
Abstract
Background/aims
To compare the ocular biomechanical properties of inactive Grave’s orbitopathy (GO) patients and healthy subjects and to evaluate the influence of severity and phenotype of GO on these parameters.
Methods
This was a cross-sectional study. All included inactive GO patients and healthy controls underwent complete ocular examination, including Goldman applanation tonometry (GAT), corneal biomechanical analysis using Ocular Response Analyser (ORA), and corneal epithelial thickness analysis using Optovue. Patients with inactive GO were classified based on the severity and orbital phenotype (predominantly myogenic or lipogenic). Comparison among groups was performed.
Results
60 eyes from 30 inactive GO patients and 30 healthy eyes were examined. Corneal hysteresis (CH) was significantly lower in inactive GO patients (9.6 [p25 8.1; p75 11.2]) compared to controls (10.4 [9.8; 11.5]) (p = 0.012). In GO patients, cornea compensated intraocular pressure (IOPcc) was significantly higher than Goldman applanation tonometry IOP (IOP-GAT) (p = 0.001). A total of 13.3% GO patients were initially classified as having ocular hypertension (OHT; defined as IOP > 21 mmHg with no signs of glaucomatous optic neuropathy) based on IOP-GAT measurement. According to IOPcc, 27.8% of GO patients were classified as OHT. In GO patients, no differences were found in corneal bimechanical properties according to the disease severity or orbital phenotype.
Conclusions
CH is significantly lower in inactive GO patients compared to healthy subjects. ORA corrected IOP was significantly higher in GO patients compared to IOP-GAT. No differences in corneal biomechanical properties between mild and moderate-to-severe GO disease and between myogenic and lipogenic orbitopathy were found.
Introduction
Graves’s orbitopathy (GO) is an autoimmune condition that causes well recognised ocular and periocular changes such as proptosis, eyelid retraction, diplopia, ocular surface problems or periorbital oedema. Although it is less commonly discussed, high intraocular pressure (IOP) has been reported to occur in about 5–24% of patients diagnosed with GO,1,2 which is significantly higher than the prevalence in general population (1.6%). 3 However, glaucoma prevalence in GO patients has been found to be similar to general population.4,5
Different theories have been hypothesised to explain this presumed lower rate of conversion to glaucoma among patients with GO and ocular hypertension (OHT), including different biomechanical properties or elevation of IOP for shorter periods during the day (e.g, on attempted upgaze).6–8 Restrictive myopathy causes an increase in IOP due to compression of the globe by thickened and/or fibrotic extraocular muscles and GO patients tend to adopt a chin-up position so that a slight downgaze relieves the elevated IOP associated with the straight-ahead position. Danesh-Meyer et al. 1 findings supported this theory and recommended to re-evaluate OHT/glaucoma status of GO subjects after strabismus and decompression surgery as their IOP measurement could significantly decrease.
Ocular Response Analyser (ORA; Reichert Ophthalmic Instruments, Depew, NY, USA) is currently the only commercially available tool that allows in vivo measurements of corneal biomechanical properties such as corneal hysteresis (CH) and corneal resistance factor (CRF). ORA also determines the noncontact intraocular pressure as Goldman-correlated IOP (IOPg) and corneal-compensated IOP (IOPcc). 9 By integrating corneal biomechanical factors with the measurement of IOP, ORA provides a more accurate estimation of IOP compared to conventional Goldman applanation tonometry (GAT). 10
Previous studies have shown that CH can vary among different age groups and ethnicity in both normal and glaucomatous eyes, independent of the central corneal thickness (CCT)11–13 While not being widely studied, CH is shown to be affected by a number of ocular and orbital diseases, including glaucoma, keratoconus, post-scleral buckling surgery, and GO, amongst others.14–19 The variation in CH can potentially lead to under- or over-estimation of IOP measured on GAT (the current gold standard for IOP measurement), resulting in delayed or unnecessary IOP-lowering treatment, respectively.
