, B and C are for the left and right eye respectively of child 2, D is for child 3, E is for child 4, and F is for child 5. The OCTs of patients 6 and 7 were not included because the preoperative OCTs were not available.
Initial characteristics, postoperative visual acuity and complications of included patients. CDVA: Corrected-distance visual acuity; IVI: Intravitreal injection of Bevacizumab.
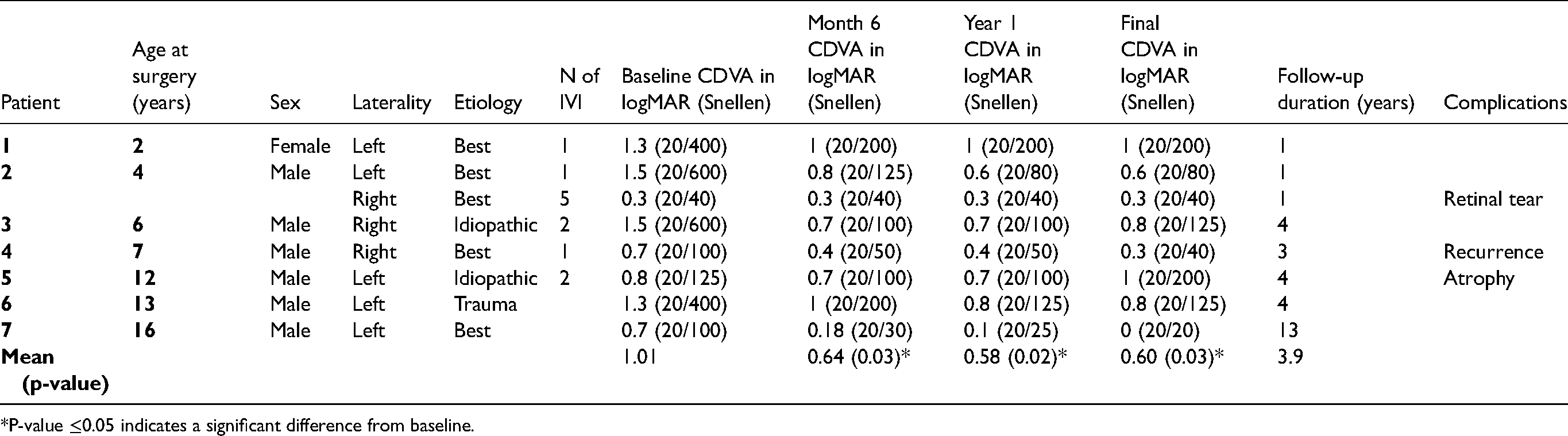
*P-value ≤0.05 indicates a significant difference from baseline.
After the year 2007 all children that presented to the clinic received at least one intravitreal injection (IVI) of 1.25mg of Bevacizumab (Avastin, Genentech Inc., San Francisco, CA) under general anesthesia prior to deciding on surgery. The indication for surgery was a low visual acuity secondary to a CNV ( ≤ 20/200), recurrence of the edema after at least two intravitreal injections or a thick fibrotic scar.
Surgical protocol
Patients were operated under general anesthesia as previously described by Sears et al. 7 In brief, a 25-gauge 3 port PPV using a surgical vitrectomy system (Constellation Vision System, Alcon surgical, Texas, USA) was performed followed by a posterior vitreous detachment. The right sclerotomy was enlarged to 20G and a localized retinal detachment was initiated after performing a small retinotomy at the posterior pole superior to the CNV membrane using a bent 32-gauge infusion cannula. The same cannula was used to dissect the CNV from the overlying retina and the underlying retinal pigment epithelium. Once the CNV was liberated, a retinal forceps (1286O forceps, DORC, Zuidland, the Netherlands) was used to grasp and remove the membrane. If bleeding occurred, intraocular pressure was increased until the bleeding stopped. Fluid-air exchange was performed at the end of the surgery and the sclerotomies were sutured. (Surgical video as supplementary material)
For the literature review, 2 of the authors (YAM and SK) conducted an online search of published articles in the Pubmed database on the 30th of April 2019. The initial search was done using the following keyword combination: (“subfoveal” or “choroidal neovascularisation” or “choroidal neovessel”) and (“children” or “pediatric” or “child”) and (“vitrectomy” or “surgery” or “removal”). Studies related to subfoveal CNV surgical removal were selected based on their titles and abstracts and were obtained and read in full. The reference list of each included study was manually screened for additional articles. Excluded studies were animal studies, experimental models and articles not written in English. Both authors unanimously agreed on the final selection of studies. For the evaluation of outcome, complications, and etiologies, the cases found in literature were combined with the cases reported in the present study. In order to facilitate comparison, CDVA from our patients was converted from Snellen to logMAR.
