
Abstract
Objectives
To compare changes in corneal biomechanical parameters one year after corneal cross-linking (CXL) in keratoconus (KCN) eyes of different severities.
Methods
Seventy-five eyes with mild, moderate, and severe grades of KCN (n = 24, 31, and 20 eyes, respectively) that were treated with CXL, based upon the standard Dresden protocol, were included. The corneal biomechanical assessment was performed using Corvis ST and Ocular Response Analyzer (ORA). Changes in Corvis's dynamic corneal response (DCR) parameters and ORA's derived parameters (corneal hysteresis (CH), and corneal resistance factor (CRF)) were assessed whilst the corneal thickness and intraocular pressure were considered as covariates.
Results
There was no statistically significant difference in the corneal biomechanical parameters obtained using both devices after surgery separately in different KCN grades, except for the deformation amplitude (DA) in the severe KCN group (P = 0.017). Changes in the classic parameters of the highest concavity phase of Corvis ST (peak distance, radius, and DA) were more positive and in the newer parameters (integrated inverse radius (IIR), deformation amplitude ratio (DAR)) more negative in the severe group compared to the other groups. Also, the mean change in CH (P = 0.710), and CRF (P = 0.565), showed a negative shift in higher grades of KCN; however, there was no significant difference in the mean changes of all parameters between different groups. (P > 0.05)
Conclusions
Similar changes in the Corvis ST and ORA parameters in mild, moderate, and severe KCN indicate biomechanical stability and the effective role of CXL in stopping the progressive nature of keratoconus in eyes of varying severities one year after CXL.
Introduction
Keratoconus (KCN) is an ectatic corneal disease characterized by progressive corneal thinning and protrusion.1,2 Corneal biomechanical failure is considered a contributing factor in the development of this disease and following changes in the corneal geometrical properties and reduced visual quality.3,4 This disorder is a progressive disease and corneal cross-linking (CXL) is the only approved treatment option for this disease and other ectatic corneal disorders. CXL is increasingly used in the treatment of keratoconus and can reduce its progression, the associated considerable impairment of vision-related quality of life, and ultimately the financial burden and socio-economic problems of this disorder.5,6 Biomechanical and microstructural changes in corneal stroma through the photo-polymerization reaction in the CXL technique improve the mechanical strength of the cornea or corneal stiffness of the anterior corneal stroma,7,8 which has been confirmed in ex vivo and experimental studies, although these measurements differ from in vivo assessments due to the destruction of the natural state of the cornea. 9
There are several grading systems for KCN severity classification, one of which is the system designed based on the collaborative longitudinal evaluation of keratoconus (CLEK) study, which divided the KCN into mild, moderate, and severe grades. 10 There is a report that indicates more considerable flattening of the cornea in the more severe KCN group following CXL and attributes it to greater corneal haziness in this specific group. 11 Also, progressive flattening and thinning of the cornea after CXL caused by severe keratoconus was reported in one case report study. 12 Koh et al. in evaluating the correlation between the keratoconus severity and biomechanical parameter of the cornea assessed using Corvis ST reported a negative correlation between the deformation amplitude ratio and integrated radius with the radius of curvature of the cornea in a 3-mm zone on the front and back surface centered on the corneal thinnest point, and a positive correlation with these topometric corneal parameters with the stiffness parameter at the first corneal applanation. 13
The current literature appears not to contain a study comparing changes in corneal biomechanical parameters and corneal geometric parameters following CXL in different stages of KCN severity. Therefore, this study was designed to assess changes in corneal biomechanical parameters evaluated using two instruments available in clinics for in vivo assessment of corneal biomechanics one year after CXL in KCN eyes classified according to severity.
Methods
This comparative and cross-sectional study included 75 eyes from 75 keratoconus patients with an age range of 14 to 38 years who received CXL based on the standard Dresden protocol. In cases where one eye received CXL, that eye was included in the study, and in cases where both eyes received CXL, one eye was randomly selected. An experienced corneal specialist (MRS) diagnosed keratoconus based on slit-lamp exam findings, retinoscopy reflex, and data of corneal imaging techniques including topo/tomography pointing to an abnormal topography pattern, abnormal indices, and patterns on the elevation and thickness maps. Change in maximum keratometry or astigmatism of the cornea by one diopter or more in tomography (Scheimpflug), in thickness at the thinnest point by at least 30 microns, and report of subjective progression of visual deterioration over the past year were criteria for confirming the progressive state of disease.
