
Abstract
Purpose
The aim of this study was to evaluate the clinicopathological features and flow cytometry (FCM) of tumor tissues in ocular adnexal diffuse large B-cell lymphoma (DLBCL).
Methods
This retrospective, multicenter case study was designed to evaluate the clinical and immunohistochemical features of tumors. DLBCL was diagnosed based on histopathology, immunoglobulin (Ig) heavy chain gene rearrangement, and FCM in all surgically removed periocular tumor tissues. This study involved assessing percentages (%) of B-cell/T-cell markers, a natural killer cell marker, and cell-surface Ig kappa/lambda (κ/λ) expression measured by FCM analysis in tumor tissues.
Results
Eleven DLBCL patients (4 men and 7 women) with 11 tumors were enrolled in this study. The median age at the time of initial presentation was 73 years. The tumor cells were immunohistochemically positive for cluster of differentiation (CD) 20, while CD5 was negative in all 8 cases tested. At the time of ophthalmic diagnosis, two cases already showed systemic dissemination of DLBCL throughout the body. FCM of tumor tissues detected a high percentage of B-cell markers including CD19 and CD20 in all 11 tumors. One case with high CD10 levels in FCM was histologic transformation from follicular lymphoma. One case with a relatively low CD20 population involved a history of systemic treatments including intravenous rituximab.
Conclusion
Although caution should be exercised when interpreting the data, FCM is useful for not only supportive diagnosis complementary to immunohistochemistry, but also facilitates a better understanding of immunopathology including histologic transformation of follicular lymphoma to DLBCL in the ocular adnexa.
Introduction
Most orbital lymphomas are of B-cell origin (97%), comprising extranodal marginal zone B-cell lymphoma (EMZL) (59%), followed by diffuse large B-cell lymphoma (DLBCL) (23%), follicular lymphoma (FL) (9%), and mantle cell lymphoma (MCL) (5%). 1 Systemically, DLBCL is the most common non-Hodgkin lymphoma, which represents a heterogeneous disease that is clinically, biologically, and molecularly diverse. 2 Two principal DLBCL molecular subtypes consist of germinal center B-cell-like (GCB) and activated B-cell-like (ABC or non-GCB), which are closely correlated with the treatment protocols and life prognosis. 3 Histologic transformation (HT) of FL, that is, evolution of low-grade FL to high-grade lymphoma, is considered to be one of the mechanisms contributing to the development of DLBCL during the clinical course.4,5 Clinicopathological studies on ocular adnexal DLBCL (OA-DLBCL), however, are limited because they are less frequent than EMZL. 6
Flow cytometry (FCM) is useful for quantitative assessment of cell-surface markers in various leukocyte populations. A previous study showed that FCM is a useful adjunct to the pathological diagnosis of ocular adnexal B-cell lymphoma, 7 and our previous studies also verified this for EMZL and FL.8,9 The characteristics of FCM in EMZL were significantly elevated B-cell markers including cluster of differentiation (CD)19 and CD20 without CD10 positivity, as well as immunoglobulin (Ig) kappa-lambda (κ/λ) light chain deviation, while FL showed higher CD10 populations than EMZL (8, 9). For DLBCL, a larger series has been reported focusing on clinical features of OA-DLBCL in an East Asian population 10 and HT from EMZL to DLBCL arising from the ocular adnexa as well as the stomach and lung 11 however, the usefulness of FCM for the diagnosis and immunopathology of OA-DLBCL is not well-described.
The aim of this study was to evaluate the clinicopathological features and FCM results of OA-DLBCL, and clarify how to handle FCM data in order to start early treatments in clinical practice.
Materials and methods
This retrospective, observational study was approved by the institutional board of Hokkaido University Hospital (IRB number: 020-0137) and Teine Keijinkai Hospital (IRB number: 2-020084-00). At the latter hospital, two patients, including the representative cases, gave informed consent for the use of their imaging and clinical and pathological information in publications. The IRB at Teine Keijinkai Hospital approved the study on an opt-out basis, in which patients were given the opportunity to refuse to participate in the study via the website, since this was a non-invasive retrospective observational study. This study complied with the Declaration of Helsinki. Patients diagnosed with ocular adnexal tumors between January 2010 and May 2020 were enrolled.