To date, there were only three studies in the literature that have examined the influence of GO on the corneal biomechanical properties.17–19 One study was conducted among the Chinese population, 17 another among Turkish population 19 and one was among the Iranian population. 18 In view of the lack of literature, this study aimed to investigate the effect of GO and the impact of GO severity and phenotype on corneal biomechanical properties, measured with ORA, among the European population.
Material and methods
In this analytical cross-sectional study, we recruited 30 Caucasian patients diagnosed with inactive GO from the multidisciplinary GO clinic at a Tertiary Referral Hospital from January 2018 to January 2019. All patients had a previous diagnosis of GO defined by the presence of one or more of the following features: proptosis, extraocular muscle dysfunction, soft tissue changes in the eye, and optic nerve involvement. All patients included in the study had an inactive disease defined as a clinical activity score (CAS) < 3 and controlled thyroid function for the last 6 months. 19
In terms of disease severity, patients were classified according to the EUGOGO Consensus Statement 20 into mild, moderate-to-severe or sight threatening disease. Exclusion criteria included: younger than 18 years of age, sight threatening disease, receiving therapy for glaucoma or systemic steroid use in the last 6 months. According to Nunery’s classification, 21 all orbits were further subdivided into two groups: one with predominantly lipogenic disease (orbits with muscle restriction from 0 to 2) and one with predominantly myogenic disease (orbits with muscle restriction graded from 2 to 8) (Figure 1). Ethical approval was obtained from the institutional ethics committee. Both eyes were included in the study if they met the inclusion criteria. For comparison purpose, a control group of 15 age- and sex-matched healthy subjects (with 30 eyes) were recruited after routine examination.

CT scan showing predominantly lipogenic orbitopathy (image A) and predominantly myogenic orbitopathy (image B). The arrows point to significantly enlarged medial rectus muscles.
One of the authors (ICG) performed optic and orthoptic examination in all the patients. The best-corrected-visual-acuity (BCVA), monocular and binocular extraocular muscles excursions, and corneal biomechanical properties (using ORA) were measured before any contact procedure to avoid any confounding effect on the corneal properties. A minimum of 3 ORA readings were recorded and the mean of the 3 or more measurements was used for analysis. All 4 ORA parameters, including IOPg, IOPcc, CH and CRF, were recorded.
All patients underwent a complete ophthalmic examination including colour vision assessment, slit-lamp biomicroscopy, Goldman applanation tonometry (IOP-GAT) (Haag-Streit, Koeniz, Switzeland) in primary straight-ahead position and upgaze, proptosis measurement (Hertel exophthalmometry) and fundoscopy. Corneal epithelial thickness was measured using anterior segment optical coherence tomography (Optovue®, manufacturer and location). Central corneal thickness was measured using a pachymeter after instillation of one drop of topical anesthetic. We measured IOP both in primary straight-ahead position and up-gaze position in all subjects.
To reduce the risk of bias, the ophthalmologist assessing the participants was masked from the ORA measurement results when performing the ophthalmological examination. All examinations were performed between 0800 and 1300 the same day when the patients were recruited.
Statistical analysis
We used SPSS software 21.0 Version (SPSS Inc., Chicago IL) for statistical analysis. The level of significance was set at P < 0.05. Non-parametric tests were used in view of non-normally distributed data (based on the skewness, kurtosis z-values, and Shapiro-Wilk test). Continuous variables were presented in median ± interquartile range (IQR). For comparison between GO patients and healthy controls, we used Mann-Whitney U and Kruskall-Wallis tests for continuous variables and Chi-square for categorical variables. We used Wilcoxon signed-ranked test to compare ORA measurements and IOP-GAT measurements in each group.
Results
Baseline characteristics
A total of 60 eyes of 30 patients from the GO group and 30 eyes of 15 healthy controls were included in the study. Both groups were age- and sex-matched and were comparable in terms of CCT and corneal epithelial thickness (Table 1). Median duration of orbital disease among GO patients was 57 moths (45; 75) and antithyroid drug treatment (ATD) was the most common treatment for thyroid function control (65.5% of patients).
Characteristic of patients and controls.