Statistical analysis
Data was collected and statistically analysed using SPSS (version 22.0, Inc., Chicago, IL). Descriptive statistics were reported as mean ± standard deviation for continuous variables and as percentage for categorical variables. A Wilcoxon rank test was used to compare continuous parameters and a Fisher's exact test was used to compare categorical parameters. P-Value <0.05 was considered as statistically significant.
Results
Overall, 8 eyes of 7 patients (6 males; 1 female) were included. Median age at surgery was 7 years (mean: 8.6 ± 5.2; range: 2–16). Median follow-up was 3.5 years (mean: 3.9 ± 3.9; range: 1–13). Etiologies were idiopathic (2 eyes), Best's disease (5 eyes) and post-traumatic (1 eye). Six eyes (75%) received a median number of 1.5 IVI of Bevacizumab (mean: 2.0 ± 1.5; range: 1–5). Table 1 presents baseline characteristics of all included eyes. Children 1 and 2 were found to have an autosomal recessive Best disease on genetic testing, children 4 and 7 had a family history and ophthalmological examination in favour of Best disease. Children 3 and 5 had a negative genetic testing.
Mean CDVA improved from 1.01 ± 0.45logMAR (range: 0.3–1.5) at presentation to 0.60 ± 0.37 (range: 0–1) at last follow-up (p = 0.03). CDVA improved in 6 eyes, decreased in one eye and remained stable in one eye. Figure 3 plots pre- and postoperative visual acuity at last follow-up in logMAR.