The main inclusion criterion was that the patient had at least one eye with progressive keratoconus based on the presence of at least one of the aforementioned criteria and required CXL. Patients with scar or haze in the central cornea, corneal thickness thinner than 400 microns at the thinnest point, history of eye disorders other than keratoconus, history of eye/corneal surgery, history of systemic conditions (autoimmune disorders, diabetic mellitus, active atopic/allergic and herpetic diseases), and breastfeeding or pregnancy at the time of progression confirmation and one year after CXL were excluded from the study.
Before starting the study, the purposes and objectives behind the design of this study and the effects and complications of CXL were explained in simple terms and conscious written consent was obtained from all patients. In addition, all steps of this study were based on the tenets of the Declaration of Helsinki. The University Ethics Committee approved this study. (Code No: IR.SBMU.RETECH.REC.1399.324)
Along with a comprehensive ophthalmic examination, Placido-disk based corneal topography with TMS-4 (Tomey Corp, Nagoya, Japan), Scheimpflug corneal tomography using the Pentacam (Oculus; Wetzlar, Germany), and corneal biomechanical assessments with Corvis ST (Oculus; Wetzlar, Germany) and Ocular Response Analyzer (ORA, Reichert Ophthalmic Instruments, Buffalo, NY, USA) were performed before and one year after CXL.
Included variables were uncorrected and corrected distance visual acuity (UDVA & CDVA) recorded in the logarithm of the minimum angle of resolution (LogMAR), and mean spherical equivalent (MSE = sphere + (cylinder/2)). In addition, Pentacam-derived variables were mean keratometry and corneal asphericity (expressed as the Q-value) on both corneal surfaces; the front surface maximum keratometry (Kmax), central corneal thickness (CCT), thickness at the thinnest corneal point (TP), and Belin-Ambrósio enhanced ectasia total deviation (BAD-D).
Recorded corneal biomechanical parameters were Corvis ST's dynamic corneal response (DCR) parameters associated with intra-ocular pressure (IOP) including length (AL1 & 2) and velocity (AV1 & 2) during the first and second applanation, the distance between the two peaks (PD: peak distance), axial displacement of the apex of the cornea (deformation amplitude (DA) and central radius of the cornea (R) at the highest concavity phase; and ORA’ derived parameters including corneal hysteresis (CH), corneal resistance factor (CRF), corneal compensated IOP (IOPcc) and Goldmann correlated IOP (IOPg). In addition to the standard Corvis ST’ DCR parameters, the new parameters including stiffness parameter at first applanation (SP-A1), integrated inverse radius (IIR), and deformation amplitude ratio (DAR = DA at the apex/ average of DA at 2 mm around the center in the two horizontal directions) were also recorded.
According to the collaborative longitudinal evaluation of keratoconus (CLEK) study's criterion and steep keratometry reading (KRs) obtained using TMS-4 topographer, the keratoconus was classified into mild (KRs < 45 D), moderate (45 ≤ KRs ≥ 52), and severe (KRs > 52 D) groups. 10
All treatments were performed by the same surgeon (MRS) according to the standard Dresden protocol (SCXL [3 * 30]) using an optical system (UV-X; Peschke Meditrade GmbH, Huenenberg, Switzerland) in the following steps: mechanical removal of corneal epithelium on a 9 mm diameter; administration of riboflavin 0.1% in 20% dextran every 2 min for 30 min to achieve proper stromal saturation of the cornea checked by riboflavin fluorescence using slit-lamp examination; 30 min ultraviolet-A light (λ = 365 nm) application with irradiance of 3 Mw/cm2 to the central 8 mm of the cornea and simultaneous continuation of riboflavin administration every 5 min during the last stage.
Data were analyzed in SPSS.22 software (SPSS, Chicago, IL, USA) after assessing the normality of quantitative data using the Kolmogorov-Smirnov test. The Wilcoxon signed ranks test was used to compare corneal biomechanical parameters before and after CXL in all subjects and separately in the mild, moderate, and severe keratoconus. The Kruskal-Wallis test was used to compare the changes in each biomechanical parameter between the different groups. A general linear model was used to compare Corvis ST and ORA's corneal biomechanical parameters in various keratoconus severity groups, while central corneal thickness (CCT), biomechanically corrected intraocular pressure (bIOP), and age were considered as covariates. Dunn-Bonferroni post hoc test was used for pairwise comparisons. The significance level was considered as P < 0.05 in all tests.
Results
Seventy-five eyes from 75 patients (37 males & 38 females) with a mean age of 21.6 ± 4.3 years were assessed. Mild, moderate, and severe KC was seen in 24 (32.0%), 31 (41.3%), and 20 (26.7%) eyes, respectively. The mean age in the mild, moderate, and severe groups was 22.1 ± 4.2, 21.7 ± 3.1, and 20.7 ± 5.9 years, respectively, with no statistically significant difference between groups. (P = 0.154)
There was no statistically significant difference in gender distribution between the three KC groups using the Chi-square test. (P = 0.637)
Mean and standard deviation of visual acuity and spherical equivalent, the IOPs measured using Corvis ST and ORA, and some geometrical corneal indices obtained using Pentacam before and one year after CXL separately in various keratoconus severities are presented in Table 1.
