
Abstract
Purpose
To compare the effects of ranibizumab, aflibercept and bevacizumab treatments in treatment-naive diabetic macular edema(DME) patients with serous retinal detachment(SRD).
Material and methods
This is a retrospective, comparative study. In a sample of 86 eyes of 86 untreated DME patients with accompanying SRD, 23 patients were treated with ranibizumab (IVR), 28 patients with aflibercept (IVA), and 35 patients with bevacizumab (IVB). All were injected intravitreally once a month for a 3-month loading dose. Subsequently, all participants were evaluated every months and if neccessary they received additional intravitreal treatments.Mean changes in best corrected visual acuity (BCVA), central retinal thickness (CRT), and SRD height over the 6-months study period were compared.
Results
At baseline, the groups did not differ in mean BCVA,CRT and SRD height. During the first 3 months, in IVA group the mean decrease in CRT and SRD height were significantly more than in the other two groups (p < 0.05 for all). However, these differences disappeared at 6 months.The number of injections was similar between the groups during the study period.
Conclusion
In patients with DME accompanied by SRD, IVA is a more advantageous option in terms of reduction in CRT and SRD height from baseline to 3 months. In the 6-month period of treatment, IVR, IVA and IVB therapies areanatomically and functionally similar and significant effective modalities.
Introduction
Diabetic macular edema (DME) is one of the most prevalent causes of visual deterioration in diabetic patients. 1 DME's multifactorial and complex pathogenesis is not yet completely known. Multifactorial deterioration of the internal and external blood-retinal barriers in its pathophysiology leads to an abnormal flow of fluid that exceeds the outflow to the neurosensory retina, causing intraretinal and subretinal fluid to accumulate. 2
Vascular endothelial growth factor (VEGF) is an angiogenic factor for endothelial cells and an important vascular permeability mediator. In diabetic retinopathy (DR), it contributes to the dissolution of the blood-retinal barrier, triggering intravascular fluid leakage from dysfunctional retinal capillaries and resulting in DME. Therefore, therapy with anti-VEGF agents is one of the most commonly used treatment strategies. 3 Three commonly used intravitreous VEGF inhibitors bevacizumab (Avastin 100 mg/4 ml; Genentech, Inc., San Francisco, CA), ranibizumab (Lucentis; Genentech, Inc., San Francisco, CA) and aflibercept (Eylea; Regeneron, Tarrytown, NY) have been demonstrated to be beneficial and quite safe for the treatment of DME.4–6
Optical coherence tomography (OCT) classifies morphological edema patterns in DME as diffuse retinal thickening (DRT), cystoid macular edema (CME) and serous retinal detachment (SRD). 7 The diagnosis of SRD is made only with OCT and its incidence has been reported to be between 13% and 45% in DME. 8 Although the effect of anti-VEGF agents have been shown in all DME types, the prognosis and treatment response of SRD is controversial. The existence of SRD may be an important indicator of success of DME therapeutic strategies. Some studies have shown that DME with SRD does not respond better after anti-VEGF treatments. 9 In addition, which VEGF inhibitor superiority to each other in SRD is not known clearly.
Herein, we performed a study comparing the six months of the efficacy of intravitreal bevacizumab (IVB), intravitreal ranibizumab (IVR), and intravitreal aflibercept (IVA) injections in the treatment of DME accompanied by SRD.
Materials and methods
Study design and participants
This retrospective, comparative, single-center study was performed in the Department of Ophthalmology of Kayseri City Hospital, Turkey. The Research Ethics Committee of Kayseri Erciyes University approved (Number:2019/270). The investigators adhered to the tenets of the Helsinki Declaration.
Medical records of treatment-naive patients who hadcenter-involved DME and who were followed up between January 2016 and November 2021 were reviewed. The inclusion flow diagram for the study was depicted in Figure 1.
