
Abstract
Purpose
To describe the course of care and outcomes for 3 uveitis patients formerly on Remicade that were non-medically switched to Inflectra.
Design
Retrospective observational case series.
Methods
•Setting: Tertiary care clinical practice. •Patient population: 3 Uveitis patients, observing both eyes for inflammation as applicable. Patients included if they had been on Inflectra for ≥2 infusions and history of Remicade use. Patients described herein had at least 1 adverse reaction to Inflectra and were switched to Remicade for medical necessity. Patients excluded if they were lost to follow-up or not examined for over 6 months during therapy. •Observation procedures/Interventions: Patients observed for adverse changes in clinical course while on Inflectra. Patients developing these changes on Inflectra were started or restarted on Remicade.
Results
The 3 patients described herein developed adverse complications while on Inflectra that required switching to Remicade. They were originally on Remicade, and their clinical course worsened beyond what had been controlled with Remicade alone. Our findings are limited by our small sample size, and further investigation is necessary to explore the scope of effects of non-medical biosimilar switching.
Conclusion
Non-medical biosimilar switching from Remicade to Inflectra may induce detrimental side-effects and significant worsening of inflammation in patients with uveitis. Non-medical biosimilar switching from Remicade to Inflectra should be discouraged, and physician input should be sought in establishing an effective and medically-necessary treatment plan for patients with uveitis.
Keywords
Introduction
Uveitis – inflammation affecting the iris, ciliary body, and/or choroid – remains one of the leading causes of blindness worldwide, accounting for nearly 15% of all cases.1,2 Early intervention for acute uveitis flares involves the use of local or systemic corticosteroids. While these medications may be effective in the short-term, they have a well-known array of side-effects and shortcomings that preclude long-term use. In particular, they accelerate the formation of cataracts in phakic individuals, induce increases in intraocular pressure in susceptible individuals leading to glaucomatous conditions, and increase the risk of recurrence of ocular surface herpetic diseases, including Varicella zoster. 3 Steroid implants have shown great efficacy in controlling complicated chronic uveitis; however, these medications carry a similar risk of glaucoma and cataract formation.4,5 Systemic steroids may also be employed in early treatment of uveitis; yet, chronic use induces the above risks of glaucoma and cataract acceleration as well as hyperglycemia, impaired wound healing, and impairment of the hypothalamic-pituitary-adrenal gland axis. In addition, these agents may not effectively treat the systemic inflammation that may be fueling ocular inflammation. 3
To best treat chronic uveitis and related systemic conditions, immunomodulatory therapy (IMT) should be used. Anti-metabolite agents – such as methotrexate (MTX), cyclosporine, and mycophenolate – are some of the first medications used to treat uveitis on a long-term basis. However, more recalcitrant or severe forms of uveitis may require injection or infusion therapy. 2 The majority of these infusion therapies are biologic response modifiers, also known as biologics – medications containing antibodies that target cytokines and/or inflammatory pathway factors. A number of such medications target tumor necrosis factor alpha (TNF-a), such as adalimumab, marketed in the United States as Humira (AbbVie; North Chicago, IL) and the only formulation of this medication indicated by the United States Food and Drug Administration (FDA) to treat uveitis. A number of adalimumab biosimilars - biologics that are nearly-identical (though not necessarily substitutable equivalent) to an existing biologic medication – have been approved by the FDA but are not yet indicated to treat uveitis. 6 The first anti-TNF-a was Remicade® (Janssen, Titusville, NJ), which contains the chimeric monoclonal antibody infliximab, that was first approved as a treatment for Crohn's disease and then rheumatoid arthritis before being applied to other autoinflammatory conditions.7,8 Since 2001, Remicade has been used to control and treat uveitis. 9 We have successfully employed it at 5 mg/kg every 4 weeks to control ocular inflammation in our patient population. 10
For 15 years, Remicade was the only form of infliximab available, and, despite being off-label in the United States, was successfully used to treat many forms of ocular inflammation. Yet, coverage providers desired alternatives and continuously established many barriers to approval, likely due to concerns of cost, often labeling the medication as “investigational.” In 2016, the FDA approved infliximab-dyyb, marketed as Inflectra (Pfizer, New York, NY), the first monoclonal antibody biosimilar. Inflectra was initially indicated to be used in a similar dosing strategy to Remicade based on previous data showing high similarity in molecular structure, pharmacokinetics, and pharmacodynamics as well as non-inferiority in clinical efficacy for ulcerative colitis, Crohn's Disease, and several arthritides. 11 Given these data and the fact that Inflectra was sold 30–40% less than Remicade, certain groups of physicians recommended that Inflectra be trialed first in patients naive to infliximab. 12 Echoing this and going further, insurance companies have at times required patients already on Remicade be switched to Inflectra, a form of Non-Medical Biosimilar Switching – a change in medication from a pre-existing medication to a biosimilar for reasons beyond a physician's judgment, such as decreased cost.
