
Abstract
Aims
To emphasize that ocular ischemic syndrome (OIS) is a rare but threatening condition. It is a consequence of occlusion or dissection of internal carotid artery (ICA).
Methods
A 66-year-old caucasian male presented in the emergency room with painful vision loss in his right eye and mild neurological symptoms. He was diagnosed ocular ischemic syndrome (OIS) in ICA and ophthalmic artery occlusion due to right ICA dissection.
Conclusions
It is very important to know and be able to recognise OIS as it may often be misdiagnosed or treated as a different entity. Patients with ICA occlusion and OIS must be treated as soon as possible by a stroke unit team to resolve ICA occlusion/dissection and by the ophthalmologist to prevent further ocular related complications.
Keywords
Introduction
Ocular ischemic syndrome (OIS) was first described by Hedges in 1963 in a 48-year-old patient 1 and the same year confirmed by Kearnst and Hollenhorst. 2
It is caused by ocular hypoperfusion due to severe carotid occlusive diseases such as, stenosis, occlusion or dissection. In OIS, the internal carotid artery (ICA) and its first branch, the ophthalmic artery, are involved. As it is a very rare condition, the exact incidence is not known; however it is estimated at 7.5 cases per million on a yearly basis. 3 Few cases have been reported in literature so far.
OIS develops especially in patients with poor collateral circulation between the ICA and external carotid artery (ECA) systems or between the right and left ICA. Patients who develop OIS show decresed or absent blood flow in ophthalmic artery and its branches: central retinal artery and posterior ciliary arteries. OIS is an ocular manifestation of systemic disease of which main symptoms are: acute or subacute visual loss, history of amaurosis fugax, and pain caused by Intraocular pressure (IOP) increase or ocular ischemic pain, described as ‘ocular angina’.3–6
Due to its systemic severity it is very important to be able to recognise OIS as it may often be misdiagnosed or treated as a different entity.
Case description
A 66-year-old caucasian male presented in the emergency room (ER) complaining about a sudden onset of pain, redness, vision loss in the right eye (RE) and mild left hemisome hypostenia. About three days earlier he had manifested ocular prodromic signs and symptoms such as amaurosis fugax and decreased vision in his right eye. He had had no history of prior redness of his eyes, fever or ocular trauma and no ocular diseases. In his medical history there were reported fasting hyperglycemia, prostatic hypertrophy, chronic respiratory failure, obesity, and in 2020 he reported an acute respiratory failure in SARS COV-19 pneumonia. Due to the association of ocular and neurological symptoms, brain computed tomography (CT) and brain and neck CT Angiography were first run in the ER. The two exams showed no visualization of the right internal carotid from its origin to the origin of the right middle cerebral artery with reduced visualization of the ipsilateral ophthalmic artery. So interventional radiologist performed an arteriography which confirmed dissecative based ICA occlusion and poor compensation from the controlateral carotid (Figure 1A). Then endovascular treatment (angioplasty and thrombectomy) (Figure 1B) was performed and later endovascolar stenting was also carried out (carotid wallstent) (Figure 1C-D). Medical therapy with double antiaggregation agents was prescribed.