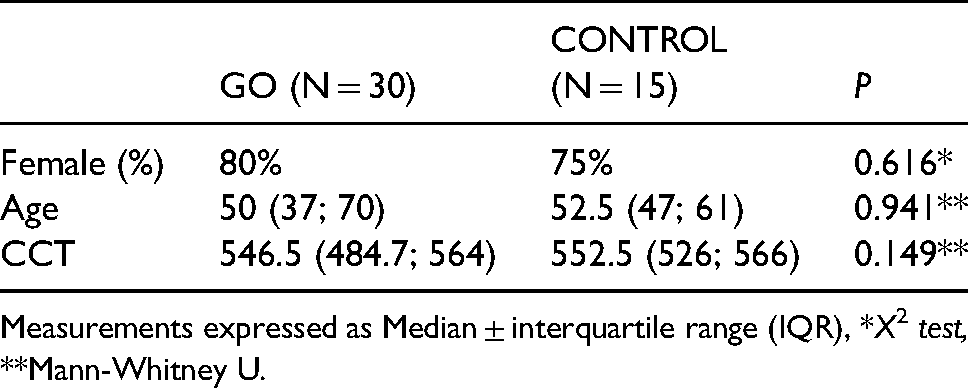
Measurements expressed as Median ± interquartile range (IQR), *X2 test, **Mann-Whitney U.
IOP measurements
IOP-GAT values measured in primary straight-ahead and upgaze position were significantly higher in GO patients (16.5 [14.2; 18.0] mmHg and 20.5 [17.0; 24.0] mmHg) than in healthy controls (14.0 [13.0; 15.0] mmHg and 15.0 [14.0; 16.0] mmHg) (Mann-Whitney U test; p < 0.001 and p < 0.001 respectively). Similarly, IOPg measured by ORA was significantly higher in GO patients as compared to healthy subjects (Table 2).
Measurement and comparison of intraocular pressure (IOP) between GO patients and healthy controls using ocular response analyser.
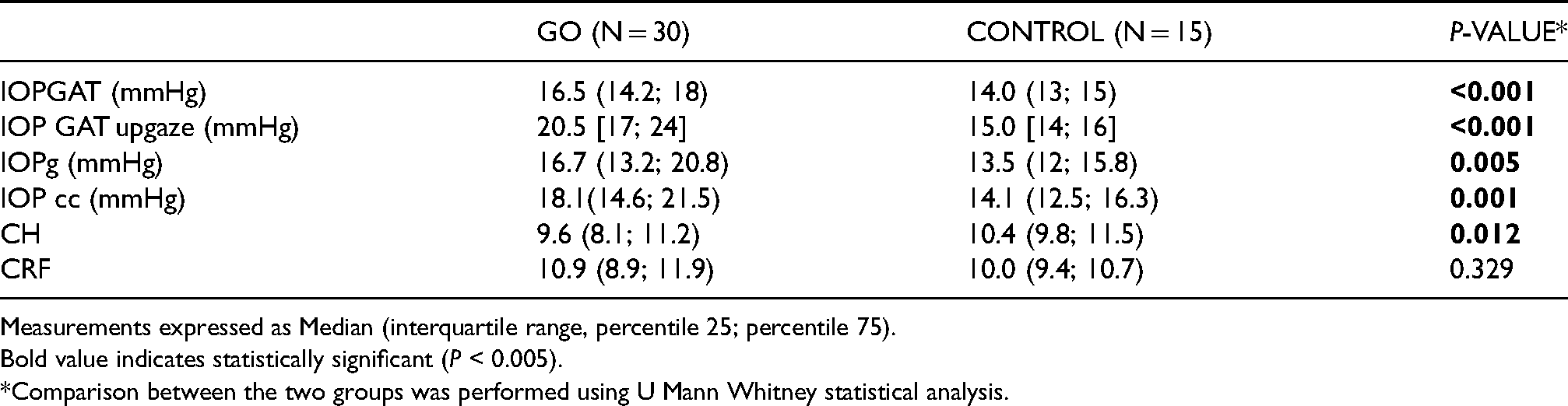
Measurements expressed as Median (interquartile range, percentile 25; percentile 75). Bold value indicates statistically significant (P < 0.005).
