
Abstract
Purpose
Acute angle-closure is a rare manifestation of choroidal metastasis. We reported a case of choroidal metastasis from lung adenocarcinoma presenting with unilateral acute angle-closure attacks relieved with radiotherapy after failed conventional medical and laser treatments. This represented the first detailed report of treatments of secondary acute angle-closure attacks in patients with choroidal metastasis
Case description
A 69-year-old female without ocular history was diagnosed with metastatic lung adenocarcinoma. One month later, she complained of blurred vision and pain in the right eye that lasted 2 days. IOP was 58 mmHg and best-corrected visual acuity (BCVA) was counting finger in the right eye. Slit-lamp examination revealed corneal edema with ciliary congestion, extremely shallow anterior chamber both centrally and peripherally, mid-dilated pupil and moderate cataract in the right eye. While the left eye was normal. B-scan ultrasound and orbital computed tomography showed an appositional choroidal detachment with an underlying choroidal thickening suggesting choroidal metastasis in the right eye. There was limited effect of medical and laser therapy. IOP was 9 mmHg in the right eye after two months of palliative external beam radiotherapy in the right orbit. BCVA was hand motion in the right eye. Slit lamp examination revealed clear cornea, deep anterior chamber in the right eye. Regression of choroidal detachment and choroidal metastasis in the right eye were observed in B-scan ultrasound.
Conclusion
This case demonstrated that patient with secondary acute angle-closure attacks from large bullous choroidal detachment related to choroidal metastasis could only be successfully treated with radiotherapy as both medical and laser therapy might not be capable of breaking angle-closure attacks.
Introduction
The prevalence rate of patients with metastatic disease with ocular involvement is around 8%-10%. 1 Choroid, due to its rich vascular supply, is the most common site of metastasis (88%). 2 Lung cancer, found in 20-29% of cases, represents as the second most common primary neoplasm that metastasize to choroid only after breast cancer (40-53%) and typically presents with unilateral involvement. 3 Although choroidal metastases (CM) may be controlled through local treatment, systemic prognosis is poor because it usually occurs in the later stages of the disseminated neoplasm, with cancer-related death in 54% of patients at one year following diagnosis. 4
Intraocular pressure (IOP) elevation secondary to CM is a rare manifestation of CM (1%), with secondary angle-closure recognized as the main mechanism. 5 It involves anterior displacement of lens-iris diaphragm by the force pushing from behind including large tumor in posterior segment, retinal detachment or choroidal detachment. 5 We reported on a patient with lung adenocarcinoma who has CM presenting with unilateral acute angle-closure attacks refractory to medical and laser treatment. The literature review of the previously reported patients with CM with acute angle-closure attack in the English-language literature were discussed.
Case presentation
A 69-year-old female was diagnosed with metastatic lung adenocarcinoma (T4N3M1) in January 2020, with lung, liver, bone and brain involved. She was commenced on gefitinib since diagnosis. She denied any ocular history including ophthalmic surgery, ocular trauma or ophthalmic medications. One month later, she complained of blurred vision and pain in the right eye that lasted 2 days. Best-corrected visual acuity (BCVA) was counting finger at 60 cm in the right eye and 0.7 in the left eye. IOP was 58 mmHg in the right eye and 26mmHg in the left eye. Slit-lamp examination revealed corneal edema with ciliary congestion, extremely shallow anterior chamber both centrally and peripherally, mid-dilated pupil and moderate cataract in the right eye. Clear cornea, deep anterior chamber and mild cataract were recorded in the left eye. The IOPs in the left eye were normal in the following visits. Gonioscopy of right eye demonstrated that the angle seemed to be closed without any identifiable angular structure. Fundus examination was blurry in the right eye while left eye was normal. B-scan ultrasound showed an appositional choroidal detachment with an underlying choroidal thickening with medium to high internal acoustic reflectivity in the right eye (Figure 1A) and orbital computed tomography (CT) revealed the presence of choroidal detachment and hyperdense choroidal thickening with contrast enhancement of the right eye (Figure 1B and 1C). T2-weighted and fluid-attenuated inversion recovery (T2-FLAIR) magnetic resonance imaging (MRI) performed two months ago demonstrated an enhanced posterior choroidal thickening with elevated lesion on the right posterolateral globe suggesting CM (Figure 1D).
