
Abstract
Background
To evaluate the functional development and, retinal and optic disc morphology using OCT in patients with septo-optic dysplasia (SOD).
Methods
This retrospective case series included patients diagnosed with SOD between 2007 and 2020. Ophthalmologic assessment included visual acuity (VA) and funduscopy at the initial and last presentation. Retinal imaging included OCT of the macula analyzing the retinal morphology, central retinal thickness volume (CRT) and ganglion cell layer (GCL). Also, scans of the optic nerve head were taken to evaluate the retinal nerve fiber layer (RNFL) and global value.
Results
38 eyes of 19 children with a mean age 6.3 ± 5.3 years were included. 31.6% showed all 3 characteristics of SOD, whereof ONH, midline defects and endocrine dysfunctions were found in 94.7%, 89.5% and 47.4% respectively. The mean VA was 0.70 ± 0.66logMar in the right eye (RE) and 0.40 ± 0.55logMar in the left eye (LE) at the initial presentation. No change of vision (RE: 0.69 ± 0.71logMar; LE: 0.31 ± 0.57logMar) was found after a follow-up period of 6.3 ± 4.5years. Funduscopy showed an ONH in 79% (n = 30/38), tortuous retinal vessels in 36.8% (n = 14/38) and a double-ring sign in 15.8% (n = 6/38). Retinal imaging showed variable morphology. 6 eyes of 4 patients showed temporal retinal thinning with corresponding GCL attenuation. The optic nerve head appearance varied between no changes, sectoral and hemispherical reduction.
Conclusions
Patients suffering from SOD show diverse expression of retinal changes such as retinal, GCL and RNFL thinning in OCT. Furthermore, visual function remained stable during follow-up examinations, indicating no further alteration due to underlying pathology.
Introduction
The septo-optic dysplasia (SOD), which was first described in 1956 by the French-swiss neurologist Georges de Morsier, is a congenital disease comprising of mid-line brain malformations. 1 This disease complex shows a high heterogeneity in structural abnormalities of the cortex. The main diagnostic criteria include optic nerve hypoplasia, agenesis of midline structures such as absence of the septum pellucidum, or hypoplasia or absence of the corpus callosum, and hypoplasia of the hypothalamic-pituitary hormonal axis, whereof at least two of the above mentioned have to be present.2,3
The SOD is a rare disease with a prevalence ranging from 1.9 to 2.5 per 100,000 births in Europe and therefore, belongs to the orphan diseases. 4 Patients generally present with ophthalmologic symptoms such as nystagmus, strabismus or decreased visual acuity next to neurological symptoms such as seizures, cerebral palsy or developmental delay, or symptoms due to hypopituitarism in form of growth hormone deficiency, hypothyroidism or diabetes insipidus. 3 But also anosmia, hearing loss or heart anomalies have been described.5,6 Therefore, also the phenotype of SOD is highly variable. 7
Several studies analyzed the clinical expression patterns and found that about 30–47% of the patients with SOD show a full expression of all three cortical abnormalities.2,8,9 A study by Atapattu et al. found that 24% of patients presented with full expression, whereas 66% showed an endocrinological deficit and about 95% showed optic nerve hypoplasia. 8 Subsequently, the ophthalmologic, neurologic and endocrine deficits can range from minimal changes to severe mental retardation or blindness. 9
The optic nerve hypoplasia (ONH), one of the main diagnostic criteria in SOD, is found in up to 90% of all patients. 5 For reasons not yet known, apoptosis of retinal ganglion cells occurs during pregnancy, resulting in an excessive thinning of the optic nerve fibers. 3 The ONH can develop uni- or bilateral.10,11 Next to the ONH, other changes such as a “double-ring sign”, vascular tortuosity and reduced vessel branching can be found.12,13 Initially, however, many patients present to the ophthalmology due to nystagmus or strabismus, which is found in 33% and 14%, respectively.14,15 In recent years, morphologic changes of ONH were examined in more detail using the non-invasive optical coherence tomography (OCT). Several studies showed thinning of retinal layers such as the ganglion cell layer (GCL) and retinal nerve fiber layer (RNFL) in patients with ONH.16,17 Furthermore, foveal abnormalities in form of foveal hypoplasia were found in up to 24% of patients with ONH. 17
As ONH in general is a rare disease, most studies analyzed the morphological changes of ONH in different underlying pathologies. We aimed to assess the morphological changes of the macula and optic disc using OCT and fundus photography in patients with ONH solely due to SOD. Furthermore, we evaluate the ophthalmologic clinical characteristics and the functional development of SOD patients at our clinic.
Methods
This retrospective, case series included patients with septo-optic dysplasia who were examined at the Department of Ophthalmology, Medical University of Vienna between 2007 and 2019. Approval of the local ethics committee (EK: 1328/2019) was obtained and the study adhered to the tenets of the Declaration of Helsinki.
In our study we defined the septo-optic dysplasia if two of the main criteria were present:
presence of hypoplasia/agenesis of the optic nerve midline defects of the brain such as absence of the septum pellucidum, or hypoplasia/ agenesis of the corpus callosum disorders involving the pituitary-hypothalamic hormonal axis
Diagnosis was confirmed via neuroimaging, which was performed in all patients. Therefore, patients with isolated midline defects, isolated ONH or isolated hypo-physical-hypothalamic dysfunctions were not included in the study.
The medical records were examined for general data on age, gender, birth and pregnancy abnormalities or seizures. The other outcome measures were divided into ophthalmologic, endocrine and radiologic characteristics.
The ophthalmologic characteristics comprised of visual acuity (VA) at the initial and last presentation, presence and type of nystagmus and strabismus and eye motility. Eye examination of the posterior segment examined typical morphologic abnormalities of the optic disc and retinal vessels.