*Comparison between the two groups was performed using U Mann Whitney statistical analysis.
Corneal biomechanical measurements
Regarding ORA parameters, CH measured in GO patients (9.6 [8.1; 11.2]) was significantly lower than the controls (10.4 [9.8; 11.5]) (Mann Whitney U test; p = 0.012) (Table 2). Therefore, when correction was applied by ORA in GO patients, IOPcc (18.1 [14.6; 21.5] mmHg) was significantly higher compared to both IOP-GAT (16.5 [14.2; 18] mmHg (Wilcoxon test; p = 0.001) and IOPg (16.7 [13.2; 20.8] mmHg) (Wilcoxon test; p = 0.007). A total of 13.3% GO patients were initially classified as having OHT (defined as IOP > 21 mmHg with no signs of glaucomatous optic neuropathy) based on IOP-GAT measurement. According to IOPcc, 27.8% of GO patients were classified as OHT. There was no significant difference in the CRF between GO patients and healthy controls (Table 2).
Potential factors that influenced the corneal biomechanical measurement
According to the EUGOGO severity classification, 24 of 60 eyes (40%) were classified as having mild disease and 36 of 60 eyes (60%) were classified as moderate-to-severe GO. There were no differences between both severity groups in terms of CH, CRF, IOPg and IOPcc measured by ORA (Table 3). When analysing CH among controls, mild GO and moderate-to-severe GO, we found CH measured in mild GO was significantly lower compared to controls (p = 0.005 U Mann Whitney) but no difference was found between moderate-to-severe GO and controls (p = 0.195 U Mann Whitney). No correlation was found between CH and exophthalmos (Spearman 0.19 p = 0.156).
Comparation of clinical and biomechanical parameters between mild and moderate-to-severe go.
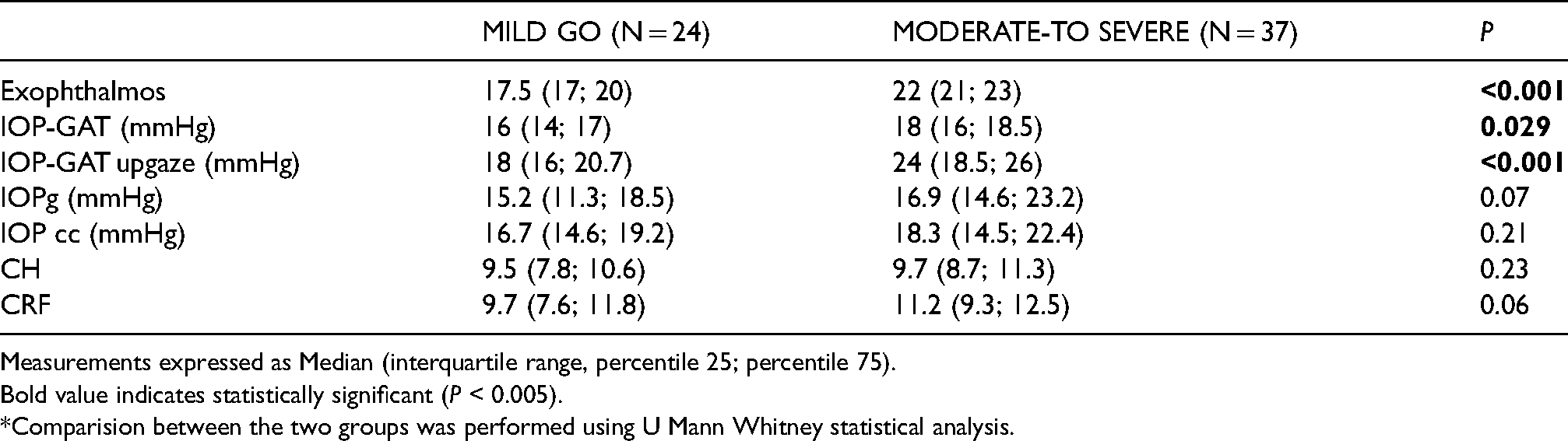
Measurements expressed as Median (interquartile range, percentile 25; percentile 75). Bold value indicates statistically significant (P < 0.005).