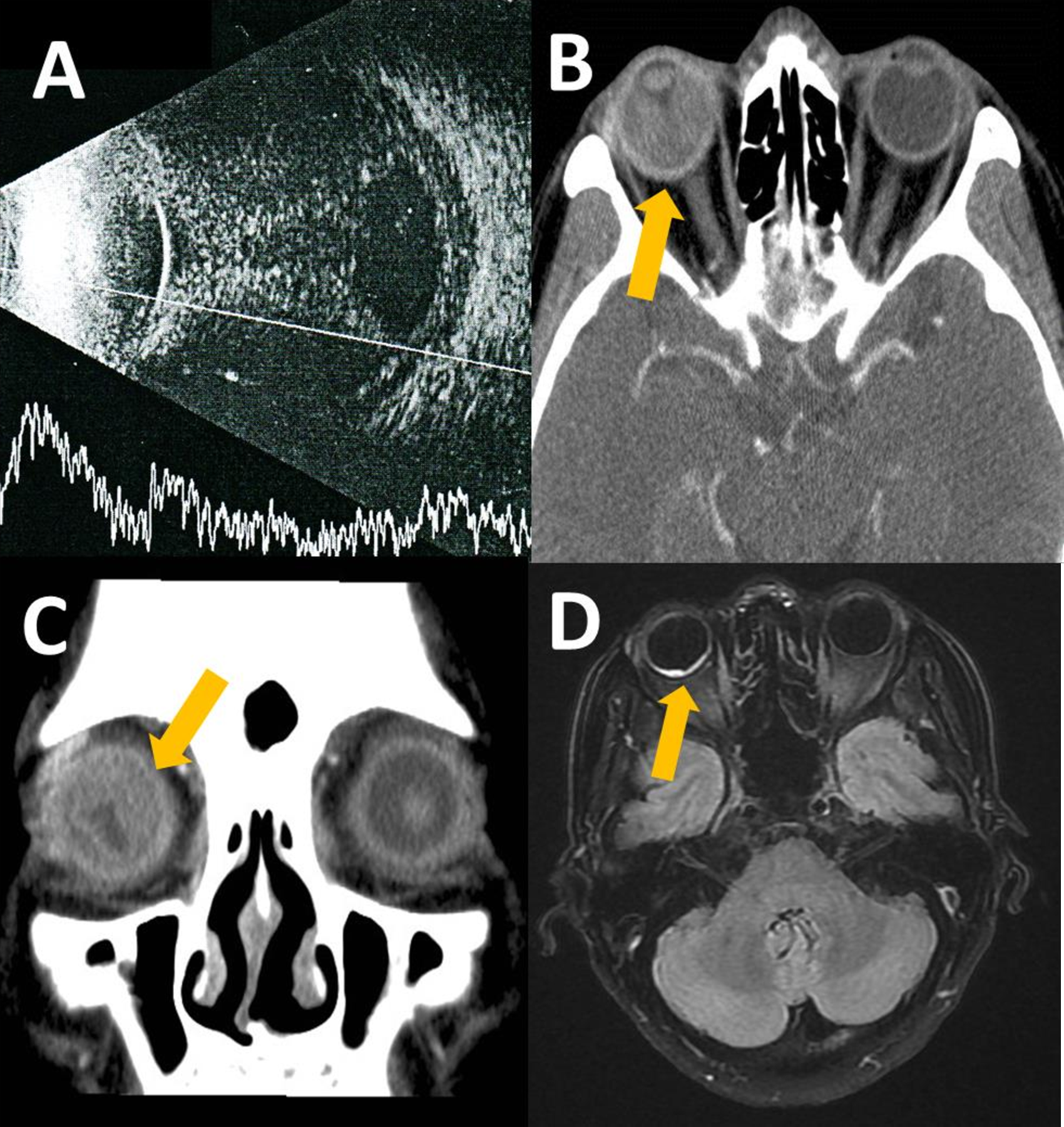
Choroidal detachment of the right eye. A, Transverse B-scan ultrasound demonstrated appositional choroidal detachment of the right eye. An underlying echogenic choroidal thickening with medium to high internal acoustic reflectivity could be seen. B, Axial orbital computed tomography (CT) with contrast showed choroidal detachment of the right eye in bi-convex configuration (arrow) and underlying hyperdense choroidal thickening with contrast enhancement. C, Coronal orbital CT view showed 360°choroidal detachment of the right eye (arrow). D, T2-weighted and fluid-attenuated inversion recovery (T2-FLAIR) axial orbital magnetic resonance imaging demonstrated an elevated hyperintense lesion at the right posterior globe (arrow).
