
Abstract
Purpose
To evaluate visual acuity, corneal aberrations, and densitometry post deep anterior lamellar keratoplasty (DALK).
Methods
Twenty-five eyes of 25 patients who underwent DALK for corneal stromal diseases with normal endothelium were enrolled in a prospective interventional study. Evaluation for corneal aberrations and densitometry postoperatively was performed using Scheimpflug imaging at 6 months. Anterior Segment Optical Coherence Tomography (ASOCT) was done for host-graft morphology. Correlation analysis of postoperative best-corrected visual acuity with corneal aberrations and corneal densitometry (CD) was performed.
Results
Big bubble deep anterior lamellar keratoplasty (BB-DALK) was successful in 18 patients, while 7 eyes underwent manual dissection due to failed BB (Big Bubble) technique. The mean BSCVA was 1.35 ± 0.46 logMAR units pre-operatively which improved to 0.36 ± 0.19 logMAR units post DALK at 6 months (P < 0.001). The mean Root Mean Square (RMS) (μm) of the magnitude of total corneal aberrations, HOA and LOA from central 6mm zone of cornea were 14.6 ± 9.2, 4.7 ± 2.9, and 13.8 ± 8.8, respectively. The mean anterior (120μm), central and posterior corneal (60μm) densitometry in 0–2mm zone were 25.8 ± 7.7 GSU, 18.7 ± 4.16 GSU and 10.09 ± 3.9 GSU respectively. A statistically significant correlation of postoperative residual stromal bed thickness, total corneal HOA, LOA, total corneal aberrations, HOA front and posterior corneal densitometry (0–2mm zone) with postoperative BSCVA was found.
Conclusion
Though there is a significant improvement in BSCVA after DALK, the quality of vision in terms of aberrometry and densitometry is suboptimal, especially in cases undergoing manual DALK compared to those undergoing big bubble formation.
Introduction
For the past 100 years, full thickness corneal transplantation has been the treatment for corneal diseases. During the last decade, for the treatment of corneal diseases that do not affect the corneal endothelium and Descemet membrane, Penetrating Keratoplasty (PKP) has been replaced by deep anterior lamellar keratoplasty (DALK), in which maximal corneal stroma is removed and host endothelium is preserved.1–5
The main advantage of DALK being that the patient's own endothelium is preserved which reduces the risk of endothelial rejection, immunological reactions and graft failure, thereby decreasing the duration of postoperative steroids. It also helps in lower rates of endothelial cell loss which leads to longer graft survival.2,6,7
Several studies8–12 have reported that the type of donor recipient interface that is achieved in DALK affects the final visual acuity outcomes. It has been observed that excellent interface optical quality is seen in cases where recipient stroma is removed upto the Descemet membrane (DM), with results comparable to PKP. While quality of vision was inferior to that seen in PKP in cases where additional stroma is left.13,14 However, some patients who had a bare Descemet membrane intraoperatively and excellent donor transparency and interface postoperatively, still did not gain good Best Spectacle Corrected Visual Acuity (BSCVA). 15
Post DALK visual performance can be limited due to multiple factors, like light scatter by surgical interface, lower and higher order aberrations, etc.14,15 However, there is still not a very clear understanding of the contribution of these factors in post DALK visual acuity.
The quantitative analysis of the optical properties after selective lamellar keratoplasty can be done by studying corneal aberrations, light scattering and thickness of the donor. 16 This has been possible due to the advancement in technology and tools like Anterior Segment Optical Coherence Tomography (ASOCT) and Scheimpflug imaging which evaluate the lenticule and host cornea separately. So far, all the available studies of aberrometry and densitometry post-DALK have been reported with indication for surgery as keratoconus. A prospective study to correlate vision with aberrometry, densitometry, and residual stromal thickness post-DALK done for varied stromal pathologies using Scheimpflug imaging and ASOCT was undertaken.
Methods
Twenty-five consecutive patients with varied stromal etiologies who underwent DALK were enrolled in a prospective interventional study. The study was approved by the Institutional ethics committee and registered (clinical trials registry- CTRI/2020/03/024283). It was conducted in accordance with the Declaration of Helsinki. Only patients with uncomplicated postoperative course were included in the study. Patients with abnormal posterior segment findings (advanced glaucoma, retinal detachment etc.) were excluded from enrollment. They were followed up for a minimum of 6 months after surgery.
All patients underwent a comprehensive ophthalmological examination. BSCVA at 6 months being primary outcome while secondary outcomes were corneal densitometry, aberrometry from anterior and posterior corneal surface and graft-host thickness. BSCVA (LogMAR), refraction, graft clarity, graft apposition, tonometry, and fundoscopy were evaluated at every follow-up. Pentacam HR imaging (Oculus, Wetzlar, Germany) was done for anterior and posterior surface aberrations, graft and host corneal thickness and densitometry. Additionally, ASOCT (SS-1000; CASIA, Tomey, Nagoya, Japan) was done for graft-host interface evaluation at 6 months follow up. The endothelial count was done using non-contact specular microscope (SP3000, Topcon, Tokyo, Japan).