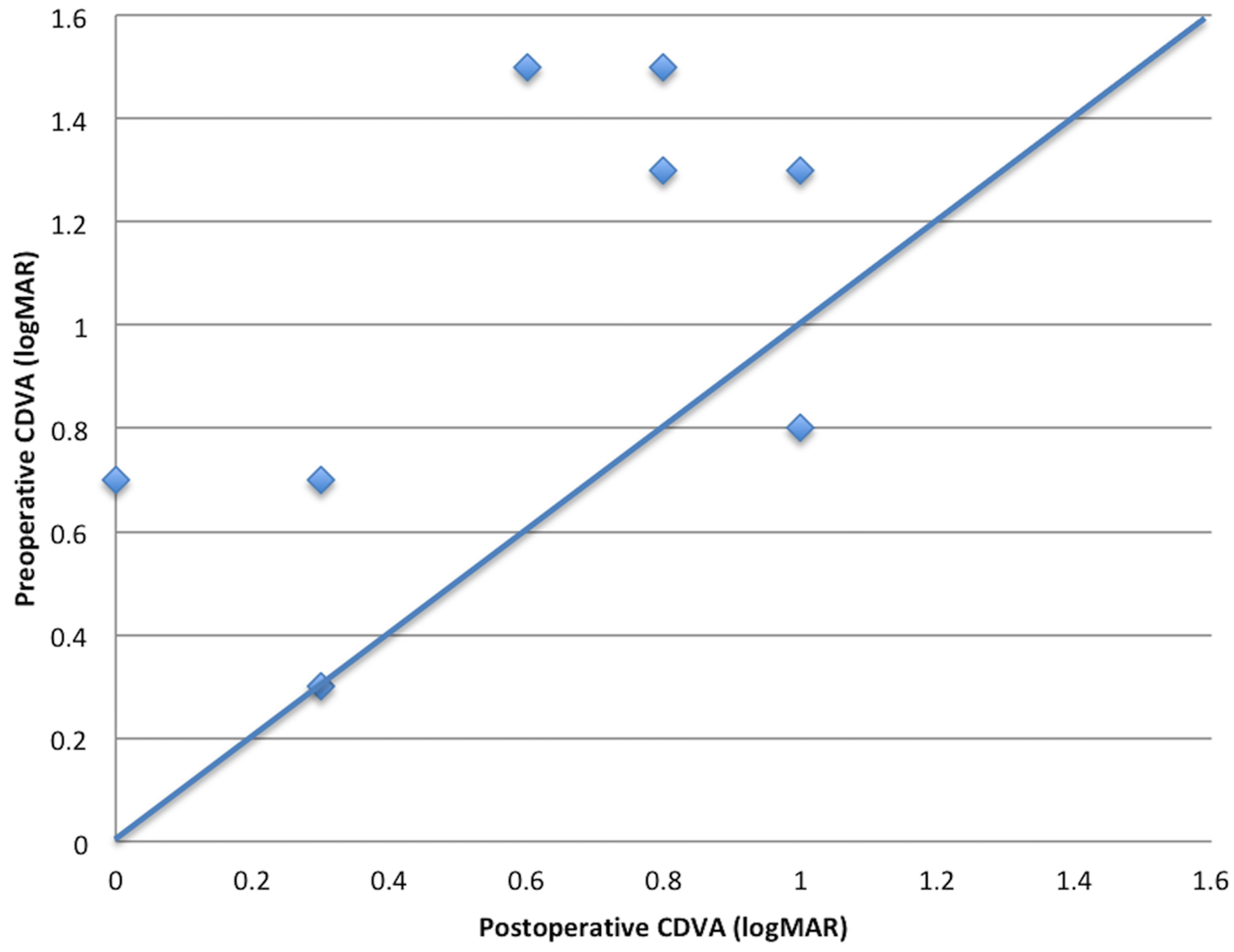
Scatter plot of the pre- and postoperative corrected-distance visual acuity (CDVA) in logMAR of all children in our cohort. Squares that are above the line represent children with improved visual acuity.
Peroperative retinal tear occurred in the eye that received 5 IVI. One eye developed a self-resolving intravitreal hemorrhage in the short postoperative period. Late recurrence occurred in one single eye with a Best dystrophy and was diagnosed at the 2-year visit. Recurrence was controlled by intravitreal bevacizumab injections. Macular atrophy developed in another eye starting also at the 2-year follow-up and manifesting itself by a progressive decrease in CDVA. None of the eyes developed cataract during the follow-up.
Literature review
The database search and manual screening of literature yielded 42 results. Of the 42 unique articles, 14 were retained based on assessments of their titles and abstracts. Of those, 4 were excluded because they were not related to submacular CNV excision and 1 article was excluded because no details were given on individual cases. 9 studies were finally selected for inclusion in this systematic review. Figure 4 reports on the flowchart used for the literature review. Table 2 presents characteristics of included studies. The literature review yielded a total of 42 eyes (41patients).