The patient was managed with topical Azopt (1% brinzolamide), Combigan (0.2% Brimonidine tartrate, 0.5% timolol), Isopto Carpine (2% pilocarpine), oral acetazolamide, intravenous mannitol and Betame (0.1% betamethasome). However, IOP level of right eye only decreased to 40 mmHg. Because there might be potential component of pupillary block besides posterior pushing mechanism of secondary angle-closure. We performed laser peripheral iridotomy (LPI) in the right eye in order to lower IOP and relieve ocular pain temporarily. The IOP decreased to 12 mmHg after LPI (Figure 2A and 2B). IOP increased gradually to 40 mmHg in the right eye in a week after LPI. The patient received palliative external beam radiotherapy in the right orbit for two months (4500Cgy/25f). IOP was 9 mmHg in the right eye after two months of radiotherapy. BCVA was hand motion at 10 cm in the right eye. Slit lamp examination revealed clear cornea, deep anterior chamber in the right eye (Figure 2C). Regression of choroidal detachment and CM in the right eye were observed in B-scan ultrasound (Figure 2D). The patient ultimately succumbed to her illness six months after the initial presentation.
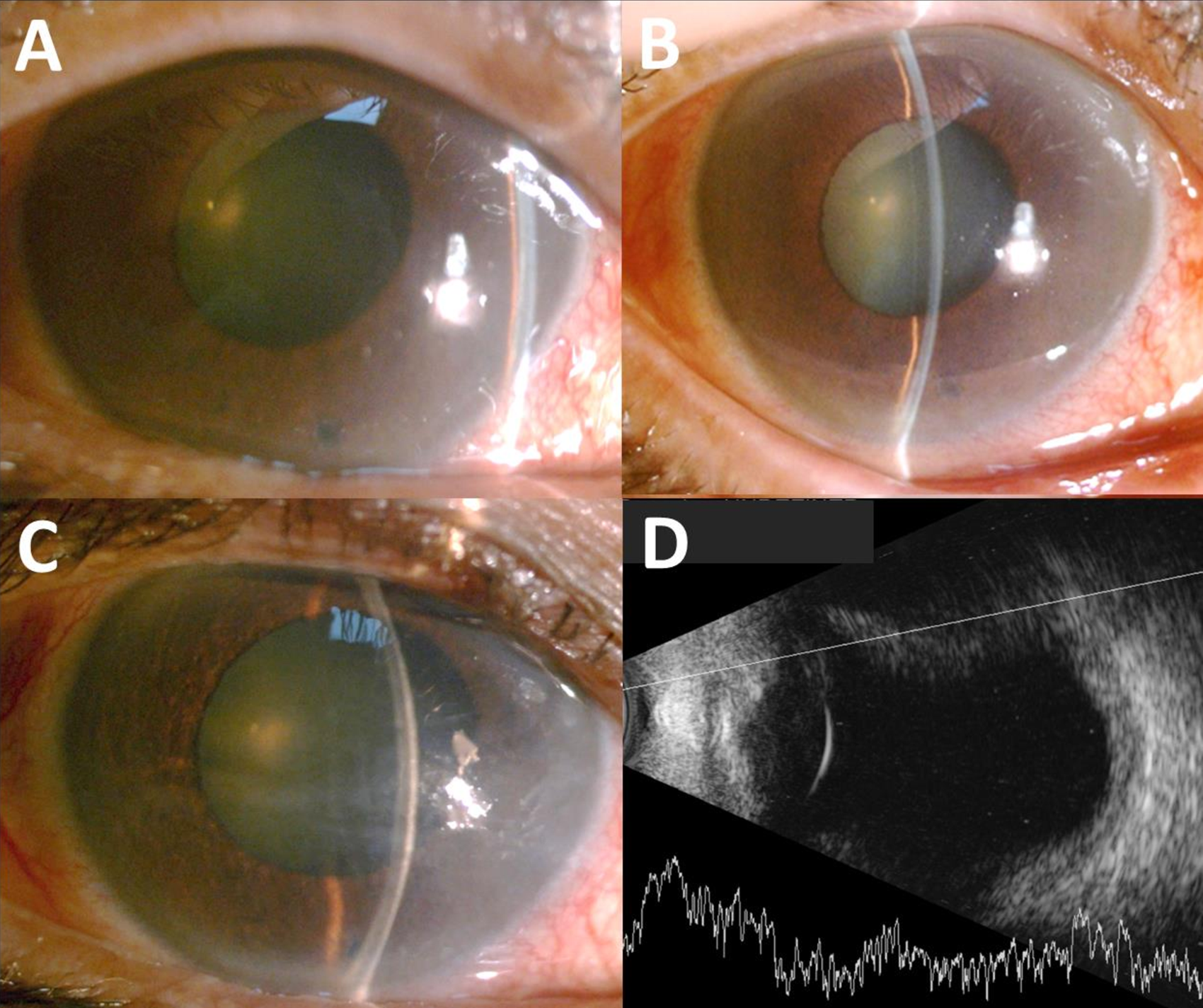
Slit-lamp photographs and B-scan of the right eye. A and B, Slit-lamp exams revealed shallow central and peripheral anterior chamber depth before radiotherapy. C, Deep anterior central chamber was observed two months after radiotherapy. D, B-scan ultrasound image showed improvement of choroidal detachment two months after radiotherapy. The underlying choroidal thickening also regressed.
Discussion
Adenocarcinoma was the most common pathological type of CM deriving from lung cancer, accounting for 47.6% of cases, followed by small cell carcinoma 21.4%. 6 Middle-aged male was more often affected. 7 Symptoms of CM included blurred vision, floaters, phosphenes, visual field defect and eye pain.2,4,8,9 Clinical ocular findings of CM included a homogenous creamy white mass with or without leopard skin pattern, sometimes with subretinal fluid visible surrounding the tumor. 