
Abstract
Purpose
To explore whether baseline visual impairment (VI) increases the risk of cognitive function impairment (CFI).
Methods
We conducted a population-based cohort study, with a six-year follow-up period. The exposure factor of interest in this study was VI. The Mini-Mental State Examination (MMSE) was used to assess participants’ cognitive function. The Logistic regression model was used to investigate whether baseline VI had an effect on CFI. Confounding factors were adjusted in the regression model. The odds ratio (OR) and 95% confidence interval (CI) were used to quantify the effect of VI on CFI.
Results
A total of 3297 participants were included in the present study. The mean age of included participants was 58.5 ± 7.2 years. Male accounted for 1480 (44.9%) of all participants. At baseline, 127 (3.9%) of the participants had VI. The MMSE score of participants who had VI at baseline decreased by 1.7 ± 3.3 points on average during the six-year follow-up, and that of participants who had no VI at baseline decreased by 1.1 ± 3.3 points on average. The difference was significant (t = 2.03, p = 0.040). Results of the multivariable Logistic regression model showed that VI was a risk factor for CFI, with an OR of 1.052 (95%CI: 1.014 to 1.092, p = 0.017).
Conclusions
Averagely, participants with VI experienced a decline in cognitive function 0.1 points faster per year than participants without VI, as measured by MMSE score. VI is an independent risk factor for CFI.
Introduction
Visual impairment (VI) is a global public health issue. It is estimated that 895 millions people would be visually impaired in 2050. 1 VI accounts for 3.8% of the global disease burden, as estimated by years lived with disability. Cognitive function impairment (CFI) is a common disease in the elderly characterized by decreased attention and memory. The prevalence of CFI is 25.5% 2 among people over 60 years of age and 30% among people over 80 years of age. 3 CFI has a significant impact on patients’ daily life and increases the risk of all-cause mortality. 4
A number of studies had explored the association between VI and CFI.5–12 Jonas JB 6 et al. reported based on a cross-sectional study that the better the best-corrected visual acuity (BCVA), the less likely the cognitive function is to be impaired. Mine M 7 et al reported similar findings. However, most of the previous studies were cross-sectional studies,7–9 which were difficult to reveal the causal relationship due to the lack of longitudinal follow-up. In addition, conclusions from cohort studies are inconsistent with those from cross-sectional studies. Hong T 11 et al. reported that VI was not associated with cognitive function decline over a five-year follow-up. Clarification of the relationship between VI and CFI is important and requires more evidence based on cohort studies. In this study, we intend to explore whether VI has a significant impact on CFI by comparing the occurrence of CFI after six years in subjects with and without VI at baseline, and reasonably considering relevant confounding factors.
Materials and methods
Study design
Participants in the present study are a subset of the Handan Eye Study (HES), which is a population-based cohort study. In the HES study, 6,830 subjects aged ≥ 30 years were recruited in October, 2006 to October, 2007 (baseline) and 5,394 subjects completed the follow-up measurement that conducted six-year later in October, 2012 to October, 2013. No other follow-up was performed except for the six-year follow-up. The details of HES was described elsewhere. 13
Ethics approval and consent to participate
The HES was approved by the ethical committee of Beijing Tongren Hospital (Ethical approval number TREC2006-22). The study was carried out in accordance with the principles of the Declaration of Helsinki. Informed consent was obtained.
The inclusion and exclusion criteria
The subjects in this study were selected from the HES study, the exclusion criteria were: 1) Lost to follow-up. 2) Death. 3) Didn’t complete MMSE examinations, or visual acuity measurement, or other required ophthalmic examinations mentioned above. The inclusion criteria were: 1) Participants who completed the Mini-Mental state Examination (MMSE) measurement at both the baseline stage and the follow-up stage. 2) Participants who completed the visual acuity measurement at the baseline stage. 3) Participants who had clear and readable eye fundus images. 4) Participants who completed required ophthalmic examinations, including intraocular pressure, visual acuity, refractive error, fundus photography, slit lamp inspection.
In the HES study, only people over 50 years old were required to take the MMSE examination, so age was the main reason why some subjects did not complete the MMSE examination.