Ophthalmic examinations such as best-corrected visual acuity (BCVA), intraocular pressure (IOP), slit-lamp microscopy, ocular position, eye movement, external ophthalmoscopy, Hess screen test, and fundus examination were performed in all patients. Then, orbital computed tomography (CT) and/or magnetic resonance imaging (MRI) were examined. All patients considered to have ocular adnexal lymphoproliferative tumors underwent biopsy of the tumors. Removed tumor tissues were cut into 3-4 pieces, the main part of which was fixed with paraformaldehyde, and histologically evaluated. The other tissues were immediately submitted for FCM without fixation. The remaining tumor tissues in selected cases were examined for immunoglobulin heavy chain (IgH) gene rearrangements by the Southern blot method. Epstein-Barr virus-encoded small RNA in situ hybridization (EBER-ISH) was performed in selected cases. The diagnosis was made on the basis of histopathology, FCM results, and/or IgH gene rearrangement monoclonality. Patients with other types of lymphoma arising from the ocular adnexa, such as EMZL, FL, MCL, and natural killer T-cell lymphoma were excluded. Only tumors of OA-DLBCL with reliable FCM data were assessed in order to achieve the objectives of this study (Table 1), whilst OA-DLBCL, which does not provide useful information on FCM from tumor tissue (e.g., conjunctival origin), was excluded from this study. Systemic investigations including whole-body CT, upper and lower gastrointestinal endoscopy (if necessary), bone marrow aspiration or biopsy, and fluorodeoxyglucose-positron emission tomography-CT (PET-CT) were performed. This study adopted the Ann Arbor staging system, a landmark staging system for lymphoma.
T-cell, b-cell, and other cell lineages (%) in diffuse large b-cell lymphoma of the ocular adnexa (ocular adnexal tumor FCM).
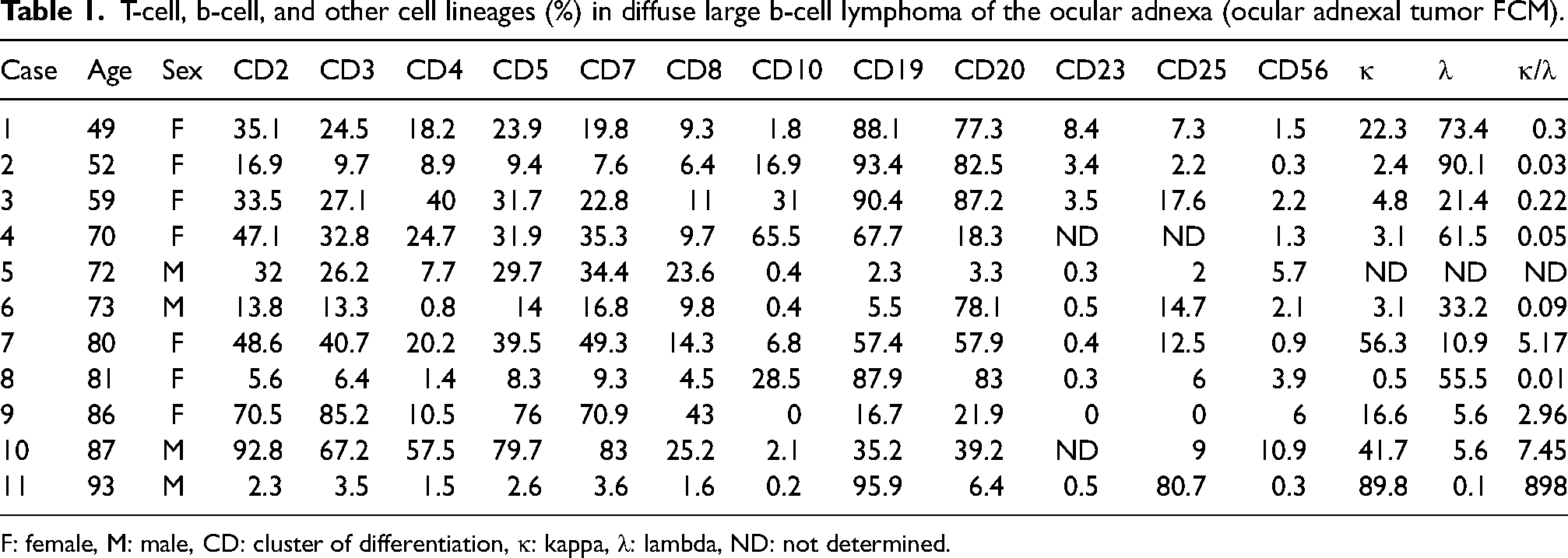
F: female, M: male, CD: cluster of differentiation, κ: kappa, λ: lambda, ND: not determined.