2 Ancillary diagnostic tool such as B-scan ultrasound was characterized by a relatively flat-and-wide mass with medium-to-high heterogenous reflectivity; retinal detachment and choroidal detachment may also be present. 3 Optical coherence tomography featured secondary changes in the retinal pigment epithelium, lumpy bumpy appearances with subretinal fluid due to its nature of hyperpermeability. 3 CT depicted hyperdense choroidal thickening with contrast enhancement. 10 MRI showed a choroidal lesion that appears isointense on T1-weighted images and hypointense on T2-weighted images. 11
In previous literature, choroidal detachment in CM was a rare occurrence, with 12 cases reported in the past.8,12–16 Among those reported, six cases combined with the manifestation of acute angle-closure attack were documented, summarized and depicted as the table below (Table 1).8,12,15,16 Kreiger et al. 12 reported a case of 57-year-old man with CM of unknown origin demonstrated several episodes of acute angle-closure attacks of right eye. Fundus examination confirmed the presence of total retinal detachment and choroidal detachment in the right eye. Stephens and Shields 14 in their review of 70 patients, found one case of metastatic melanoma with secondary glaucoma due to hemorrhagic choroidal detachment. Shields et al. 8 reported a survey of 242 patients with CM, only three patients (1.2%) had elevated IOP with the mechanism of acute angle-closure due to either choroidal detachment or retinal detachment. The primary tumor was a bronchogenic carcinoma in two patients, and a cutaneous melanoma in one. Chen et al. 16 reported a case report of 47-year-old woman with Sjögren syndrome presenting acute angle-closure in the right eye as an initial manifestation of metastatic lung adenocarcinoma; B-scan ultrasound showed retinal