Retinal imaging included OCT and fundus photography, which were performed in patients with visual acuity better than 1.0 log MAR and only mild nystagmus. The images were used to assess structural changes in the macula, optic nerve head and retinal vessels. For OCT scans, a Heidelberg Spectralis OCT® (Heidelberg Engineering, Dossenheim, Germany) was used, whereas for wide field fundus photography an Optos Optomap (Optomap P200; Optos plc, Dunfermline, UK). OCT scans of the macula were analyzed regarding central retinal thickness and volume as well as the thickness and volume of the ganglion cell layer. Furthermore, foveal hypoplasia was evaluated using the structural grading classification published by Thomas et al. 18 The retinal nerve fiber layer (RNFL) and global value of the optic nerve head on OCT scans was analyzed as well as the pattern of RNFL reduction.
The endocrine characteristics included the presence and type of dysfunction, whereas the neuro-radiologic characteristics comprised of structural abnormalities of the optic nerve, chiasma, septum pellucidum, corpus callosum and the pituitary glands.
Statistical analysis
Microsoft Excel ® 2010 was used for collecting patients’ data, which was then converted to SPSS ® version 20 (SPSS, Inc., Chicago, IL) for statistical analysis. Nominal data is given as numbers or percentages, whereas continuous data is given as means ± standard deviations (SDs). Following Kolmogorov-Smirnov test, no normal distribution of the vision data was found. Therefore, Wilcoxon signed rank test was performed to analyze the change of vision between initial and last visit.
Results
This study included 19 children, 12 male and 7 female. The mean age, when patients initially presented at the eye clinic, was 6.3 ± 5.3 years (range 0–18 years). Almost a third of the patients (n = 6/19; 31.6%) showed all three main characteristics of SOD. OHN was found in 94.7% of children (n = 18/19), whereas midline defects were seen in 89.5% (n = 17/19) and endocrine dysfunctions in 47.4% (n = 9/19).
The circumstances of birth and pregnancy are known in only 12 of the 19 children. 41.2% of children (n = 5/12) were born at the expected date, whereas 25.0% of the children premature (n = 3/12). The age of the mothers at birth ranged between 18 and 40 years. Patients’ records showed several maternal diseases such as obesity (BMI > 38), congenital CMV infection, fetal alcohol syndrome or drug abuse (opiates: positive).
Evaluation of the neonatal examinations showed that 47.4% of the children (n = 9/19) presented with abnormalities shortly after birth. Two children had hypoglycemia which resulted in severe seizures, whereas two showed jaundice. One baby presented with a respiratory distress syndrome, whereas another with severe asphyxia at birth. Also several dysmorphic facial features (n = 4) such as retrognathia (n = 1/4), dysmorphic ears (n = 2/4), dolichocephaly (n = 1/4), missing distal phalanx of two fingers (1/4) or dysmorphic philtrum (n = 2/4) were found.
Endocrine and radiologic abnormalities
Hormonal changes were found in almost half of the children (n = 9/19; 47.4%).The main dysfunctions were found within the growth (n = 7/19; 36.8%) and thyroid (n = 7/19; 36.8%) hormonal axis, followed by deficiencies of the adrenocorticotropic (ACTH) in 26.3% (n = 5/19), prolactin in 10.5% (n = 2/19) and vasopressin hormones in 5.3% (n = 1/19). The expression of the hormonal changes was highly variable. 7 children had multiple hormonal deficiencies (two dysfunctions: n = 2; three dysfunctions: n = 4; four dysfunctions: n = 1), whereof both growth and thyroid hormonal was affected in 6 children.
The primary radiologic findings were abnormalities of the midline in 89.7% (n = 17/19) whereof the corpus callosum was mainly affected in 73.7% (n = 14/19) followed by the septum pellucidum in 42% (n = 8/19). A hypoplasia of the optic chiasm was seen in 47.3% (n = 9/19), whereas the pituitary gland in 36.8% (n = 7/19).
Cortical malformations were found in 21.1%, whereof 2 patients each had either a schizencephaly or a polymicrogyria. Furthermore, other changes such as hydrocephalus (n = 3/7), ventriculomegaly (n = 2/7), arachnoid cyst (n = 1/7) or aplasia of the fornix (n = 1/7) were found. And at least one episode of epileptic seizures was reported in 31.6% of the children (n = 6/19), whereas one child received VP-shunt during the observational period.
Ophthalmologic abnormalities
A hypoplasia of the optic nerve was the main finding in all children (n = 18/19), whereof bilateral in 88.9% (n = 16/18). Further ophthalmologic findings included strabismus in 73.7% (n = 14/19), which mainly presented as an exotropia (n = 8). Nystagmus was seen in 53.0% (n = 10/19). Motility was impaired in 21.1% of patients (n = 4/19), in which the both horizontal eye movements were affected likewise (abduction: n = 2; adduction: n = 2). Squint surgery was performed in 8 patients one to 14 years after the initial presentation. In all cases, surgery was performed to reduce ocular torticollis and strabismus but not nystagmus. One to seven years after the initial surgery, squint surgery was repeated to treat inferior oblique overaction in two patients, whereas in one case squint surgery was repeated to treat persistent esotropia.