Measurements and definitions
Outcome measurements
Cognitive function was measured using MMSE test, which is a short test with 30 questions assessing participants’ general cognitive state from following dimensions: spatial orientation (“Where are you now?” “What state are you in?” “County?” “City?” “What is the name of this place?”), temporal orientation (“What is today's date?” “Month?” “Day of the week?” “Year?”), immediate memory and evocation memory (participants need to repeat names of three objects immediately after demonstration, and need to recall them after several minutes), attention and calculation (count backwards from 100 by sevens), and language (including naming, repetition, reading, and spontaneous writing). Total scores of MMSE range from 0 to 30.
The MMSE is one of the most widely used instrument for measuring cognitive function.14–17 MMSE comprehensively evaluates cognitive function from multiple dimensions. It has been proved to have high sensitivity and specificity in detecting cognitive function impairment. 17
Measurement of visual acuity and definition of VI
Visual acuity was measured using the LogMAR number chart under standardized lighting conditions at a distance of 4 meters. If the participants cannot identify any numbers at 4 m, they need to move to the distance of 3 m, 2 m, or 1 m. If the number is still not recognized, then the following measurement will be performed in turn: fingers counting, hand motions, light perception. The best corrected visual acuity (BCVA) of the better eye <20/60 was defined as VI. 18
Diagnosis of ocular diseases
Glaucoma was defined using the definition developed by the International Society for Geographical and Epidemiological Ophthalmology (ISGEO). 19 Cataract was assessed by ophthalmologists with slit lamp microscopy examination after pupil dilation using the Lens Opacification Classification System III. 20 The presence of diabetic retinopathy (DR) was assessed from the retinal fundus images using the modified Airlie House classification system for the Early Treatment of Diabetic Retinopathy. 21 Early age-related macular degeneration (AMD) was defined as presence of either 13 : (1) large indistinct soft or reticular drusen, or (2) both large distinct soft drusen and retinal pigmentary abnormalities. Late AMD was defined as the presence of geographic atrophy (GA) or neurovascular AMD. Presence of newly developed ocular diseases is defined as that subjects had none of the following ocular diseases (cataract, DR, AMD, Glaucoma, and central retinal vein occlusion) at baseline, but had them at follow-up. The ophthalmological examinations were performed at both the baseline and the six-year follow-up.
Cognitive function was measured by MMSE examinations. CFI was defined as a negative change in MMSE score from the baseline to follow-up. In the present study, we also did additional analysis, where we took negative change of MMSE score of 3 points as the cut-off value to define CFI, because it was reported that a change in MMSE of at least 2–4 points indicated a reliable change at the 90% confidence level. 22 Measurements of demographic information and lifestyle risk factors were completed using a structured questionnaire, described in detail elsewhere.13,23
Statistical analysis
Shapiro-Wilk test was used to check whether the continuous variables were normally distributed or not. Variables subject to normal distribution were described by means and standard deviation (SD), otherwise, the median and inter-quartile range (IQR) were used. The T-test was used to compare continuous variables between participants with and without VI at baseline. The Chi-square test was used to compare categorical variables between participants with and without VI at baseline. Logistic regression model was used to explore the relationship between VI and CFI, and confounding factors were adjusted in multivariable Logistic regression model. All the analysis was done using an open source R program (Version 4.0.0). The significance level was set to be 0.05, two tailed.
Results
Characteristics of included participants
Initially, there were 6830 participants in the HES. 5394 completed the six-year follow-up. 1436 who didn’t complete the follow-up were excluded, including 507 death and 929 lost to follow-up.1624 who didn’t complete the MMSE measurement were further excluded. 438 without readable eye fundus images were also excluded. In addition, 35 without measurement of visual acuity were excluded. Finally, a total of 3297 participants were included in this study (Figure 1). The average age of the participants in this study was 58.5 ± 7.2 years (Table 1), male accounted for 1480 (44.9%) of all participants. 351 (10.7%) were employed. Only 803 (24.4%) finished middle school or higher education. 2914 (88.4%) were married. 2824 (85.6%) of the subjects had an annual income of less than 5000 RMB. 893 (27.1%) were current smokers, 491 (14.9%) of the subjects had a drinking habit. The mean systolic pressure of the subjects were 144.5 ± 22 mmHg. The mean body mass index of the subjects was 24.6 ± 3.8 Kg/m2. The mean blood glucose level was 5.9 ± 1.5 mmol/L. The mean MMSE score measured at baseline and follow-up were 24.3 ± 5.2 points and 23 ± 5.1 points respectively. 127 (3.9%) of the participants had VI at baseline.