and choroidal detachment in the right eye. Of these six cases, the primary tumor site was lung in three cases, and with only one case well-documented.8,16 In our case, the patient with CM from lung adenocarcinoma presented acute angle-closure attacks in the right eye. B-scan ultrasound and CT proved the presence of almost 360° bullous appositional choroidal detachment. The size and extent of such large choroidal detachment could displace the lens-iris diaphragm anteriorly resulting in secondary angle-closure.
Clinical information on choroidal metastatic patients with acute angle-closure in previous studies and on the patient in this study.
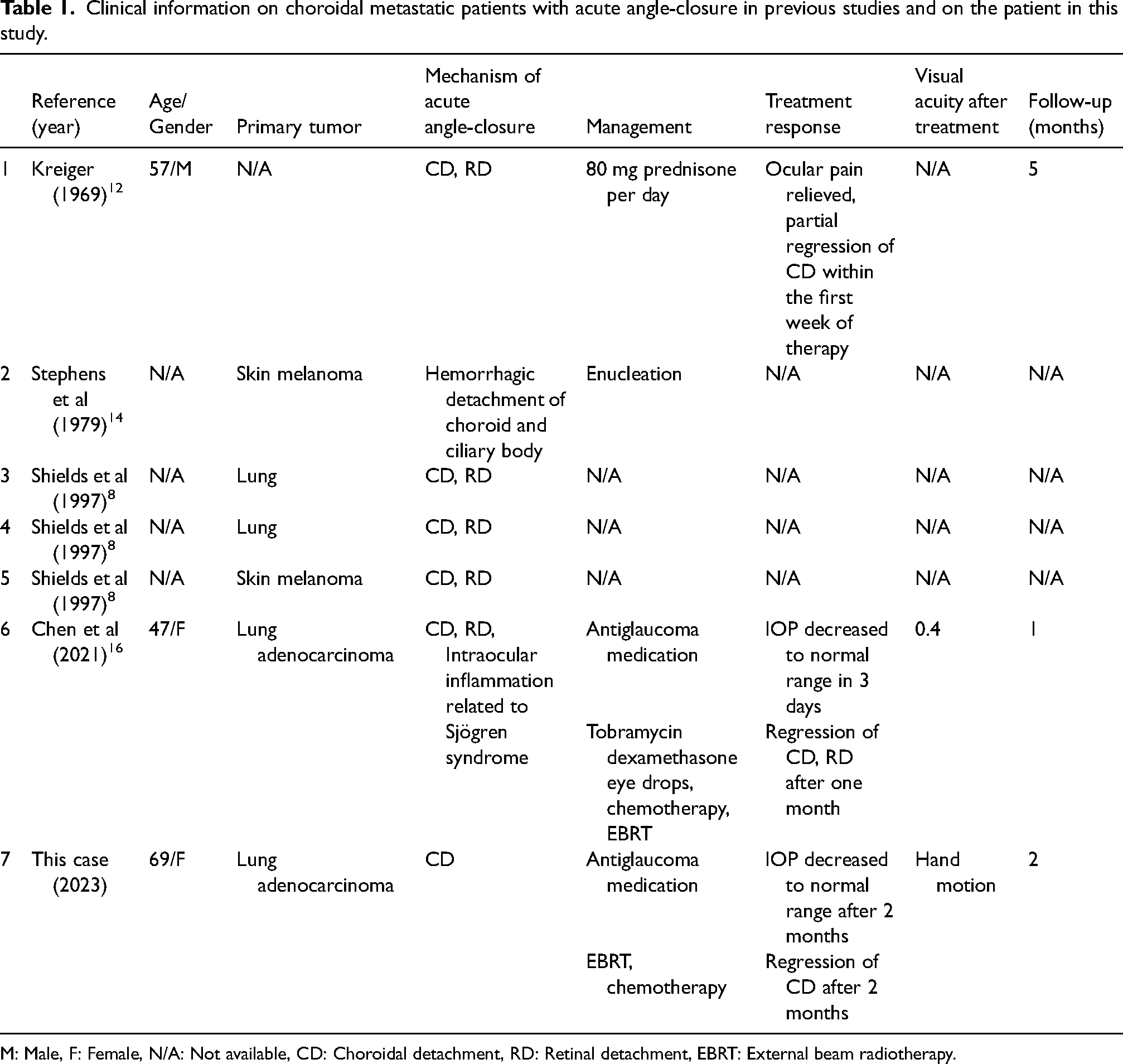
M: Male, F: Female, N/A: Not available, CD: Choroidal detachment, RD: Retinal detachment, EBRT: External beam radiotherapy.
Treatment options of CM should be chosen on the basis of various factors including the physical condition of the patient, the location and extent of intraocular metastasis and the presence or absence of distant metastases. In cases of isolated CM or oligometastatic disease, a local treatment is recommended including radiotherapy, intravitreal bevacizumab, laser therapy, cryotherapy, or resection. 17 In cases of multimetastatic disease threatening survival, local treatment won’t be initiated until overall metastatic disease is properly controlled, with the exception that the ocular symptoms are very severe or a long delay before chemotherapy; palliative radiotherapy in such cases can be performed first. 3
For the management of secondary angle-closure caused by choroidal detachment from CM, Kreiger et al. 12 reported relief of eye pain and partial receding of choroidal detachment using high dosage of steroid (80 mg prednisolone per day), but treatment effect on either IOP or the anterior chamber depth was not recorded. Chen et al. 16 reported that the IOP returned to normal in three days after treatment with topical antiglaucoma agents