Mean and SD of visual acuity, spherical equivalent, IOP, keratometry, corneal asphericity, thickness, and BAD-D before and after CXL separately in different keratoconus grades. (n = 75 eyes).
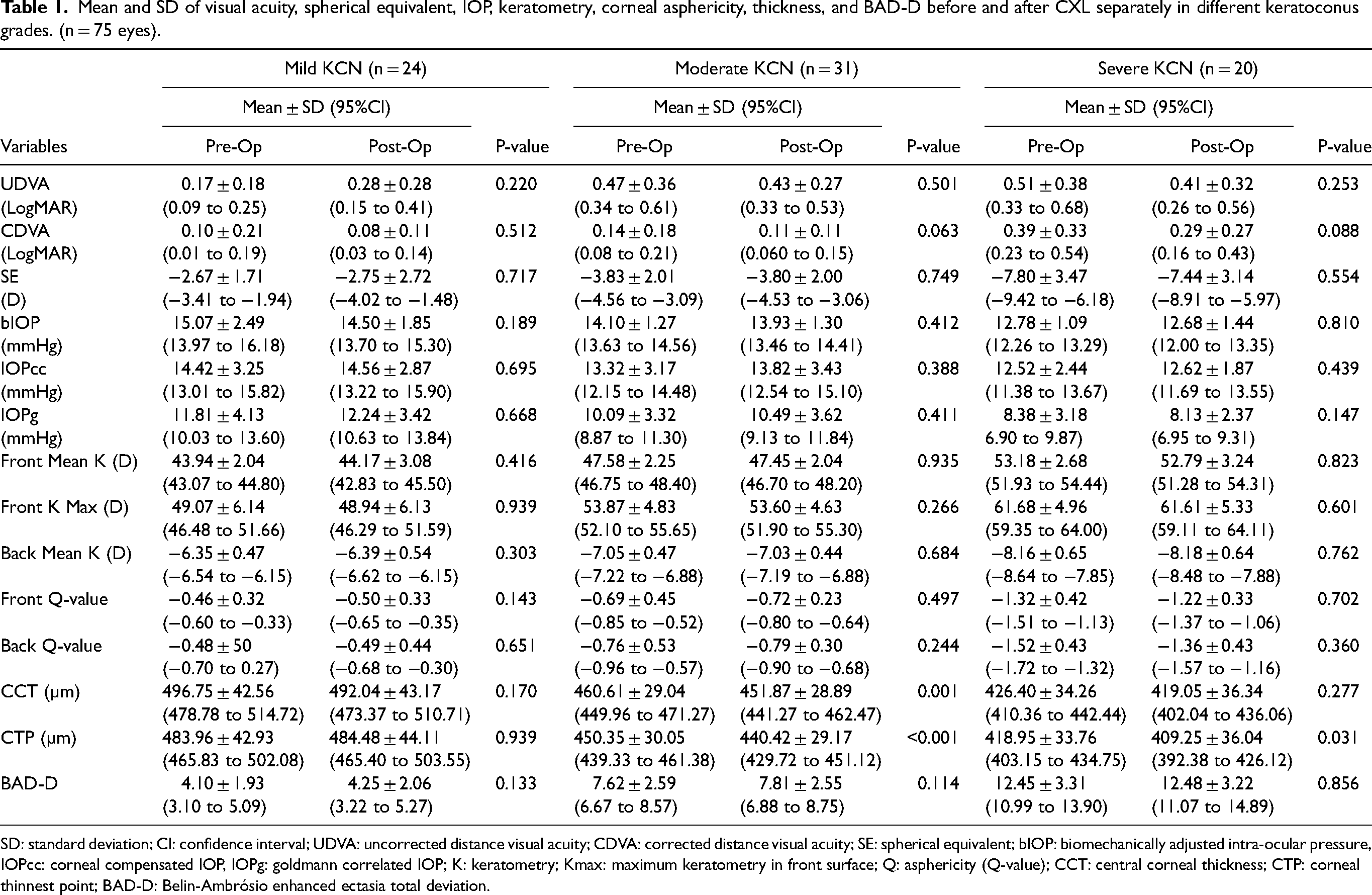
SD: standard deviation; CI: confidence interval; UDVA: uncorrected distance visual acuity; CDVA: corrected distance visual acuity; SE: spherical equivalent; bIOP: biomechanically adjusted intra-ocular pressure, IOPcc: corneal compensated IOP, IOPg: goldmann correlated IOP; K: keratometry; Kmax: maximum keratometry in front surface; Q: asphericity (Q-value); CCT: central corneal thickness; CTP: corneal thinnest point; BAD-D: Belin-Ambrósio enhanced ectasia total deviation.