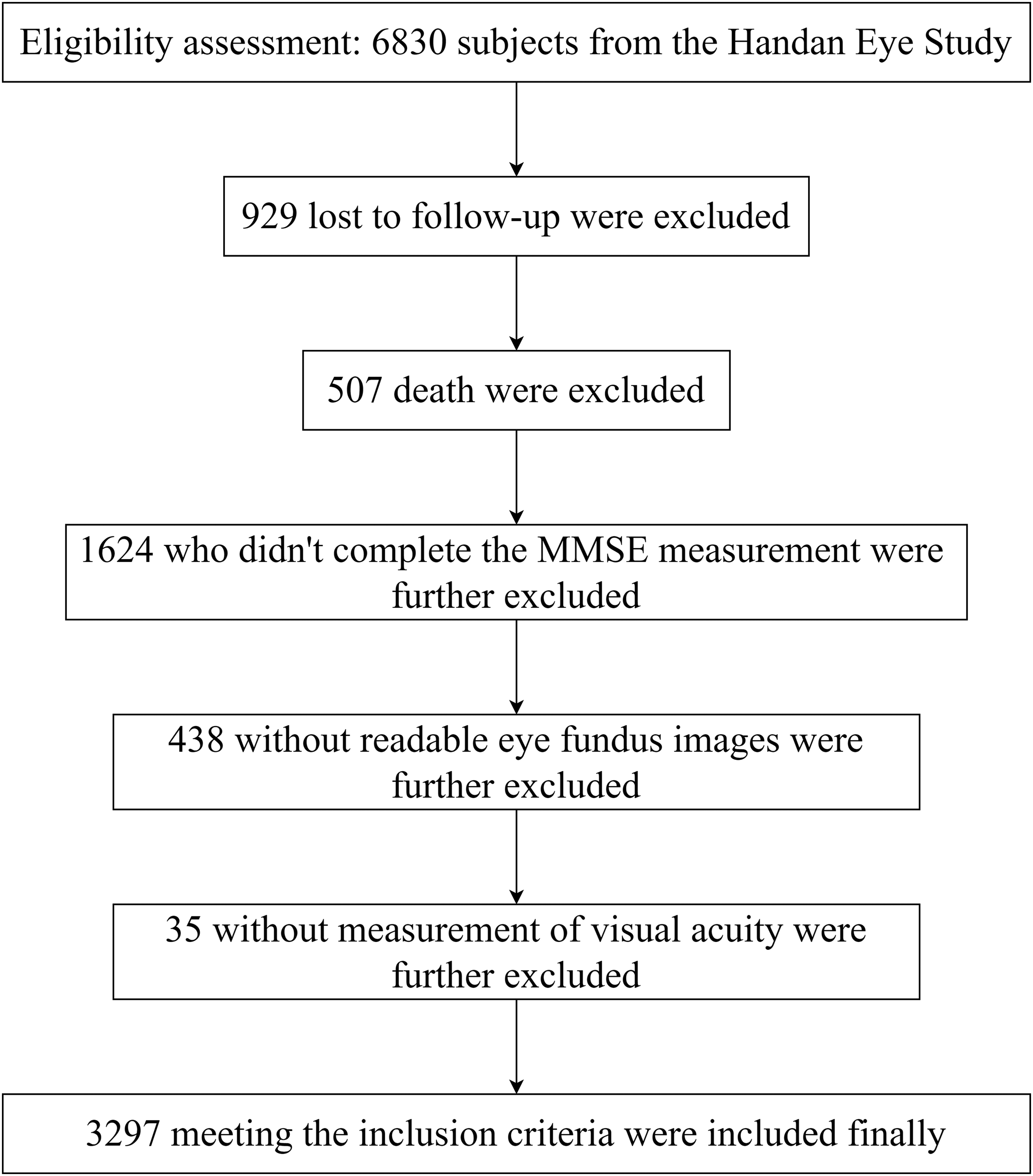
Flow chart of participants selection.
Characteristics of the included participants.