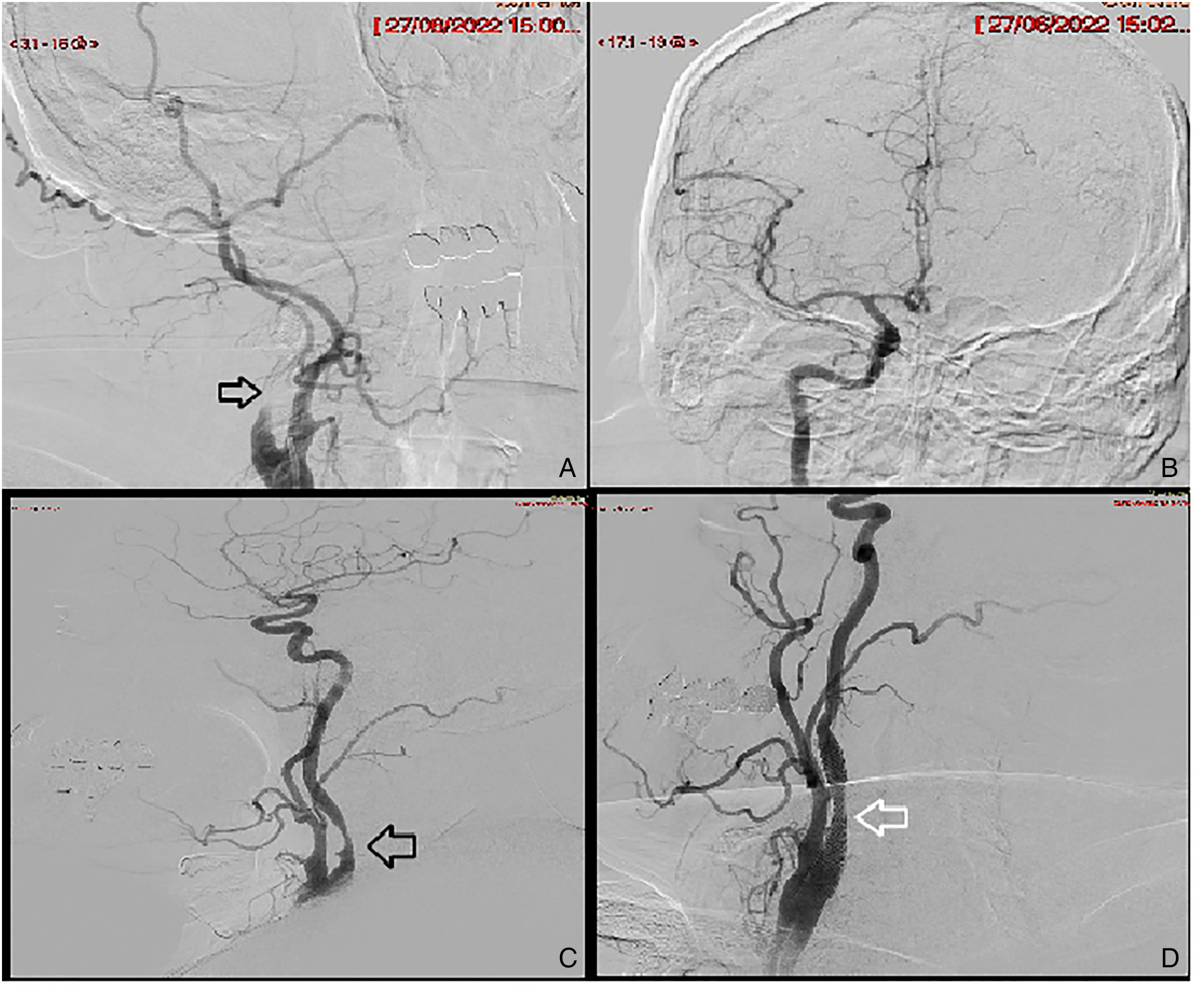
(A) dissection of the internal carotid artery without intracranial opacification: (B) recanalisation of the internal carotid artery and intracranial circulation after angioplasty at the level of the dissection; (C) evidence of ICA stenosis on angiography; (D) control angiography after placement of two carotid stents with restoration of vessel calibre.
After the endovascular treatment, the patient complained about persistent ocular pain, redness and vision loss and he was referred to the ophthalmology service accordingly.
