
Abstract
Purpose
To compare the clinical outcomes of intracorneal ring segment (ICRS) implantation in eyes with advanced vs. mild/moderate keratoconus (KCN).
Methods
A retrospective analysis of 141 eyes of 111 patients with KCN who underwent ICRS implantation. Preoperative maximum keratometry (Kmax) was <57 diopters (D) in 70 eyes and >57 D in 71 eyes. Postoperatively, corrected distance visual acuity (CDVA), Kmax, and intraoperative and postoperative complications were assessed at 1 day, 1 month, and 1 year.
Results
Corneas with a preoperative Kmax >57 D experienced greater reduction in axial curvature after ICRS implantation than corneas with a preoperative Kmax <57 D (7.0 D vs. 5.5 D, p=0.005) and gained more Snellen lines of CDVA (3 vs. 1, p<0.001) by 1 year postoperatively. The incidences of the most prevalent complications (explantation, extrusion, and infectious keratitis) did not differ significantly between the two groups (p=0.29, p=0.99, p=0.98).
Conclusions
The visual and topographic effects of ICRS implantation are greater in eyes with more advanced KCN, with no increase in the incidence of the most common complications.
Manuscript
Keratoconus (KCN) is a non-inflammatory disease characterized by corneal thinning and steepening, resulting in progressive optical deterioration of the cornea. 1 For patients with mild to moderate disease, intracorneal ring segments (ICRS) have been employed to affect a reduction in corneal curvature and thereby improve the refractive status of the operated eye.2–4 However, patients with advanced KCN have typically been regarded as ineligible for ICRS, owing to a suspected increase in risk for various postoperative complications (segment extrusion and overlying corneal melt) and suspected decrease potential for visual benefit.5,6 Moreover, no studies have documented outcomes for ICRS implantation in eyes with very advanced KCN. Because eyes with advanced KCN often have fewer treatment options than their mild to moderate counterparts, studies showing safety and efficacy for existing procedures in this population may be an efficient and simple way of improving patient outcomes. Here, we present results of a large consecutive series of patients with advanced KCN undergoing ICRS implantation and compare the outcomes against a matched cohort of eyes undergoing the same procedure for mild to moderate KCN.
Patients and methods
This study comprised a retrospective review of 141 consecutive eyes in 111 patients who underwent ICRS implantation for KCN from one tertiary referral center: Parker Cornea in Birmingham, AL, USA between March 2017 and March 2020. Institutional Review Board approval was obtained, and the study was conducted in accordance with the tenets of the Declaration of Helsinki. Informed consent was acquired from each patient.
All patients were examined by slit lamp biomicroscopy and rotating Scheimpflug corneal tomography (Pentacam HR; Oculus, Wetzler, Germany). Clinical features at presentation included thinnest point thickness (TPT), maximum keratometry (Kmax), and corrected distance visual acuity (CDVA).
After diagnosis of KCN, each patient was considered for ICRS implantation if they met the following criteria: CDVA ≤ 20/50, contact lens intolerance, no significant central corneal opacity, and minimum corneal thickness of 450 μm at the site of the planned corneal incision. For the purpose of this study, patients were classified as having “advanced” vs. “mild/moderate” KCN if their maximum keratometry (Kmax) value exceeded 57 diopters (D), which is the literature-supported upper limit value beyond which ICRS is no longer traditionally recommended. 7 Each patient underwent the implantation of one or two 0.350 mm ICRS (Intacs, CorneaGen, Seattle, WA) depending on the location of the cone via a manual implantation technique. 3 Specifically, a guarded diamond blade set to 80% corneal thickness at the location of the incision site was used to make a single temporal radial incision. After applying suction, a pocketing hook was used to create a small stromal pocket at the base of the incision. Arc-shaped corneal separators were inserted into the stromal pockets to bluntly dissect semicircular channels between the lamellar planes, the ICRS were gently inserted, and the incision was closed with a single suture or fibrin-based adhesive, if needed. Two ICRS were placed for centrally located cones, whereas only one ICRS was placed for corneas with inferior cones (i.e., isolated inferior steepening). All patients received standard postoperative protocol with topical antibiotic and steroid eye drops three times per day for 1 week. All intraoperative and postoperative complications were recorded. Patients demonstrating progressive disease underwent ultraviolet corneal crosslinking (CXL) according to Dresden protocol following ICRS implantation. 8 Disease progression evaluation in regard to eligibility for corneal crosslinking is multivariable, including visual and tomographic changes, including but not limited to corneal thinning more than 10 µm, increase in back elevation or front elevation, increase in Kmax, increase of 1 D of cylinder refractive power, increase of 2 D of spherical refractive power.