Corneal wavefront aberrations
Pentacam HR imaging software version 1.21r24 was used for corneal wavefront aberrations measurement at 6 months (Oculus, Wetzlar, Germany). The images were taken by a trained optometrist in standard scotopic conditions with undilated pupil. Wavefront aberration data is provided for anterior, posterior and total cornea. Average of three measurements was used to calculate the root mean square (RMS) values (μm) of total corneal aberrations, LOA and HOA across the central 6.0 mm diameter of the cornea. Zernike polynomial expansion upto 6th order was used to calculate wavefront errors.
Corneal densitometry
The densitometry program in Pentacam automatically locates corneal apex and takes 25 images over different meridians of cornea with uniform blue light source. Grayscale unit (GSU) is used to indicate the densitometry output; value ranges from 0 (minimum light scattering) to 100 (maximum light scattering). The software is provided with coded instruction to subdivide the cornea into 4 concentric zones areas; central zone from 0–2mm; second zone extending from 2 to 6mm; next from 6 to 10mm and fourth from 10–12mm zones. Corneal depth is divided as anterior layer (120µm), central layer and posterior layers (60µm). The central layer has no fixed thickness; it is measured by subtraction of anterior and posterior layers thickness from overall corneal thickness. 17 All measurements were taken under uniform ambient light in the same clinical assessment. In this study, densitometry analysis was done for all layers in 0 to 2 mm zone only (overlying the pupil). Peripheral values were excluded because they were beyond graft host junction and outside the optical zone.
Twenty subjects with no significant ophthalmological problem were also enrolled in the study for assessment of normative data of aberrometry and densitometry from both eyes on Scheimpflug under similar conditions.
Surgical technique
All patients underwent DALK after informed consent under peribulbar/ general anesthesia. Surgeries were performed by a single corneal surgeon (RA). Partial thickness trephination was done using Hessberg Baron trephine (7.5mm trephine size in 3 patients, 22 patients had either 8.5 or 9mm). The trephines were set to 70–80% of averaged peripheral thickness from four points intraoperatively. This partial-thickness trephination was deepened. Superficial debulking of the corneal stroma was done, Cleavage between stroma and DM was attempted using standard “big bubble” technique with a bevel down, bent 30-gauge needle. In cases of successful big bubble, supradescemetic stromal layers were incised using a 15-degree knife and removed using divide and conquer technique after replacing air with 1% sodium hyaluronate. In cases where attempt to form big bubble failed repeatedly, manual dissection layer by layer of recipient corneal stroma was done as deep and close to DM as possible.
For all transplants, donor corneal buttons preserved in corneal storage medium at 4°C were used. 0.06% trypan blue dye was used to stain DM and endothelium of same sized donor graft which were then scraped using a dry sponge. Any residual viscoelastic material and debris were washed off from the recipient stromal bed prior to suturing of the graft. Donor graft suturing was done by 16 interrupted 10-0 nylon sutures.
Topical prednisolone 1% eye drops (started 4 hourly followed by stepwise tapering thereafter and continued at once a day dose after 6 weeks), topical antibiotics (tobramycin 0.3% 6 hourly for 6 weeks), and topical lubricant drops (carboxymethylcellulose 0.5% 6 hourly to be continued for 6 months) were administered to all patients. 0.5% loteprednol eye drops were used instead of 1% prednisolone eye drops in steroid responders. Follow-up was done on day 1, day 4, then weekly for a month, then monthly thereafter till 6 months. Loose sutures were removed during follow up as required. However, all sutures were removed by 6 months. Parameters at study visit at 6 months were used for data recording and analysis.
Statistical analysis
Continuous variables were presented as median and mean ± SD and categorical variables were presented in percentage (%) and number. Kolmogorov-Smirnov test was used to assess normality of the data. Nonparametric test was used if the normality was rejected. Independent t /Mann-Whitney Test was used for comparison of quantitative variables and pre and post BSCVA were compared using paired t test.
Correlation of various parameters with post-operative BSCVA was done using Spearman rank correlation coefficient. P value of <0.05 was taken statistically significant. Statistical Package for Social Sciences (SPSS) version 21.0 was used for data analysis.
Results
In this study, 25 eyes of 25 patients (15 eyes keratoconus, 10 eyes non keratoconus) undergoing DALK were evaluated. As none of the patients had any complications, so all 25 eyes were included in the analysis. Intermediate follow-up (2–4 months) was affected for three patients on account of COVID lockdown however all patients were evaluated as per the protocol at six months after undergoing surgery.
Table 1 summarizes the demographic characteristics of the study population. There was associated vernal keratoconjunctivitis in 5 eyes of 5 keratoconus patients. Seventeen patients (68%) underwent DALK with type 1 bubble formation, seven patients (28%) underwent layer by layer dissection and in 1 patient (4%) type 2 bubble was formed. Micro perforation of DM occurred in one case only, however did not need to be converted to PK. Type 1 bubble formed in 86% of keratoconus patients and in 40% of non keratoconus patients. Layer by layer dissection was done in remaining 14% of keratoconus and 50% of non keratoconus patients.
Characteristics of the study population.