For the FCM method, cells were first incubated with fluorescein isothiocyanate / phycoerythrin (FITC/PE)-conjugated antibodies against T-cell markers (CD2, CD3, CD4, CD5, CD7, and CD8), B-cell markers (CD19, CD20, and CD23), a killer cell marker (CD56), CD10 as a marker of germinal center B cells, and cell-surface Ig κ/λ. After preparation of the cell suspension, the antibody reaction was carried out for 30 min at room temperature; within 2 h after washing when the cells were resuspended, five-color flow cytometric analysis was performed using a flow cytometer. Several parameters based on morphological characteristics and the FITC/PE intensity of the pan-leukocyte antigen CD45 were used to analyze the different cell populations.
Results
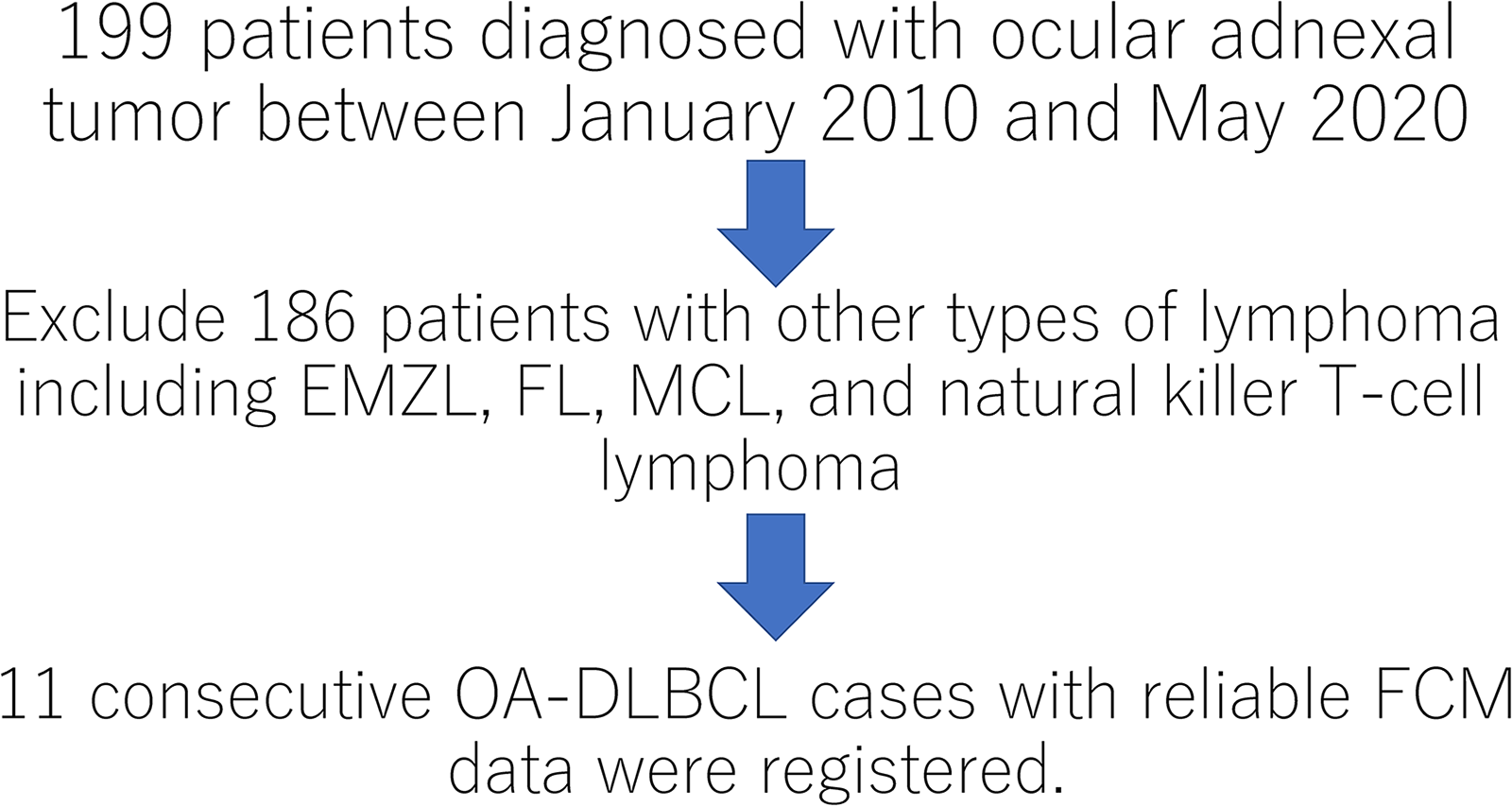
Flowchart fnor patient registration in this study.