There was no statistically significant difference in the mean uncorrected and corrected VA, MSE and the IOPs measured using both devices before and one year after CXL using the Wilcoxon signed ranks. (P > 0.05) Wilcoxon signed-ranks test did not show significant flattening in mean keratometry and corneal asphericity at both corneal surfaces, maximum keratometry in the front corneal surface, and BAD-D after CXL separately in all groups. (P > 0.05) Thickness comparison pre- and post-CXL showed a significant difference only in CCT for the moderate KCN group (P = 0.001) and in CTP for the moderated (P < 0.001) and severe (P = 0.031) groups.
The mean changes (postoperative – preoperative values) in VA, MSE, the IOPs obtained using Corvis ST and ORA, and some geometrical corneal indices using Pentacam following CXL separately in various KCN grades are presented in Table 2.
Mean and standard deviation of changes in VA, SE, IOP, keratometry, corneal asphericity, thickness, and BAD-D using Pentacam following CXL separately in mild, moderated, and severe KN groups. (n = 75 eyes).
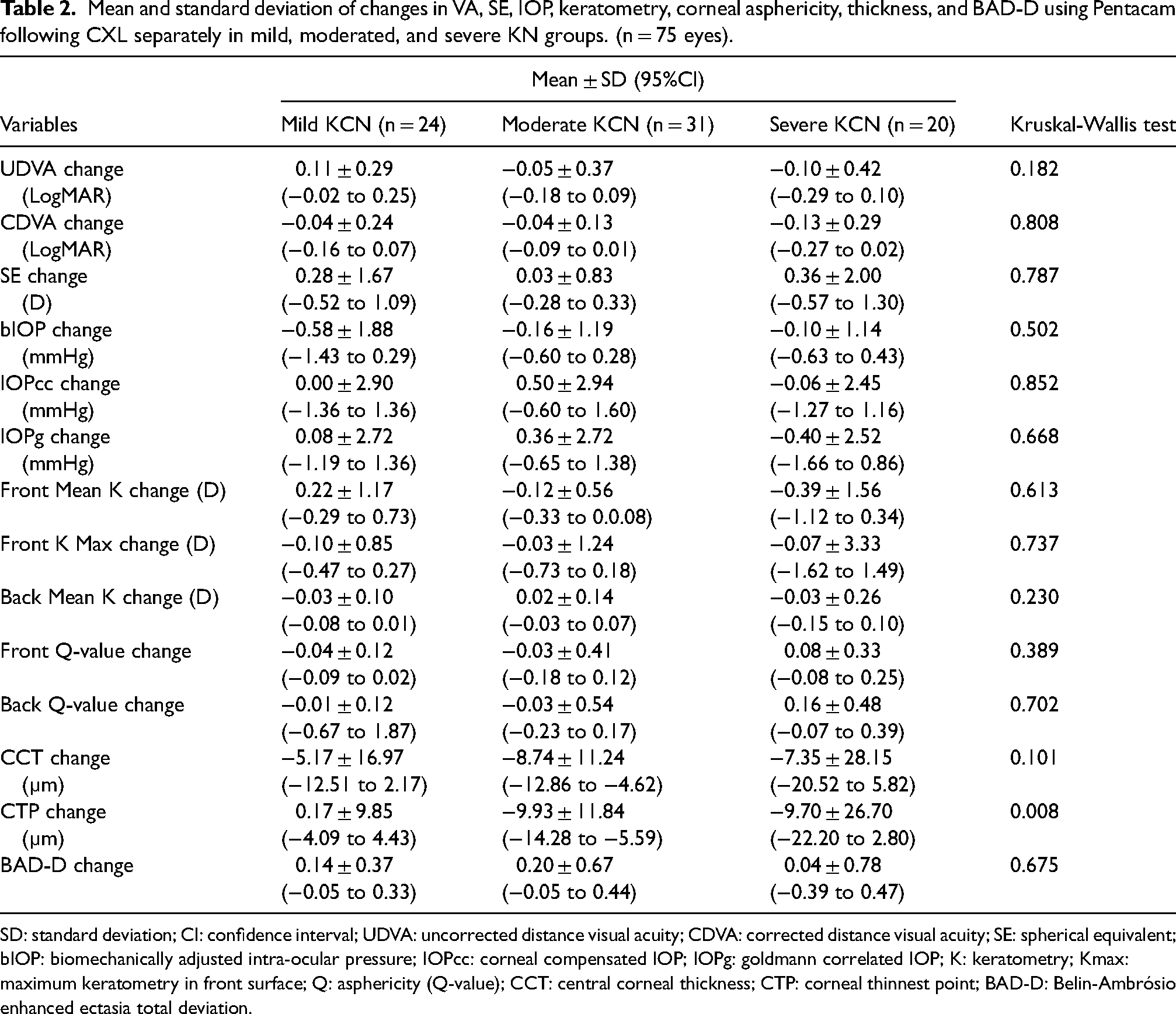
SD: standard deviation; CI: confidence interval; UDVA: uncorrected distance visual acuity; CDVA: corrected distance visual acuity; SE: spherical equivalent; bIOP: biomechanically adjusted intra-ocular pressure; IOPcc: corneal compensated IOP; IOPg: goldmann correlated IOP; K: keratometry; Kmax: maximum keratometry in front surface; Q: asphericity (Q-value); CCT: central corneal thickness; CTP: corneal thinnest point; BAD-D: Belin-Ambrósio enhanced ectasia total deviation.