The primary outcomes were changes in axial curvature and CDVA, both of which were collected and analyzed at 1 day, 1 month, and 1 year postoperatively. Change in Kmax was defined as the difference between preoperative and postoperative Kmax at each follow-up visit. Maximum flattening was defined as the greatest difference between preoperative and postoperative axial curvature at any single location on the cornea. For reference, maximum flattening most commonly occurred at or adjacent to the location of segment implantation, while Kmax was often located slightly more centrally. Patients who elected to undergo ICRS explantation of all segments for subjective glare and photopsia were excluded from analysis for all subsequent visits.
Statistical analysis was performed using SAS Software Suite (version 9.4; SAS Institute). Continuous variables were expressed as mean (median, range). The one-sample Shapiro-Wilk test was used to assess normality of distribution. Comparison between groups was performed using the one-way ANOVA test for continuous variables with normal distribution and Kruskal-Wallis test for continuous variables without normal distribution. Comparison of categorical variables was performed using the likelihood ratio Chi-square test and Fisher's exact test when indicated. Binary logistic regression analysis was performed to identify factors potentially predictive of changes in corneal curvature or CDVA, which could act as confounders. Variables found to be significant in univariate analysis at a level of p<0.10 (preoperative TPT and number of segments implanted) were entered into multivariate multiple regression models using the stepwise Wald method, which further excluded variables non-contributory to the fit of the model (p>0.05). Trends in corneal curvature and CDVA were assessed using multivariate linear regression and multivariate logistic regression when appropriate. Effect modification was assessed using interaction regression models, which were used to generate trend plots for variables with significant interaction. A two-sided p-value <0.05 was considered statistically significant for results of all regression models.
Results
There were 141 eyes in 111 consecutive patients who were diagnosed with KCN and treated with ICRS implantation over a 3-year period. Patients who underwent explantation of all segments (n=5) were excluded from analyses of all time points after explantation.