Visual acuity in his right eye (RE) revealed no light perception. Biomicroscopy showed painful red eye with conjunctival hyperemia, corneal edema, Descemet's folds, no light pupillary reflex, no tyndall in anterior chamber and cataract. Intraocular pressure, measured with Goldmann tonometer, was 8 mmHg. Dilated fundus examination showed narrowed retinal arteries with colesterol emboli (Hollenhorst emboli) inside the arterial lumen in both superior and inferior temporal arteries and in superior nasal artery, dilated retinal veins, diffuse retinal whitening with cherry-red spot and diffused dot mid-peripheral retinal hemorrhages.(Figure 2C) OCT exam showed internal and middle retinal layers ischemic edema (Figure 2A) and the OCTA revealed the absence of macular flow both in superficial and deep capillary vascular plexus. Fluorescein angiography showed prolonged arm-to-choroid and arm-to-retina circulation time and irregular and prolonged retinal filling time (Figure 3A-B). In the late phases leakage of the major retinal vessels, in particular arteries, was observed (Figure 3C). We also found optic disk hyperfluorescence and areas of peripheral ischemia. We found superficial dot hemorrhages presented like round hypofluorescent areas. Indocyanine green angiography showed prolonged arm-to-choroid circulation time and prolonged intrachoroidal circulation time. We found choroidal hypoperfusion manifested as areas of vascular filling defects in the posterior pole. (Figure 3D-E-F)

(A) OCT at baseline exam showes internal and middle retinal layers ischemic edema; (B) at follow up in the OCT image it would seem it is not possibile to recognize the intermediate and the external retinal layers; (C) fundus multicolor image showes narrowed retinal arteries with colesterol emboli (Hollenhorst emboli) inside the arterial lumen in both superior and inferior temporal arteries and nasal superior arthery, dilated retinal veins, diffuse retinal whitening with cherry-red spot and diffused dot mid-peropheral retinal hemorrhages. (D) OCT-A showed the complete absence of retinal blood flow and both superficial and deep capillary plexus were not detectable.
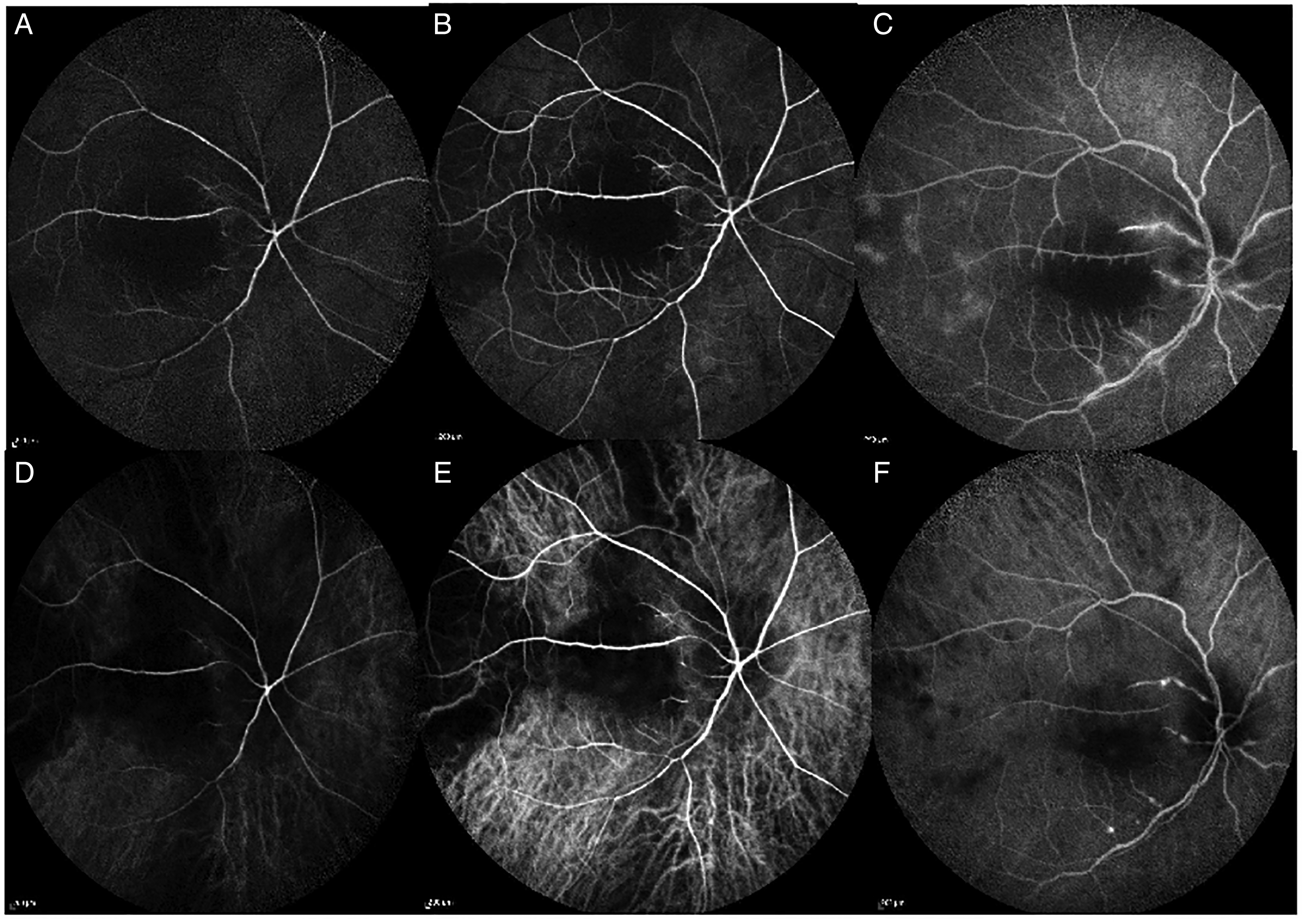
(A-B) fluorescein angiography early phases shows prolonged arm-to-choroid and arm-to-retina circulation time and irregular and prolonged retinal filling time (C) fluorescein angiography mid-late phases leakage of the major retinal vessels, (D-F) Indocyanine green angiography showe prolonged arm-to-choroid circulation time and prolonged intrachoroidal circulation time, choroidal hypoperfusion manifested as areas of vascular filling defects in the posterior pole.
