
Abstract
Purpose
Our study evaluated macular and optic disc vascular density (VD) changes in patients diagnosed with keratoconus, as compared with gender and age-matched healthy controls, in relation to the keratoconus stage.
Methods
This comparative cross-sectional study included adult patients who received a diagnosis of keratoconus at the Cornea Clinic. All scans consisted of two 4.5 mm × 4.5 mm images of the optic disc area and 6 × 6 mm images of the macular area using optical coherence tomography angiography.
Results
The study included 67 patients (26 women (38.8%) and 41 men (61.2%)) and 74 controls (31 women (41.9%) and 43 men (58.1%)). The mean ages of the keratoconus group and the control group were 30.0 ± 8.0 and 31.1 ± 7.5, respectively. Macular VD (whole, superficial, and deep) and peripapillary VD (whole) values were decreased statistically significant compared with the control group (p < 0.01 and p = 0.015, respectively). The keratoconus stage was negatively correlated with both the macular VD (p = 0.048, r = −0.314) and whole-peripapillary VD values (p = 0.03, r = −0.34).
Conclusion
Keratoconus might affect the posterior and anterior segments due to similar etiologies, including diminished collagen quality. Therefore, examination of the posterior segment should be performed thoroughly in keratoconus patients.
Introduction
Keratoconus is an eye disease that starts in the teenage years and progresses with irregular astigmatism, progressive corneal thinning, and corneal protrusion. 1 Abnormal collagen synthesis is thought to play a role in the pathogenesis of the disease. 2 An extensive study conducted in the Netherlands showed that the prevalence and incidence of keratoconus have increased compared to epidemiological studies that were completed 20 years ago. 3
Keratoconus is a multifactorial disease.4,5 Although it occurs sporadically, it is associated with diseases that include Down syndrome, 6 Turner syndrome, Leber congenital amaurosis, retinitis pigmentosa, mitral valve prolapse, 7 connective tissue disorders (including the Marfan and Ehlers–Danlos syndromes), osteogenesis imperfecta, and pseudoxanthoma elasticum. 8 Most of these diseases are disorders of collagen metabolism.
Previous studies have examined the central macular thickness (CMT), 9 choroidal thickness (CT), 10 lamina cribrosa thickness, 11 and normotensive glaucoma incidence 12 in keratoconus patients. In addition, cases with central serous chorioretinopathy and choroidal neovascular membranes have been reported in patients with keratoconus.13,14
In this study, we evaluated macular vascular and optic disc vascular density (VD) pathophysiologic changes in patients who were diagnosed with keratoconus during followed-up in our clinic, based on previous studies of the changes in the posterior segment of keratoconus. To the best of our knowledge, no previous report has evaluated the posterior segment using optical coherence tomography angiography (OCTA).
Materials and methods
Patients
This comparative cross-sectional study was performed between July and September 2019 at the Dr. Sadi Konuk Training and Research Hospital of the Health Sciences University in Bakırköy, Istanbul. This study comprised patients between the ages of 17 and 47 who were diagnosed with keratoconus at the Cornea Clinic of the Eye Department. The study comprised all newly diagnosed and previously followed patients who visited the cornea clinic within predetermined periods. The research protocols for this study were approved by the Ethics Committee of Dr. Sadi Konuk Research and Education Hospital and conducted in accordance with the tenets of the Declaration of Helsinki. Each participant or his/her guardian(s) provided written informed consent. The ethics committee approved the consent procedure. The age- and gender-matched control group consisted of healthy individuals with no history of ocular or systemic diseases. If both eyes were eligible, one eye was chosen at random for each subject. Patients who wore contact lenses removed their lenses at least 24 h before the examination.
Clinical keratoconus was diagnosed based on the presence of at least one biomicroscopic sign15,16 (including Vogt’s striae, Fleischer’s ring, or corneal thinning) and one or more of the following topographic map indices: (1) focal steepening areas more significant than 47 diopters (D) located in the cone protrusion zone surrounded by concentric decreasing power zones, (2) angling of the hemi-meridional differences more significant than 20–30° in a bow tie pattern, and (3) inferior–superior asymmetry more significant than 1.4 D within the mid-peripheral cornea.