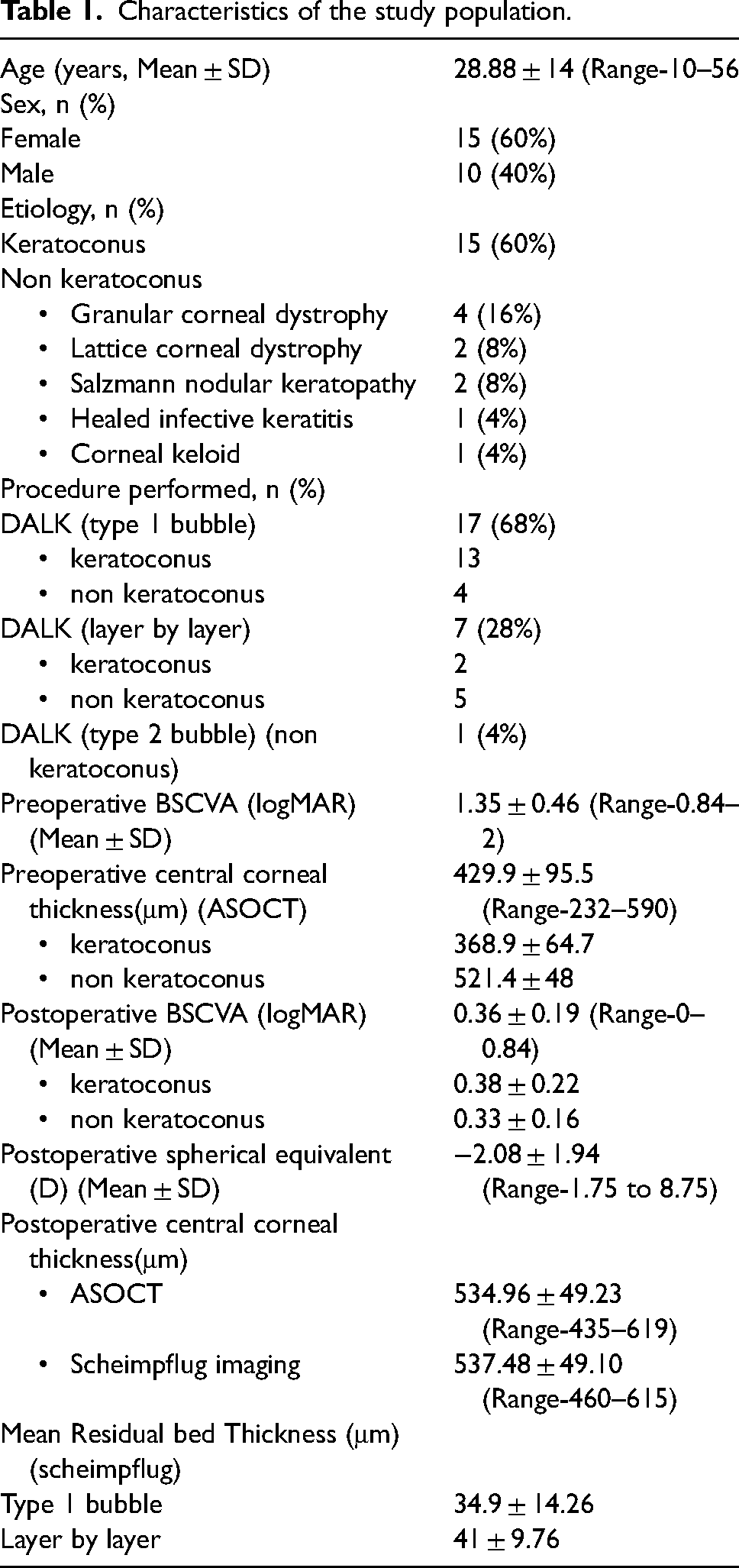
There was significant improvement in mean BSCVA from 1.35 ± 0.46 logMAR units (range 0.84–2 logMAR) pre-operatively to 0.36 ± 0.19 logMAR units (range 0–0.84 logMAR) 6 months postoperatively (p <0.001). Of all eyes, 16 (64%) achieved a BSCVA of 0.3 logMAR units or better. Four patients (16%) had BSCVA between 0.3–0.6 logMAR units. Five patients (20%) had a postoperative BCVA of 0.6 logMAR units or less. Of these one patient had dry ARMD, one patient developed steroid-induced glaucoma and had glaucomatous disc changes (had irregular follow up due to COVID-19 lockdown for 2 months) and one patient developed early nuclear cataract. Two patients belonged to non keratoconus group and one to keratoconus group. Remaining two patients had interface haze though grafts were transparent.
The BSCVA in 15 patients with keratoconus improved from 1.42 ± 0.47 logMAR units preoperatively to 0.38 ± 0.22 logMAR units (range 0.84–2 logMAR) postoperatively. While the BSCVA in non-keratoconus patients improved from 1.22 ± 0.43 logMAR units (range 0.602–2 logMAR) to 0.33 ± 0.16 logMAR units (0.176–0.602 logMAR) postoperatively. There was no significant difference in postoperative BSCVA between the two groups (p = 0.57).