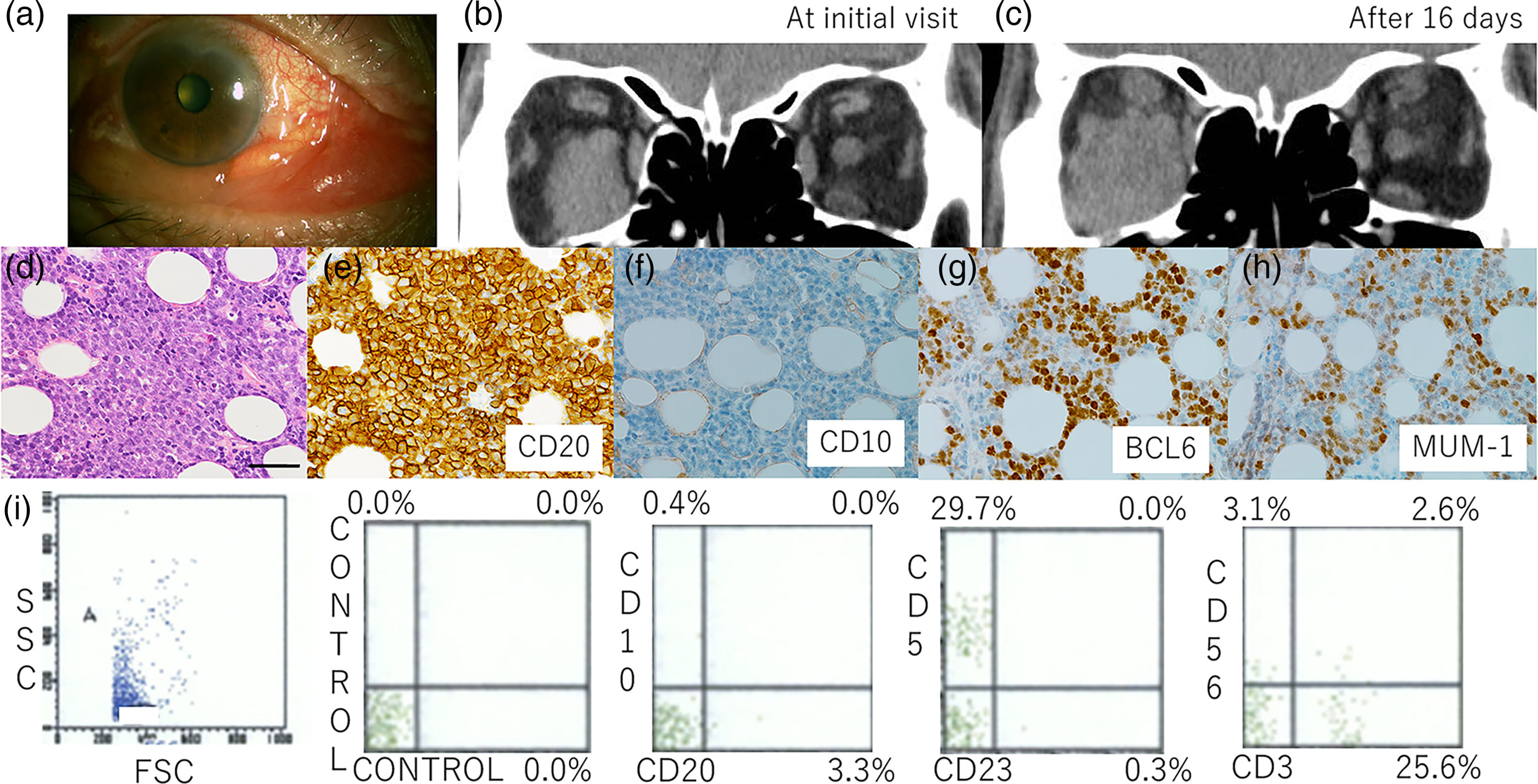
Imaging, pathological, and immunostaining findings in case 5.

