
Abstract
Purpose
To report a case of recurrent acute retinal necrosis (ARN) in an eye filled with silicone oil previously complicated by rhegmatogenous retinal detachment (RRD).
Observations
A 68-year-old gentlemen with successfully treated herpes simplex virus type 1 (HSV1) ARN complicated by RRD requiring pars plana vitrectomy (PPV) with silicone oil tamponade, presented with a relapse of ARN with silicone oil in situ. Remission of recurrent retinitis was achieved using combined systemic oral and intravitreal antiviral therapy.
Conclusions and Importance
RRD is a significant complication of ARN which may require surgery with silicone oil tamponade. Recurrence of ARN retinitis can be effectively treated with intravitreal Ganciclovir and Foscarnet injections in a silicone oil filled eye with concurrent oral antiviral therapy. Aqueous humour sampling proved useful in the monitoring of disease activity.
Introduction
Advances in pharmacotherapies have resulted in the increasing use of intravitreal treatments for retinal disease including diabetic retinopathy, age-related macular degeneration, retinal vein occlusion, endophthalmitis, uveitis, intraocular malignancies, and viral retinitis.
Acute Retinal Necrosis (ARN) is a destructive necrotising retinitis with an incidence of 1 case per 1.6–2 million in the UK. 1 varicella zoster virus (VZV) is the most common cause and can affect all age groups. 2 VZV and HSV1 are more prevalent in the elderly, HSV2 in the younger population, and cytomegalovirus (CMV) in the immunocompromised. 3 Visual outcomes of ARN are poor and complicated by an increased risk of associated retinal detachment, macular oedema, macular ischaemia, chronic vitritis, and optic neuropathy. 4
Urgent treatment for ARN using antiviral agents should not be delayed for laboratory confirmation. Systemic therapy, intravenous and oral, targets viral replication and provides prophylaxis for the fellow eye, with intravitreal therapy targeting the affected unilateral eye. Oral Valaciclovir and Famciclovir are known to have high levels of bioavailability and efficacy. 5 Intravitreal treatment options include Foscarnet and Ganciclovir. Combination therapy with systemic oral and intravitreal injection is thought to have the optimal therapeutic potential. 6 Combined use of oral and intravitreal antivirals have been shown to be associated with a decreased risk of retinal detachment. 7
The risk of rhegmatogenous retinal detachment (RRD) in association with ARN ranges between 20–73%. 8 An optimal approach for management of RRD with ARN has not been developed due to the rarity of the condition and difficulty to perform trials. Options include scleral buckle, cryopexy, and pars plana vitrectomy (PPV) with silicone oil tamponade. Prophylactic vitrectomy has been proposed to lower the rate offig
retinal detachment in a retrospective case series. 9 The efficacy of prophylactic retinal laser demarcation remains unclear due to contrasting evidence from a small case series. 10
Silicone oil is an important tool in vitreoretinal surgery with properties that facilitate intraocular tamponade. However, the hydrophobic nature of silicone oil may impact the efficacy of intravitreal therapy due to drug delivery, absorption, dosage, and retinal toxicity. 11
We report our experience of intravitreal antiviral treatment in a silicone oil filled eye following RRD secondary to ARN and review the current literature on this topic.
Case report
A 68-year old immunocompetent male with a background of atrial fibrillation, hypertension, and stable minimal change disease, was referred by his optometrist for further assessment of a possible haemorrhagic posterior vitreous detachment. His ophthalmic history included previous left HSV keratitis and left pseudophakia.
On examination visual acuity was noted to be 20/20 in the right eye and counting fingers in the effected left eye. Anterior segment was unremarkable with clear corneas and quiet anterior chambers bilaterally. Fundal examination of the right eye was normal while the left showed marked vitritis with two faintly merged foci of yellow raised lesions with surrounding haemorrhage and vascular attenuation in the peripheral superotemporal retina, which was associated with two retinal holes. An Acute Retinal Necrosis (ARN) in the left eye was suspected.