However, studies suggest this kind of non-medical biosimilar switching may be fraught with adverse outcomes for patients. One meta-analysis suggested that for every 11 patients undergoing non-medical switching, 1 patient will lose response to infliximab. 12 In addition, given the logistical difficulty with the pre-authorization process for required biosimilars, patients treated with Remicade may have a low circulating dose of infliximab for an extended period, making them prone to form anti-infliximab antibodies in the environment of low drug level. 13 If a lack of response to infliximab were to develop, it may lead to increases in medication dosage, potential treatment failure to any infliximab-based therapy, and increased risk of potential side effects from higher circulating drug levels. Such a scenario would complicate anti-inflammatory therapy for susceptible patients, impair their quality of life, and be more costly for the patient, their clinician, their health insurance company, and the healthcare system overall. In the case series herein, we discuss three patients formerly on Remicade who underwent non-medical biosimilar switching to Inflectra and their outcomes.
Methods
This work is a retrospective observational case series at our tertiary ophthalmology clinic, the Massachusetts Eye Research and Surgery Institution (MERSI). Our chart review study was approved by the New England Institutional Review Board (#IRB00000533), performed in compliance with the Health Insurance Portability and Accountability Act, and in accordance with the Declaration of Helsinki. Written consent was obtained for study participation and identifiable imaging.
Our electronic medical record database was queried for patients treated with Inflectra for 2 or more infusions and any prior Remicade therapy. Patients were excluded for loss to follow up or lack of physical examination at MERSI for over 6 months. This search found 7 patients not yet in remission: 4 were switched from Remicade to an infliximab biosimilar and have not shown symptoms of active/breakthrough disease or side-effects. The other 3 had been on Inflectra but were switched back to Remicade out of medically-relevant necessity. These latter cases are described below.
Case series
Case 1
A 35-year-old woman with history of juvenile idiopathic arthritis (JIA) presented to us in 2009 with right eye (OD) discomfort and blurriness. She was started on our Remicade protocol (300 mg) in 11/2009 and eventually kept on a dose of 800 mg every 4 weeks, mycophenolate mofetil, and indomethacin. In 2/2020, she reported worsening joint inflammation and had evidence of mild breakthrough inflammation (e.g. 0.5+ cell) with no discernable posterior inflammation (Supplemental Figure 1). Her rheumatologist then substituted her Remicade with Actemra (Genentech, South San Francisco, CA) every 4 weeks in 5/2020. She was given 3 doses of this medication, but it treated neither her joint nor her eye conditions effectively. As her ocular inflammation was better controlled with Remicade, we attempted to restart this medication. However, her insurance denied this, and she was started on Inflectra 400 mg in 4/2021 with 3 biweekly loading doses and subsequent every-4-week maintenance dose per manufacturer's protocol.
When she received her initial loading doses, the patient's inflammation was quiet. However, 2 months after starting the medication in 6/2021, she developed intermittent paresthesia of her right hand and foot. These persisted through 8/2021. Due to problems with her insurance, she did not receive her infusion in 9/2021. However, despite feeling well with resolution of her paresthesia before her infusion in 10/2021, she still had 2+ cell OD after her infusion, suggesting that her inflammation worsened on Inflectra. We stopped this medication and planned to restart our Remicade protocol as soon as possible. When she was seen again in 1/2022 on the rest of her regimen, she had 4+ cell OU, markedly worse than it had been before starting Inflectra. Fluorescein angiogram (FA) revealed worse papillitis than had been seen before Inflectra (Figure 1), and optical coherence tomography of the macula (OCTmac) revealed developing macular edema (Figure 2). Our Remicade protocol eventually restarted in 5/2022, and she has had slow recovery from peak inflammation after Inflectra. Overall, the substitution of Inflectra not only failed to control her inflammation but also indirectly allowed unprecedented inflammation because of the need to stop the medication.