Mean postoperative BSCVA in type 1 bubble DALK patients was 0.33 ± 0.2 logMAR units and in layer by layer was 0.4 ± 0.19 logMAR units. The single patient with type 2 bubble had postoperative BSCVA as 0.477 logMAR units. The difference in BSCVA between type 1 bubble and layer by layer dissection was not statistically significant (p = 0.38). Mean accepted spherical equivalent was −2.08 ± 1.94 D with a range of 1.75 to −8.75D.
The mean postoperative residual stromal bed thickness (RSBT) was 38.24 ± 15.36 μm (range10–80 μm) on Scheimpflug imaging and 32.76 ± 12.79 μm (range 18–60 μm) on ASOCT. As the difference between the two modalities was not significant statistically, the RSBT on scheimpflug imaging was considered for analysis. The mean RSBT in patients with type 1 bubble was 34.9 ± 14.26 μm, whereas in patients with layer by layer DALK was 41 ± 9.76 μm. There was no significant difference between the groups, but a trend towards lesser thickness in type 1 bubble group was observed (p = 0.25).
Table 2 shows postoperative total aberrations, LOA, and HOA (RMS) from front, back, and total cornea, 6 months post surgery. All aberrations were higher in study subjects compared to normative data (p < 0.001). Comparison of aberrations between type 1 bubble and layer by layer dissection patients showed higher value of all aberrations in layer by layer subpopulation, however the difference was not statistically significant. Table 3 shows comparison of aberrations between keratoconus and non-keratoconus group. A trend towards lower mean of all aberrations was seen in keratoconus patients than non keratoconus patients, however this was not significant statistically.
Comparison of aberrations of front, back and total cornea (RMS) between Type 1 bubble and Layer by Layer DALK.
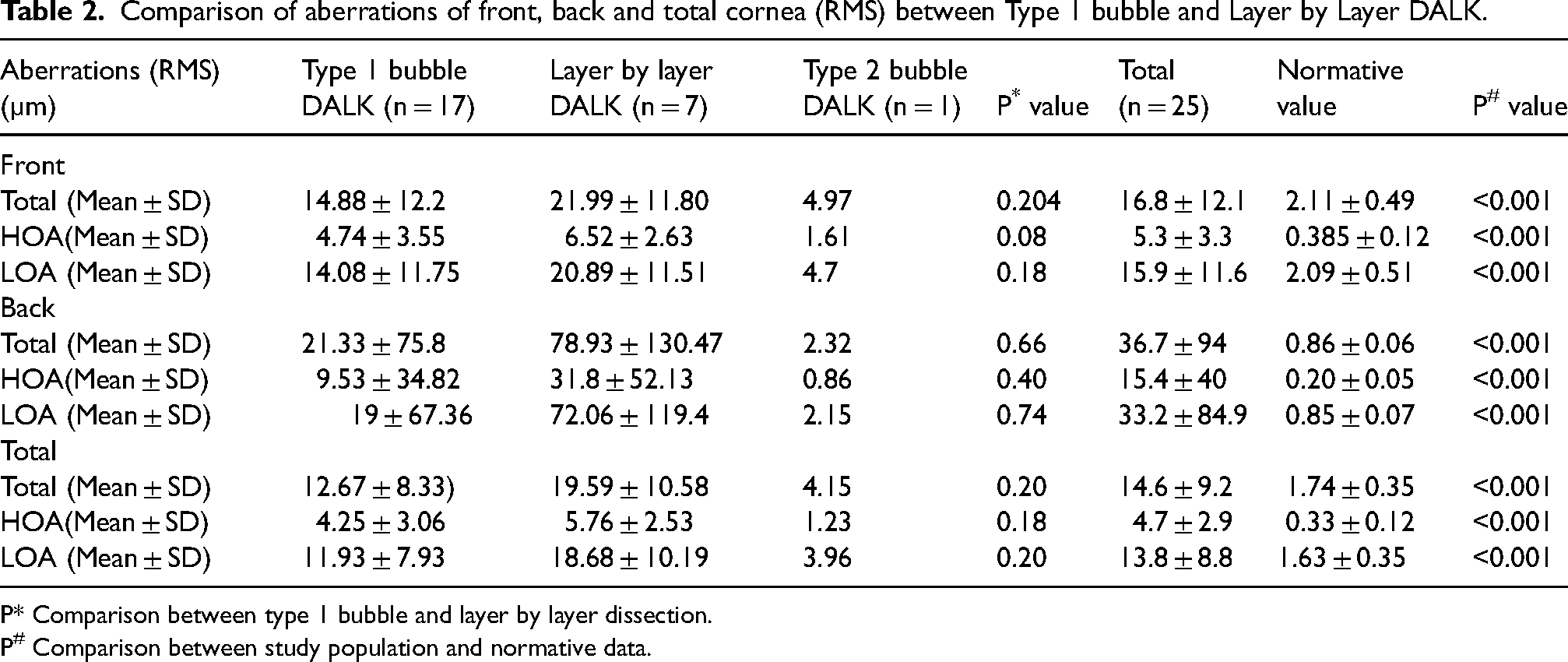
P* Comparison between type 1 bubble and layer by layer dissection.