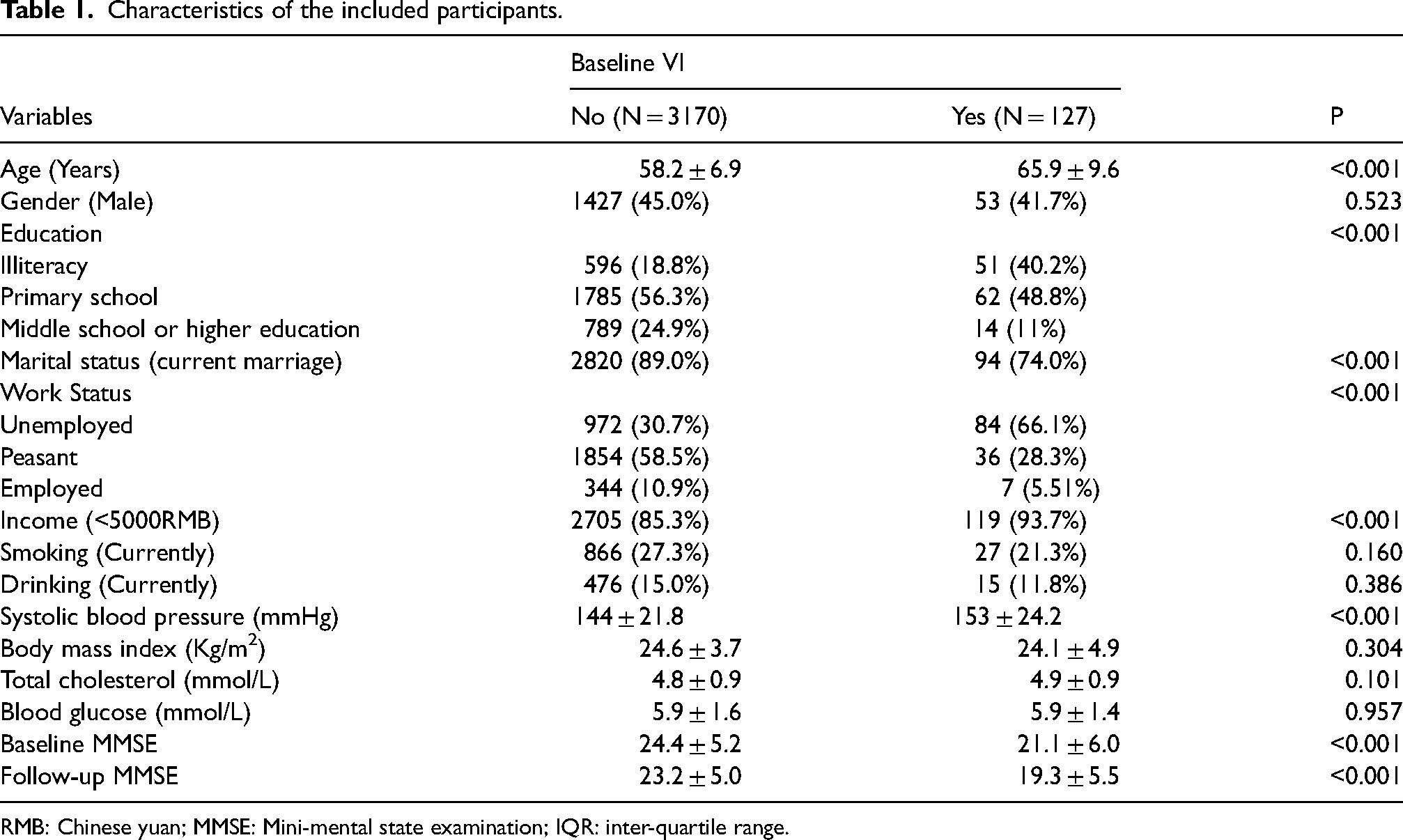
RMB: Chinese yuan; MMSE: Mini-mental state examination; IQR: inter-quartile range.
Compared with participants without VI at baseline, participants who had VI were older (p < 0.001), with higher proportion of illiteracy (p < 0.001), with lower proportion of marriage (p < 0.001), less employed (p < 0.001), lower income (p < 0.001), higher systolic blood pressure (p < 0.001), lower MMSE score (p < 0.001).
Six-year change in MMSE score
Participants were divided into two subgroups according to whether they had VI at baseline. During the six-year follow-up, MMSE scores decreased by 1.7 ± 3.3 points in participants with VI and 1.1 ± 3.3 points in participants without VI compared with the baseline. The difference was significant (t = 2.03, p = 0.040). The distribution of the six-year change in MMSE score of both groups was shown in Figure 2.