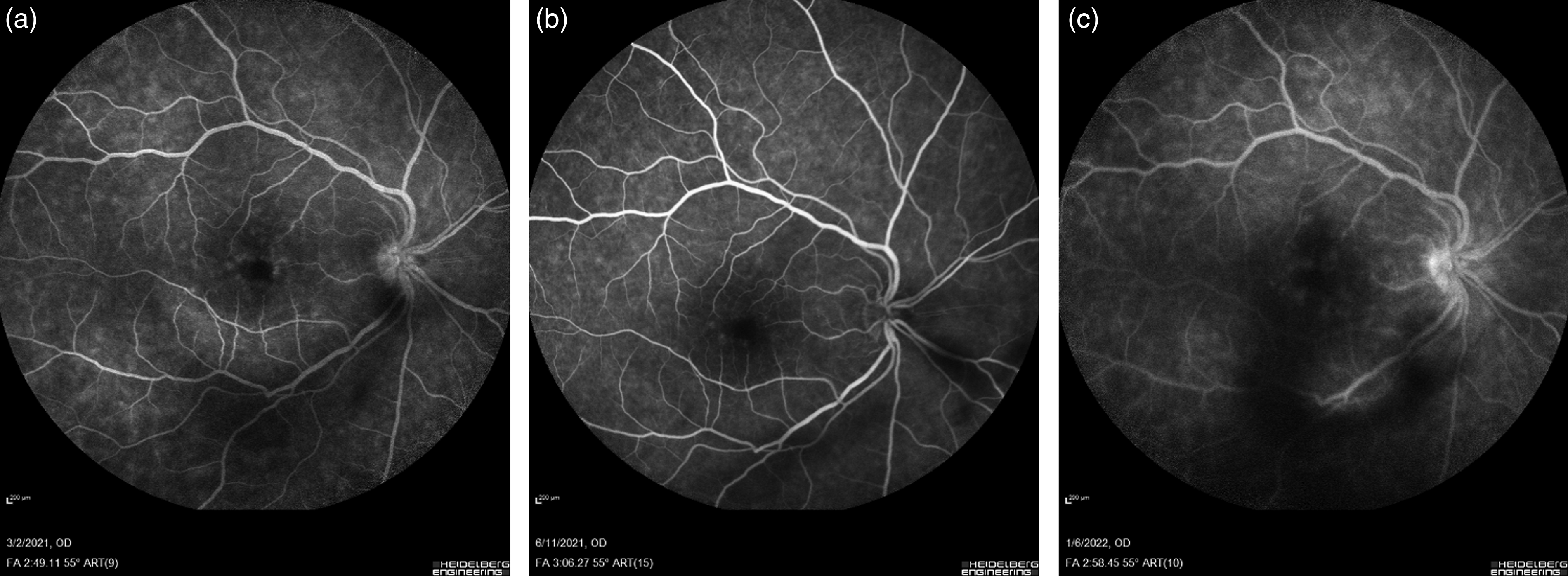
Inflammation OD in Case 1’s patient had unprecedented worsening after Inflectra use as evidenced by FA. (a) Central FA 3 months before Inflectra. (b) Central FA 2 months after starting Inflectra. (c) Central FA 4 months after stopping Inflectra.