Clinical features at presentation and related treatments are listed in Table 1. Comparison of patients with advanced KCN vs. mild/moderate KCN revealed thinner TPT (427 μm vs. 469 μm, p<0.001) and inferior mean CDVA (LogMAR: 0.44 vs. 0.32, p=0.003), specifically a lower likelihood of having CDVA ≥ 20/40 (46% vs. 68%, p=0.04). Eyes with advanced KCN were more likely to have 2 ICRS implanted (25% vs. 9%, p=0.008). No difference in rate of segment explantation (p=0.29) or subsequent ultraviolet corneal crosslinking (CXL) (p=0.29) was noted.
Intracorneal Ring Segment Implantation in Advanced Keratoconus. Clinical Features and Treatments.
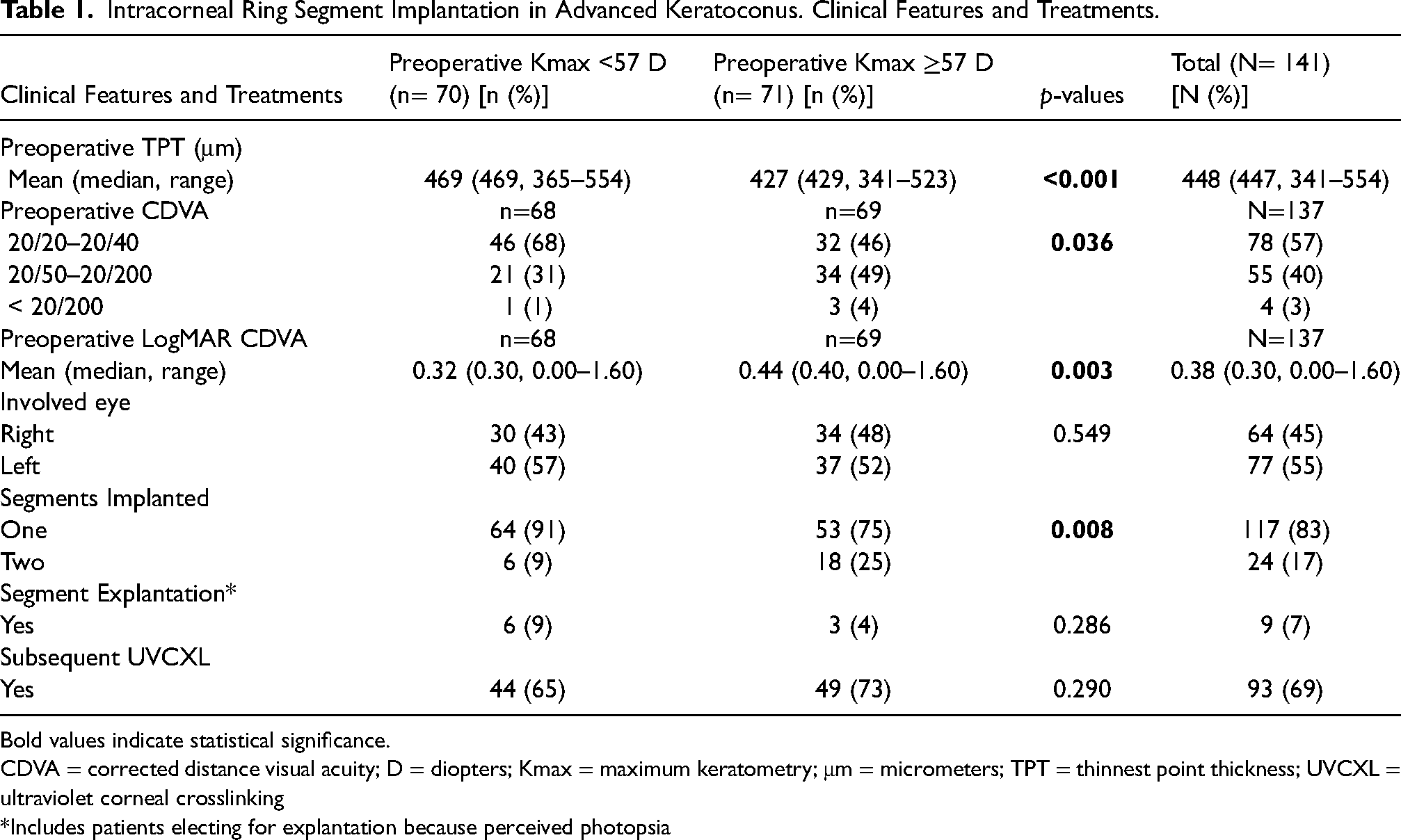
Bold values indicate statistical significance.
CDVA = corrected distance visual acuity; D = diopters; Kmax = maximum keratometry; μm = micrometers; TPT = thinnest point thickness; UVCXL = ultraviolet corneal crosslinking
*Includes patients electing for explantation because perceived photopsia
Intraoperative and postoperative complications are as follows: seven eyes (5%) experienced complications, and no difference in rate was noticed between eyes with advanced KCN and mild/moderate KCN (4 vs. 3, p=0.73). The most common complications were infectious infiltrate (n=4) and segment extrusion (n=4), which exhibited the same rate in the two groups, each exhibiting 2 episodes of infectious infiltrate and segment extrusion (p=0.98 and p=0.99, respectively). One eye experienced intraoperative posterior corneal perforation into the anterior chamber during channel dissection; however, the segment was successfully placed, and no postoperative complications were noted in that eye.
For the total population, median preoperative CDVA was 20/40 and improved to 20/30 at 1 day, 20/30 at 1 month, and 20/25 at 1 year postoperative. For mild/moderate KCN, median preoperative CDVA was 20/40 and improved to 20/30 at all postoperative timepoints. For advanced KCN, median preoperative CDVA was 20/50 and improved to 20/40 at 1 day, 20/35 at 1 month, and 20/25 at 1 year postoperative. Eyes with advanced KC saw greater improvement in CDVA than eyes with mild/moderate KCN (3 Snellen lines vs. 1 Snellen line, p<0.001), including a higher percentage of eyes gaining 5 or more Snellen lines (13% vs. 8%) and a higher percentage of eyes losing 2 or more Snellen lines (5% vs. 2%). Median LogMAR visual acuity improved more in the advanced cohort (0.40 to 0.10) than in the mild/moderate cohort (0.30 to 0.18). Eyes with very advanced KCN (preoperative Kmax ≥70 D) experienced improvement of median CDVA from 20/80 to 20/28 in the first postoperative year (Figure 1). Subsequent CXL did not impact the magnitude of CDVA improvement following ICRS implantation.
