
Abstract
Background/Objectives
Reconstruction of the medial canthal region is challenging due to the complex regional anatomy. Options to reconstruct a medial canthal tendon sacrificed during tumour removal is limited. We present a novel surgical technique where hinged tarsal flap serves to substitute the canthal tendons.
Methods
This is a retrospective consecutive case series of five patients that underwent canthal reconstruction using this novel technique between May and December 2020. Electronic patient records and medical photograph database were reviewed. Patient demographics, co-morbidities, location and histology of the lesion, size of the resultant defect, reconstructive technique and post-operative complications were noted.
Results
All patients had good eyelid stability with no malposition, lagophthalmos or exposure keratopathy. No or minimal distraction of the eyelid from the globe, good cosmetic outcomes and no troublesome watering was reported. No wound dehiscence, no sight loss and no further surgical intervention was warranted.
Conclusion
Multiple techniques have previously been described to reattach the medial canthal tendon with silk or supramid sutures. Transnasal wiring, stainless-steel screw and mini-plate fixation are also described, but carry a high risk of complications and are unfamiliar amongst most oculoplastic surgeons. Our technique is quick and simple and utilises autogenous tissue without breaching the periosteum which acts as a natural barrier to tumour infiltration.
Refashioning the canthal tendon aids to lengthen the remaining eyelid stump, reducing the horizontal length required to reform the newly constructed eyelid and facilitates the reconstruction.
Introduction
Basal cell carcinomas (BCC's) occur in the medial canthal region in 30% of cases. 1 Reconstruction of this area is particularly challenging due to the complex regional anatomy. It serves important functional and aesthetic purposes. Defects can compromise the lacrimal drainage system causing troublesome epiphora. In some instances, this can be addressed during primary repair. However, with extensive defects where upper and lower canaliculi have been resected, delayed surgical techniques may be more appropriate. Insertion of a Lester jones tube at a later date can be considered. This is infrequently required in this cohort of patients as tear production decreases with age. 2 Epiphora can also result if the eyelid is not satisfactorily anchored posteriorly at the medial canthus, ensuring the eyelid sits adequately against the globe. This prevents pooling of tears between the globe and distracted eyelid, facilitating tear drainage. It is important to ensure adequate tension and stability of the eyelid to prevent lid malposition and optimise eyelid contour, cosmesis and avoid telecanthus. 3
In cases where the medial canthal tendon (MCT) is completely sacrificed during tumour removal, options to refashion a MCT to anchor the lid to periosteum or bone are limited. The MCT originates from the anterior and posterior lacrimal crest. This fuses temporal to the lacrimal sac then splits to attach to the tarsal plate in the upper and lower eyelid. The attachment to the anterior lacrimal crest is tough, whereas the posterior attachment is frail but ensures the lid is drawn posteriorly and is adequately opposed to the globe. 4
If a stump of MCT attached to the posterior lacrimal crest can be identified, reattachment of the tarsal plate to this stump will ensure the eyelid is adequately anchored posteriorly. If no residual MCT can be identified then direct fixation of tarsal plate to the posterior lacrimal crest periosteum can be achieved with a 5/0 vicryl suture. If the periosteum is deficient or absent a titanium miniplate can be fixed to the bone and used to anchor the tarsal plate. 3 Multiple techniques have previously been described to reattach the MCT with silk or supramid sutures. Supramid carries high rates of infection and abscess formation. 5 Transnasal wiring and a stainless-steel screw placed in the naso-orbital region to anchor the MCT and miniplate fixation have also been described.3,6,7 These are rarely used in modern day practice due to potential complications and their unfamiliarity amongst oculoplastic surgeons. Risk of injury to ocular and periocular structures, profuse bleeding from nasal mucosa, pressure necrosis, skin ulceration, perinasal scarring and epistaxis are all recognised complications of these techniques.
One option to refashion the MCT is a periosteal rotational flap. 8 Periosteum is a resilient autogenous structure, which is easily harvested and mobilised from the bridge of the nose. The main drawback in patients with periocular tumours is that the periosteum is considered a natural barrier to tumour extension and therefore, disruption of this barrier should be carefully considered and ideally utilised as a last resort.
We present a case series utilising an alternative novel surgical technique where a hinged tarsal flap serves to substitute the canthal tendons. To the best of our knowledge this has never been reported in the literature.