Although the observed acuity changes were approximately two more lines in the CDVA and one more line in the UDVA one year after CXL in the severe group compared to the mild group; however, these changes were not statistically significant different using the Kruskal-Wallis test. (P > 0.05) The changes obtained in MSE were 0.28 D, 0.03 D, and 0.36 D in the direction of less myopia in mild, moderate, and severe KCN groups, respectively. Kruskal-Wallis test showed no significant difference in MSE and IOP among different groups. (P > 0.05)
Mean keratometry changes in the front corneal surface in mild, moderate, and severe KCN groups 0.22 D, −0.12 D, −0.39 D and in the maximum keratometry were −0.10 D, −0.03 D, and −0.07 D, respectively. Corneal asphericity changes in both corneal surfaces were in the more prolateness direction in mild and moderate groups, while the severe group showed changes 0.08 and 0.16 in the less prolateness direction in the front and back surfaces, respectively. However, changes in all corneal shape and thickness parameters and BAD-D showed no statistically significant difference using the Kruskal-Wallis test (P > 0.05), except for corneal thickness at the thinnest (P = 0.008) points among various severity groups. Dunn-Bonferroni post hoc test showed a significant difference in mean CTP between mild with moderate KCN groups. (P = 0.005)
The mean and standard deviation of corneal biomechanical parameters assessed using Corvis ST and ORA before and after CXL in three KCN groups are shown in Table 3.
Mean and SD corneal biomechanical parameters using corvis ST and ORA pre- and post-CXL separately in different KCN severity grades. (n = 75 eyes).
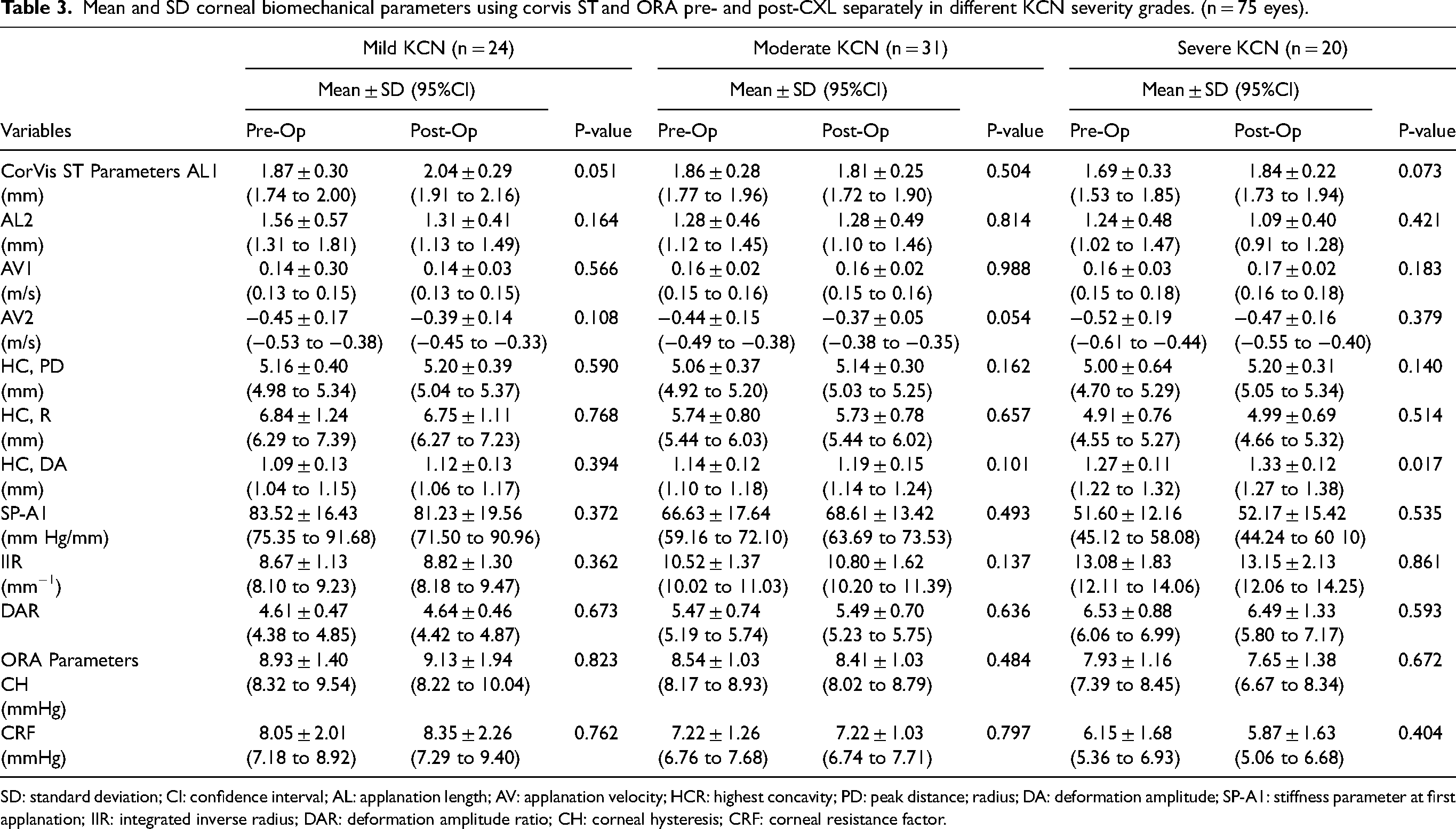
SD: standard deviation; CI: confidence interval; AL: applanation length; AV: applanation velocity; HCR: highest concavity; PD: peak distance; radius; DA: deformation amplitude; SP-A1: stiffness parameter at first applanation; IIR: integrated inverse radius; DAR: deformation amplitude ratio; CH: corneal hysteresis; CRF: corneal resistance factor.
Considering the corneal biomechanical parameters obtained using Corvis ST and ORA, there was no statistically significant difference in comparing the mean of each parameter before and after surgery separately in different KCN grades except the deformation amplitude (DA) in the severe KCN group (P = 0.017) using the Wilcoxon signed rank test.