The mean visual acuity of the patients was 0.70 ± 0.66 logMar in the right eye and 0.40 ± 0.55 logMar in the left eye at the initial presentation. Occlusion therapy was performed in seven children, whereas early supportive visual therapy was provided in eight cases. At the last follow-up visit at the age of 12.3 ± 9.0 years, the functional outcome had remained almost unchanged. The right eye had a vision of 0.69 ± 0.71 logMar (p > 0.05) and the left eye of 0.31 ± 0.57 logMar (p > 0.05). In six children functional assessment was not possible due to severe neurologic impairment at either visit. (See Figure 1 shows the functional development)
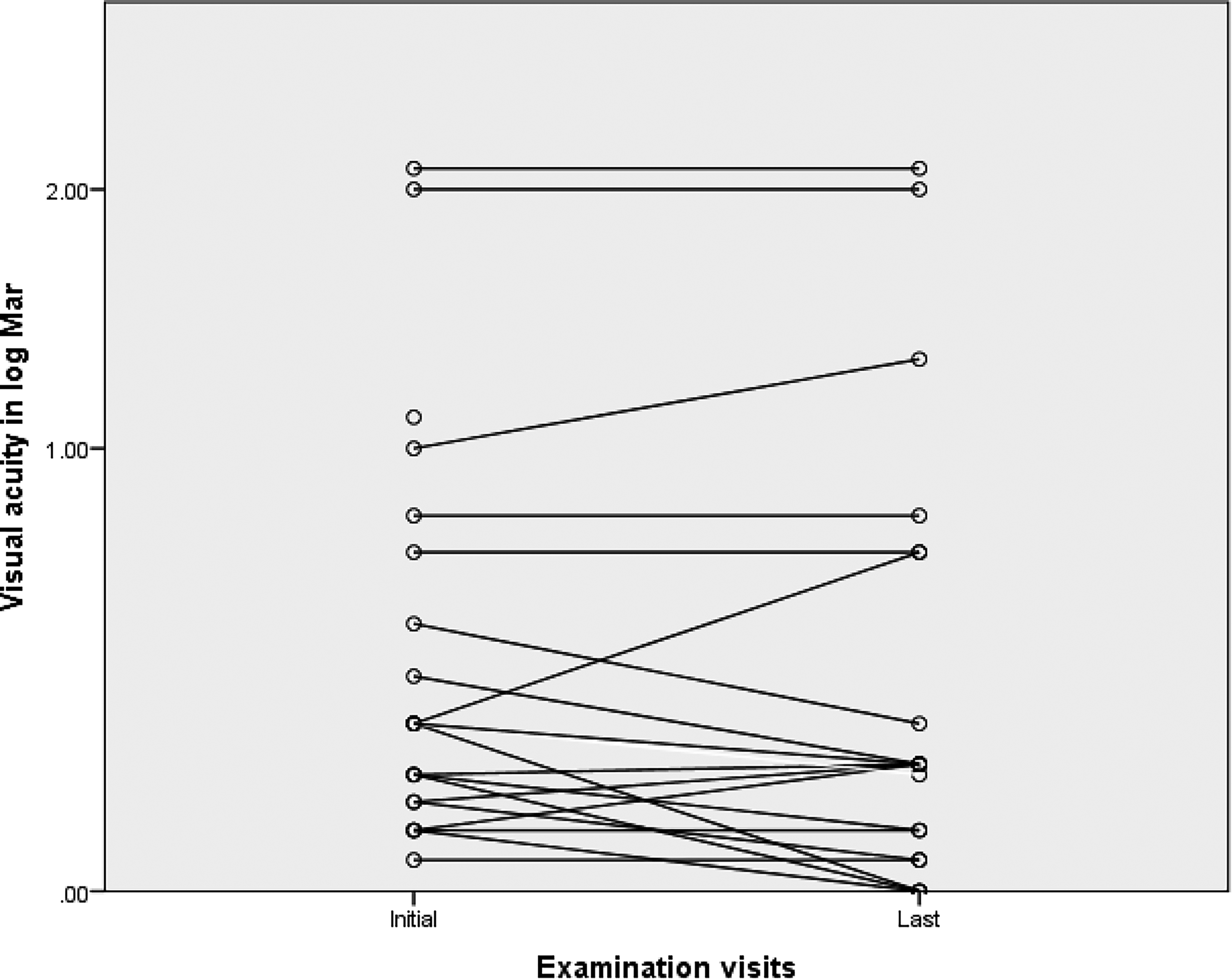
Development of visual acuity of both eyes in patient with SOD. Interpolation line connecting the vision of the initial (age: 6.3 ± 5.3 years) and last visit (age: 12.3 ± 9.0 years). Visual acuity in Log Mar is presented on a logarithmic scale with base 2.
Clinical fundus examination showed tortuous retinal vessels in 36.8% of eyes (n = 14/38). A hypoplasia of the optic nerve head was found in 79% of eyes (n = 30/38), whereas the typical double-ring sign was seen in 15.8% of the eyes (n = 6/38). Also, retinal pigment epithelium irregularities were seen in 13.1% of eyes (n = 5/38).
Retinal imaging was performed in 6 patients, whereof in 4 eyes of three patients image quality of the OCT scans was very low and therefore, not included for analysis. Therefore, retinal imaging was possible in 8 eyes of five patients.