*Comparision between the two groups was performed using U Mann Whitney statistical analysis.
IOP-GAT in both straight-ahead position and upgaze were significantly higher in moderate-to-severe GO compared to mild GO (p = 0.015 and p < 0.001 Mann-Whitney U) (Table 3). In upgaze position IOP increased by a median of 4 mmHg [2; 8] in moderate-to-severe GO, and by 2 mmHg [1; 3] in mild GO (Mann-Whitney U test; p = 0.001).
When comparing the biomechanical parameters of GO patients based on the type of orbital disease [i.e., predominantly lipogenic (type I) or myogenic (type II)], no significant differences were found with regard to CH (Mann Whitney U; p = 0.87) and CRF (Mann Whitney U; p = 0.29) between both groups.
In myogenic orbits (n = 24), IOP-GAT measured in primary straight-ahead position (p = 0.015), upgaze (p < 0.001) and IOPg (p = 0.026) were significantly higher than those measured in lipogenic orbits (U Mann Whitney). IOPcc was significantly higher than IOP GAT measured in straight-ahead position in both lipogenic (p = 0.018 Wilcoxon) and myogenic GO (p = 0.036 Wilcoxon).
Finally, analysing the treatment used to control thyroid function in GO patients (65% medical treatment, 17,2% thyroidectomy and 17,2% radioiodine), no significant differences were found in CH between patients receiving medical or definitive (radioiodine or surgery) treatment (p = 0.337 U Mann-Whitney).
Discussion
Measurement of IOP is crucial in guiding the management of various ophthalmic conditions, particularly OHT and glaucoma. Corneal biomechanics can influence the accuracy of GAT and other tonometers. In this study, we found that CH in Caucasian GO patients with inactive disease and controlled thyroid function was significantly lower as compared with normal subjects. Therefore, the number of GO patients initially classified as OHT (based on IOP-GAT measurement) doubled when the corneal biomechanical properties were considered (based on the IOPcc reading).
The Ocular Response Analyzer (ORA; Reichert Ophthalmic instruments), is a non-contact device that measures the corneal response to indentation by a rapid air pulse. The air pulse causes the cornea to move inward, past applanation and into a slight concavity before returning to normal curvature. Corneal deformation is recorded by an electrooptical infrared system. Using the first and second applanation points, ORA provides 2 biomechanical parameters, namely CH which reflects the ability of corneal tissue to absorb and dissipate energy (a viscoelastic property) and CRF which offers a measurement of corneal resistance.
CH is not a static physical property like corneal thickness as it has been shown to be lower in various types of glaucomatous eyes and other degenerative disorders.22–24 In keratoconus, both CRF and CH are reduced, and their values decrease as the severity of keratoconus increases.25,26 Eyes with postoperatively corneal oedema, 27 Fuchs’ dystrophy 28 high myopia 29 or Marfan Syndrome, 30 have also been reported to show lower CH values. The lower CH has also been associated with progressive worsening of the visual field in glaucoma patients. 23 According to Koetcha, 23 corneal biomechanics reflects the viscoelastic properties of the cornea and mechanical strength of stromal collagen fibrils interacting with the extracellular proteoglycan matrix.
In GO, during the active inflammatory stage of the disease, T-cell mediated response leads to increased glycosaminoglycans (GAGs) synthesis and recruitment of new fat cells from orbital adipose precursor, causing enlargement of intraorbital tissues. In vivo structure of the cornea in GO have been studied by using confocal technology. Villani et al. 31 found increased stromal cell density in GO patients (both active and inactive), a reduction in epithelial cell density and an increased number of activated keratocytes compared to controls. They related those structural changes to 2 inflammatory mechanisms: evaporative dry eye typically occurring in GO and systemic disease itself. However, we could not find in the literature reports describing corneal histology in GO patients.
Considering the physiopathology of GO, one would hypothesise that GAGs are also overexpressed in the cornea stroma, which is similar to the changes occurred in other orbital tissues (e.g., extraocular muscles). 32 If that was the case, we would expect an increased CH and CRF valued as it has been reported for children with mucopolysaccharidosis, 33 a condition that leads to an accumulation of GAGs in all tissues of the body, including the cornea. According to our findings, however, CH is lower in GO patients with inactive disease compared to controls, and some ultrastructural changes that should be elucidated may occur in the cornea.