The mean changes in DCR parameters obtained using Corvis ST and the pressure-derived parameters of ORA following CXL separately in three KCN grades while CCT, bIOP, and age were considered as covariates are presented in Table 4.
Mean and standard deviation of changes in corneal biomechanical parameters using corvis ST and ORA after CXL separately in different KCN severity grades and CCT, bIOP, and age as covariates. (n = 75 eyes).
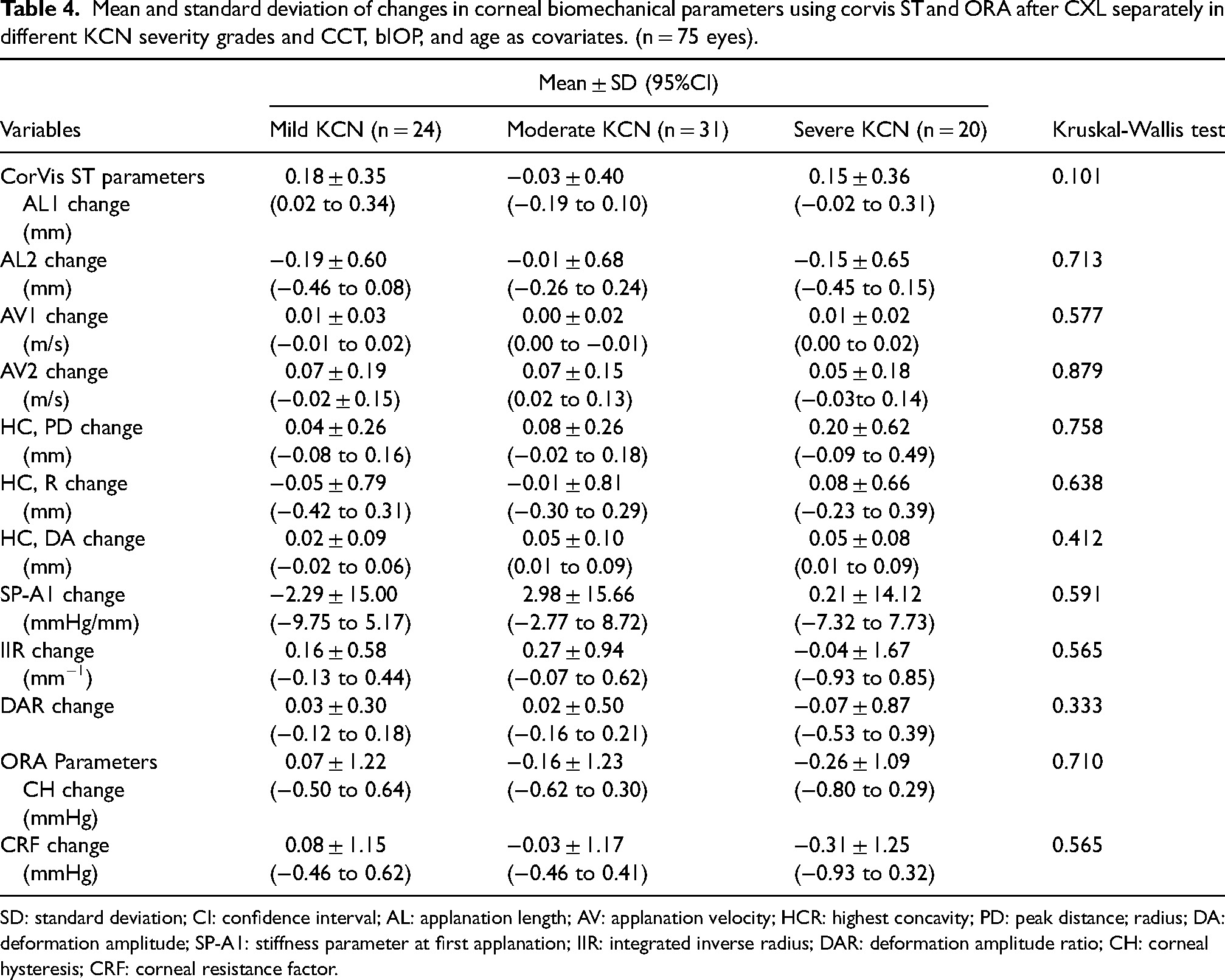
SD: standard deviation; CI: confidence interval; AL: applanation length; AV: applanation velocity; HCR: highest concavity; PD: peak distance; radius; DA: deformation amplitude; SP-A1: stiffness parameter at first applanation; IIR: integrated inverse radius; DAR: deformation amplitude ratio; CH: corneal hysteresis; CRF: corneal resistance factor.
Comparison of the observed changes in the biomechanical parameters of Corvis ST showed that the highest and lowest changes were related to the stiffness parameter at first applanation and the velocity of corneal apex during the first applanation in all grades of KCN, respectively. Changes in the classic highest concavity parameters of Corvis ST (PD, R, and DA) were more positive and in the newer parameters (IR, DAR) more negative in the severe group compared to the other groups. However, the Kruskal-Wallis test did not show a significant difference in the mean changes of Corvis ST's biomechanical parameters between different groups. (P > 0.05)
Although the mean change in pressure-derived parameters of ORA, CH (P = 0.710), and CRF (P = 0.565), showed a negative shift associated with higher grades of KCN severity; however, the changes did not show a statistically significant difference among the different groups.
Discussion
The current study showed that CXL is an effective option to halt the progressive nature of keratoconus and to provide visual and structural stability in keratoconus with various severities by comparing the visual, refractive status, corneal geometrical, and biomechanical parameters before and one year after treatment for patients of different severity of KCN. These results compare well with previous studies. Our four-year longitudinal study of corneal biomechanical parameters showed that CXL was able to increase corneal stiffness by creating new covalent bonds in the stroma and at least prevent further corneal weakening. 14 The present study was designed in a shorter period of time on keratoconus patients of the same race, in the same previous center and with similar imaging conditions, and showed that the observed changes in each DCR parameter of Corvis ST and ORA's pressure-derived parameter were not significantly different in mild, moderate, and severe KCN.