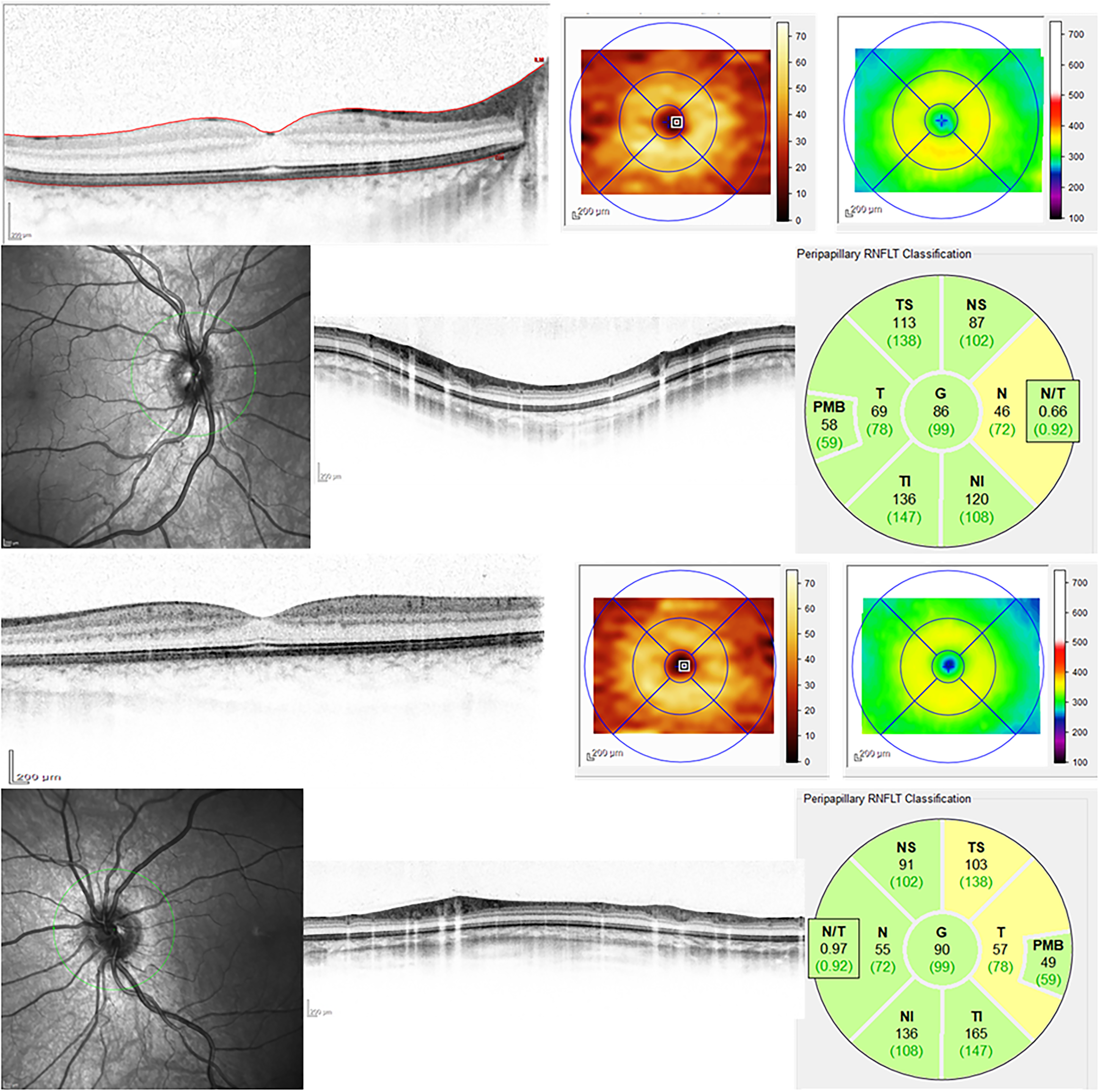
The expression of retinal and optic nerve head changes was highly variable (see Table 1). However, tortuous retinal vessels seen on fundus examination could be found on fundus photography (see Figure 2) as well as infrared imaging. On retinal OCT scans, abnormal foveal depression in form of foveal hypoplasia was visible in both eyes of 2 patients. Temporal retinal thinning was seen in six eyes of four patients on macula scans, which was also seen in the GCL of patient 1 (Figure 3). But, although temporal thinning in the macula scan was seen in patient 4 (Figure 5), the GCL showed total reduction in the RE with corresponding VA decrease and no reduction in the LE with normal vision. On the contrary, patient 2 with normal VA did not show changes in CRT and GCL (Figure 4).
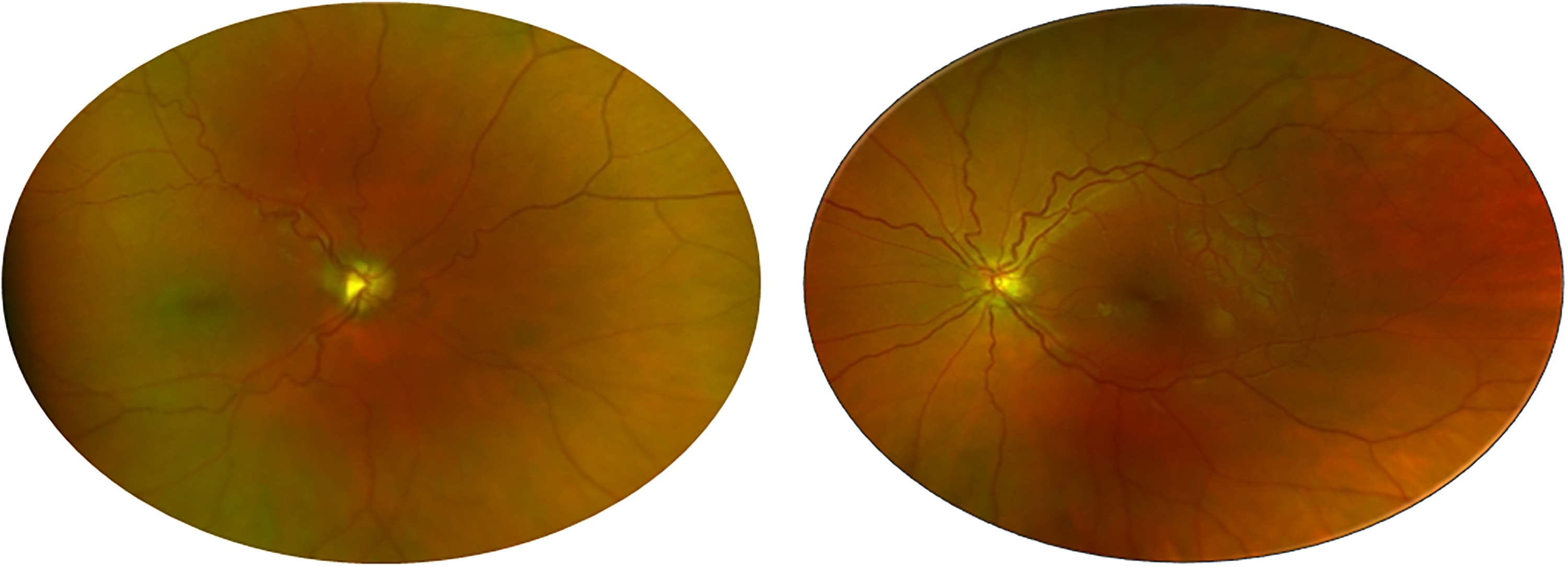
Shows fundus images of both eyes of patient 3, a 21-year old female, with a vision 1.30 log Mar in the right eye (Snellen equivalent: 0.05) and 0.05 log Mar in the left eye (Snellen equivalent: 0.9). This patient presented with an ONH and hormonal changes, radiologic examination did not show any midline abnormalities. Eye examination showed an exotropia and nystagmus, whereas no motility deficiency. Funduscopy showed a pronounced hypoplasia in the right eye, whereas only minimal in the left eye.