Subsequently a diagnostic vitreous biopsy was performed. The patient was provisionally commenced on oral Valaciclovir 1 g twice daily and received one intravitreal injection of Ganciclovir (2 mg/0.1 ml) without delay. Polymerase chain reaction (PCR) analysis of the vitreous sample was positive for HSV1. Following diagnostic confirmation, the dose of oral Valaciclovir was increased to 2 g three times per day for 10 days and then reduced to 1 g three times per day. A second intravitreal injection of Ganciclovir (4 mg/0.1 ml) was administered one week later as per evidence based recommendations. 12 Systemic work up was unremarkable except for mildly reduced, but stable, estimated glomerular filtration rate (eGFR) secondary to longstanding minimal change disease.
At 2 weeks review a localised rhegmatogenous retinal detachment (RRD) in the superotemporal quadrant developed at the site of acute retinal necrosis. This was promptly treated with circumferential scleral buckle, and cryotherapy retinopexy. Two months later the retinitis resolved, visual acuity was 20/80, and Valaciclovir reduced to 500mg three times per day for a period of 3 months.
Two months later the patient developed a second inferotemporal RRD, from a retinal break at 4 o’clock, in the previously effected left eye. (Figure 1) This was managed emergently with pars plana vitrectomy (PPV), retinal cryopexy, endolaser retinopexy, and silicone oil tamponade. Retinitis was quiescent during this time.
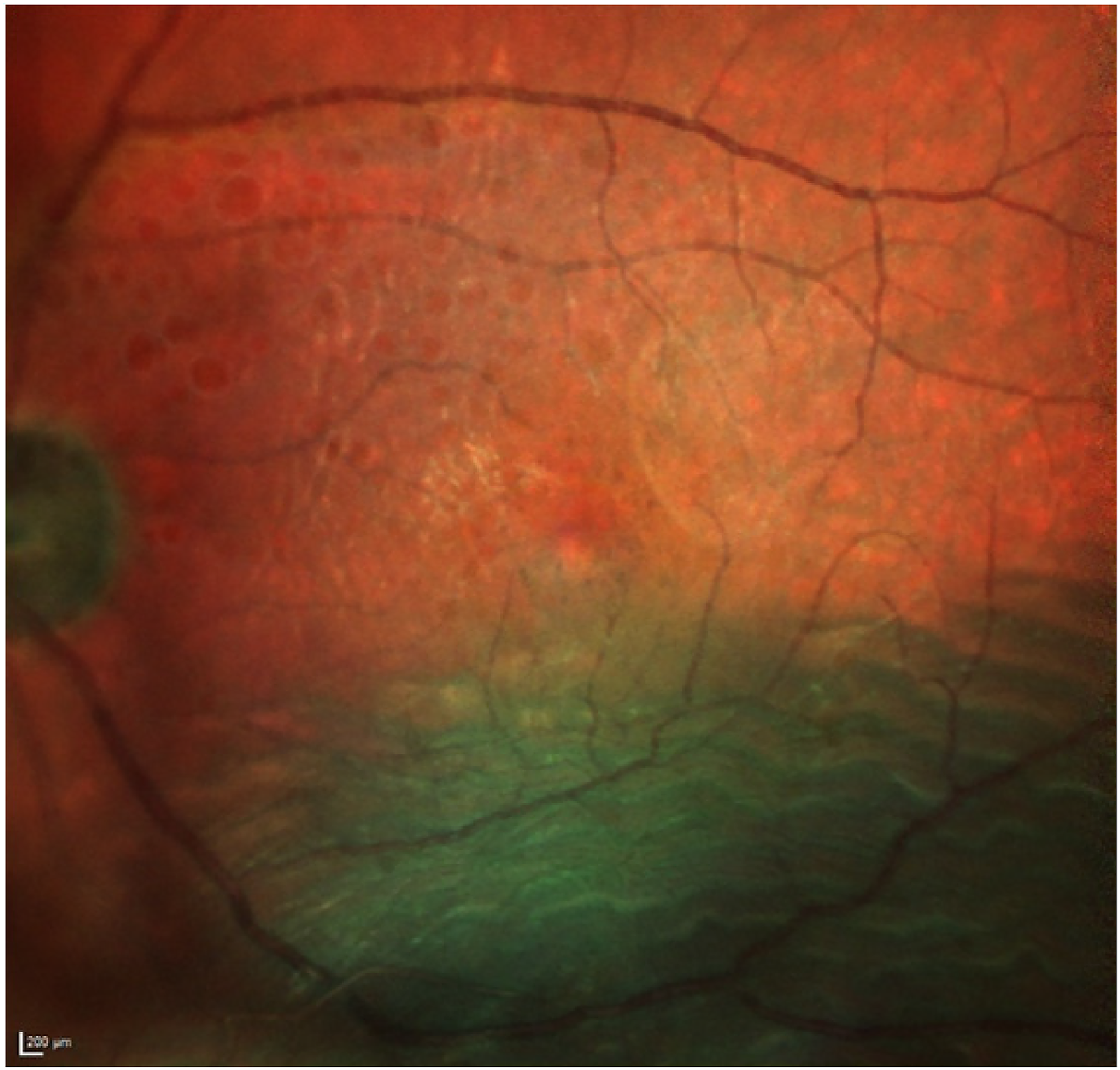
A colour fundus photograph of the left eye demonstrating an inferotemporal retinal detachment abutting the fovea.