Visual acuity, although improved one year after CXL, did not show statistically significant changes. Visual stability based on the acuity measured at distance without and with the best correction in the mild, moderate, and severe KCN group was consistent with previous studies that reported stability of vision in both short- and long-term assessments of the CXL effect.14,15 Similar stability in the refractive status expressed by MSE was seen the same as the study by Tasci and colleagues in 5 years follow up after CXL. 16 Although significant changes in MSE or corrected distance visual acuity of the eye were reported in some studies 7 ; however, the absence of such a change does not indicate the ineffectiveness of CXL, as this technique is a corneal stabilizing method and not a refractive surgery technique method that aims to cause considerable changes in refraction. It was reported that CXL's effect on the refractive power is not via changes in the corneal curvature, but other factors such as changes in index of refraction and/or corneal hydration. 17
Unlike previous studies, there were no statistically significant changes in corneal shape parameters including keratometry reading and corneal asphericity one year after CXL separately in all KCN severity groups. These findings are consistent with Sedaghat et al. and Grewal et al.'s studies.14,18 Changes in the severe KCN group were similar to those in the other groups, although it was reported that an increased corneal flattening effect may be seen in advanced keratoconus associated with corneal haziness formation, which is more likely in these specific KCN cases after CXL.11,12
Decrease in CCT in the moderate group and CTP in moderate and severe groups after CXL are consistent with previous studies,19–21 although they reported these changes six months versus one year after treatment in the current study. It was reported that multiple scattering in the corneal stroma secondary to CXL may cause some artifacts in postoperative thickness measurement, 22 so that an OCT-based device provides a real pachymetry.