Imaging, pathological, and immunostaining findings in case 4.
Discussion
Our 11 cases with OA-DLBCL had several clinical features, as follows: advanced-age patients (median age: 73 years), predominantly female (63.6%), and predominantly unilateral disease (90.9%). The tumor was mostly located in the orbit (54.5%) followed by lacrimal gland (36.3%) and lacrimal sac (9.0%). The initial ocular symptoms were eyelid swelling (63.6%), ptosis (18%), ocular proptosis (9%), and lacrimal sac swelling (9%). According to the Ann Arbor staging system, 77.0% (7 out of 9 patients) were seen with stage I, while 11.0% already showed systemic dissemination with stage III and IV at the diagnosis of OA-DLBCL. The multicenter study included 100 patients with OA-DLBCL who had a median age of 70 years, 54.0% were women, and 91% had unilateral lesions. 2 The most common tumor location was the orbit (54%), followed by conjunctiva (35%), lacrimal gland (18%), and eyelid (15%). 2 The most common ocular symptoms were lid swelling (75.0%), followed by irritation (32.0%), epiphora (23.0%), exophthalmos (20.0%), diplopia (16.0%), and ptosis (14.0%) (2). According to the Ann Arbor staging system, 56.0% were seen with stage IE, 15.0% with stage IIE, 6.0% with stage IIIE, and 23.0% with stage IVE. 2 Our clinical features including age, unilateral disease, ocular symptoms, and staging were consistent with those of previous multicenter studies.2, 13 Interestingly, the current study characteristically presented two cases of rapid growth on a weekly basis, and cases with marked eyelid swelling on initial ocular examinations. Therefore, OA-DLBCL should be suspected with such rapidly developing tumors, and be pathologically diagnosed more urgently than other ocular adnexal tumors.
We have previously reported the usefulness of FCM findings using tumor tissues in the diagnosis of EMZL and FL.8, 9 McKelvie et al. analyzed the clinicopathological findings together with FCM of ocular adnexal lymphoproliferative disorders, including 8 cases with OA-DLBCL; however, the details of FCM findings are unknown. 14 Therefore, data acquisition in clinical practice and the usefulness of FCM in the diagnosis of OA-DLBCL has yet to be elucidated. In our study, importantly, ophthalmologists could obtain FCM results as early as a couple of hours after submission to FCM analysis, being clearly much faster than routine histopathological diagnosis in clinical practice. Therefore, FCM is likely to contribute to the urgent evaluation of orbital tumors with rapid tumor growth, including OA-DLBCL.