So the final diagnosis was ocular ischemic syndrome in the right eye whereas left eye was healthy.
Manifesting pain the patient was treated with cicloplegic topic drops (ciclopentolate), steroid drops (dexamethasone 2 mg/ml ocular drops) and underwent argon laser therapy over retinal ischemic areas.
After a few days of topical therapy, ocular symptoms improved and inflammation of the anterior segment decreased but there was no improvement of visual acuity.
After two months both fluorescein and indocyanin green angiography were repeated and showed prolonged arm-to-choroid and arm-to-retina circulation and retinal filling time. There were no more ischemic peripheral retina areas, while there were the scars caused by the argon laser spots. In OCT there was no more hyperreflectivity of the inner and middle retinal layers, but severe thinning of the retinal neuropithelium (Figure 2B).
The OCT-A exam showed complete absence of retinal blood flow and both superficial and deep capillary plexus were not detectable.(Figure 2D) Slit lamp examination showed no inflammation and descemet's folds were disappered. There was no rubeosis iridis, nor angular new vessels at the gonioscopy exam.
There was no light pupillary reflex. Intraocular pressure measured with Goldmann tonometer was 16 mmHg. Dilated fundus exam showed whitening of the whole retina with filiform retinal vessels and a hollenhorst emboli inside the lumen of both superior and inferior temporal artery, and superior nasal artery.
Visual acuity still revealed no light perception.
This case report was performed according to the Declaration Of Helsinki. Patient informed consent had been acquired in October 2022
Conclusions
Ocular ischemic syndrome is an uncommon but potentially blinding condition as a result of severe ocular hypopefusion. 4 It is a rare condition which may represent the first sign of internal carotid artery dissection (ICAD).6,7 The classic signs and symptoms of ICAD consist of pain in the ipsilateral neck, head and orbital regions, cerebral or retinal ischemia.5–7 Although It is a rare condition, it is important to know how to diagnose and how to manage it, in order to avoid futher complications, such as ocular pain and neovascular glaucoma. As reported in our case, it is necessary to perform a complete ophthalmological exam, searching for signs such as ocular pain and anterior segment inflammation to perform a differential diagnosis with unique central retinal artery occlusion (CRAO). In fact, in CRAO, we only find retinal ischemia whith cherry spot sign, but not hypotone, descemet's folds and pain. Iris neovascularization is more common in OIS than CRAO, so we decided to have retinal panphotocoagulation over ischemic area to avoid neovascular glaucoma in a blind eye. In this case report we want to emphasize that ophthalmogists should be trained to distinguish OIS to CRAO. As a matter of fact, the ophthalmologist may be the first to manage patients with ICAD that primarily presenting with ocular symptoms.
It is essential to establish a correct differential diagnosis between the two pathologies, because both of them must be referred to a stroke unit team (radiologist and neurologist) but with two different timings. Indeed a patient with OIS has to receive immediate treatment in the ER by means of prompt neuroradiological exams and interventional procedures 5 as in the case we described when the patient underwent ICA angioplasty and thrombectomy.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.