P# Comparison between study population and normative data.
Comparison of aberrations of front, back and total cornea (RMS) between keratoconus and non keratoconus patients.
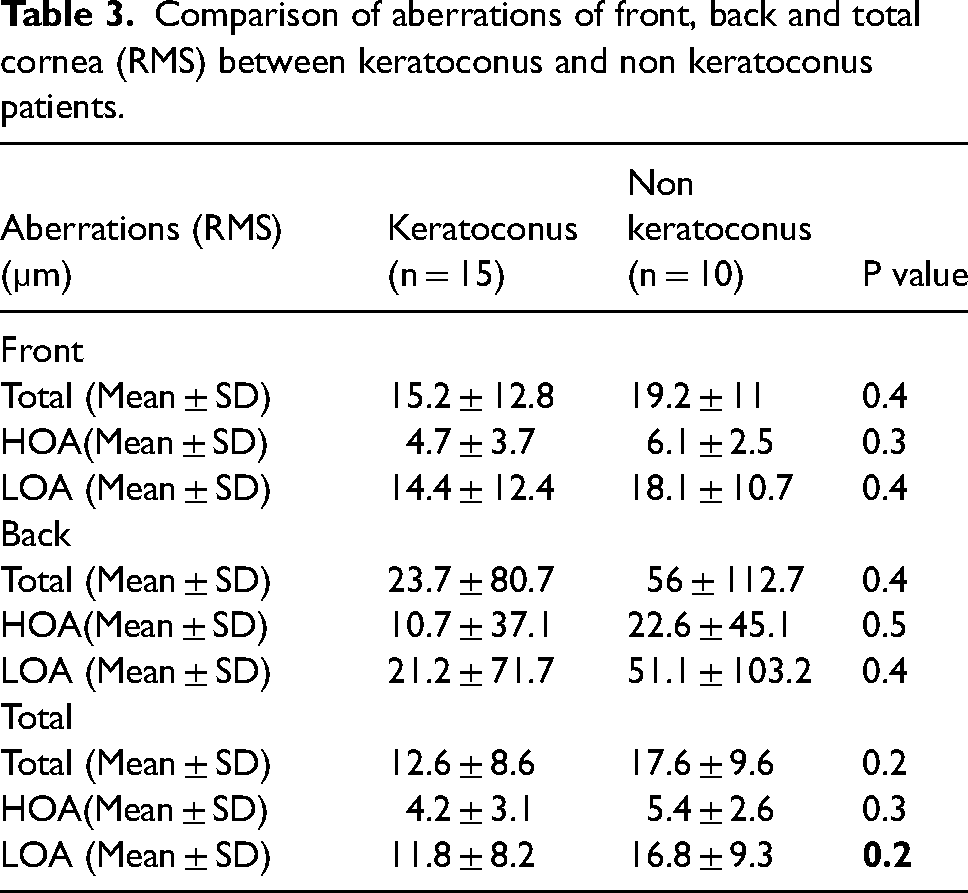
Table 4 shows the corneal densitometry output of zone 0 to 2mm of anterior, central, and posterior layers. On comparison of corneal densitometry in 0–2mm zone of type 1 bubble DALK and layer by layer DALK, the results in anterior and central layers were comparable though there was a trend towards lower densitometry in posterior cornea in type 1 bubble (9.1 ± 3.1 GSU) than layer by layer dissection group (11.7 ± 5.1 GSU) (Figure 1). Posterior densitometry values being very close to normative data in type 1 bubble cases with less variability [Coefficient of variation (CV) – 35] than cases done with layer by layer technique. (CV- 43.6). Densitometry in posterior cornea of patients with interface haze was 20.4 GSU and 16.7 GSU.