Methods
This is a retrospective consecutive case series of all patients that underwent canthal reconstruction using this novel technique. We retrospectively reviewed all case notes, both electronic and written. Patient demographics, location and histology of the lesion, medical co-morbidities, medications including anticoagulants and smoking status were recorded. The size of the resultant defect following Mohs micrographic surgery (MMS), reconstructive technique and post-operative complications were also noted. We reviewed all available photographs from the medical database, including pre-operative lesions, defects following tumour excision and reconstruction.
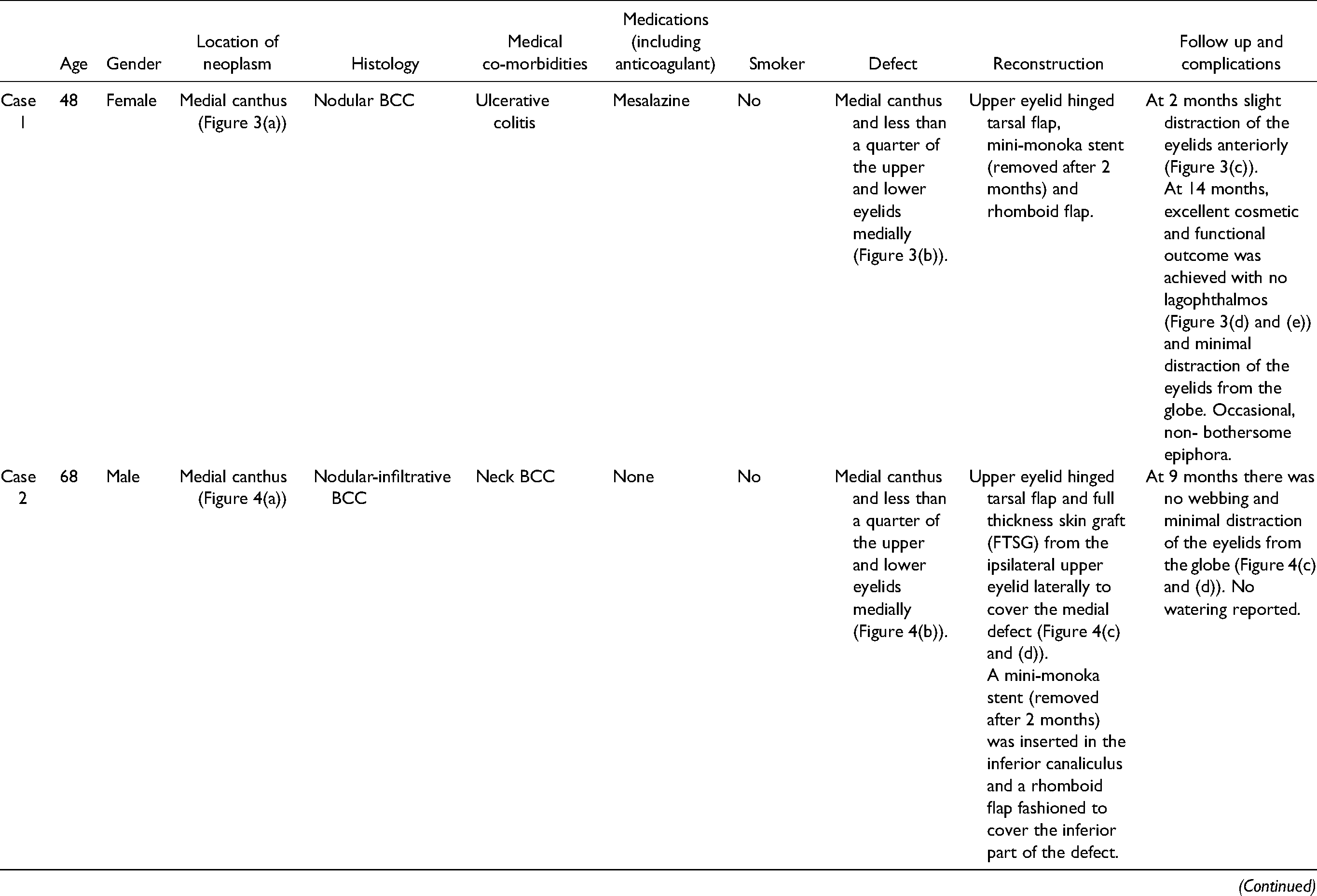
This technique has been utilised in 5 patients following loss of the medial or lateral canthal tendon after MMS of a BCC, performed by the supervising author between May 2020 and December 2020. All patients underwent a hinged tarsal flap to reform the medial or lateral canthal tendon combined with other reconstructive techniques as detailed in Table 1.