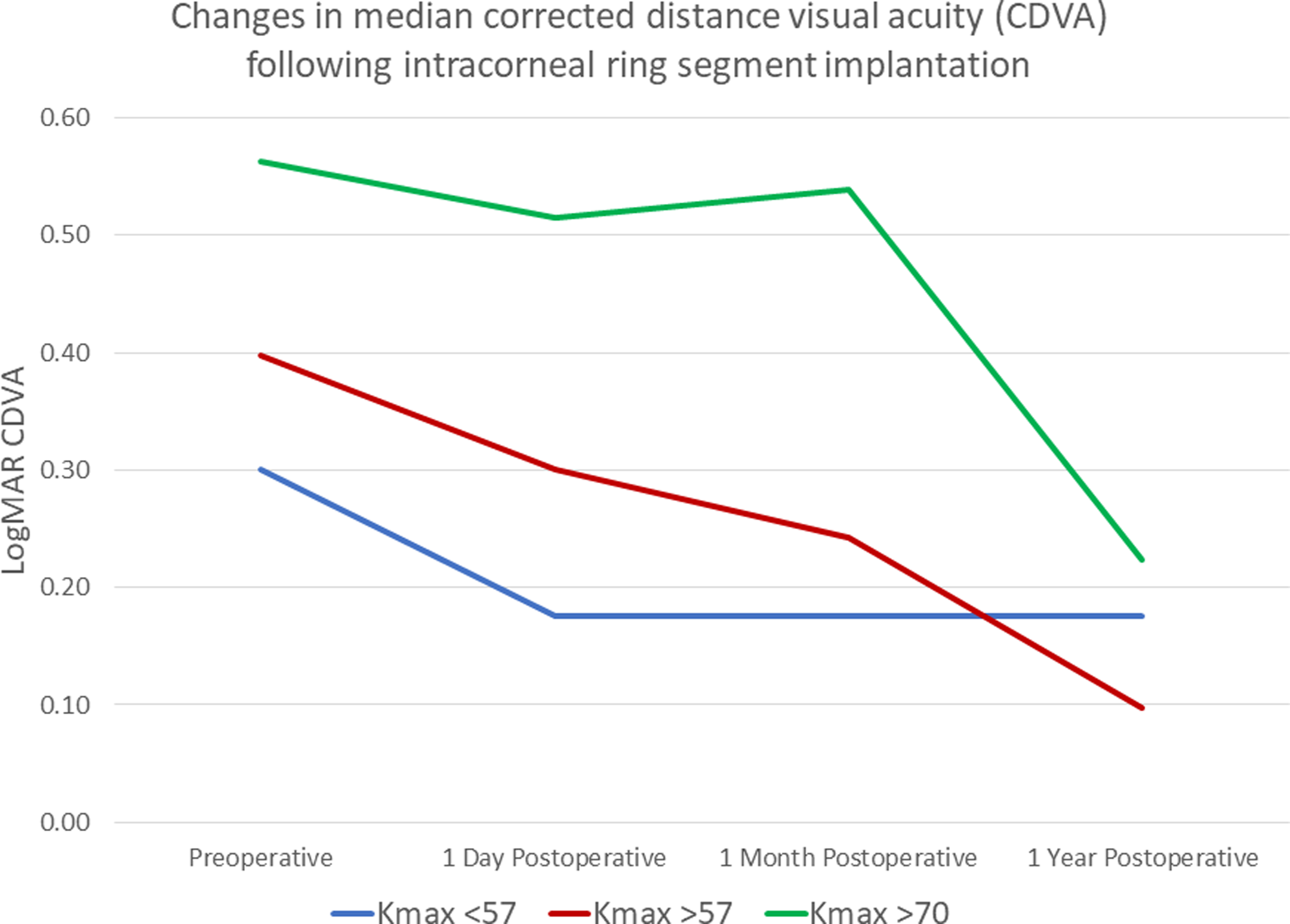
Line graph demonstrating the changes in median corrected distance visual acuity (CDVA) following intracorneal ring segment implantation, stratified by preoperative maximum keratometry (Kmax): Kmax <57 diopters (D), Kmax ≥57 D, and Kmax ≥70 D. Eyes with more advanced keratoconus demonstrate a greater degree of improvement in CDVA postoperatively, particularly by 1 year.