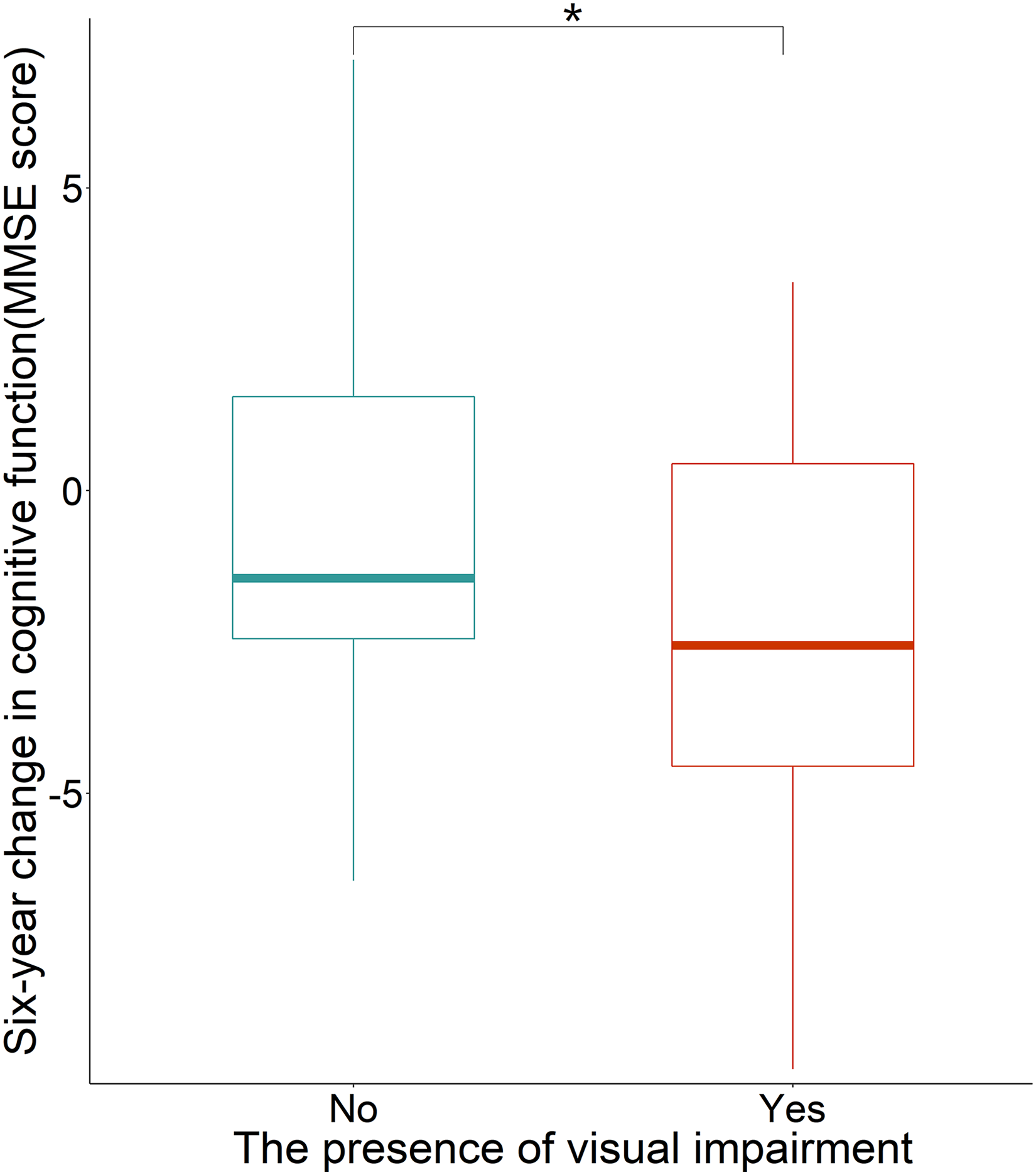
Distribution of the six-year change in cognitive function measured by Mini-mental state examination.
Relationship between VI and CFI
Results of the univariable Logistic regression models (Table 2) showed that 13 variables (age, gender, education,work status, income, smoking, drinking, systolic blood pressure, VI, history of cataract, history of glaucoma, history of diabetic retinopathy, and presence of newly developed ocular diseases during the six-year follow-up) were significantly associated with CFI. These 13 indicators were further put into the multivariable Logistic regression model (Table 2).