Details the patient demographics, co-morbidities, lesion histology and location, size of the resultant defect, reconstructive technique, follow up and complications.
We adhered to all tenants of the declaration of Helsinki. Waiver off consent was given by institutional ethics committee as this was a retrospective study.
Surgical technique
Figure 1 illustrates the surgical technique. Operations were performed under local or general anaesthetic (LA/GA). With LA, the surgical site is infiltrated with 0.5% bupivacaine with adrenaline (1 in 200, 000). Figure 1(a) and (b) demonstrates the extent of the defect. The patient had a small temporal portion of their lower eyelid remaining, necessitating reconstruction with a Hughes flap in addition to a hinged tarsal flap. In Figure 1(c), a 4/0 silk traction suture was placed and the upper eyelid everted using the desmarres retractor. To ensure stability of the upper eyelid, a mark was made 4 mm from the lid margin, and residual tarsus above that point incised horizontally and vertically towards the superior fornix. The tarsus was dissected from the overlying orbicularis and advanced on its conjunctival pedicle (Figure 1(d)). The retractors (levator aponeurosis and mullers) were also recessed. A mark was made vertically near the edge of the tarsal plate (Figure 1(e) and (f)) and a tarsal flap fashioned using a wick blade (Figure 1(g)). Curved artery clips were used to expose periosteum at the posterior lacrimal crest (Figure 1(h)). Double ended 5/0 vicryl was passed through the periosteum (Figure 1(i)) ensuring the lid is anchored posteriorly and well opposed to the globe. Both ends of the suture were then passed through the full thickness of the tarsal strip, from its posterior to anterior surface (Figure 1(j) and (k)). The suture is tied with the knot located on the anterior surface of the tarsal flap (Figure 1(l)). Once the reconstruction is complete, a compressive dressing was applied with gelonet, double pads and elastoplast and left in place until follow up at 1 week. At 2 weeks patients are advised to commence massage for 5 min every hour for the first month, then 5 min four times a day for 6 months then twice a day for 6 months.