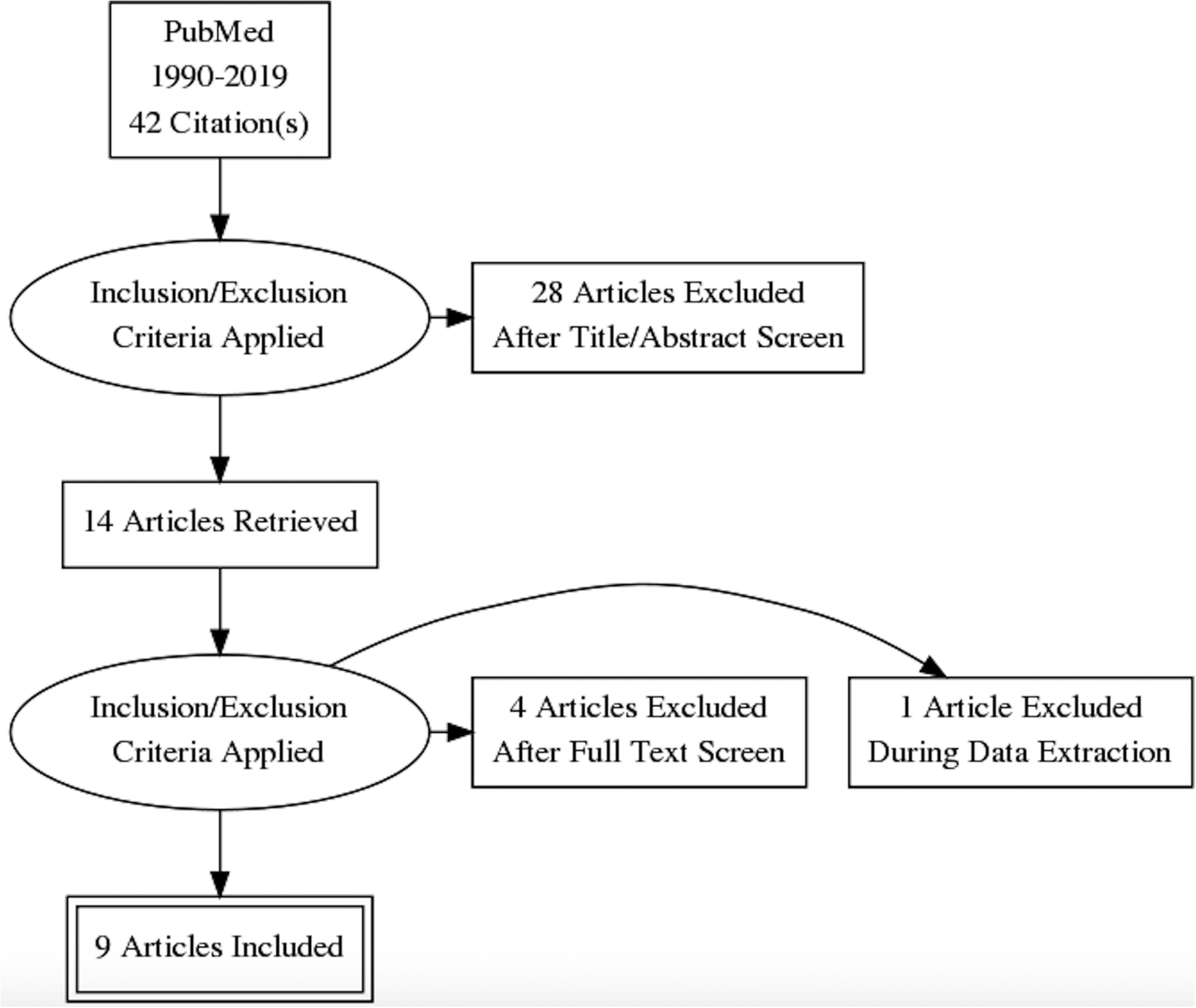
Pubmed search algorithm used for systematic literature review. Out of the 42 articles found on Pubmed, only 9 articles were included in the literature review.
Description of studies included in the literature review with design, number of cases, etiologies, follow-up period and complications.
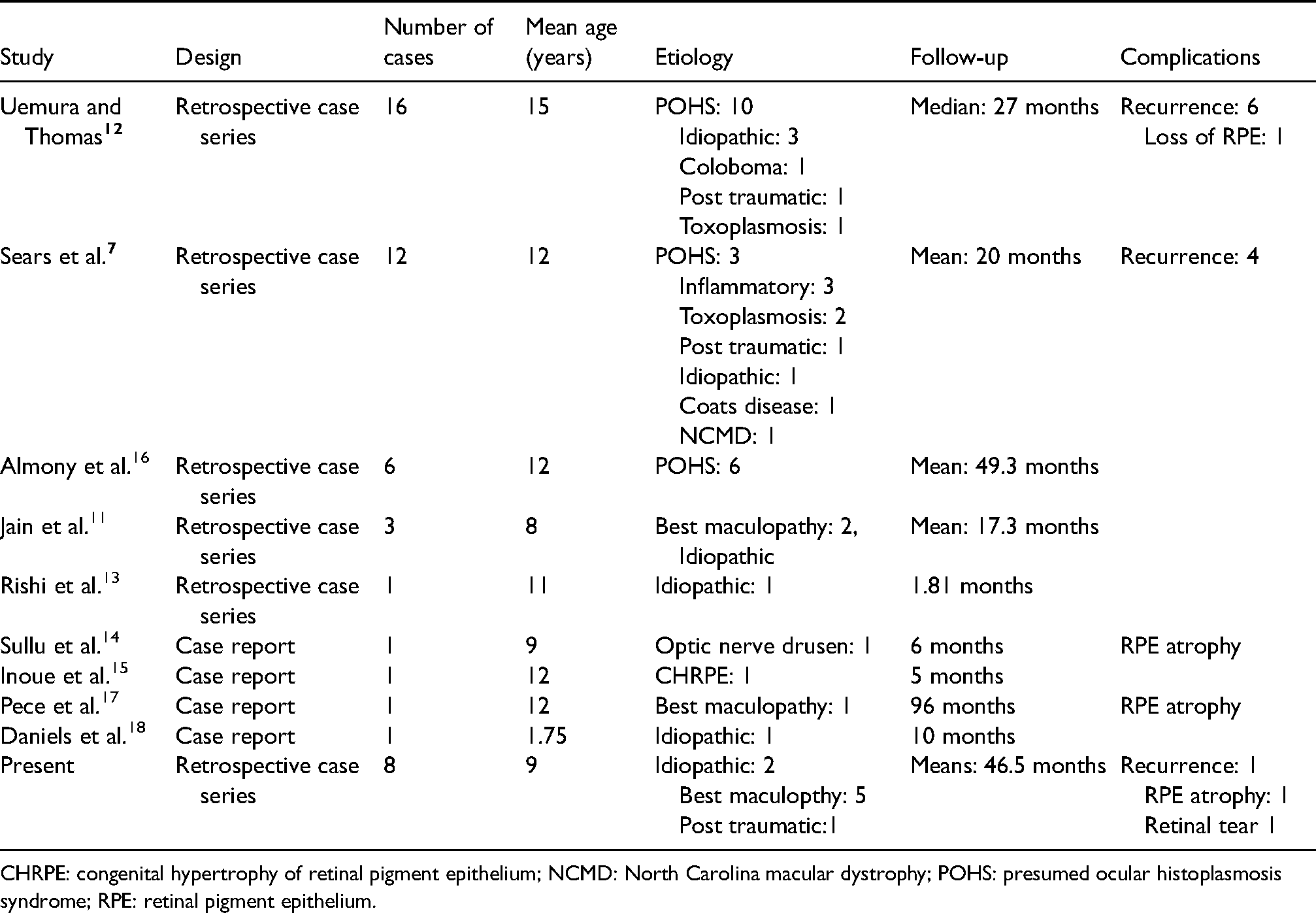
CHRPE: congenital hypertrophy of retinal pigment epithelium; NCMD: North Carolina macular dystrophy; POHS: presumed ocular histoplasmosis syndrome; RPE: retinal pigment epithelium.
The literature review in addition to the cases in our study yielded a total of 48 children (50 eyes) equally divided between genders that underwent surgical ablation of a subfoveal CNV. Two children had a bilateral CNV. Mean age was 12.2 ± 4.3 years (21months-18years). Table 3 represents all their etiologies.
Distribution of etiologies of all 50 cases (literature and present study) and the recurrence rate of each etiology.
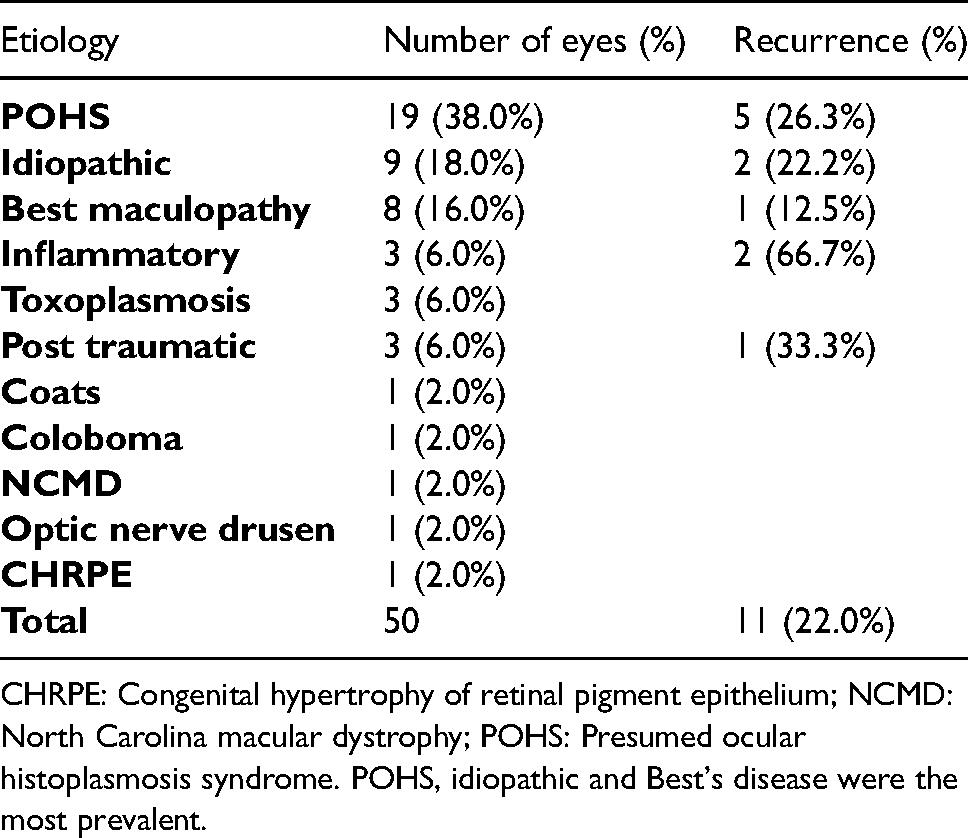
CHRPE: Congenital hypertrophy of retinal pigment epithelium; NCMD: North Carolina macular dystrophy; POHS: Presumed ocular histoplasmosis syndrome. POHS, idiopathic and Best's disease were the most prevalent.