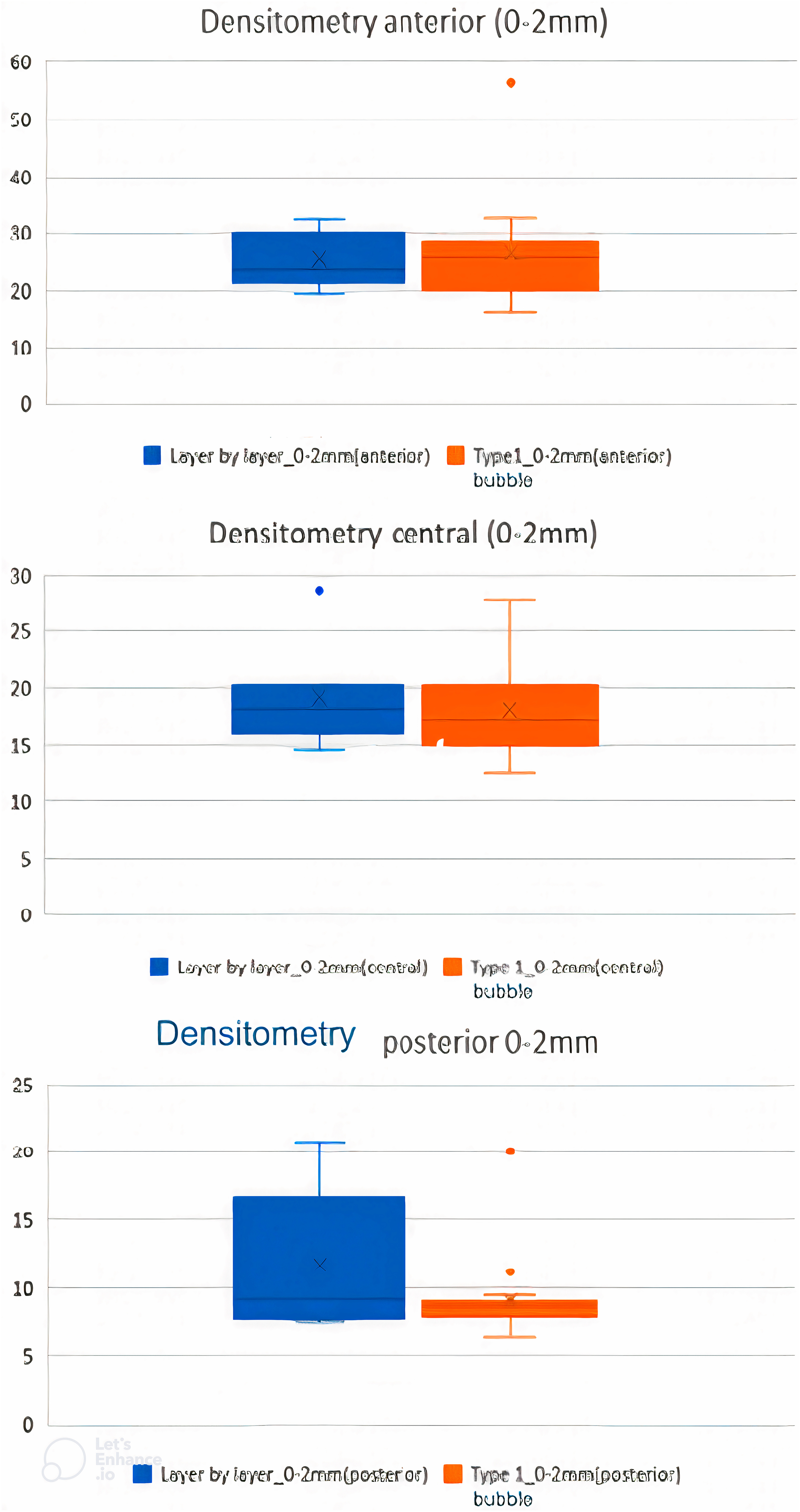
Comparison of densitometry (gray scale units) between type 1 bubble and layer by layer DALK.
Comparison of densitometry (gray scale units) between type 1 bubble and layer by layer DALK.
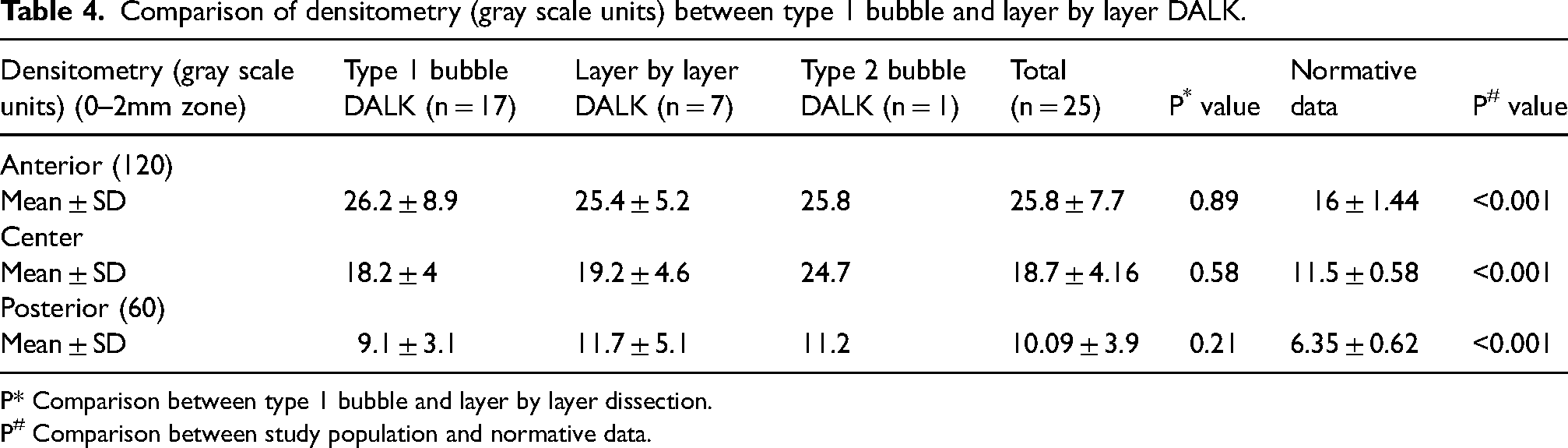
P* Comparison between type 1 bubble and layer by layer dissection.
P# Comparison between study population and normative data.