Despite the initial resolution, a relapse of ARN occurred 6 months later. (Figure 2) Full thickness retinal necrosis was identified in the inferonasal retina. Anterior chamber tap and PCR confirmed the presence of HSV1. The patient was subsequently commenced on oral Valaciclovir 2 g three times per day for 10 days, and then reduced to 1 g three times per day for 3 months.
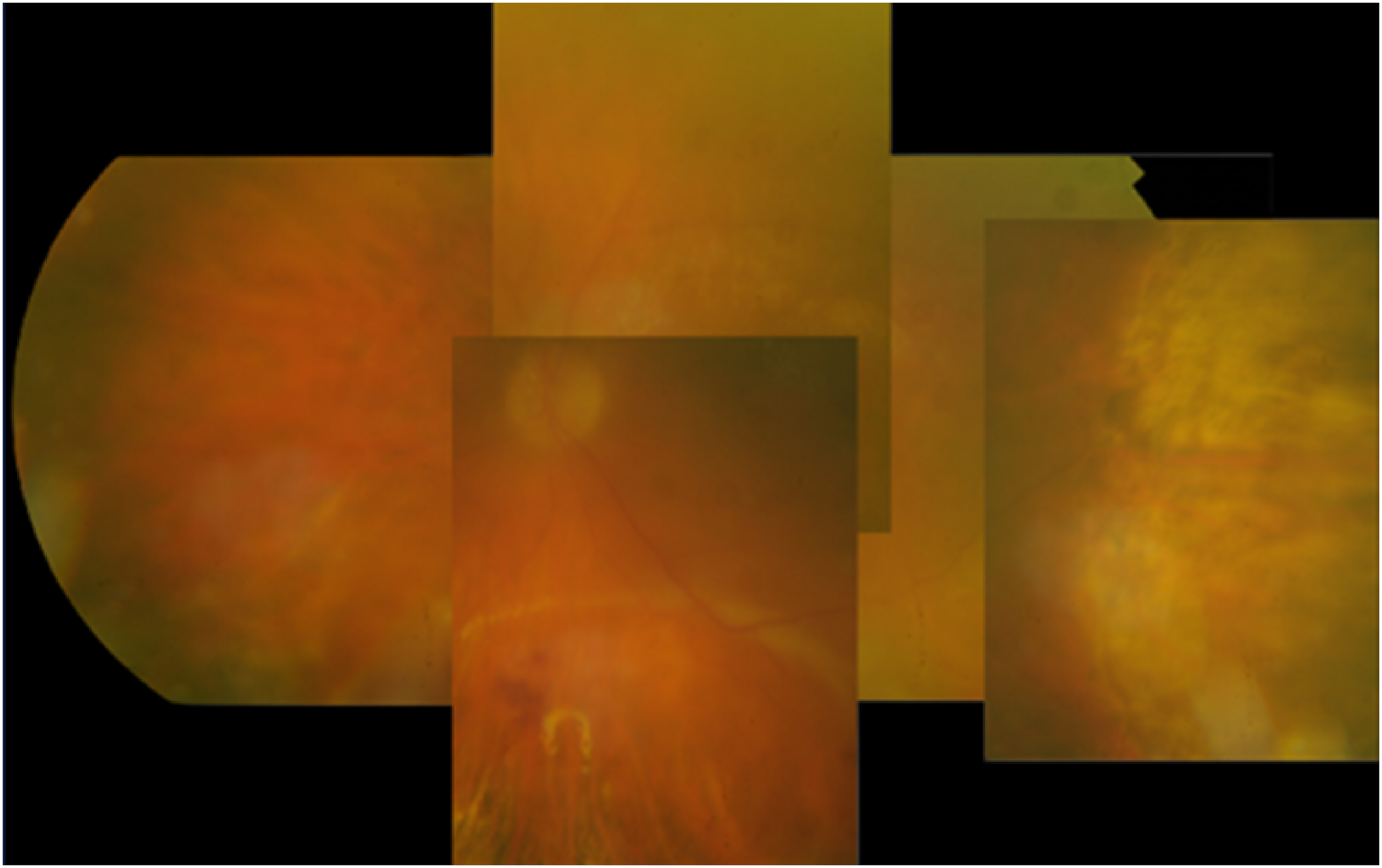
A mosaic of superimposed colour fundus photographs of the left eye taken from the primary position of gaze demonstrating an active relapse of acute retinal necrosis, with marked vitritis, active inferonasal necrosis, and a larger old temporal lesion.