Mean CDVA of all eyes improved from 1.00 ± 0.37 logMAR to 0.52 ± 0.42 (p < 0.01). Fifty percent of eyes (25 eyes) achieved a VA of 20/50 or better at the last follow-up with 68% (34 eyes) starting with a CDVA of 20/200 or worse. Only 5 children, in the present study, received IVI prior to surgery. None of the children, in the remaining studies included in the literature review, received IVI prior to surgery.
Discussion
The present study reports on the outcome of surgical excision of submacular CNV in children mostly after anti-VEGF treatment. Overall, surgical intervention seems to be beneficial, with the mean CDVA improving from 1.01logMAR to 0.60logMAR (p = 0.03) after a median follow-up time of 3.5 years (range: 1–13 years). 6 out of 8 eyes improved, one eye remained stable and one eye deteriorated.
A total of 8 eyes (7 children) with a mean age of 8.6 ± 5.2 years (range: 2–16) were included in our study. The present study reports on the cohort with the youngest mean age, while the youngest child receiving surgery with an age of 21 months was reported by Daniels et al. 18 Above all, none of the previous studies have reported on surgical CNV removal after anti-VEGF treatment.
Surgery was decided based on several variables: low visual acuity secondary to the CNV ( ≤ 20/200), thick fibrotic scar and recurrence of the edema after at least two IVI. A thick fibrotic neovascular membrane leads to tenting of the retina resulting in a poor anatomical and functional outcome. The rationale for surgery in eyes with a visual acuity better than 20/200 but recurrent macular edema was to reduce the risk associated with repeated general anesthesia and IVI. In literature, a mean number of two IVI were needed to control CNV, which was also our threshold before intervention.19,20 In our study 6 eyes of 5 children received at least one IVI of Bevacizumab prior to surgery. In the case that received 5 injections, a more adherent neovascular membrane was noted and as a result a retinal tear occurred perioperatively. Several studies reported on the fibrotic changes occurring in neovascular membranes after anti-VEGF treatment, which could explain the high adherence of membrane to the retina and the choroid.21,22 Therefore care must be taken during the membrane dissection process, especially if IVI of anti-VEGF have been administered in the history. In the case a surgery is planned, it is advised to limit preoperative IVI.
The present study as cases reported in the literature support the benefit of surgery on visual acuity. A limitation of VA improvement, due to amblyopia especially in children developing unilateral CNV before the age of 7, should also be considered.