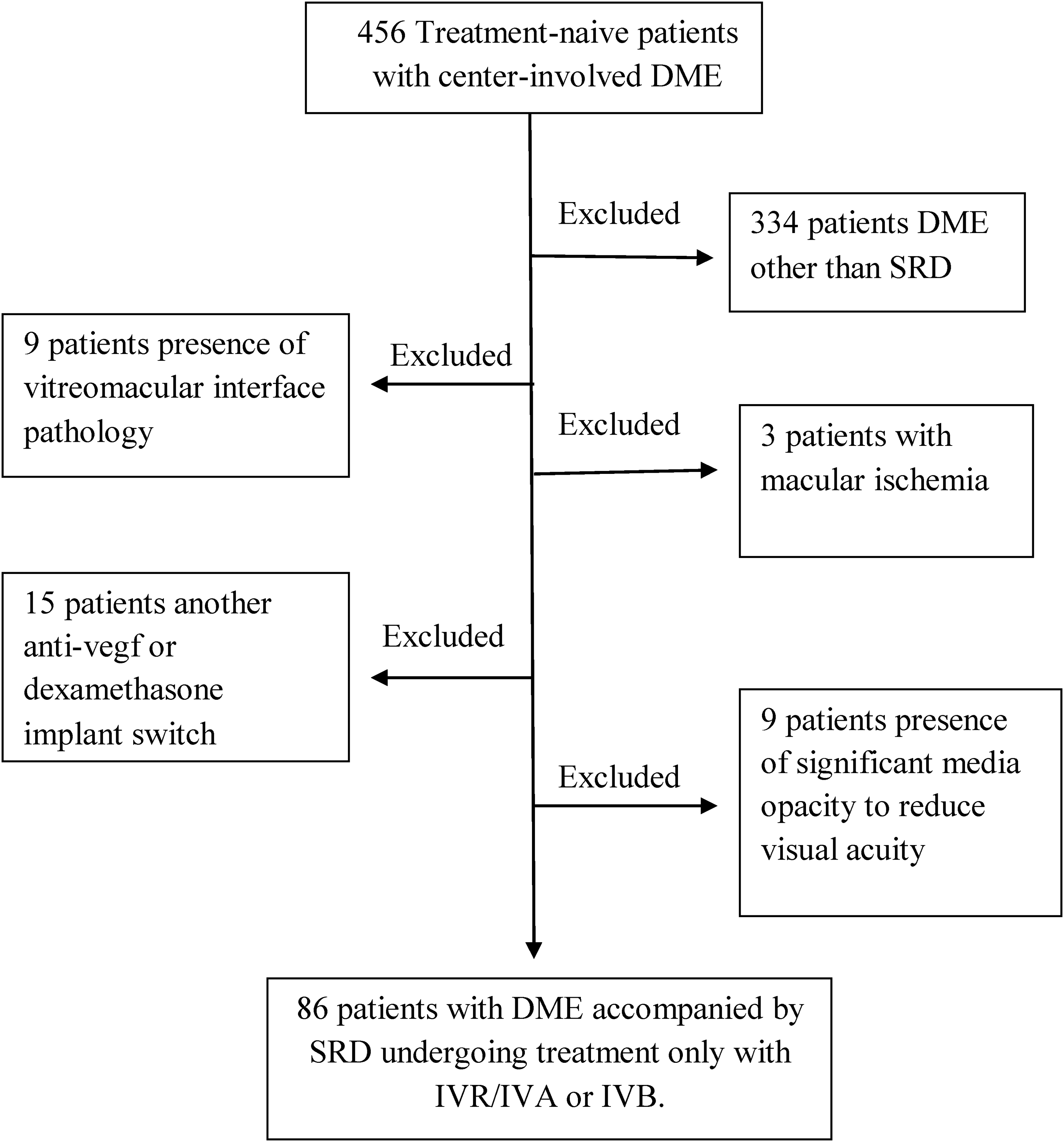
The flowchart of the patient selection process.
Patients with retinal disease other than DR (dry and wet-type macular degeneration, retinal vein occlusion etc.), macular laser (grid or focal), macular ischemia (macular ischemia was characterized as more than two consecutive quadrants of disturbed or expanded foveal avascular zone), presence of vitreomacular traction or epiretinal membrane, previous history of vitreoretinal surgery, corneal disease, cataract or posterior capsule opacification affecting visual acuity and causing media opacity decreasing Spectral domain OCT image quality were excluded from the study. At last, there were 86 eyes of 86 patients with DME accompanied by SRD who met the inclusion criteria.
Data collection and SD-OCT measurements
Best-corrected visual acuity (BCVA) measured by using the ETDRS protocol, slit-lamp biomicroscopy, intraocular pressure with Goldmann applanation tonometer, dilated fundus biomicroscopy, and total number of injections were recorded on the medical charts of the patients.
A fundus fluorescein angiogram (FFA Visucam NM/FA, Carl Zeiss, Germany) was performed to confirm the diagnosis, eliminate the presence of retinal neovascularization, and determine macular ischemia.
The CRT (central retinal thickness) was obtained from the central 1-mm subfield area from SD-OCT (Heidelberg Engineering, Heidelberg, Germany). CRT was specified as the vertical distance between the retinal pigment epithelium (RPE) and the internal limiting membrane in the central fovea and was automatically calculated using the built-in mapping software of the OCT system. The SRD height was measured manually with the built-in caliper tool of the OCT unit and calculated (Figure 2).