The stability of the disease status according to BAD-D in all KCN groups one year after CXL confirms the results of a previous study, in which this index was reported as a better indicator for evaluating the progression of keratoconus due to the consideration of several corneal parameters. 23
As reported, biomechanical alteration of the cornea is probably to be associated with the onset and development of KCN. 2 The current study did not show any statistically significant difference in all Corvis ST's DCR parameters before and one year after CXL separately for different grades of KCN severity, except for DA in the severe KCN group. This finding agrees with the Nielsen et al. study, which report a significant increase in HC-DA, 97 days after CXL, although their sample was not classified according to the severity of KCN.24,25 Similar finding was reported by comparing this parameter in keratoconus eyes with and without a history of CXL.
Considering the biomechanical parameters at the HC phase (PD, R, DA, IIR, and DAR), the increase in PD, R and the decrease in DA, IIR, and DAR are compatible with corneal stiffening.26,27 The highest changes in these parameters except IIR were seen in the severe KCN group, and the changes indicate non-significant improvement in the corneal mechanical strength except DAR and IIR compared to mild and moderate groups.
SPA1 is one parameter that is claimed to be a better indicator of the overall resistance to deformation, and higher values indicate a stiffer cornea biomechanically. 28 The mean changes in this parameter in the mild, moderate, and severe KCN groups were −2.29, 2.98, and 0.21 mmHg/mm, decrease in mild group and an increase in other groups, but these changes were not statistically significant. This finding is consistent with a previous study evaluating 4-year changes in corneal biomechanics after CXL, 14 and contrary to some previous studies.28–30 However, it demonstrates the fact that CXL prevented the progressive biomechanical failure of the cornea for at least one year postoperatively. Importantly, there was no difference in the effect of CXL on changes in this parameter in different groups of keratoconus severity.
The results of the current study did not show a significant increase in CH and CRF after CXL, despite the reported improvement in corneal stiffness in the in vitro evaluations, which is consistent with previous short- and long-term follow-ups following CXL.14,31–33 At higher severity grades of KCN, there was a non-significant reduction in both pressure-derived parameters of ORA, although these changes were not considerable between groups which was the main objective of the current study.
Changes in all Corvis ST and ORA indices in all KCN severity groups do not indicate an increase in corneal stiffness after CXL, so it seems more logical to evaluate changes in these parameters together with other indices such as BAD-D to evaluate the effects of CXL on the cornea. 24
The first limitation of this study was the small number of keratoconus eyes in each of the different severity groups, although the total number of subjects in the study met the sample size power calculation. Another limitation was the short-term follow-up and failure to investigate parameters derived from the ORA response curve waveform. Another weakness is not considering the effect of cone location on corneal biomechanical changes in different KCN groups, although this becomes quite difficult when added to the varying level of KCN severity and would have meant a very large cohort would be needed so that subjects could be divided according to KCN severity and also apex position. Assessment of the corneal biomechanical status after CXL in keratoconus eyes with differences in the rate/severity of progression, for example, considerable corneal thinning or other morphological changes within 3 months versus the same changes over a one-year period is an idea for future studies.
In conclusion, the present study showed similar effects of CXL according to the observed changes in each dynamic corneal response parameter of Corvis ST and ORA's pressure-derived in mild, moderate, and severe KCN. The observed corneal biomechanical stability in keratoconus eyes with various severities based on the biomechanical parameters one year after CXL demonstrated the effective role of this treatment option to halt the progressive nature of keratoconus. Visual and structural stability in mild, moderate, and severe keratoconus eyes is another evidence that points to the stabilizing role of the CXL technique.
Footnotes
Acknowledgement
All authors have equal contributions to this paper. The authors would like to thank the staff at Didar eye clinic and the participants who made this study possible. This research was supported by the Deputy of Research of Shahid Beheshti University of Medical Sciences (Code No.: IR.SBMU.RETECH.REC.1399.324).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.