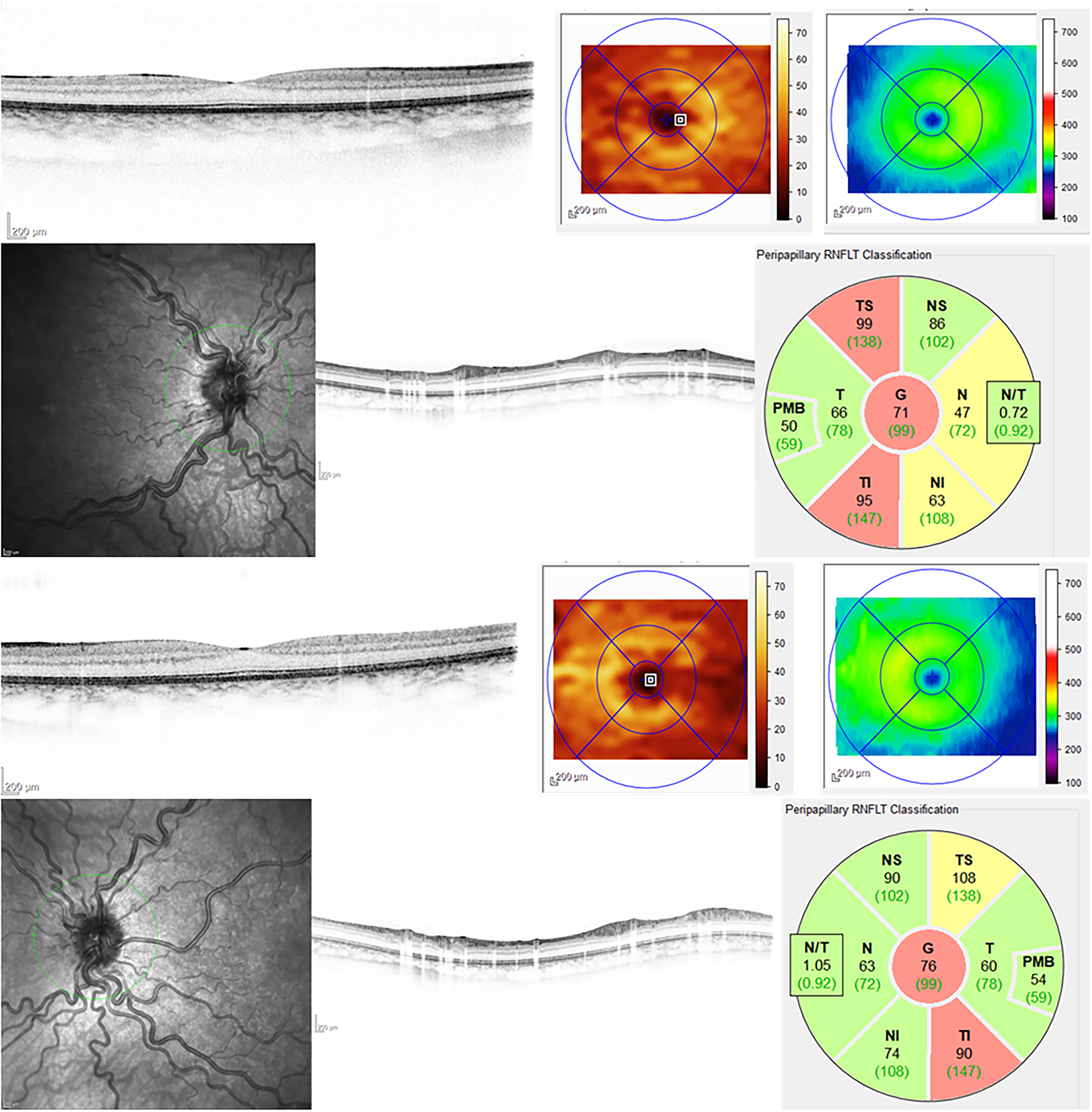
Shows patient 1, eight-year old male child with vision 0.0 log Mar (Snellen equivalent: 1.0) in both eyes. On radiologic imaging an ONH and midline abnormalities were found but no endocrine deficiency was found. On eye examination, no strabismus or nystagmus was seen in this case as well as no sign of motility deficiency. On fundus examination, no optic nerve head hypoplasia was found but pronounced vessel tortuousity in both eyes. On OCT imaging, the retina shows a normal foveal depression, but the temporal retina appears thinned. This impression was also found on examination of GCL, where a temporal atrophy was seen. Optic disc imaging shows decrease of the peri-papillary RNFL predominantly in the temporal inferior and superior segment.