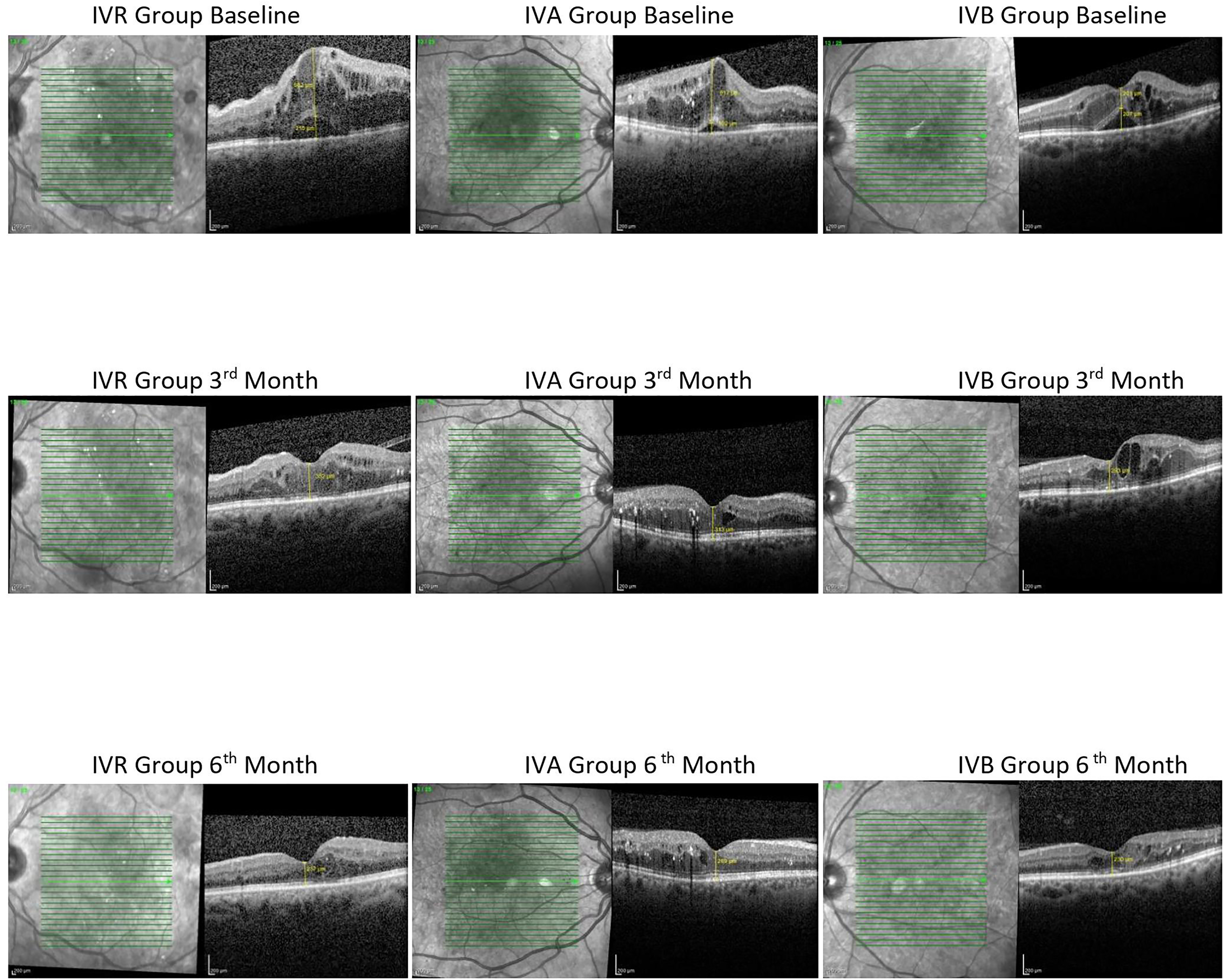
Illustration of height measurement from each group of diabetic macular edema accompanied by serous detachment at baseline, 3rd month and 6th month.
Intravitreal injection procedure
All the injections were performed in the operation room, under sterile conditions, 4 mm behind the limbus in phakic eyes, while 3.5 mm behind in pseudophakic eyes with a 30 Gauge syringe under topical anesthesia. All of the participants were given medication with % 0.5 moxifloxacin five times a day for 5 days after the injection.
Following the application of three monthly doses of anti-VEGF, all participants were assessed every four-weeks and treated with pro re nata (PRN) protocol in case of recurrence according to functional and anatomical parameters. Recurrence was described as BCVA loss of ≥5letters between 2 consecutive visits, SRD persistence, CRT>300 μm, or CRT increase of >10 percent. The BCVA, CRT and SRD height were recorded before and at-3 and-6 months post-treatment.
Statistical analysis
All data analysis was performed using IBM SPSS (Statistical Package for the Social Sciences) version 25. Normality distribution was checked with the Shapiro Wilk test, while categorical variables were analyzed using the chi-square test. Determining descriptive statistics, ‘mean ± standard deviation’, and ‘percentage (%)’ were used. A one-way ANOVA with post hoc Bonferroni test was used to compare variation across the three groups. Pearson's correlation testwas used to examine the relationships among the measured variables.P value of less than 0.05 was considered significant.