There are in the literature two other studies that have found lower values of CH in GO patients compared to controls. However, Moghimi et al. 18 included patients without specifying their thyroid status or their eye disease stage (active or inactive). In Karabulut et al. study, 19 although VISA system was used to score the activity, thyroid status was not recorded. In those previous reports, inflammation and structural changes in corneal tissues due to dry eye were considered as the possible cause of CH changes in GO patients.
In our study, however, all selected patients had been clinically inactive and euthyroid for at least 6 months. No inflammation was present in their clinical exam and corneal epithelium map (Optovue), which was used to identify ocular surface disease, was comparable between both controls and GO patients. Therefore, other corneal ultrastructural changes, not directly related to dry eye disease or systemic inflammation, might account for the decrease in damping ability of the cornea found in GO. Pathogenesis of GO includes different degrees of extraocular muscle enlargement, fibrosis and increased orbital pressure that contributes to the higher IOP values found in GO patients compared to controls in primary position and the exaggerated increase in the upper gaze. 34 Based on the orbital phenotype, no differences in CH or other biomechanical properties were found between predominantly lipogenic or myogenic orbits. Similarly, no difference in CH was found between mild and moderate-to-severe GO, which is consistent with Karabulut et al. finding. 19 This could be explained by the fact that GO severity classification is based on clinical assessment of parameters like eyelid retraction, exophthalmometry or diplopia, 19 that, according to our findings, do not modify corneal properties. We also found no significant difference in CRF between GO patients and healthy controls. Although CRF derives mathematically from CH, the discrepancy between CH and CRF in our study represents the fact that each of these parameters reflects a different corneal biomechanical property. CH shows the viscoelastic mechanical damping ability of the cornea, and CRF indicates elastic resistance to it.
OHT in subjects with GO is estimated to be between 5% and 24%.1,5,35 In our study, 13.3% of GO patients were initially classified as having OHT based on IOP-GAT measurements, but when ORA correction was applied, 27.8% of patients were considered as having OHT. In those patients, closer IOP monitoring, functional and structural optic nerve tests were scheduled in case IOP lowering medication was needed.36,37 Persistent IOP rise may be associated with progression of glaucomatous neuropathy and lower CH has been associated with VF progression in glaucoma. 23 Therefore, further follow-up of our cohort of GO patients will elucidate which percentage of these patients finally develop glaucomatous optic neuropathy and if CH prove to be an independent predictor of glaucoma susceptibility in GO.
One of the limitations of our study lies in its cross-sectional design, with no long-term follow-up to determine if the patients classified as having OHT by IOPcc develop glaucomatous optic neuropathy. In addition, the sample was not large enough to identify differences in the CCT of GO patients compared to controls and patients were selected from an ophthalmic tertiary referral center, which could bias the severity of the cases. Despite these limitations, the homogeneity of our sample in terms of thyroid function control and inactive state of the disease make our observations useful and clinically meaningful. This is the first study that evaluates if CH is affected by severity or phenotype (myogenic/ lipogenic) of the disease. All the subjects who were evaluated belonged to the same ethnic group, avoiding potential biases related to interracial variations.
In conclusion, CH in inactive and euthyroid Grave’s Orbitopathy patients is lower compared to control eyes. According to our results there is no significant difference in corneal biomechanical properties between mild and moderate-to-severe GO nor between myogenic and lipogenic orbital disease. This finding suggests that corneal ultrastructural changes occurring in GO are not related to severity of the disease (in terms of clinical parameters – EUGOGO protocols) or predominantly myogenic/lipogenic orbital changes. IOP-GAT may underestimate IOP in inactive GO patients and close follow up should be specially consider in patients with borderline IOP readings and suspicious cupping.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Correction (March 2023):
Article updated to correct the title to “Influence of corneal biomechanical properties on intraocular pressure measurement in different types of Graves' orbitopathy”.