Shows patient 2, an eleven year old male child, with a vision of 0.1 log Mar in the right (Snellen equivalent: 0.8) and 0.0 log Mar in the left eye (Snellen equivalent: 1.0). Radiologic findings included all three main characteristics of SOD: ONH, midline abnormalities and hormonal changes. In this case also, no strabismus, nystagmus or motility deficiency was seen. Fundus examination showed no hypoplasia of the optic disc or tortuous retinal vessels. On retinal OCT imaging, a normal foveal depression was found. Also GCL layer segmentation did not show any pathologic changes. Only minor changes of the optic nerve head can be seen.
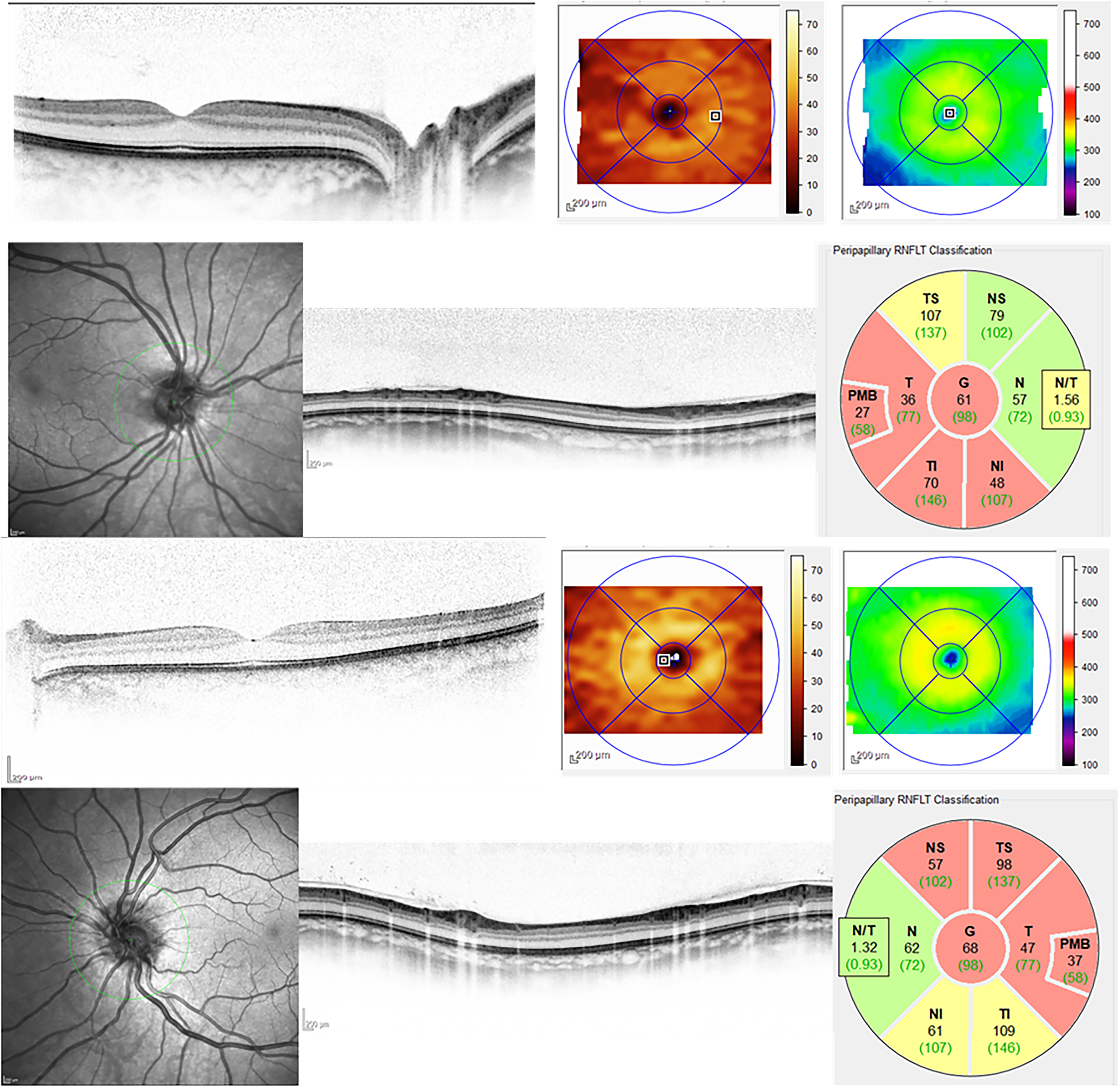
Shows patient 4, a 26-year old female, with a visual acuity of 0.7log Mar in the right eye (Snellen equivalent: 0.2) and of 0.22 log Mar in the left eye (Snellen equivalent: 0.6). She presented with two of the main criteria: ONH and midline abnormalities. On orthoptic examination, the patient had an exotropia and a nystagmus. The motility did not show any impairment. On fundus examination a hypoplasia of the optic nerve head was found but not tortuous retinal vessels. OCT scans of the macula show a temporal thinning in the right eye and a global reduction of the GCL, whereas in the left eye normal retinal and GCL were found. But, the optic nerve head show extensive RNFL damage and on the infra-red image a sunken, almost vanishing optic nerve head is seen.