This study further compared FCM findings and immunohistochemical results. CD20 was immunohistochemically positive in all 11 cases, where FCM showed that CD20 and/or CD19 was generally high and most cases revealed κ/λ deviation. These results suggest that FCM results in tumor tissues could help diagnose OA-DLBCL. However, this study discusses FCM results complementing OA-DLBCL diagnosis from 3 aspects regarding sample acquisition, interpretations of T-cell markers, and CD20 populations. First, in Case 5 (the first representative case), both CD19 and CD20 percentages were low together with high as proportions of T-cell markers and the lack of deviation in the κ/λ ratio. These results suggest that the resected tissues submitted for FCM did not contain sufficient amounts of DLBCL cells, although the histopathology specimen led to the diagnosis. Therefore, FCM could show a predominance of T cells without detection of a clonal B-cell population, as illustrated by Case 5, suggesting that this underscores the role of FCM as an ancillary test in lymphoma diagnosis. Second, immunohistochemical examinations showed negative results for CD5 in all 9 cases tested, and FCM showed a low CD5 percentage in most cases, but high levels in Cases 9 and 10. In these two cases, CD2 and CD3 were much higher than CD19 and CD20 with a high κ/λ ratio. Therefore, although two color analyses, looking at dual distribution of CD3/CD5 and CD5/CD20, were not available in this study, it might reflect the large number of reactive T cells infiltrating the tumor tissues. Third, in Case 4, histopathological results determined OA-DLBCL suggestive of transformation from FL; however, FCM showed high CD19, but low CD20 percentages. Since the patient has received R-CHOP chemotherapy, intravenous rituximab administration given to this patient might contribute to the down-regulation of cell-surface CD20 expression in OA-DLBCL, as previously reported. 15 Interestingly, the tumor cells were immunohistochemically positive for CD20 in Case 4. Tokunaga et al. proposed that a decrease in the copy number of MS4A1 (CD20) located at 11q12 could down-regulate CD20 mRNA expression in de novo DLBCL with a CD20 immunohistochemistry-positive/FCM-negative phenotype, suggesting that similar mechanisms underlie the phenotype in OA-DLBCL patients treated with intravenous rituximab administration. 16
Taken together, although FCM findings in tumor tissues are likely to support the diagnosis of OA-DLBCL and provide objective quantitative results complementary to immunohistochemistry, caution is required in interpreting the FCM findings, as follows: 1) the resected tissues submitted for FCM might not contain malignant lymphoma cells, 2) high T-cell proportions could reflect reactive T cells infiltrating DLBCL tissues, and 3) anti-CD20 targeted treatment may lead to the underestimation of the B-cell population, so B-cell markers including CD19 should always be assessed after anti-CD20 targeted therapy.
There are two possible mechanisms underlying the onset of HT from FL to DLBCL: divergent evolution of two distinct tumor populations from the original progenitor cell or emergence of an aggressive subclone from FL cells.17–19 Risk factors for HT include a higher FLIPI score at diagnosis (Age > 60 years, >4 nodal sites, LDH elevated, Hemoglobin < 12 g/dL) and grade 3-4 FL. 5 There was a report about HT of FL to DLBCL with a simultaneous MYC and BCL2 translocation (double-hit). It is also important to keep in mind that HT to DLBCL has been shown to be associated with a poor prognosis, with a median survival time of 14−27 months. 20 However, little is known about the contribution of FCM to the diagnosis of HT to DLBCL. In our case of HT of FL to DLBCL (Case 4), CD10 level was markedly high, being 65.5% higher than in other cases. Since our previous study showed many cases of high CD10 levels in FCM of FL, 9 CD10 values in FCM of OA-DLBCL might support the diagnosis of HT from FL.
The Hans algorithm using immunohistochemistry is widely accepted as a mechanism to divide DLBCL into GCB and non-GCB. 21 The algorithm is based on immunohistochemical expressions of CD10, BCL6, and MUM1 proteins. The GCB types includes CD10(−), BCL6( + ), MUM1(−) immunotypes, and CD10( + ) immunotypes, with varying proportions11,21 and generally a better prognosis. 22 This study classified DLBCL into GCB or non-GCB according to the Hans algorithm, and showed their association with clinicopathological parameters in patients. Indeed, there were 2 cases (Cases 2 and 4) consistent with the GCB type in this study: one case of HT from FL (Case 4), in which CD10 percentages in FCM were high, and the other case (Case 2) showing immunohistochemical CD10 positivity in the tumor tissue, where CD10 in FCM was relatively low, although there seems to be some discrepancy of results between FCM and immunohistochemistry. Taken together, high CD10 levels in FCM in OA-DLBCL may indicate two etiologies: HT from FL and GCB type; however, the prognosis remains controversial.
According to a recent review of clinical FCM data analysis in hematologic malignancies, 23 computational analysis methods including combined dimension reduction and clustering methods have been introduced, which are likely to contribute to the clinical work-up of systemic hematological malignancies. Therefore, the computational analysis based on FCM data would be expected to be employed for diagnosis and managements of patients with OA-DLBCL.
In conclusion, although caution is required when interpreting the FCM data, FCM findings in tumor tissues could support the diagnosis of OA-DLBCL and provide objective quantitative results complementary to immunohistochemistry, including tissue transformation from FL to DLBCL in the ocular adnexa.
Footnotes
Abbreviations
Precis
This study highlights clinical approaches using flow cytometry for the diagnosis and better understanding of the pathophysiology of ocular adnexal diffuse large B-cell lymphoma.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.