Risk factors of cognitive function impairment: multivariable logistic regression model.
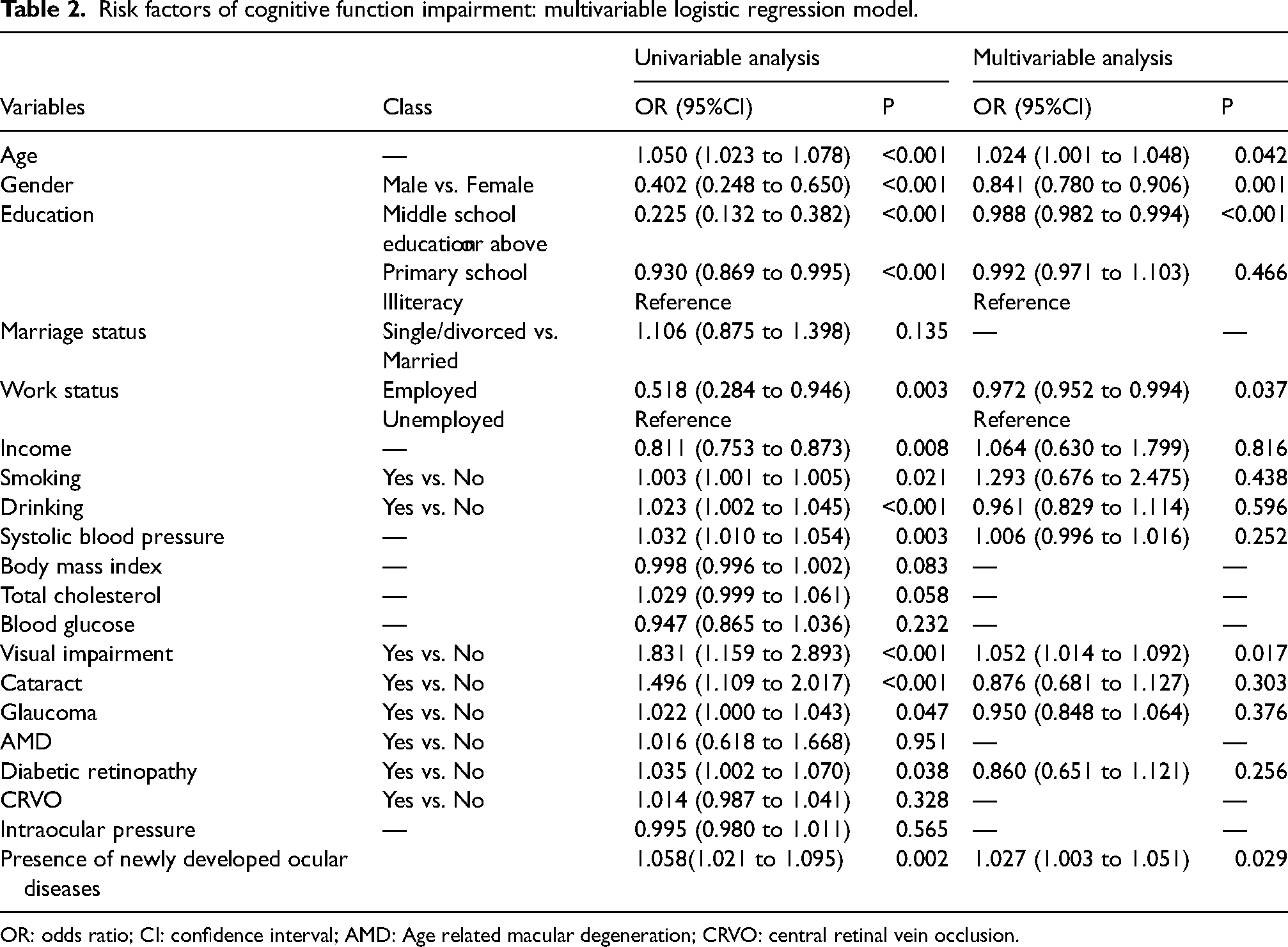
OR: odds ratio; CI: confidence interval; AMD: Age related macular degeneration; CRVO: central retinal vein occlusion.