The patient received two doses of intravitreal Ganciclovir (4 mg/0.1 ml) with silicone oil in situ 3 days apart. Clinical improvement with a reduction in the area of necrosis was noted thereafter but aqueous humour samples were persistently positive. A further intravitreal injection of Ganciclovir (4 mg/0.1 ml) was administered 6 weeks after the last. Due to the establishment of resistance, determined clinically, the patient was commenced on Foscarnet (2.4 mg/0.1 ml) and received a total of 4 injections at weekly intervals.
The retinitis remained clinically quiescent after stopping the intravitreal injections and aqueous humour PCR remained negative for at least 3 years. (Figure 3) Tapering of oral valaciclovir proved challenging during this period due to recurrent flares of herpetic keratouveitis requiring maintenance therapy. Valaciclovir was eventually stopped 32 months after the last intravitreal injection. Chronic cystoid macula oedema and an epiretinal membrane was found on macular SD-OCT with a timeline of OCT findings described below. (Figure 4) Botulinum A induced upper lid ptosis was helpful for a persistent corneal epithelial defect. Most recent visual acuity was 20/200 with oil in situ, and the patient remains systemically well otherwise.
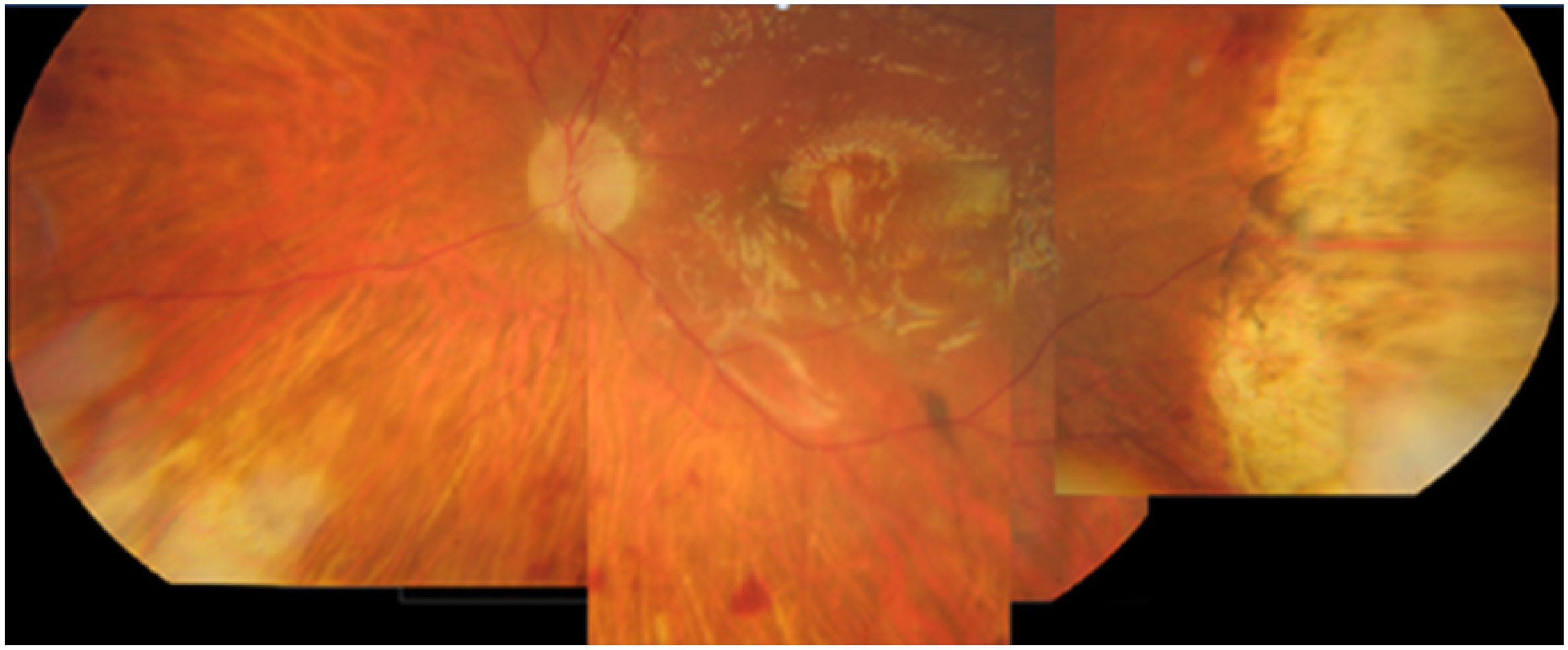
A mosaic of superimposed colour fundal photographs demonstrating a quiescent posterior segment with silicone oil in situ. Chronic changes of acute retinal necrosis are noted inferonasally and temporally.

Multicolour image (b) red free image (c) macular SD-OCT scan. Imaging on presentation of ARN relapse under oil demonstrating Kyrieleis plaques along the temporal venous and arterial arcades, preretinal deposits on the fovea, and vitritis. (d) MultiColour image (e) Red free image (f) Macular SD-OCT scan. Following completion of intravitreal antiviral treatment, resolution of vitreous hyperreflectivity, Kyrieleis plaques, and foveal preretinal deposits is demonstrated. (g): Chronic macular oedema and epiretinal membrane noted under oil, 2 years after intravitreal antiviral treatment.