On comparison of densitometry output (0–2mm zone) between keratoconus and non-keratoconus groups a trend towards lower values in keratoconus patients in central (18.3 ± 3.2 vs19.2 ± 5.5 GSU) and posterior layers (9.1 ± 2.6 vs 11.5 ± 5.2GSU). Anterior densitometry values in keratoconus group (27 ± 9.2GSU) were higher than those in non-keratoconus group (24.2 ± 4.7GSU). Five patients in the keratoconus group also had associated vernal keratoconjunctivitis and had epithelial defects that persisted for 4 weeks and upon healing left faint epithelial scars which probably accounted for the higher anterior densitometry values.
Table 5 shows regression analysis of BSCVA with postoperative residual stromal bed thickness, wavefront aberrations, and densitometry data. There was a significant correlation of postoperative logMAR BSCVA with postoperative residual stromal bed thickness, total corneal HOA and LOA, HOA from anterior surface, and posterior corneal densitometry in 0–2mm zone. For this correlation analysis, three cases with clear grafts and other causes for subnormal vision were excluded.
Correlation of postoperative BSCVA at 6 months with various parameters. (Spearman rank correlation coefficient).
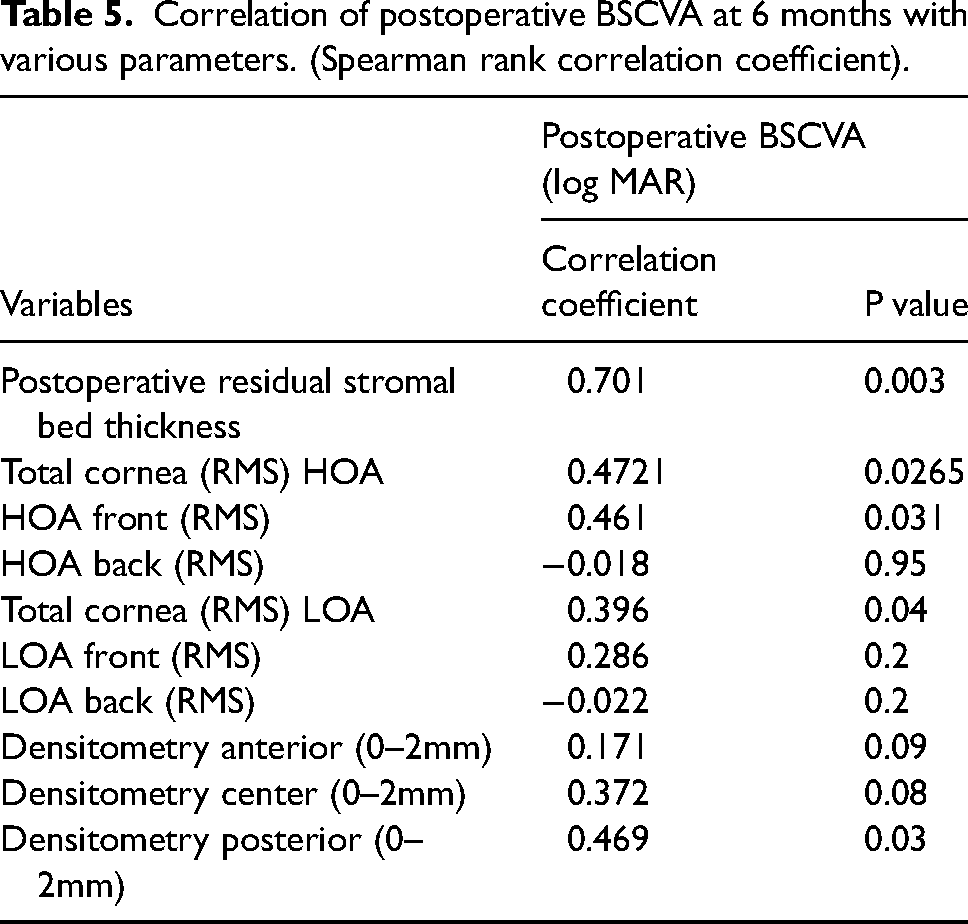
There was no significant correlation of HOA (back), LOA (front and back), and densitometry of the anterior and central layers with BSCVA.
Discussion
Visual outcome after DALK may be suboptimal despite clear cornea and transparent donor-recipient interface. This has reportedly been affected by multiple factors like irregular graft host interface, graft morphology, light scatter from interface and corneal aberrations. With improved image resolution using anterior segment imaging, various elements contributing to visual outcomes after DALK can be analyzed. The aim of this study was to analyze corneal aberrometry and densitometry influencing quality of vision after DALK performed for wide spectrum stromal diseases.