Results
A total of 86 eyes of 86 treatment-naive DME patients were analyzed. The patients were divided into three groups; the IVR group consisted of 23 patients, the IVA group consisted of 28 patients, and the IVB group consisted of 35 patients. Each patient completed the 6-month follow-up period. The demographic and clinical characteristics of the enrolled patients summarised in Table 1. There was not a statistically significant difference in both study groups concerning age, gender, duration of diabetes, mean HbA1c level.
Comparison of demographic, ocular and systemic findings of the groups.
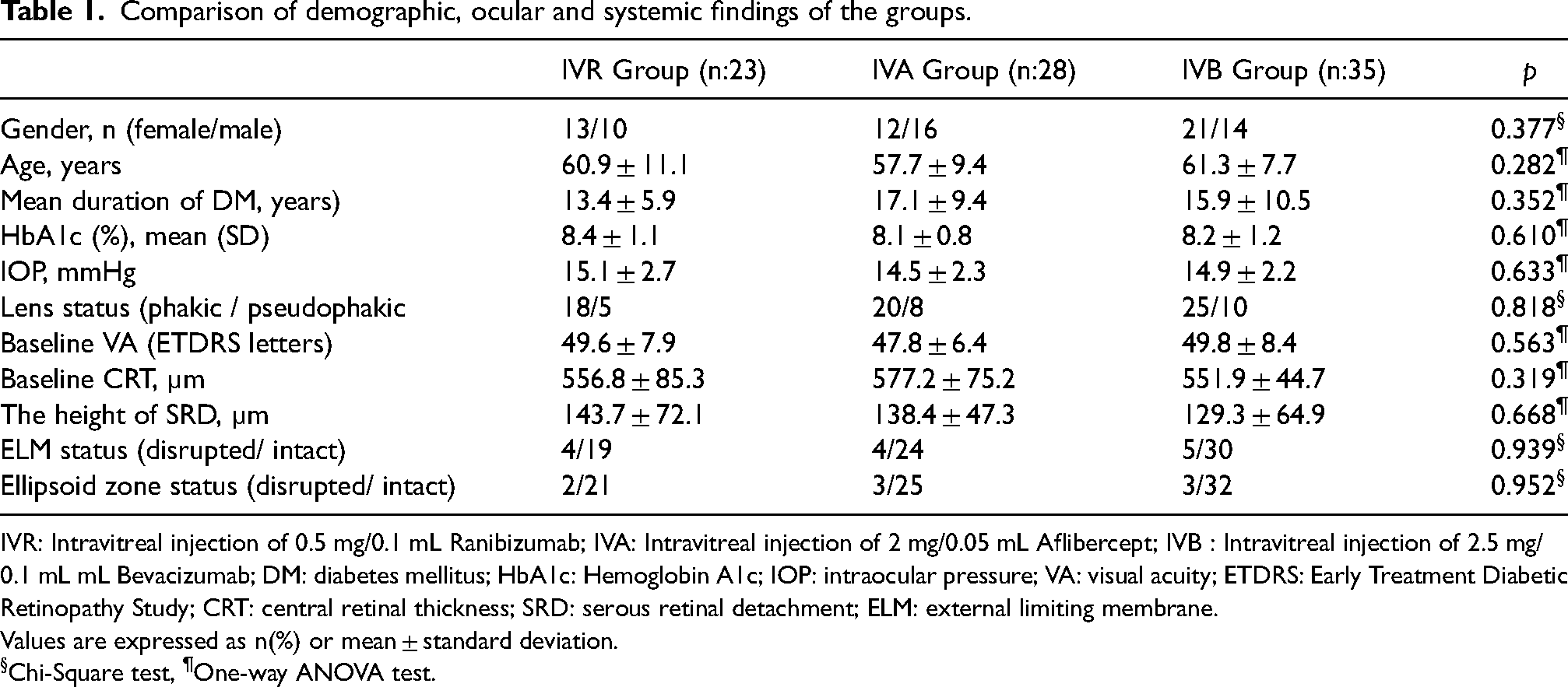
IVR: Intravitreal injection of 0.5 mg/0.1 mL Ranibizumab; IVA: Intravitreal injection of 2 mg/0.05 mL Aflibercept; IVB : Intravitreal injection of 2.5 mg/0.1 mL mL Bevacizumab; DM: diabetes mellitus; HbA1c: Hemoglobin A1c; IOP: intraocular pressure; VA: visual acuity; ETDRS: Early Treatment Diabetic Retinopathy Study; CRT: central retinal thickness; SRD: serous retinal detachment; ELM: external limiting membrane.
Values are expressed as n(%) or mean ± standard deviation.
Chi-Square test, ¶One-way ANOVA test.
During the 6-month follow-up period, the number of injections performed in the IVR, IVA and IVB groups were 5.0 ± 0.7, 4.8 ± 0.9, 5.1 ± 0.8, respectively (p = 0.230). Table 2 shows the mean values of the BCVA, height of CRT, and SRD at baseline and 3 and 6 months after injection.Changes in the mean values of CRT, BCVA, and height of SRD from baseline are shown in Table 3.