Changes in corneal curvature after ICRS implantation are listed in Table 2. The mean reduction in Kmax by 12 months postoperatively was 2.4 D, and eyes with advanced KC demonstrated greater flattening than eyes with mild/moderate KCN (3.2 D vs. 1.5 D, p=0.01). Maximum flattening at any point on the cornea was 6.4 D by 12 months postoperatively, and eyes with advanced KCN experienced more flattening that eyes with mild/moderate KC (7.0 D vs. 5.5 D, p=0.005) (Figure 2). Preoperative Kmax is predictive of the degree of maximum flattening after ICRS implantation. Yet its interaction – or effect modification – with other preoperative metrics, such as preoperative TPT, also significantly correlates with maximum flattening (p=0.02), meaning the effect of TPT on postoperative flattening depends on the steepness of the cornea. Although maximum flattening at 1 year postoperative does not trend with preoperative TPT in mild/moderate KCN, thinner corneas typically demonstrate a greater degree of maximum flattening than thicker corneas in eyes with advanced KCN (Figure 3). Subsequent CXL did not impact the magnitude of corneal flattening following ICRS implantation.
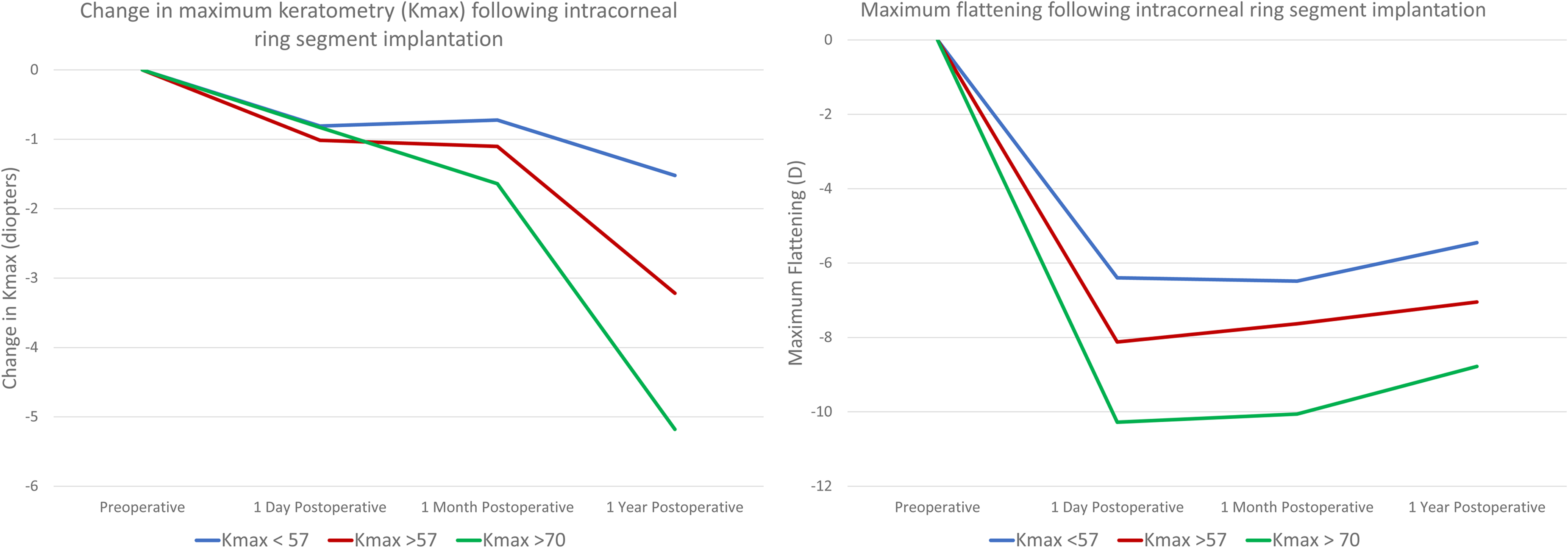
Line graphs demonstrating the changes in maximum keratometry (Kmax) and maximum flattinging following intracorneal ring segment implantation, stratified by preoperative keratometry: Kmax <57 diopters (D), Kmax ≥57 D, and Kmax ≥70 D. Flattening of Kmax seems to occur throughout the first year after surgery. Eyes with more advanced keratoconus demonstrate a greater degree of reduction in Kmax at 1 year postoperatively. Notably, there is no significant difference in reduction of Kmax with the first postoperative month. Conversely, the value of maximum flattening is its greatest immediately postoperatively and decreases through the first postoperative year, suggesting the shape of corneas may “normalize” throughout the first postoperative year. Eyes with more advanced keratoconus demonstrate a greater degree of maximum flattening at 1 year postoperatively.