Imaging results of the macula and optic nerve head using OCT in patients with septo-optic dysplasia.
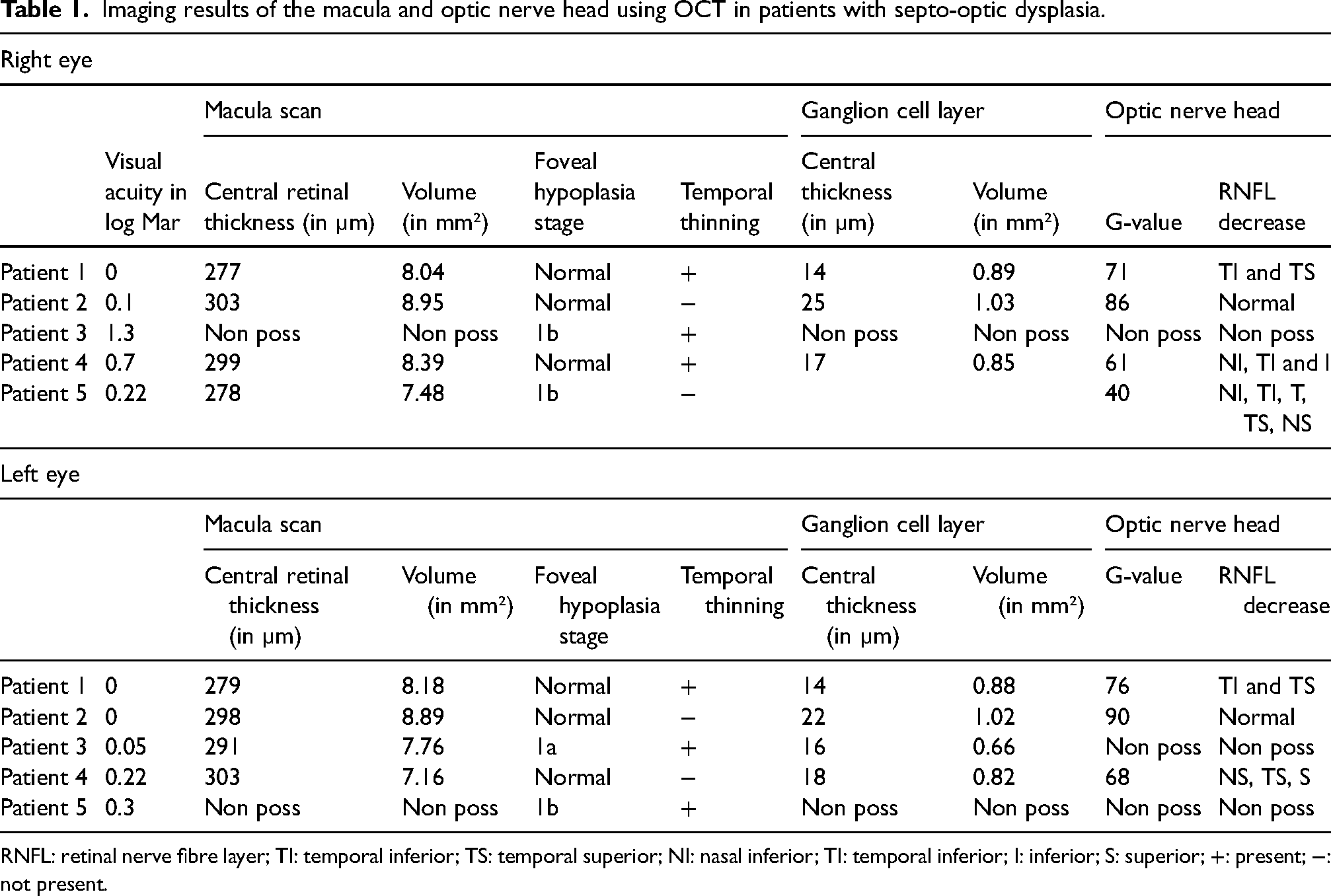
RNFL: retinal nerve fibre layer; TI: temporal inferior; TS: temporal superior; NI: nasal inferior; TI: temporal inferior; I: inferior; S: superior; +: present; −: not present.
Also the appearance of the optic nerve head varied to a surprising degree. The global value of the retinal nerve fiber layer (RNFL) ranged between 40 to 90%. One patient showed hardly any change of the RNFL (patient 2 of Figure 4), whereas one patient sectoral changes (patient 1 of Figure 3) and in another patient a hemispherical reduction were found (patient 4 of Figure 5).
Discussion
Several studies analyzing morphologic changes of the macula and the optic nerve head in patients with ONH found retinal thinning of the GCL and the RNFL.16,17 SOD shows a high variability not only in structural abnormalities but also the clinical expression. Therefore, presence or absence of ONH in these patients can result in different morphologic changes on OCT. In this case series, we examined patients with ONH due to septo-optic dysplasia only and present volumetric results of the macula and optic nerve head using OCT
About a third of our patients showed the full classic triad of SOD, comprising of ONH, midline defects and endocrine dysfunctions, which is comparable to results from literature.2,8 The main abnormality, ONH, was found in 94.7% of patients, followed by midline defects in up to 89.5% and endocrine deficits in 47.4%. In general, endocrine deficits are reported more frequently (70% to 90%) than midline defects (43% to 74%). The given percentages, however, indicate the variability of SOD.5,8,19,20
Also, the extent of the endocrine deficits varies greatly. While some patients have no or only isolated hormonal deficits, others show a severe degree of pan-hypopituitarism. In our study, the two most important hormone deficiencies, growth and thyroid dysfunction, were found in more than one third of the patients, which is in line with previous studies.14,19
Interestingly, the main midline defects found in our study population were abnormalities of the corpus callosum in 73.7% followed by septum pellucidum in 42%. In literature, however, the main affected area is the septum pellucidum in up to 60% followed by a dyplastic corpus callosum in only 11% to 50%.5,20–22 This might be another example of the high variability of SOD.