DALK has been found comparable to PKP for anterior corneal diseases in various studies done in the past.18,19 The improvement in postoperative BSCVA after DALK in keratoconus cases has been reported to be better than 6/12 in 70–80% of cases.20,21 In our study, however, BSCVA of 6/12 or better was achieved in 64% patients at 6 months. Vision was poor in three (12%) patients unrelated to corneal causes and two (8%) patients had poor vision due to interface haze. Since varied etiological cases were taken for DALK, mean BSCVA better than 6/12 was achieved in only 64% cases. However, no significant difference was seen in mean BSCVA between keratoconus and non-keratoconus etiologies. Also, technique of DALK did not significantly impact the BSCVA (type 1 BB and manual dissection). Similar results have also been reported in earlier studies.22,23
Previously HOAs from anterior cornea, interface and posterior cornea have been studied post DALK. Javadi et al. 11 compared DALK and PKP and commented that DALK and PKP eyes have similar HOAs. Suzuki et al. 16 in 2019 found significant correlation of visual acuity at 12 months after DALK with HOAs from anterior corneal surface and total cornea but not posterior cornea. Other studies have also found no significant correlation of postoperative BSCVA with HOAs post DALK. 15 This has been explained by the fact that variation in HOA magnitude and interface haze less likely affects high luminance, high contrast visual acuity. In a study using adaptive optics, Pantanelli et al 24 showed improvements in visual acuity and contrast sensitivity after correcting HOAs post DALK proving the role of HOAs as a limiting factor for vision post DALK. HOAs in our study were found to be higher in operated DALK patients than age-matched normal population. Presence of irregularities at the level of epithelium (post healed epithelial defect), stroma, and interface probably accounted for this finding. We found significant correlation of anterior HOA and total corneal HOA and LOA with postoperative BSCVA.
Corneal wavefront aberrations were also compared between type 1 bubble DALK and layer by layer dissection DALK and found trend of all aberrations to be lower in type 1 bubble DALK compared to layer by layer, particularly the posterior corneal aberrations. The difference, however was not significant statistically. The trend of lower posterior aberrations in type 1 bubble DALK can be explained by smoother interface in Type 1 bubble than in layer by layer DALK. No studies related to comparing the aberrations between the two techniques of DALK exist. Also there was a trend towards lower aberrations especially from the posterior surface in keratoconus group than in non-keratoconus group. Higher cases had successful type 1 bubble in keratoconus group.
Corneal densitometry at 6 months post DALK in the study was also compared to normative database and found to be significantly higher. When divided by layer, only anterior 120 μm showed the maximum backscatter, with the minimum backscatter at the posterior 60 μm, possibly because of epithelial haze and epithelial-stromal irregularities occurring post healing of epithelial defects (postoperative complication seen in many patients). However, there was an inverse correlation of posterior densitometry in the 0–2mm zone with postoperative BSCVA implying the importance of a smooth and regular posterior surface.
We found limited studies analyzing the corneal densitometry and its correlation with BSCVA. Alzahrani et al in 2017 25 compared DALK and PKP using corneal densitometry as a parameter measured by Oculus Pentacam and found significantly higher corneal densitometry after DALK compared to PKP. Also, postoperative BCVA significantly correlated with corneal densitometry in DALK. In 2019, Scorcia et al 26 compared the visual outcomes and corneal densitometry in keratoconus patients who underwent visco-bubble (VB-DALK) deep anterior lamellar keratoplasty and big-bubble (BB-DALK). A significantly high densitometry was seen in the VB-DALK group in the first 3 months (23.97 ± 5.34 vs 17.13 ± 4.44 grayscale units), but no significant difference was seen at 1 year. In the current study, on comparing the densitometry in 0–2mm zone of type 1 bubble DALK and layer by layer DALK cases, the mean results were comparable with a mild increase in corneal densitometry in posterior cornea in layer by layer dissection group. However, the variability in densitometry from posterior cornea was far more in manual DALK than that in type 1 bubble cases highlighting the importance of precision and repeatability in type 1 BB cases.
The residual stromal bed in DALK has an effect on the postoperative visual and optical quality. 11 Residual stromal bed thickness measured by ASOCT and Scheimpflug were similar, although interface delineation was better with scheimpflug imaging. We found a significant inverse correlation of postoperative residual stromal bed thickness with postoperative BSCVA, i.e. lesser the thickness, better the visual acuity. This was in agreement with Arjomond et al 13 who found that visual acuity was similar to PKP in eyes with recipient bed thickness <20 μm but was significantly reduced with recipient bed thickness >80 μm. Knuttson et al 27 in a study in 2015 compared modified big bubble DALK and manual dissection DALK for keratoconus and found that stromal residue was not measurable in patients with big-bubble DALK, whereas mean residual stromal thickness in manual DALK group was 30.50 ± 27.60 μm. They showed a significant correlation of BSCVA with residual stromal thickness with lesser residual stromal thickness correlating with better BSCVA.
To the best of our knowledge, the detailed study of corneal aberrometry and densitometry using Scheimpflug imaging software and its correlation with postoperative BCVA in eyes undergoing DALK for varied etiologies has not been done in a prospective manner. Also, a comparison of BB-DALK versus layer by layer dissection has not been done for cases of variable etiologies. In conclusion, both corneal aberrometry changes and densitometry measurements showed a trend towards a negative impact on BSCVA post DALK. Further, a trend of lower aberrations and densitometry from the posterior corneal surface in cases with type 1 BB compared to manual layer by layer technique is observed. The major limitation of this study being a small sample size and short follow-up time. Small sample size was mainly due to the study being carried during COVID pandemic. A similar study with a larger sample size of patients with varied etiologies undergoing DALK and followed over a long period would give more definitive results.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.