Intragroup and intergroup comparisons of central retinal thickness, the height of serous retinal detachment, and best-corrected visual acuity measurements.
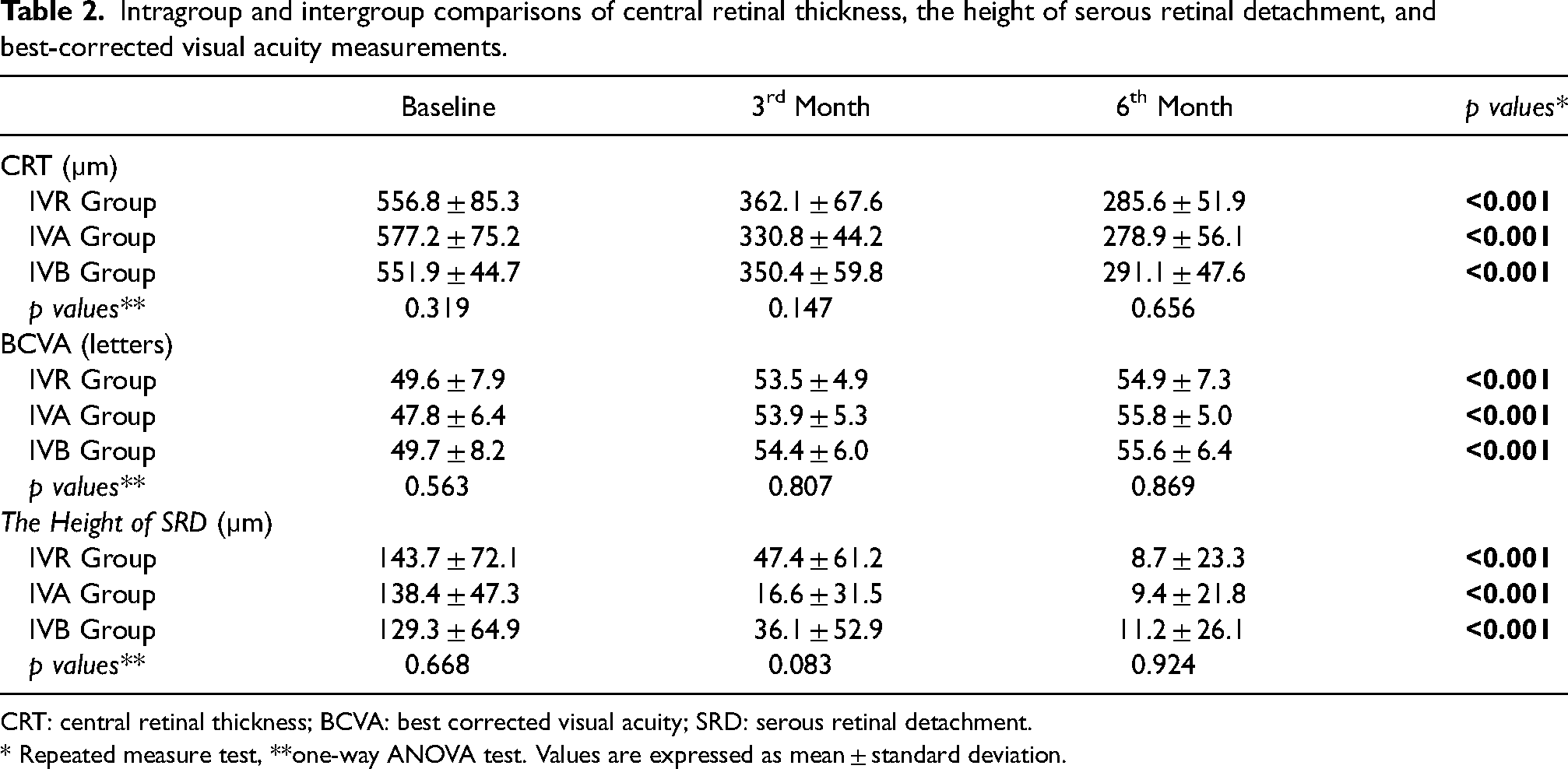
CRT: central retinal thickness; BCVA: best corrected visual acuity; SRD: serous retinal detachment.
* Repeated measure test, **one-way ANOVA test. Values are expressed as mean ± standard deviation.
Comparison of the mean changes of central retinal thickness, best corrected visual acuity and the height of serous retinal detachment measurements in follow up period between the groups.