The exclusion criteria included patients suffering from nonkeratoconus ocular diseases in both eyes (e.g., keratectasia, corneal degeneration, retinal disease like macular disease, diabetic retinopathy, and myopic degeneration), optic nerve disease (e.g., optic neuritis, optic atrophy), changes in visual field and any other retinal changes, ocular trauma, eye surgery, or any significant media opacity that obscured the fundus. The Amsler–Krumeich classification system was used to grade the severity of keratoconus; which considers the patient’s refractive error, central keratometry readings, central corneal thickness, and the presence or absence of scarring. Eyes classified as Stage 4 were excluded from the study because of their low image quality (signal strength index < 8/10).
Examinations
All participants underwent complete ophthalmologic examinations, including best-corrected visual acuity (decimal fraction), intraocular pressure using Goldmann applanation tonometry, slit-lamp examination of the anterior segment, and fundoscopic examination; all examinations were conducted by the same clinician (U.F.). Following the examination, we obtained corneal tomography using a Sirius device (Costruzione Strumenti Oftalmici; Florence, Italy) and retinal nerve fiber layer (RNFL) and OCTA measurements using an RTVue device (RTVue-XR OCT, Avanti version 2018.0.0.14; Optovue Inc., Fremont, CA, USA) from all patients.
The diagnosis of keratoconus was made by a corneal specialist based on the biomicroscopic examination and corneal tomography findings. Sirius tomography, which combines a slit-illumination system with an automatically rotating Scheimpflug camera to produce a three-dimensional model of the anterior segment, was used to perform a corneal topographic examination in a darkroom.
OCTA was performed by the same technician using the spectral domain OCT in the morning (9:00–11:00 am) to avoid possible diurnal variations. The split-spectrum amplitude-decorrelation angiography algorithm was used to process the volumetric scans. All scans included two 4.5 × 4.5 mm images of the optic disc area and two 6 × 6 mm images of the macular area. The RNFL thickness was averaged from a 3.4 mm diameter circular sampling profile centered on the optic disc. The OCTA device automatically performed the sectorial division of the peripapillary region as superior and inferior hemi-radial peripapillary capillaries, and all quantitative results were recorded.
The total scanned area occupied by blood vessels was used to define the peripapillary or macular VD. The VD was defined as the number of pixels with a decorrelation value over the noise threshold of the region, which was two standard deviations greater than the mean decorrelation value. 17 The radial peripapillary capillary (RPC) segment’s peripapillary vessels were studied in the superficial retinal layers. The RPC segment extends from the internal limiting membrane to the nerve fiber layer. The peripapillary region was divided into six sectors using the Garway–Heath map, and VDs were calculated for the entire peripapillary area (average) and for each sector.18,19
The macular VDs analyzed in this study assessed the superficial vascular plexus present in the inner layers of the retina (extending from the internal limiting membrane to the inner plexiform layer). The macular VDs were analyzed over a 1.5 mm-wide parafoveal, circular annulus centered on the macula. The parafoveal region was divided into four sectors of 90° each (nasal, inferior, superior, and temporal sectors).
All measurements were performed using the manufacturer’s tools and Analytical AngioVue software (RTVue-XR OCT, Avanti version 2018.0.0.14; Optovue Inc., Fremont, CA, USA). Only images with a signal strength index > 8/10 were used for the analysis of VD.
Statistical analysis
The statistical analysis was performed using the Statistical Package for the Social Sciences (SPSS), version 21.0 (SPSS, Inc., Chicago, IL, USA). The distribution of the data was evaluated using the Kolmogorov–Smirnov test. To compare the groups, Student’s t-test was used to analyze parametric data, and the Mann–Whitney U test was used to assess the nonparametric data. The Pearson correlation coefficient was used when two parametric variables were measured, and the Spearman correlation coefficient was calculated when variables were nonparametric. Multivariable analyses were performed using the general linear model included in SPSS. Statistical significance was set at P < 0.05.
The primary outcome measures were differences in peripapillary and macular VDs between the patients with keratoconus and the control eyes. The secondary outcome measures were the correlations between the keratoconus stages and the peripapillary or macular VD.
Results
This study included 67 eyes from 67 patients: 26 women (38.8%) and 41 men (61.2%) with 74 eyes of 74 control subjects: 31 women (41.9%) and 43 men (58.1%). The mean ages of the keratoconus patients and the control group were 29.0 ± 7.7 years and 30.8 ± 8.0 years, respectively.
According to the Amsler–Krumeich classification staging system for keratoconus, 44 (68.7%) patients were diagnosed as Stage 1, 13 (20.3%) patients as Stage 2, and 7 (10.9%) patients as Stage 3.