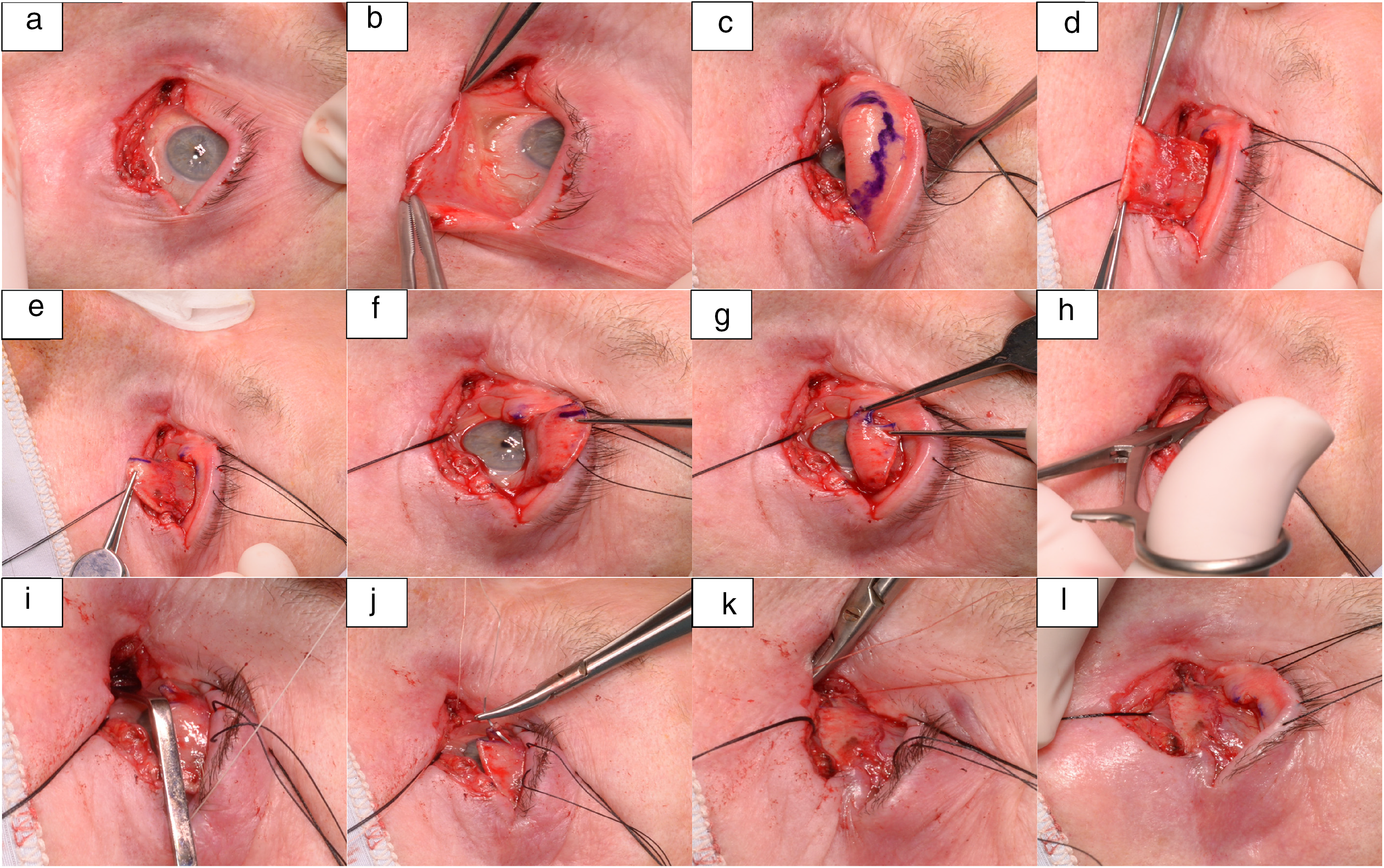
Illustrates how this novel surgical technique, the hinged tarsal flap is performed.
Figure 2 illustrates a simplified diagram of our hinged tarsal flap technique.

Illustrates a simplified diagram of the hinged tarsal flap technique. (a) Illustrates a left lower eyelid medial canthal defect (red hashed region illustrates the defect). (b) illustrates a mark made vertically near the edge of the tarsal plate along most of its length. (c) illustrates the tarsal flap after it is fashioned using a wick blade and rotated at 90 degrees on its hinge. (d) the red line illustrates placement of a double ended 5/0 vicryl suture through the posterior lacrimal crest and then both ends passed through the full thickness of the tarsal strip from its posterior to anterior surface, in vertical alignment. (e) illustrates position of the eyelid once both ends of the 5/0 vicryl are tied together, bringing the eyelid into a good anatomical position.
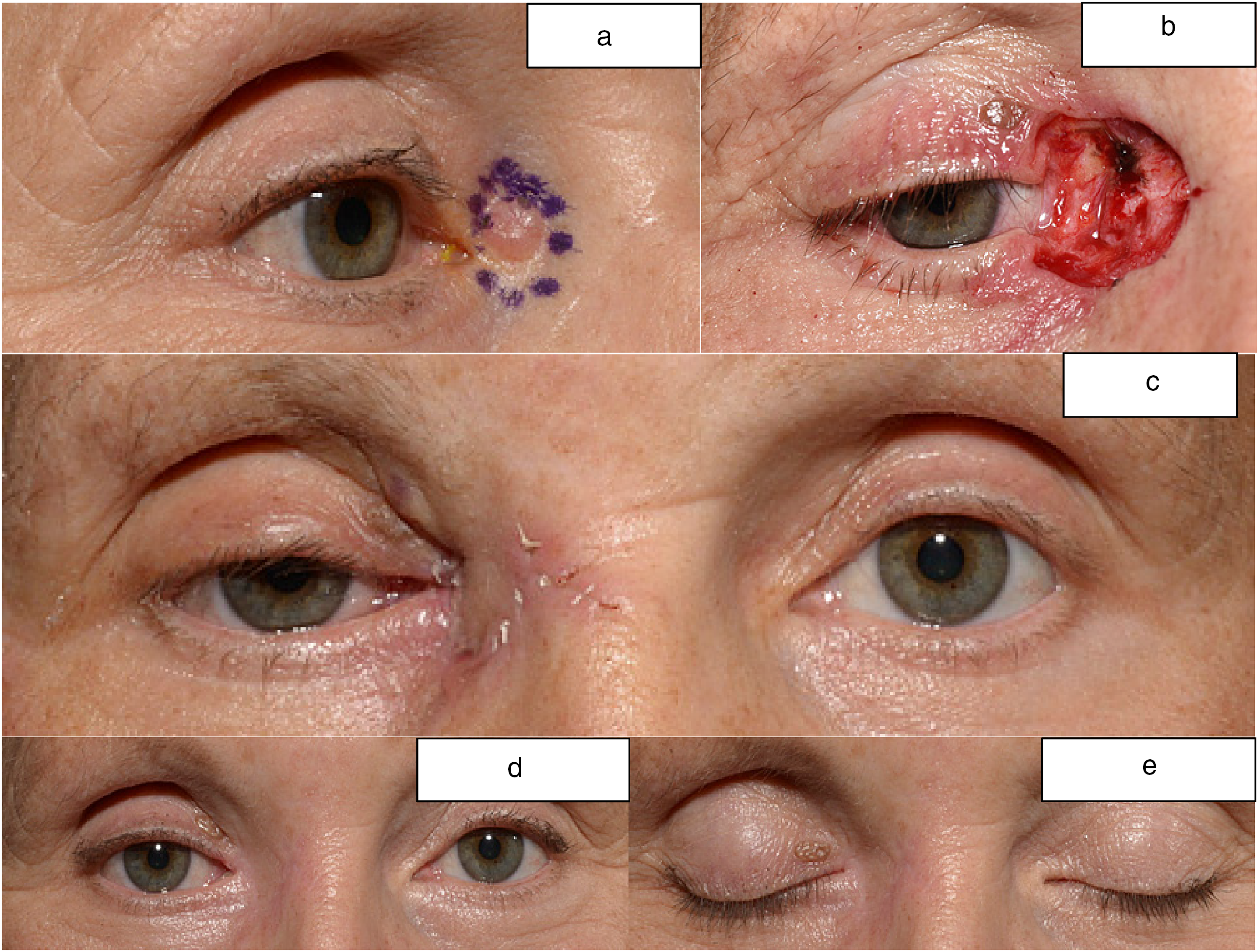
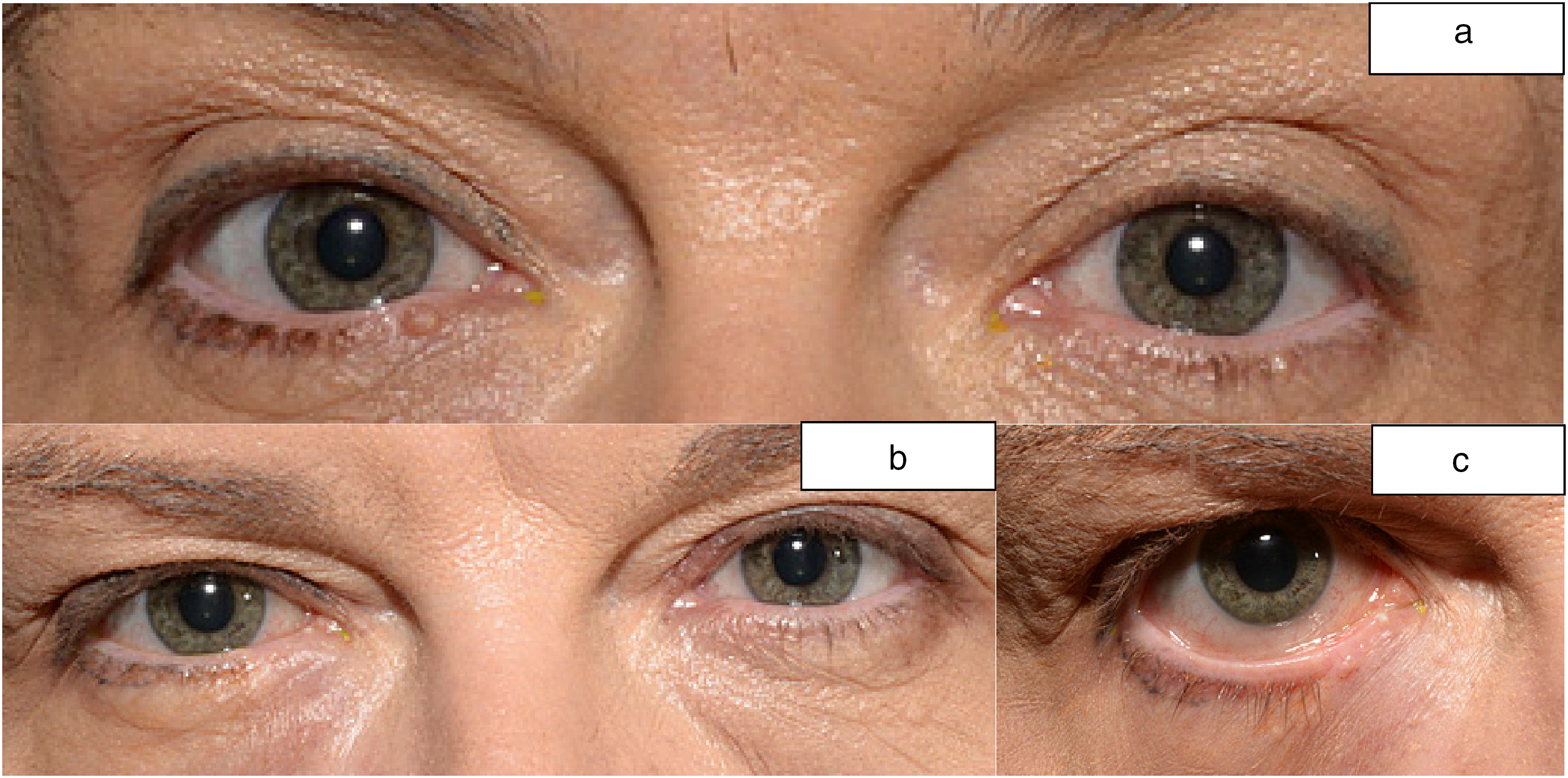