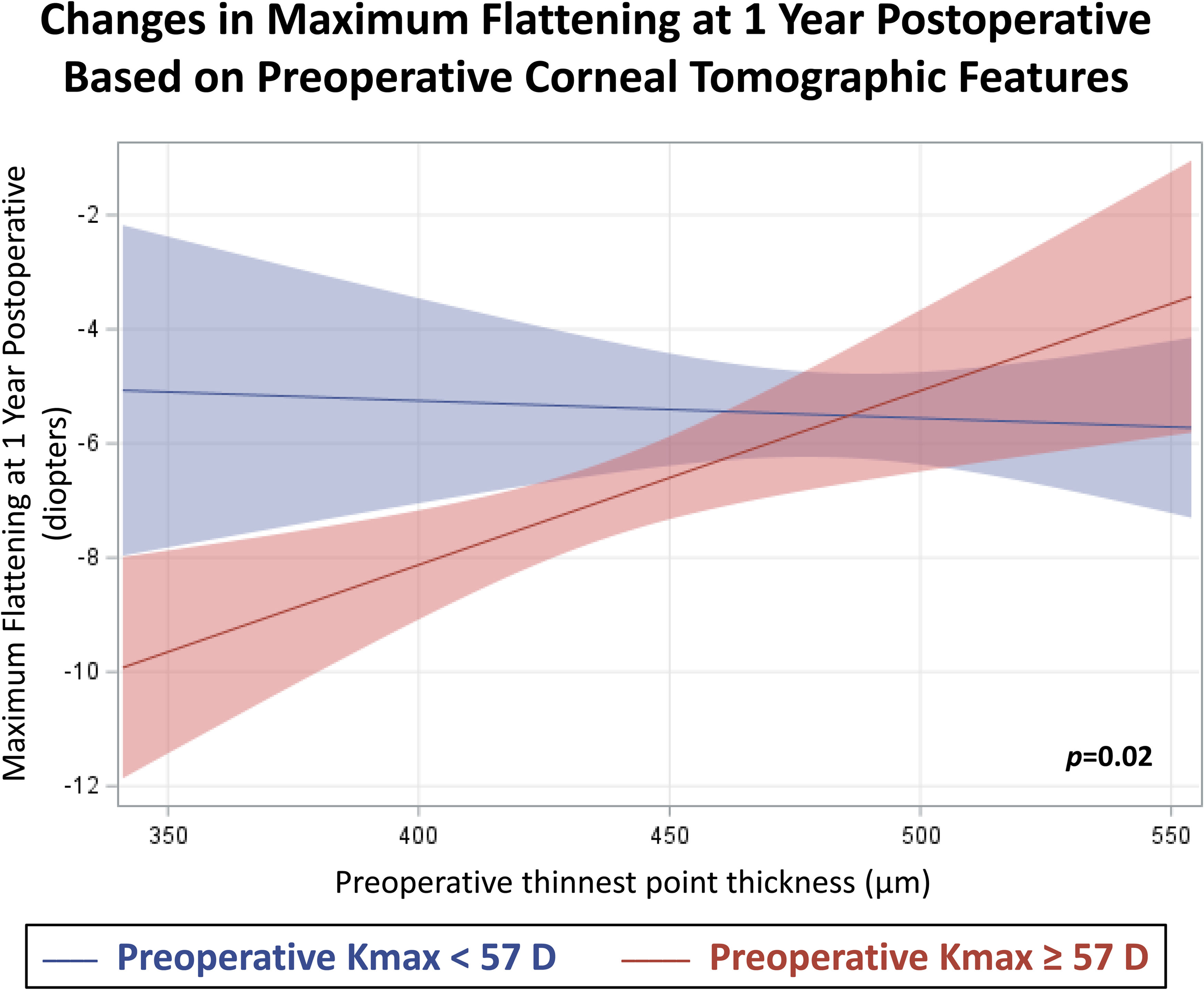
Plot of interactions between preoperative maximum keratometry (Kmax) and preoperative thinnest point thickness (TPT) to demonstrate effect modification on the outcome of changes in corneal curvature. In addition to preoperative Kmax and preoperative TPT correlating with maximum flattening at 1 year, the interaction between the two variables significantly contributes to the prediction of maximum flattening (p=0.02); therefore, TPT has a greater effect on flattening in eyes with advanced keratoconus compared to eyes with mild/moderate keratoconus.