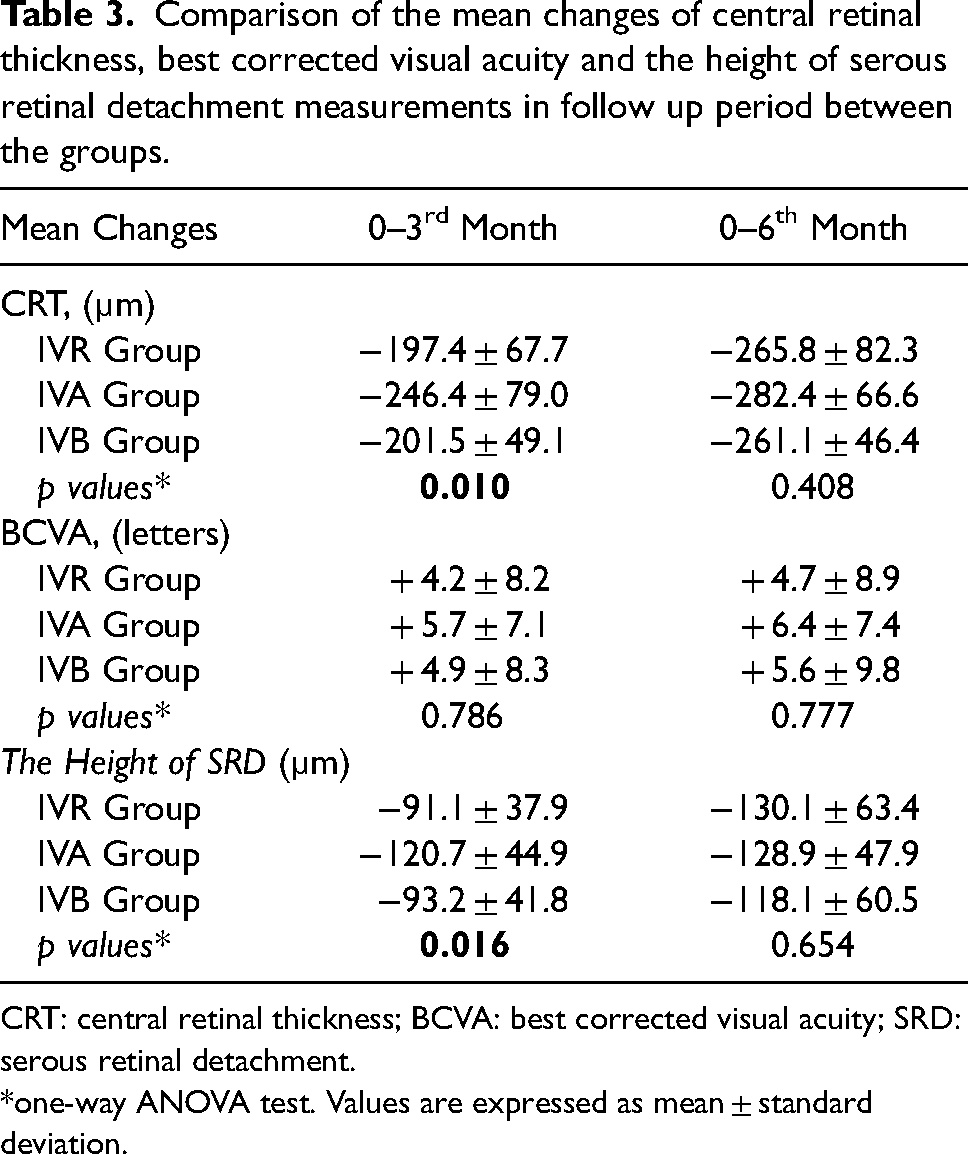
CRT: central retinal thickness; BCVA: best corrected visual acuity; SRD: serous retinal detachment.
*one-way ANOVA test. Values are expressed as mean ± standard deviation.
The mean baseline BCVA was similar among groups (p = 0.563). In three groups, BCVA improved significantly at at months 3 and 6 compared with baseline (p < 0.001 for all). The change in BCVA was not statistically different between the three groups (p = 0.786, p = 0.777, respectively). At six months, 35% of the IVR group, 39% of the IVA group and 31% of the IVB group gained 10 or more ETDRS letters (p = 0.809).
The baseline CRT's before the injection were similar between the groups (p = 0.319). CRT was significantly decreased at 3 and 6 months visits from baseline in all groups (p < 0.001).The mean changes in CRT was significantly greater in the IVA group than in the IVR and IVB group at 3 months (p = 0.024, p = 0.021, respectively), but there was no difference at 6 months (p = 0.408). CRT less than 275 microns was detected in the IVR, IVA and IVB groups at 6 months in 60.9%, 57.1% and 54.3%, respectively (p = 0.884).
The mean baseline SRD heights were similar in each group (p = 0.668). SRD height significantly decreased at 3 and 6 months visits from baseline in both groups (p < 0.001).The mean changes in SRD was significantly greater in the IVA group than in the IVR and IVB group at 3 months (p = 0.042, p = 0.034, respectively), but there was no difference at 6 months (p = 0.654).At 3th month SRD completely resolved 48%, 68% and %57 of the patients in theIVR, IVA and IVB group respectively (p = 0.349). At 6th month SRD completely resolved 83%, 86% and 80% of the patients in theIVR, IVA and IVB group respectively (p = 0.838) The relationship between BCVA, CRT, and SRD measurement baseline in all patients is shown in Table 4. There was a significant correlation between baseline BCVA and CRT (r: −0.649, p < 0.001), but there was no correlation between BCVA and SRD (r: −0.104, p = 0.339). There was no serious ocular or systemic adverse events during the follow-up. No clinical findings of proliferative DR were reported in any patient.