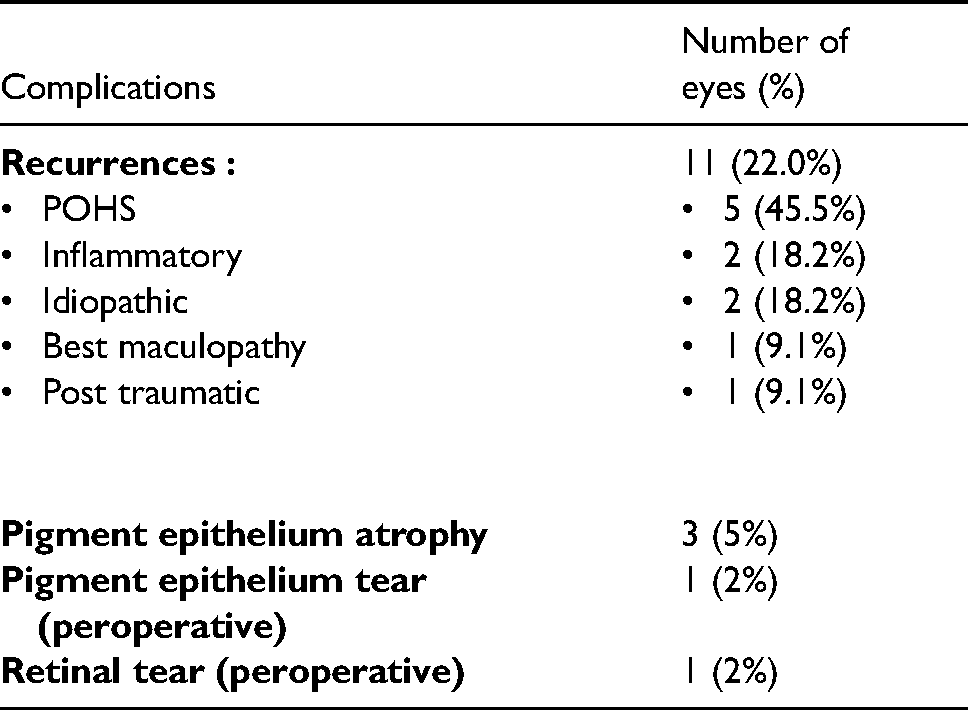
Several peri- and postoperative complications were reported (Table 4). Recurrence was the most frequent complication and occurred in 11 eyes (22.0%). Recurrence rate varied depending on the study and the CNV etiology. Uemura and Thomas who included mostly POHS children with CNV reported the highest recurrence rate of 37.5% (6 eyes). 12 Similarly, Sears et al. who also included mostly inflammatory etiologies reported a rate of 33.3% (4 eyes). 7 In our study, only one eye with Best maculopathy had a recurrence of the CNV. Delay to recurrence varied from a mean of 1.9 months in the study Uemura and Thomas 12 to 2 years in our study. Table 3 reports on the etiologies associated with recurrence. No cataract progression was reported in any of the included articles.
Complications of all 50 cases (literature and present study) and the etiologies of all eyes that developed recurrence. POHS: Presumed ocular histoplasmosis syndrome.
The limitation of our study is its retrospective aspect and the limited number of cases included. Furthermore, an improvement in children cooperation with age could explain in part the improvement of visual acuity measurement.
Conclusion
In conclusion, surgical removal of submacular CNV in children is a safe and effective treatment option. It results in a functional and anatomical improvement especially that most of the CNV in children are of type 2 and have a unique entry site. IVI of anti-VEGF are being proposed for the treatment of CNV, but doubts over their systemic safety have been rising as well as constraints related to the administration of the injection in children which is usually done under general anesthesia. Furthermore, despite controlling the CNV activity, the neovascular membrane remains under the retina affecting visual acuity and the anti-VEGF related fibrosis of the membrane can make its surgical removal more complicated, increasing the risk of a retinal or RPE tear. Finally, the therapeutic choice of CNV in children should be done on a case-by-case basis taking into account the age of the child, the etiology of the CNV, the response to anti-VEGF therapy, the location and size of the CNV and the surgeon's experience.
Supplemental Material
sj-m4v-1-ejo-10.1177_11206721221112537 - Supplemental material for Surgical removal of submacular choroidal neovessels in children: Outcome and literature review
Supplemental material, sj-m4v-1-ejo-10.1177_11206721221112537 for Surgical removal of submacular choroidal neovessels in children: Outcome and literature review by Youssef Abdelmassih, Sylvain EL Khoury, Pascal Dureau, Catherine Edelson, Florence Metge and Georges Caputo in European Journal of Ophthalmology
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.