Results of the multivariable Logistic regression model showed that age, VI, and the presence of newly developed ocular diseases were both risk factors of CFI, the odds ratios were 1.024 (95%CI: 1.001 to 1.048), p = 0.042 and 1.052 (95%CI: 1.014 to 1.092), p = 0.017, and 1.027 (95%CI: 1.003 to 1.051), p = 0.029, respectively. That is to say, with one year increase of age, the risk of CFI increases by 2.4%. The risk of CFI of participants with VI increases by 5.2% compared to those who have no VI. Participants who developed ocular diseases had 2.7% higher risk of CFI than those who didn’t develop ocular diseases during the six-year follow-up. Male gender (male vs. female), higher education (Middle school education or above vs. illiteracy), and work status (employed vs. unemployed) were protective factors of CFI. The odds ratios were 0.841 (95%CI: 0.780 to 0.906), p = 0.001, 0.988 (95%CI: 0.982 to 0.994), p < 0.001, and 0.972 (95%CI: 0.952 to 0.994), p = 0.037, respectively. The risk of CFI in men is 15.9% lower than that in women. Compared with the illiteracy, subjects with middle school education or above have a 1.2% lower risk of CFI. The employed have a 2.8% lower risk of CFI than those unemployed.
In the additional analysis (Appendix 1), BCVA was quantitatively analyzed and showed the same results as in Table 2. That is, age and the presence of newly developed ocular diseases are both risk factors of developing CFI, while better BCVA, higher education, male gender, and employment are protective factors for CFI. We also conducted a supplementary analysis (Appendix 2), using the change in MMSE score to three points as the cut-off value for defining CFI, and reached the same conclusion.
Discussion
The present study aimed at investigating whether VI had an effect on CFI through a six-year follow-up. The main findings were: 1) 127 (3.9%) of the elderly in rural area of China were visually impaired. 2) The decline rate of the MMSE score was nearly 0.3 points/year and 0.2 points/year for subjects with or without VI, respectively. 3) VI was an independent risk factor for CFI.
In the present study, the prevalence of VI was close to that of urban India 24 but higher than that of the united states or Japan.25,26 The reasons may be manifold. On one hand, urban residents have higher income and more access to health services, which reduces the risk of VI to a certain extent. On the other hand, part of the reason may be that the average age of the participants in this study was older than that of previous studies. Overall, participants’ mean MMSE score was 24.3 points at baseline, and decreased to 23 at the six-year follow-up. Considering the age of the participants, the MMSE score of the participants in this study was lower than that of previous studies, and decreased at a faster speed. In 2005, Zhang Q 27 et al. surveyed 2603 Chinese adults aged ≥ 64, the average MMSE score was 27.1 points, and dropped to 24 points ten years later. Li W 28 et al. followed up 3246 Chinese elders (aged ≥ 60) for six years, and found that the MMSE score decreased from 26 points to 25.8 points on average. In contrast, the cognitive function of the participants in the present study was worse, this may partly because the participants in this study came from rural area, most of them had low educational level and most of them were unemployed. While lower education and unemployment are risk factors for CFI, as discussed below.