Correlation analysis between the best corrected visual acuity and OCT parameters before intravitreal injection for all patients.
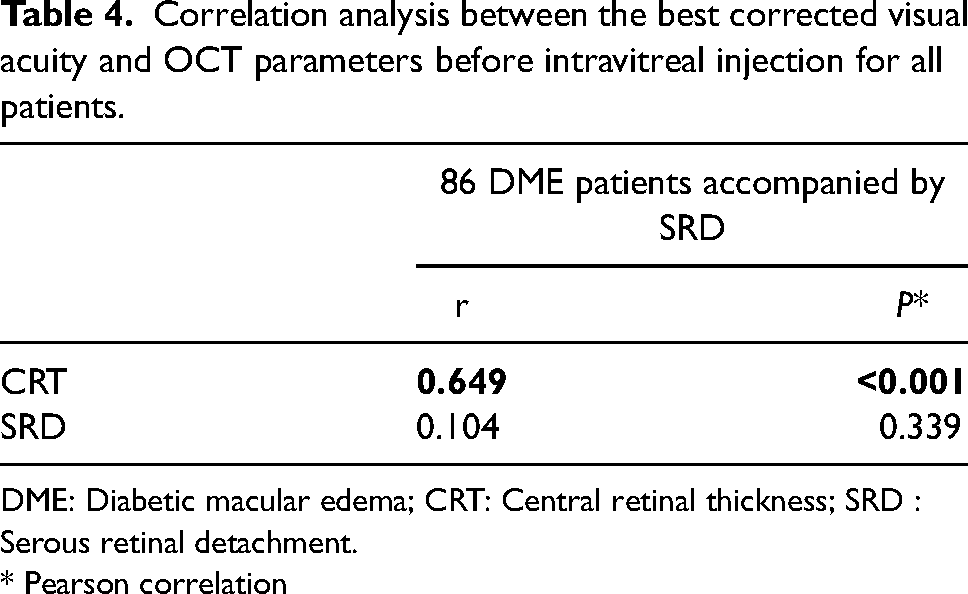
DME: Diabetic macular edema; CRT: Central retinal thickness; SRD : Serous retinal detachment.
* Pearson correlation
Discussion
In this study, we evaluated the treatment response of three different types of VEGFinhibitors (ranibizumab, aflibercept and bevacizumab) in treatment-naive DME patients accompanied by SRD. Our results demonstrated that IVA was superior to CRT and SRD height decrease after 3-loading injections of an anti-VEGF drug, however, there was similar visual and anatomical resultsin all groups at 6 months.
Three subtypes of edema have been identified morphologically in DME: DRT, CME and SRD. 7 It is thought that the main mechanism in the formation of SRD is leakage from the retinal or choroidal circulation into the subretinal space by exceeding the drainage capacity. 10 In addition, it has been reported that there may be abnormalities in the retinal pigment epithelium that allows the excess fluid from the choriocapillaris to pass to the sensory retina. 11 Since different mechanisms may underlie in different types of DME, treatment selection may vary according to edema types. Furthermore, it has been reported in the literature that DME accompanying SRD may have different treatment responses.
The efficacy of anti-VEGF therapy in DME and its subtypes have been demonstrated in many studies. In Protocol-T Diabetic Retinopathy Clinical Research Network study, the effectiveness of three anti-VEGF drugs— aflibercept, bevacizumab, and ranibizumab — were compared during a 2-year follow-up of DME patients. There was no significant difference in visual acuity gain for all 3 agents in patients with good initial visual acuity at first year In the group of patients with visual acuity 20/50 or worse at baseline, IVA was found to be more effective than the other two agents in improving vision. 12 Nevertheless, there is no clear consensus on the effect of SRD on intravitreal treatment modalities in DME.
In some studies, the presence of SRD may result in inadequate anti-VEGF response; However, others have reported that adequate response can be obtained in the presence of SRD and may be a favorable prognostic factor. Koytak et al. reported that there was no statistically significant difference between the DRT, CME and SRD subtypes in the improvements in BCVA following IVB injection, but a significant reduction in CRT was observed in the CME and SRD subtypes than in the DRT subgroup. 13 Kim et al. IVB treatment applied in patients with DME subtypes was evaluated, in SRD subtype compared to other types of CRT that showed better reduction but similar visual acuity. 14 In our study we did not evaluate the efficacy of existence of different subtypes of DME on BCVA. However, we found that all 3 anti-VEGF drug significantly improved BCVA similarly in all patients agreed with those 2 studies.