(a) illustrates a nodular basal cell carcinoma (BCC) in the right medial canthal region. (b) Illustrates the defect following excision by Moh's micrographic surgery (MMS). (c) Illustrates the post-operative appearance 2 months following reconstructive surgery (RS) with slight distraction of the eyelids anteriorly. (d and e) Illustrates the post-operative appearance 14 months following RS.
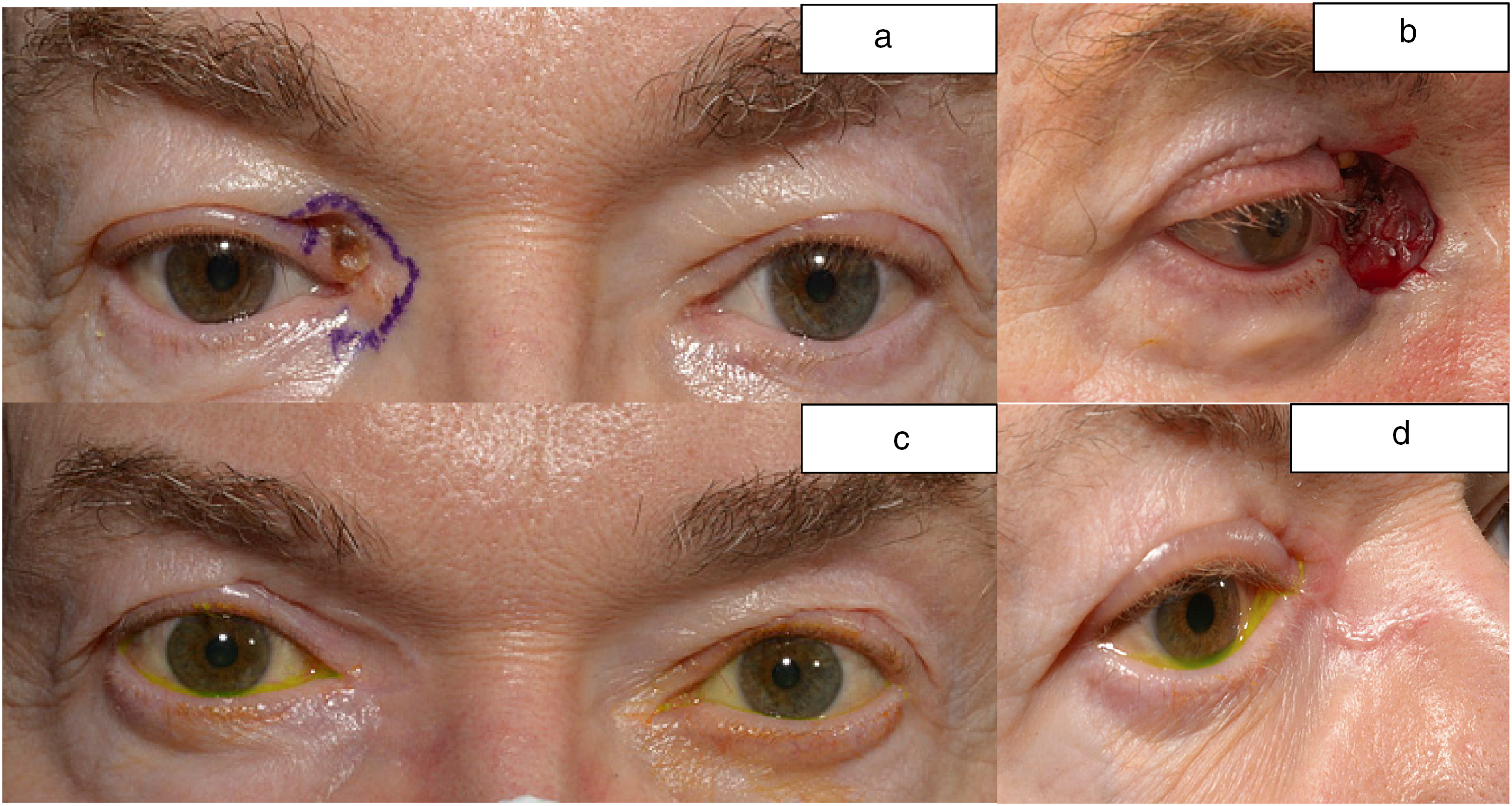
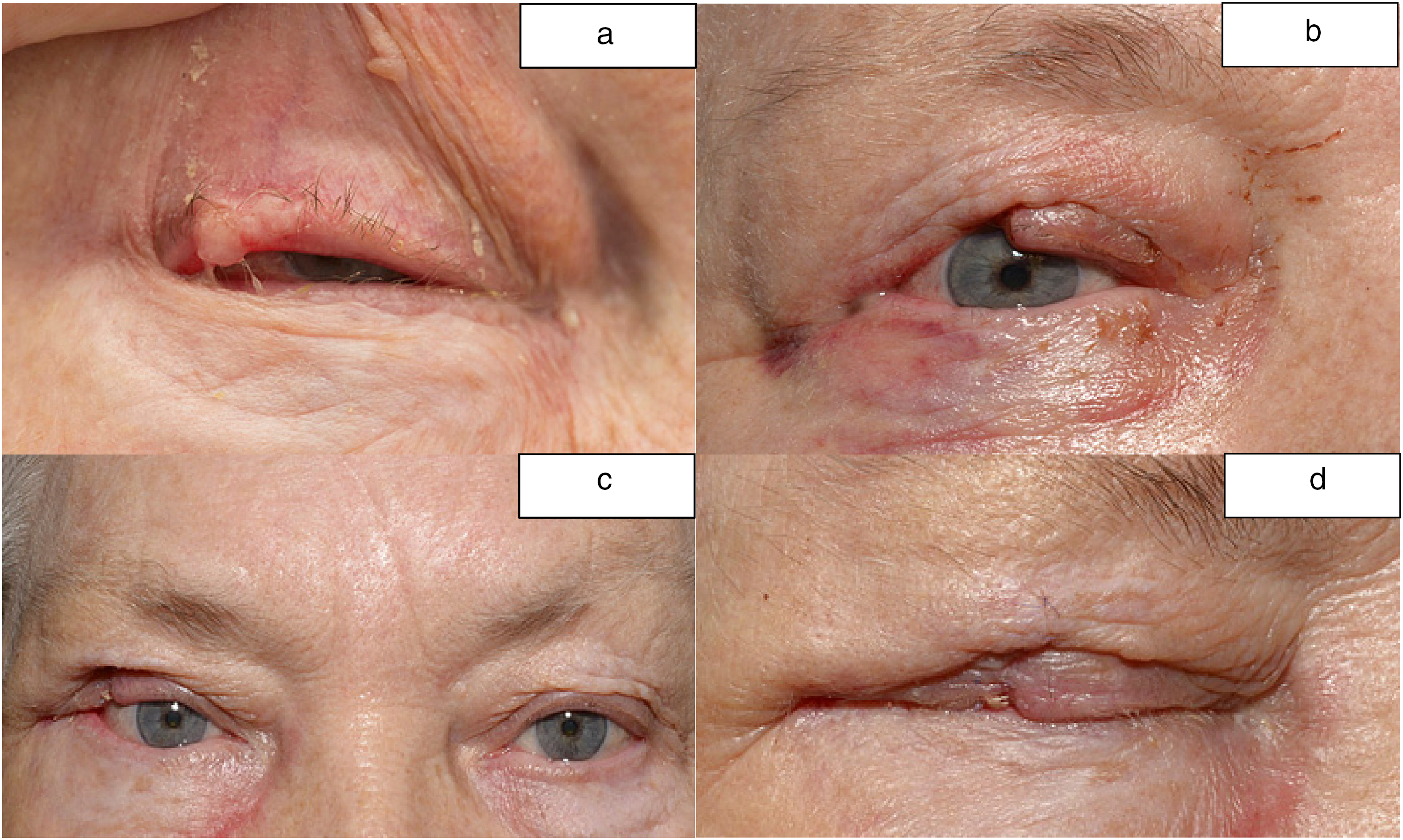
(a) illustrates a nodular-infiltrative BCC in the right medial canthal region. (b) Illustrates the defect following excision by MMS. (c and d) Illustrates the post-operative appearance at 9 months following RS with minimal distraction of the upper eyelid from the globe.
(a) illustrates a nodular BCC in the medial third of the right lower eyelid. (b and c) Illustrates the post-operative appearance at 8 months.
(a) illustrates a nodular BCC in the lateral third of the right upper eyelid. (b) Illustrates the defect following excision by MMS. (c and d) Illustrates the post-operative appearance at 10 months.
Results