The statistical differences of the macular VD and peripapillary (RPC-VD) values between the patients and the control group are shown in Table 1 and Figure 1. According to the Table 1 and Figure 1, there was a highly significant difference between the keratoconus patients and the control group in the whole macular and RPC VD values (p < 0.001). No significant difference was observed in keratoconus and control groups in terms of foveal retinal thickness and average RNFL (p = 0.17; p = 0.63; respectively) The keratoconus stage was negatively correlated with the macular VD and whole RPC-VD values (p = 0.048, r = −0.314; p = 0.03, r = −0.34, respectively). The linear regression analyses of the negative correlation between the keratoconus stage and the macular VD and RPC-VD values are shown in Figure 2.
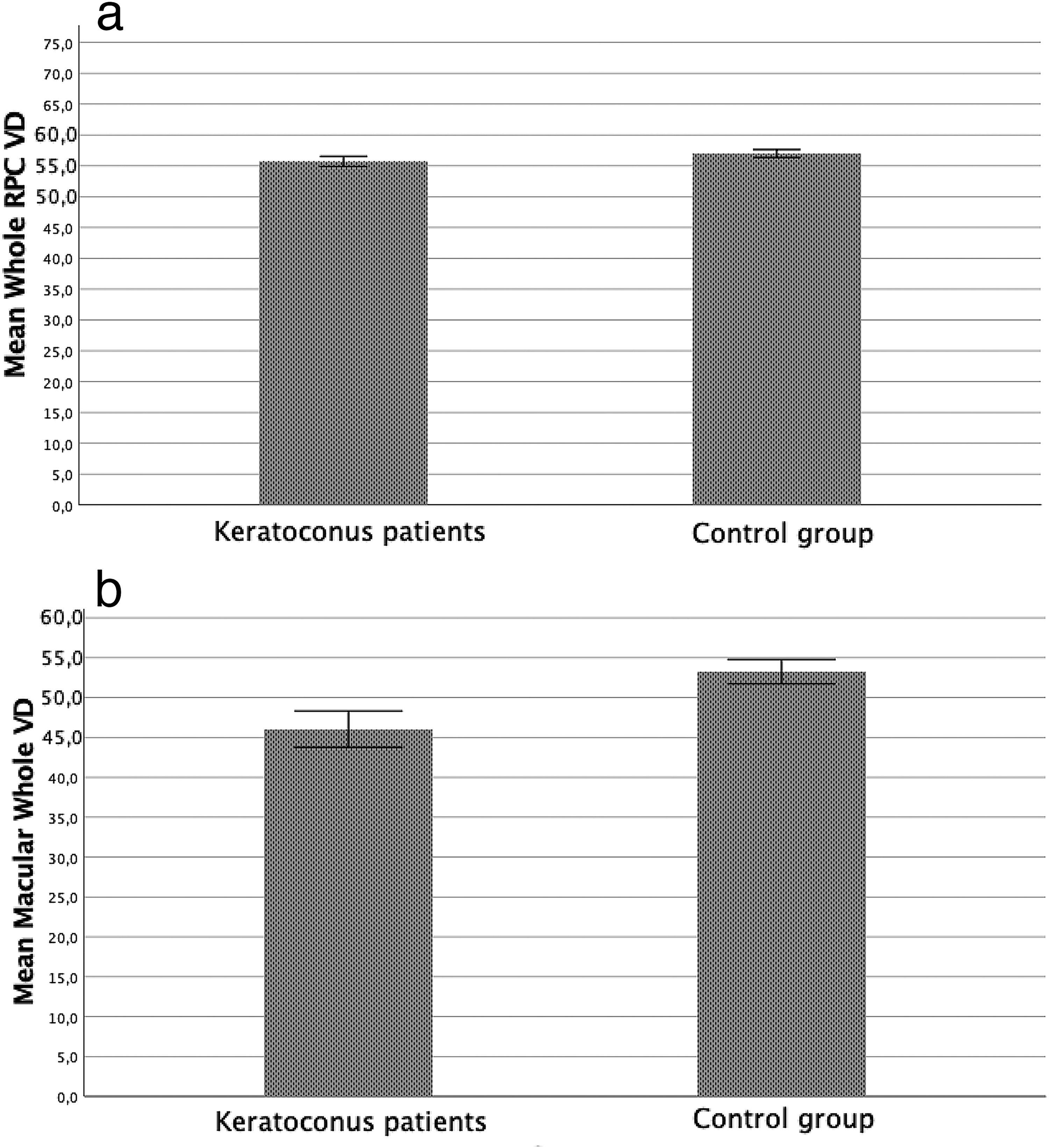
(a) RPC VD values in KC patients and control group. (b) Deep VD values in KC patients and control group.