In 2000, Miller et al. introduced the term SOD plus, which, next to the classic triad of SOD, includes additional cortical malformations in form of schizencephaly and polymicrogyria. 23 In our study we observed such malformations in 21.1%, which shows that cortical malformations are common in SOD and should, therefore, be included in the classification.
In literature, two presenting ophthalmic symptoms prompting a referral to an eye specialist center are strabismus and nystagmus, which are found in up to 14% and 47% in literature, respectively.14,20 Both features represent abnormal findings and as a result, dilated fundus examination is obligatory, where other clinical features of SOD such as vessel tortuosity, reduced vessel branching, or ONH can be found. In our case series, strabismus (73.7%) and nystagmus (53.0%) were found more commonly than compared to literature, which can be related to the high degree of bilateral ONH causing more severe visual impairment. ONH was found in almost 95% of patients, whereof bilateral in 88.9% in our series.
To our knowledge, this is the first study to present visual function over time in patients with SOD. When evaluating the visual development, VA ranged between 0 logMar (Snellen equivalent: 1.0) and amaurosis but stable functional outcome was found during a 6.3 ± 4.5 year follow-up period. Occlusion therapy was performed in seven children who did not show severe bilateral ONH resulting in amaurosis at the initial presentation. Most of the patients had unchanged results or a change of one line. A greater visual improvement of two and three lines was seen in five eyes of four patients, whereas a reduction of three lines in one eye of one patient. Thus showing, that vision is affected by the underlying disease but does not alter with age. Therefore, parents with SOD children can be reassured that vision will not decline over time and occlusion therapy has some beneficial effects on vision in selected cases.
Previous studies using OCT examining ONH patients showed significant thinning of the retina in general and, the GCL and RNFL in particular, which we also saw in our study population.16,17,24 SOD patients showed various morphologic manifestations, but specific patterns could not be identified. In general, a global retinal thinning was observed in study population, except patient 2, who despite having all three SOD characteristics, showed normal retinal morphology and visual acuity. Next to retinal thinning, pronounced temporal atrophy of the retina was found, which was also evident in the ganglion cell layer. Another interesting finding was seen in patient 4, who had a mixed expression in between both eyes. In one eye, normal vision and subsequently minimal retinal and GCL thinning was observed, whereas the second eye showed decreased vision with retinal and pronounced GCL atrophy. Also, RNFL analysis showed different patterns ranging from minimal thinning to hemispherical reduction. Our study results confirm that ONH due to SOD shows a high variability.
One of the main weaknesses of the study is that OCT scans of only eight patients were available and images of three patients had to be excluded due to low image quality. Furthermore, morphological assessment via OCT was not possible in eight patients due to severe neurologic and visual impairment, and nystagmus which significantly reduced the ability to fixate of the patients. Therefore, results of patients with extensive visual impairment or nystagmus were not included to the case series. Furthermore, as imaging analysis of 5 patients already showed a high variability of retinal morphology, further studies with higher number of SOD patients are required to provide a greater insight in morphologic changes of the retina and allow classification of expression patterns corresponding to the visual function. For example, hand-held OCT offers the possibility to examine patients with nystagmus or severe visual impairment during examinations under general anesthesia, and to allow more detailed assessment of morphology in these patients.
Another shortcoming of this study is the retrospective design. Data on pregnancy, maternal diseases and age, are incomplete. We can only provide marginal insight, although young maternal age is discussed as an important risk factor for SOD.25,26 But we can provide insight on prenatal situation, where abnormalities after birth were found in 47.4%. Several studies showed that hypoglycemic events or hyperbilirubinemia are common in SOD children soon after birth, which we also observed in 21.1% of our children.2,20 Furthermore, we observed several dysmorphic facial features such as dental, ear or lip abnormalities. Dysmorphia has been more commonly reported in literature during the last decades.27,28 Therefore, postnatal abnormalities or dysmorphia should raise awareness for further investigation of underlying causes including SOD.
One of the take home messages is that septo-optic dysplasia is a rare condition, which is often difficult to diagnose given the considerable heterogeneity and clinical variability. However, children with nystagmus and strabismus present early in life. A comprehensive ophthalmic assessment including dilated fundus examination is performed which may then reveal clinical features such as optic nerve hypoplasia, vessel tortuosity and reduced vessel branching indicative for SOD, thus prompting neuro-imaging at an early stage of life. Therefore, close cooperation between ophthalmologists and pediatricians is critical for the diagnosis of orphan diseases.
In conclusion, given the high heterogeneity of the disease, we were able to provide insight into the different ophthalmic manifestations such as retinal, GCL and RNFL thinning using OCT in patients suffering from septo-optic dysplasia. OCT, being non-invasive, provides a great possibility for diagnosing patient with ONH un- or related to SOD at an early age and therefore should be implemented into clinical routine for objective assessment and visualization of the optic nerve head. But, further studies are needed to evaluate these aspects in more detail.
Furthermore, visual function showed stable development with increasing age of the patients, decline in vision was seen as a rare occasion in the study population. But treatment in form of squint surgery as well as occlusion and early supportive therapy had beneficial effect on visual function and secondary complications such as torticollis. Therefore, an individualized pediatric and ophthalmologic management at a highly specialized department is required to allow the best possible visual development in those children.
Footnotes
Acknowledgment
None.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Statement of ethics
For this retrospective analysis local ethics committee approval was obtained.