Cases are detailed in Table 1. All patients had good stability of the eyelid with no eyelid malposition, lagophthalmos or exposure keratopathy. No or minimal distraction of the eyelid from the globe was noted. No troublesome watering of the eye was reported. All patients had a good cosmetic outcome, there was no wound dehiscence and no further surgical intervention warranted. No sight loss ensued.
Conclusion
Reconstruction of the MCT is required in cases where it is completely resected as an unavoidable consequence of tumour infiltration and subsequent resection. To date, this technique has only been used in patients where the medial or lateral canthal tendon has been resected during cancer excision, however it could be utilised for reconstruction following traumatic loss of the canthal tendons.
We believe our technique offers multiple advantages. It is relatively quick and simple to perform. It utilises autogenous tissue, without breaching the periosteum which acts as a natural barrier to tumour infiltration. In most cases where the MCT is resected following excision of a periocular cancer, it is of extreme benefit to be able to refashion the canthal tendons to reduce the horizontal length required to reform the newly constructed eyelid and facilitate the reconstruction. We believe this technique should form part of any oculoplastic surgeon's armamentarium to aid eyelid reconstruction. It can be utilised with other reconstructive techniques to lengthen the remaining stump of the eyelid. It has excellent functional and cosmetic outcomes with no significant complications encountered in our series. Larger comparative case series are needed to further explore outcomes of this surgical technique.
Footnotes
Abbreviations
Acknowledgements
We would like to acknowledge our medical photographers, Emily Hogan and Ben Taylor- Day for the images in this publication.
Author contributions
MA was responsible for conducting a search to identify suitable patients, data collection, literature search and writing the manuscript. CW was responsible for conducting a literature search, writing the manuscript and reviewing the manuscript. KT reviewed and provided feedback on the report.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.