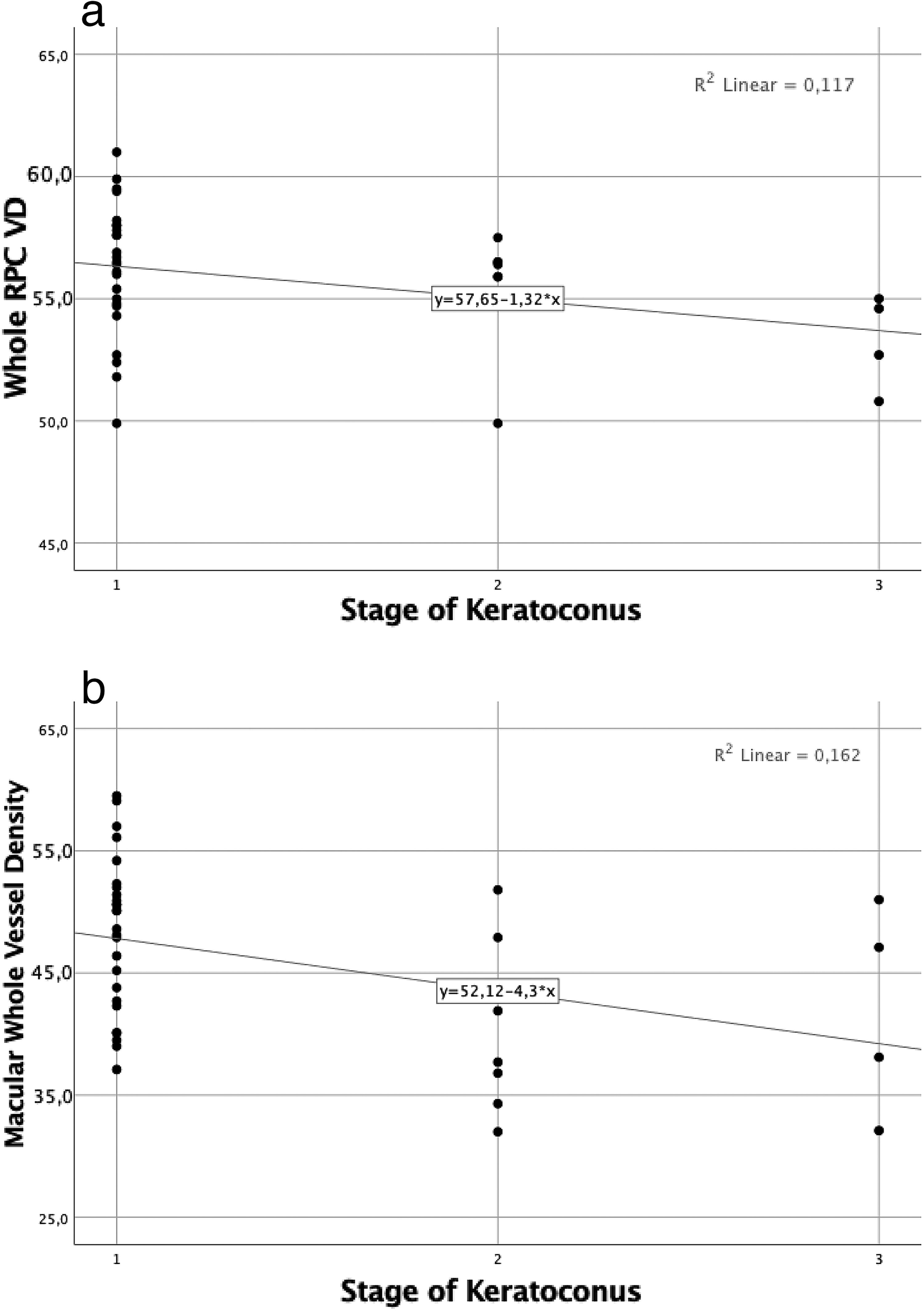
(a) The relation between stage of KC and RPC VD whole. (b) The relation between stage of KC and RPC VD deep whole.