Disease remission was established following the use of a combination of Ganciclovir and Foscarnet intravitreal therapy in a silicone filled eye with concurrent systemic therapy.
Review of literature and discussion
Our search revealed one publication describing the use of intravitreal antiviral agents in silicone oil filled eyes. Meshi et al reported two cases of viral retinitis with silicone oil tamponade. 13 The findings of Meshi et al highlighted the efficacy of adjunctive low dose Foscarnet and Ganciclovir intravitreal antiviral injections for PORN and ARN in silicone oil filled eyes previously complicated by retinal detachment.
Rhegmatogenous retinal detachment (RRD) secondary to ARN is an established complication, with extensive retinal involvement linked to increased risk. There is a predisposition for retinal tears to form at the boundary between vital and necrotic ischaemic retina. 9 The use of silicone oil in RRD repair coupled with the potential of ARN to relapse suggest scenarios in which the use of intravitreal antiviral under silicone oil is warranted.
The first case described a 38-year-old HIV positive male patient diagnosed with bilateral progressive outer retinal necrosis (PORN) due to VZV. Initially, a combination of systemic (intravenous induction and oral maintenance) and intravitreal antiviral therapy was commenced. Bilateral intravitreal injections of Foscarnet (2.4 mg/0.1 ml) and Ganciclovir(2 mg/0.05ml) were performed twice weekly for induction. A total exudative retinal detachment developed in the left eye with treatment being subsequently halted. In the right eye a superior retinal detachment developed which was treated with pars plana vitrectomy (PPV) and silicone oil tamponade. Following this, intravitreal therapy with low dose Foscarnet and Ganciclovir was continued on a weekly regimen in the silicone oil filled eye, with a total of 5 injections of each drug. With combined systemic and intravitreal therapy retinitis improved and lesions regressed, with a best corrected visual acuity (BCVA) of 20/60 on discharge. In the 9 months following no retinitis or detachment recurrence were described.