and corticosteroid eye drops. The author suggested that the excellent response of angle-closure attack to medical treatment might be associated with intraocular inflammation from Sjögren syndrome in addition to choroidal detachment from CM. In our case, antiglaucoma agents, corticosteroid and LPI were ineffective against relieving angle-closure attacks. It was only after receiving radiotherapy for 2 months could IOP return to normal readings along with deepening of anterior chamber and improvement of choroidal detachment. It was inferred that radiotherapy caused the regression of CM and large bullous choroidal detachment, thereby reducing the pushing force from behind the iris-lens diaphragm and eliminating secondary angle-closure. This represented the severity of choroidal detachment in our case was greater compared to the case of Chen et al., 16 where in our case it took two months to relieve IOP elevation whereas in the case of Chen et al. 16 it took three days.
In conclusion, this was a rare case of lung adenocarcinoma with CM presenting with intractable acute angle-closure attacks due to large bullous choroidal detachment. The secondary angle-closure attacks couldn’t be managed with medical and laser treatments. Only local radiotherapy provided dramatic improvement in choroidal detachment and CM, thereby relieving angle-closure attacks. Such large choroidal detachment could take longer treatment duration. Ophthalmologist should be prompted to consult radiologist for management once detected cases like this for better treatment outcome.
Footnotes
Declaration of Helsinki
We confirm that the study and data collection conform to all local laws and are compliant with the principles of the Declaration of Helsinki.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
We have obtained the ethics committee approval and informed consent from the patient.
Informed consent
The consent to publish this case was gathered from the patient.