Quantitative results of sim K, CCT, CXL history, RT, macular and peripapillary VD
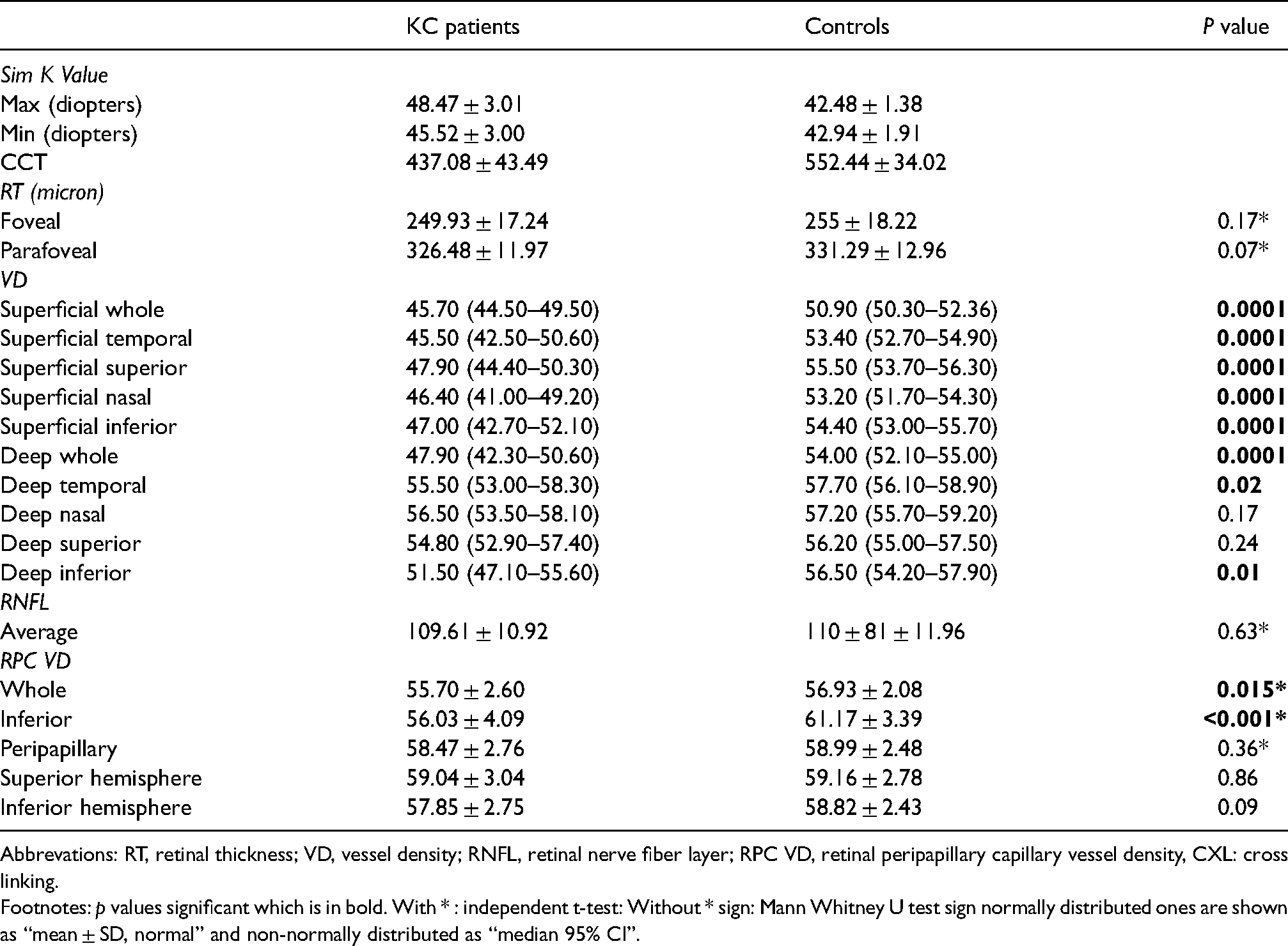
Abbrevations: RT, retinal thickness; VD, vessel density; RNFL, retinal nerve fiber layer; RPC VD, retinal peripapillary capillary vessel density, CXL: cross linking.