Intracorneal Ring Segment Implantation in Advanced Keratoconus. Changes in Corneal Curvature.
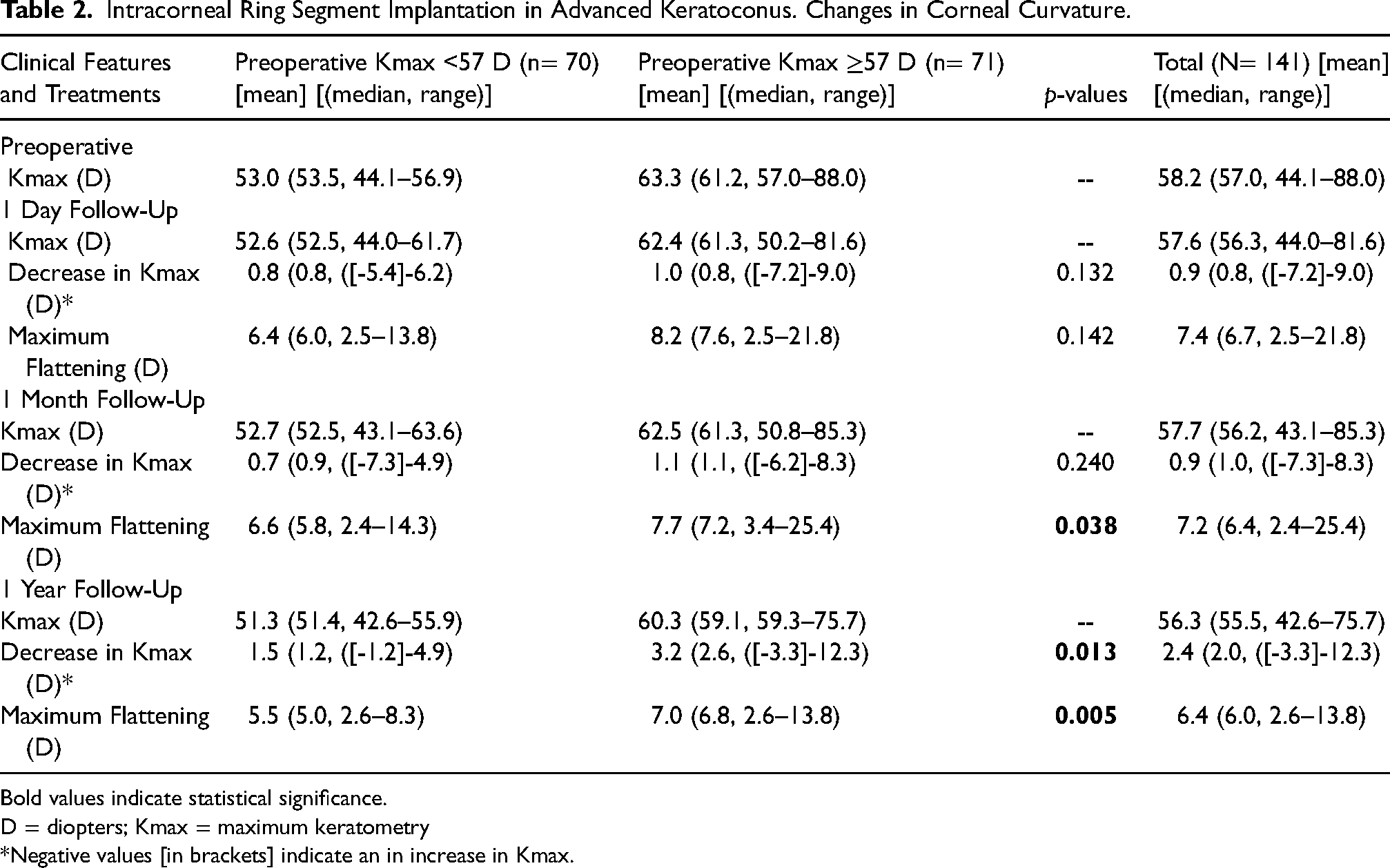
Bold values indicate statistical significance.
D = diopters; Kmax = maximum keratometry
*Negative values [in brackets] indicate an in increase in Kmax.