The second case was a 66-year-old diabetic patient with ARN secondary to VZV. A diagnostic vitrectomy was required at which point an inferior retinal detachment was identified. Following retinal reattachment, laser retinopexy, and silicone oil tamponade, low dose intravitreal Foscarnet (1.2 mg/0.05ml) was administered at the end of the surgery. Weekly injections of Foscarnet were continued for 8 weeks with systemic treatment. Regression of lesions occurred, and no recurrence of retinitis or detachment were noted at review 9 months after surgery.
Our case demonstrates disease control and regression using combination intravitreal and systemic antivirals in a silicone oil filled ARN effected eye. To our knowledge we report the second case of intravitreal antivirals in a silicone oil filled human eye for the treatment of ARN. Like Meshi et al, we used concurrent oral antiviral agents. Oral antiviral agents provide an equivalent dosage to intravenous antiviral agents. 14 However, our management differs with the first line use of high dose intravitreal Ganciclovir as opposed to low dose Foscarnet 1.2 mg/0.05mL. High dose Ganciclovir has been shown to reduce viral DNA titres. 15 Unlike Meshi et al we did not use corticosteroids. There is limited evidence for the use of adjunctive corticosteroid, and a conclusive improvement of outcomes has not been determined. 6
ARN is a chronic disease that can relapse. Delayed relapse of up to 19 years has been reported and therefore long term follow up is warranted. 16 In our own case, recurrence occurred in the presence of silicone oil 6 months following vitrectomy. There are no standardised guidelines for monitoring patients despite the potential for recurrence. A strategy focused on achieving a balance between managing clinical capacity and timely clinical evaluation could be effective but challenging, akin to other retinal disease services. Such strategies may prove difficult to formulate due to practises being adopted from the findings of observational studies and the impossibility of a clinical trial. Monitoring disease activity in the presence of silicone oil tamponade may be challenging. We found that measuring the viral load in aqueous samples analysed with PCR is a useful tool for monitoring disease activity and determining treatment endpoints.
The presence of silicone oil may affect the pharmacokinetic and pharmacodynamic properties of antiviral agents within the eye. Solubility of antiviral drug is altered in the presence of hydrophobic silicone oil. The volume of distribution becomes limited to the preretinal space exposing the retina to high, potentially toxic concentrations. Efficacy of anti-VEGF antibody preparations and corticosteroids have been described without retinal toxicity.17–19
Animal studies have shown safety with findings supporting clinical practice of using unadjusted dosage of intravitreal antiviral injection and implant. Ganciclovir dosages of up to 200 mcg/0.1 mL were safe for serial intravitreal injection in rabbit eyes filled with silicone oil.20, 21 Retinal toxicity was only demonstrated with excessive unadjusted injection dosage in rabbit eyes. 22
Silicone oil has been hypothesised to have antimicrobial and antiviral properties. Silicone oil is composed of organic and inorganic polymers with repeat Siloxane subunits. Silicone oil has been demonstrated to have antiviral activity against HSV-1 due to nutrition exhaustion and toxic effects to the virus. 23 In vitro bactericidal activity has also been demonstrated and theorised to supplement the antimicrobial properties of intravitreal antibiotics, while in vitro fungistatic activity is limited to 30 days. 24
Future analysis may permit titration of optimal dosing and identifying retinal toxicity of intravitreal antivirals in silicone oil filled eyes with the use of electroretinography. Distinct conclusions may be difficult to produce from a small dataset due to the rarity of this condition. A larger case series in the future would be beneficial in confirming our own observations.
Conclusion
The use of intravitreal antivirals in combination with systemic therapy has proven successful in the treatment of ARN relapse in an eye filled with silicone oil previously complicated by retinal detachment. We have demonstrated disease control and good tolerance with unadjusted doses of intravitreal Ganciclovir and Foscarnet.
We recommend repeated aqueous sampling as a useful tool in monitoring disease activity in the presence of long-term silicone oil tamponade. Standardised guidelines of tapering down antiviral are yet to be developed to optimise the long-term medical management of this condition.
Footnotes
Authorship
All authors attest that they meet the current ICMJE criteria for Authorship.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.