Footnotes: p values significant which is in bold. With * : independent t-test: Without * sign: Mann Whitney U test sign normally distributed ones are shown as “mean ± SD, normal” and non-normally distributed as “median 95% CI”.
Discussion
The study results indicated that keratoconus eyes had decreased macular and peripapillary VDs compared with the control eyes. These values decreased as the keratoconus stage increased. These findings might provide insight into the disease’s natural etiology in terms of its effect on the retina, vessel changes associated with collagen impairment, and inflammatory changes.
In many studies on keratoconus, it has been argued that advanced astigmatism does not affect OCT measurements in these patients.10,20–22 In a more specific study on the effect of astigmatism on OCT measurements, it was revealed that astigmatism did not affect macular thickness and did not significantly affect RNFL thicknesses. 21 In another cross-sectional study, it was emphasized that refractive error might affect signal strength, but OCT measurements were not influenced in those with normal signal strength. 22 These findings suggest that a possible artifact would not significantly affect the OCT values in keratoconus patients. In addition, we excluded measurements with low signal strength from our study to avoid potential errors.
Gutierrez-Bonet et al. found that the CT was thicker in patients with keratoconus. They associated this result with an excess of collagen type I in vein vessels. 10 Akkaya and Kucuk 11 reported that the lamina cribrosa was significantly thinner in keratoconus patients than in the control group, which suggests that the structural changes in the cornea of keratoconus patients might affect the sclera and optic nerve. Sahebjada et al. showed that the inner and outer macular thicknesses are affected by the early stages of keratoconus; when the disease progresses, the central fovea and macular volume are also affected. 9 Our data suggest that these structural properties of the cornea may be related to VD.
Several factors may contribute to decreases in VD values. The fact that keratoconus is a disease related to collagen metabolism suggests that the vascular wall might also affected because there are similar types of collagens in both tissues (types I, III, V). 23 Changes in some enzyme levels cause collagen disorder. 24 Matrix metalloproteinases are thought to be responsible for stromal degradation in keratoconus, 25 which also affects collagen. Some publications have suggested that this collagen disorder is associated with premature death. 26 Likewise, the strong association with connective tissue diseases (e.g., mitral valve prolapse and aortic aneurysm) is due to the presence of a collagen disorder. 27 Retinal vessels can be affected in the same way. In addition, inflammatory biomarkers are shown to be elevated,28,29 and oxidative stress markers are proven to be dysregulated in patients with keratoconus disease,30,31 which might contribute to decreases in the VD values.
Our study had a few limitations. We did not look at extra-ocular confounders (such as cigarette smoking, 32 or microvascular disease 33 ), which could have influenced the CT and corneal rigidity. Furthermore, axial length, which cannot be assessed with OCTA, was not analyzed in the present study.
Conclusions
Findings of our study suggest that keratoconus may affect posterior segment. Therefore, a posterior segment examination should be performed before considering keratoplasty. This highlights the need for more longitudinal studies on VD changes in keratoconus patients. In addition, posterior segment and VD changes among the relatives of keratoconus patients might be a predictor of keratoconus, could be used in suspicious cases, and might be useful as new biomarkers of keratoconus. Changes in peripapillary and macular VDs might be used as earlier indicators of the progression of keratoconus than changes in the CT, RNFL, and CMT measurements.
Footnotes
Author contributions
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work as a whole, and have given their approval for this version to be published. Sibel Zirtiloglu: study concept, design and main surgeon; Mustafa Suat Alikma: statistics and data analysis; Ozge Pinar Akarsu Acar: drafting and reviewing the manuscript; Fatih Guven: data entry and drafting the manuscript; Utku Furuncuoglu: drafting the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Project number and institution responsible for the approval of the Research Ethics Committee: 2018/3l6; Bakirkoy Dr. Sadi Konuk Training and Research Hospital.
Statement of ethics
The research protocol for this study was approved by the Ethics Committee of the Dr. Sadi Konuk Research and Education Hospital and conducted in accordance with the tenets of the Declaration of Helsinki. Each participant or their guardian(s) provided written informed consent. The ethics committee approved the consent procedure.
Study approval statement
This study protocol was reviewed and approved by Bakirkoy Dr. Sadi Konuk Eğitim ve Araştırma Hastanesi Klinik Araştırmalar Etik Kurulu, approval number “2021-15-11.”
Consent to participate statement
Each participant or their guardian(s) provided written informed consent. The ethics committee approved the consent procedure.
Data availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.