The present study found age was a risk factor of CFI, besides, female had a higher risk of CFI than male. Miyawaki CE 29 et al. reported similar findings that among the oldest adults (80 to 116 years), women were twice as likely to be cognitively impaired as men (32.9% vs. 15.7%). Zhang Z 30 reported that Chinese women were more susceptible to cognitive impairment than men. Age was also reported to be a risk factor for CFI in previous studies.27,31 The mechanism of decline in cognitive function with age is not well understood, it has been suggested that the changes in white matter and declines in neurotransmitter levels with aging maybe associated with the changes in cognitive function. 32 One widely accepted hypothesis is that the deposition of amyloid-β in the brain with aging is one of the key pathological features of cognitive impairment.33,34
It has been reported that education was an important influence factor for cognitive function.31,35–37 Leggett A 36 et al. suggested that increasing access to education may help reduce the risk of cognitive impairment later in life. Another cohort study 37 found education contributed to a 15.8% reduction in CFI cases over 16 years of follow-up. Our findings are consistent with previous researches in which middle school education or above reduced the risk of CFI by 1.2% compared to illiteracy. Our study also shows that employment appears to be a protective factor for cognitive function, reducing the risk of CFI by 2.8% compared to unemployment. This makes sense because most jobs require mental activity, which has been reported to reduce the risk of cognitive impairment.38–40 Qiu JY 39 et al. found that cognitive leisure activities helped reduce the risk of CFI among the Chinese elderly based on 16 years follow-up. A randomized controlled trial 40 reported a significant improvement in overall cognitive function in 126 cognitively impaired, inactive older adults who conducted mind-body activity for 12 weeks. The mechanism by which mental activity helps reduce the risk of CFI can be explained by the concept of “brain reserve,” in which people who engage in intellectual activity have more brain reserve and less age-related hippocampal atrophy. 41 In addition, mental activity promotes the formation of new dendrite branches and synapses, which helps deepen the brain's ability to enhance the brain’s network of capillaries, and absorb new neurons. 41 On the other hand, most jobs requires not only mental activity but also physical activity, which has been reported to help upregulate brain-derived neurotrophic factor (BDNF). 42 While BDNF plays an important role in the growth and maintenance of cognitive neurons and contributes to improved cognitive function. 43
In recent years, not only the ophthalmologists, but also brain researchers begun to pay attention to the close relationship between VI and CFI. It was reported that VI could predict CFI in patients with Parkinson’s disease.44–46 Gbessemehlan A 47 et al. suggested that improving vision might be an easy way to decrease the incidence of cognitive disorders. Several ophthalmology studies reported similar results.5,7 Zheng DD 10 et al. suggested that maintaining good vision might be an important intervention for alleviating age-related cognitive decline. Hu W 48 et al. also reported that VI was an independent risk factor for incident dementia. Our results are consistent with previous reports, through a six-year follow-up, we found that VI increased the risk of CFI by 15.9% for the elderly in Chinese rural area. The mechanism by which VI affects cognitive function is unclear. In terms of structure and morphology, the microstructure and morphology of white matter as well as the macroscopic structure of patients with poor vision were more extensively changed than those with normal vision. 45 One hypothesis is that VI reduces the ability of the elderly to engage in activities that maintain health and leads to reduced brain stimulation, which may be a risk factor for cognitive decline.49,50 Another hypothesis goes that both VA and cognitive decline may share the common cause, such as age, inflammation or deterioration of central nervous function.51–53
In summary, VI is an independent risk factor for CFI in the elderly in Chinese rural area. To be specific, the presence of VI could increase the risk of CFI by 15.9% compared to participants without VI.
Strength and limitation
The strength of the present study includes a relatively large sample size, and the prospective cohort study design. The limitation lies in that the data was relatively old, and MMSE examination was only performed in part of the subjects, which might cause selection bias. Besides, SD-OCT, and examinations on colour vision, contrast sensitivity and visual field was not performed in this study, although the results are of important reference value.
Supplemental Material
sj-docx-1-ejo-10.1177_11206721231169613 - Supplemental material for Visual impairment as a risk factor of cognitive function impairment: A six-year cohort study
Supplemental material, sj-docx-1-ejo-10.1177_11206721231169613 for Visual impairment as a risk factor of cognitive function impairment: A six-year cohort study by Kai Cao, Jie Hao and Ning-Li Wang in European Journal of Ophthalmology
Supplemental Material
sj-docx-2-ejo-10.1177_11206721231169613 - Supplemental material for Visual impairment as a risk factor of cognitive function impairment: A six-year cohort study
Supplemental material, sj-docx-2-ejo-10.1177_11206721231169613 for Visual impairment as a risk factor of cognitive function impairment: A six-year cohort study by Kai Cao, Jie Hao and Ning-Li Wang in European Journal of Ophthalmology
Footnotes
Ethics approval and consent to participate
The study protocol of HES was reviewed and approved by the ethical committee of Beijing Tongren Hospital (Ethical approval number TREC2006-22). The research was conducted according to the tenets of the Declaration of Helsinki. The written informed consents from the participants were obtained before taking apart.
Authors’ contributions
(I). Conception and design: Ning-Li Wang (II). Administrative support: Ning-Li Wang (III). Provision of study materials or patients: Ning-Li Wang (IV). Collection and assembly of data: Kai Cao, Jie Hao (V). Data analysis and interpretation: Kai Cao (VI). Manuscript writing: All authors (VII). Final approval of manuscript: All authors.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the grants from the Ministry of Science and Technology of China (No. 2007CB512201).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.