On the other hand, Seo et al evaluated different morphological type DME with IVR treatment response and it was determined that the efficiency was the lowest in SRD subtype. 15 Similarly, Shimura et al. compared IVB treatment with different types of DME and highlighted the weakest effect in SRD type. 9 Our aim was to find out how the three anti-VEGF drugs behaved in DME with SRD subtype to reveal that if existence of SRD was a poor prognostic factor.
In a retrospective study evaluating the efficacy of IVR treatment in different types of DME, they reported that although IVR treatment was anatomically successful in the SRD subtype, functional success was low. They attributed this to the fact that damage to the ellipsoid region and outer limiting membrane might be more in these patients. 16 We found that not only IVR but also all three anti-VEGF drugs was similar on both anatomical and functional success (decrease in CRT and increase in BCVA) at 6 months period. However, we did not evaluate the correlation between the time interval of SRD exictence and BCVA or CRT. It can be postulated that long-term detachments can trigger apoptotic processes inside the retina and may trigger irreversible changes. Hence, in a further research the correlation between the condition of elipsoid region with the duration of SRD exictence and the anti-VEGF treatments should be studied.
The Ozkaya et al. study compared the effects of IVR and IVA in DME patients with SRD. Although both IVA and IVR were effective in terms of their anatomical and functional results, they found that IVA was more effective in the 12th month. 17 In contrast, we found that all three agents were similarly effective on decreasing CRT and increasing BCVA. However, we found the IVA superiority in decreasing CRT and SRD height in 3-months period.
The greater effectiveness of IVA in regression of SRD may be due to its additive effect on PIGF other than VEGF.Although the VEGF pathway is known to play the most important role in DME, non-VEGF molecules may play a role, especially in SRD-related DME. One of these molecules is PIGF, which has not been discussed much. Aflibercept has a effect on VEGF-A, as well as PIGF. 18 While VEGFA is known to play a central role in both physiological and pathological conditions, the role of PIGF seems to be specific to pathological conditions. 19 Aflibercept ability to bind both VEGFA and PIGF can have additional useful effects on diabetic retinopathy. The PIGF blockage has been shown to inhibit the steps after tumor necrosis factor alpha to protect the retina from high glucose damage. 20 PlGF is secreted by retinal pigment epithelial cells in response to hypoxia. Studies have shown that in DME has higher PIGF concentrations in both the anterior chamber and vitreous. 21 A theory in the pathogenesis of SRD is the failure of the retinal pigment epithelium (RPE) pump mechanism. 11 It attaches to VEGFR-1 receptors, causing disruption of tight junctions between RPE cells, thus causing subretinal fluid accumulation and macular edema.22,23 In addition, it has been shown that the PlGF antibody inhibits inflammation and angiogenesis in the DR mouse model. 24 Moreover Lazzara et al showed that PIGF inhibition improves diabetes-related inflammation in retinal cells. 20 The greater effectiveness of IVA in regression of SRD may be due to its additive effect on PIGF other than anti-VEGF agents.
It has been reported that dexamethasone implant may be an effective option in the treatment of SRD accompanied by DME.25–27 It is thought that dexamethasone acts by regulating the permeability of vascular structures and by regulating retinal pigment epithelial pump failure.11,28 Ozdemir et al. reported that the dexamethasone implant causes an increase in BCVA and a decrease in SRD and CRT in patients with SRD accompanied by DME. 29 On the other hand, Vujosevic et al compared intravitreal dexamethasone and IVR in DME patients with SRD and found no difference between SRD solutions. 30 In our study, three different types of anti-VEGF were compared. In all three types, it was found that by the end of six months, 80% and more (highly effective) fluids were dissolved in all of the patients.
The major limitations of our study include its retrospective design, represents the results of a single center and short follow-up period results. Longer follow-up duration can also enlighten more precisely the response to different type of anti-VEGF therapies and the conditions for alternative options.
In conclusion our study demonstrated that IVR, IVA and IVB are anatomically and functionally effective treatment modalities in DME patients with SRD. IVA is more effective than IVR and IVB in improving BCVA, CRT, and SRD elevation from baseline to 3 months. These results should be confirmed by additional studies with more participants and longer follow-up periods.
Footnotes
Author’s Contributions
Ender Sirakaya - corresponding author. Deniz Kilic - coauthor. Hatice Aslan Sirakaya - coauthor. Designed the study: Ender Sirakaya, Deniz Kilic. Collected the data: Ender Sirakaya, Deniz Kilic, Hatice Aslan Sirakaya. Analyzed the data: Ender Sirakaya, Deniz Kilic. Wrote the paper: Ender Sirakaya, Deniz Kilic, Hatice Aslan Sirakaya. All authors have read and approved the final manuscript.
Data availability
All data generated or analysed during this study are included in this article. Further enquiries can be directed to the corresponding author.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics committee approval
This retrospective study was approved by the local ethics committee (Ethics committee decision: Erciyes University 2019/270).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from patients who participated in this study.
Peer-review
Externally peer-reviewed.