Discussion
Historically, penetrating keratoplasty (PK) and deep anterior lamellar keratoplasty were the standard of care in patients with advanced KCN despite often suboptimal visual outcomes, potential wound healing and suture related complications, and risk for continued disease progression, graft instability and dehiscence, allograft reaction and rejection, etc.9,10 Conversely, ICRS implantation serves as one of a relatively small number of minimally invasive surgical interventions that consistently improves visual acuity for populations with KCN, yet the reported change in CDVA ranges widely among individuals: from a loss of 3 Snellen lines to a gain of 8 Snellen lines.6,11–13 In 2006, Alió et al initially suggested that eyes with a higher preoperative mean keratometry, especially >55 D, experienced worse visual outcomes following ICRS implantation because a high percentage of eyes saw decreased visual acuity postoperative had steeper corneas, yet this early conclusion was drawn based on the results of only 4 eyes. 5 However, more recent studies have been more positive, for example, Kahn et al demonstrated dramatic flattening in eyes with advanced KCN following ICRS implantation, reaching 12.0 D in one case and achieving contact lens tolerance in all cases. 14
Evidence is mounting to make the argument that ICRS implantation in eyes with advanced KCN can be safely implemented to improve quality of life both immediately (better visual acuity) and long term (prevention of PK), but no large studies have directly compared the outcomes of patients with advanced KCN and patients with mild to moderate KCN until this one. Our study was designed to assess safety, functional effectiveness, and structural effectiveness in eyes with advanced KCN and comparing it to eyes that received the same treatment for mild to moderate KCN.
For safety, the severity of KCN did not impact the rate of complications following ICRS implantation. There was no significant difference in explantation rate between mild/moderate and advanced KCN, and most eyes underwent explantation electively for visual distortions, rather than extrusion or stromal melt. Segment migration and segment extrusion was managed with segment repositioning, except in cases with concomitant secondary bacterial keratitis, when explantation was performed. All eyes that developed secondary bacterial keratitis were successfully treated with topical antibiotic drops. For the patient who underwent intraoperative posterior corneal perforation, the surgery was successfully completed without postoperative complications, and the patient experienced 2 Snellen lines of CDVA improvement and 14.6 D of maximum flattening on the first postoperative day. Notably, no patients required PK within the follow-up period.
For functional effectiveness, while the entire cohort exhibited visual improvement, the outcome in eyes with advanced KCN was objectively better, with median CDVA improving from 20/50 to 20/25. Moreover, eyes with very advanced KCN (Kmax > 70D) underwent even greater relative improvement in median CDVA, from 20/80 to 20/28. The improvement in the patients’ functional capacity stems from the structural effectiveness of ICRS implantation, particularly in eyes with advanced KCN, which not only demonstrated an additional 1.5 D of maximum flattening at 1 year compared eyes with mild/moderate KCN but also an additional 1.7 D in reduction of Kmax at 1 year. Yet preoperative corneal curvature is not the only metric that may be predictive of postoperative flattening. For eyes with advanced KCN, preoperative TPT may play a role as well. Intuitively, in this group, thinner corneas – given their weakened biomechanical stability – exhibit a greater degree of flattening after ICRS implantation than thicker corneas with advanced KCN, yet this interaction between preoperative corneal thickness and keratometry does not hold true as a predictor of postoperative flattening in eyes with mild/moderate KCN (Figure 3). Caution should be used when interpreting this result, however, because ICRS implantation is contraindicated in eyes with extremely thin corneas (corneal thickness < 450 μm at the site of implantation), which may truly be a more significant risk factor for certain complications (especially segment extrusion and stromal melt) than corneal curvature. 7
Limitations to this study include its retrospective design. Intermediate follow-up appointments (between 1 month and 1 year) often took place with a referring physician or optometrist, so incremental trends within the first year were not able to be analyzed. Longer follow-up after 1 year could lend more insight to stability of visual and tomographical outcomes. Past medical history, such as allergies or atopy, could provide key information that may correlate with which patients develop segment migration or extrusion, given their increased likelihood to engage in eye rubbing.
In summary, while significant literature suggests that ICRS implantation is an appropriate measure to improve visual outcomes in eyes with mild to moderate KCN, ICRS implantation may also be a safe and effective procedure for the treatment of eyes with advanced KCN, displaying a greater degree of improvement in CDVA (3 Snellen lines vs. 1 Snellen line), reduction in Kmax (3.2 D vs. 1.5 D) and maximum flattening at any point on the cornea (7.0 D vs. 5.5 D). These results suggest that ICRS implantation may be a viable option to improve vision in patients with advanced KCN, particularly when combined with the stabilizing effects of CXL, which may prevent the need for more invasive treatments.
Footnotes
Abbreviations/Acronyms
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article