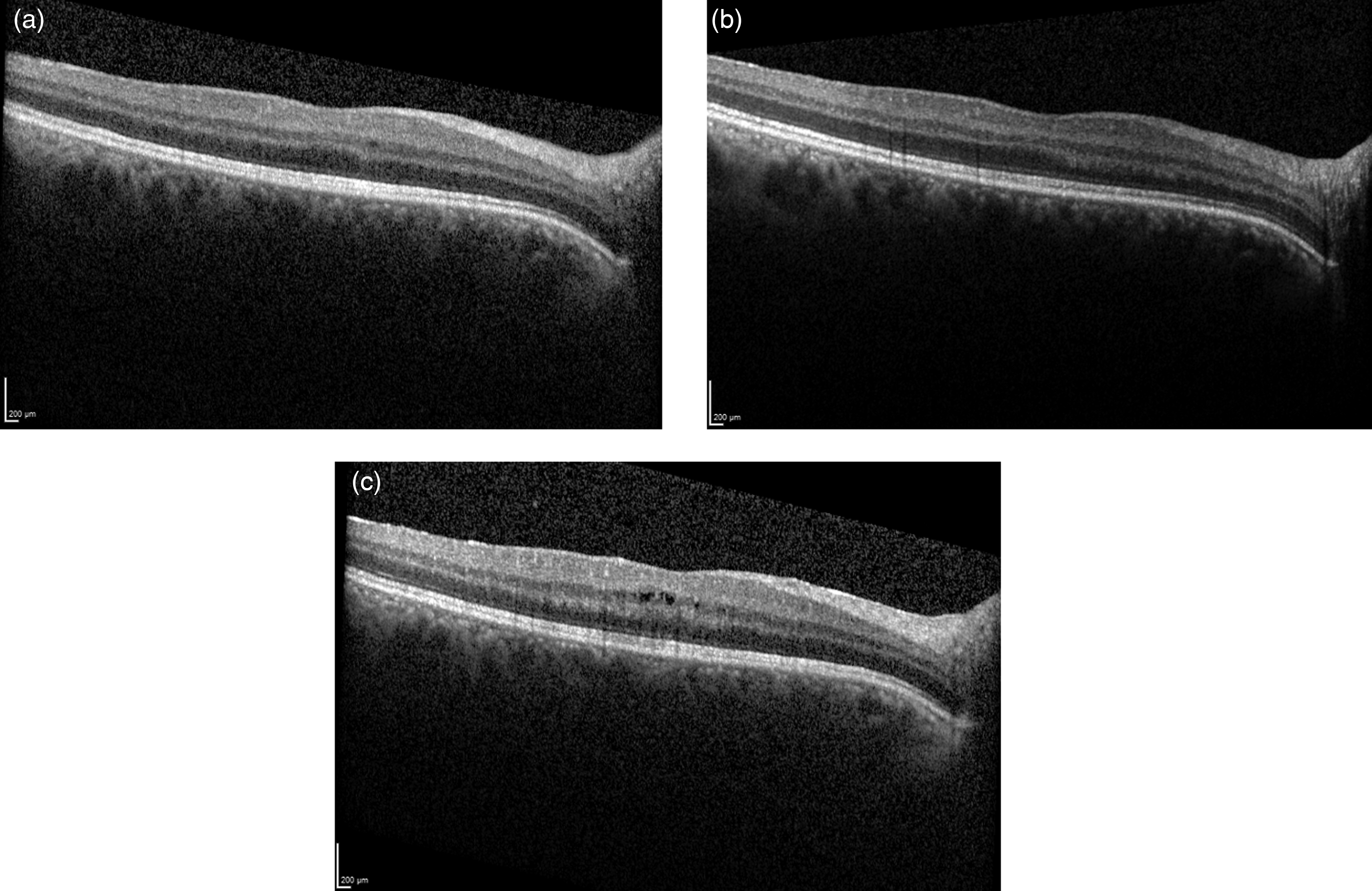
Inflammation OD in Case 1's patient had unprecedented worsening after Inflectra use as evidenced by OCTmac. (a) OCTmac 3 months before Inflectra. (b) OCTmac 2 months after starting Inflectra. (c) OCTmac 4 months after stopping Inflectra.
Case 2
A 51-year-old woman with history of chronic orbital inflammation OD starting 1 month after right orbital trauma presented to us in 2015 for evaluation and treatment planning. At the time, her condition only responded to IV methylprednisolone; neither non-steroidal anti-inflammatory drugs, MTX, nor mycophenolate could control this condition. She was started on our Remicade protocol (400 mg) in 1/2016. As she had persistent right orbital pain on the day of her third loading Remicade infusion in 2/2016, we administered trans-septal triamcinolone OD and planned to increase Remicade to 600 mg every 4 weeks. In 3/2016, we added MTX 15 mg subcutaneous injection weekly, and her next visits showed improvement of her orbital inflammation. There was still some periorbital edema and persistent pain in 7/2016, and we were concerned about development of anti-infliximab antibodies; blood work drawn that appointment was negative for this. We then increased Remicade to 800 mg. She had a flare of periorbital inflammation with scleritis OD in 9/2016, and she was given a 200 mg MTX infusion. She noted, however, that her symptoms greatly improved shortly after Remicade infusion but waned over the next couple of weeks. Weekly MTX was increased to 20 mg, and her flare subsided. She was hospitalized in 3/2017 for recurrent urinary tract infection and was taken off Remicade at the hospital. She returned to our clinic in 6/2017 off Remicade for 4 months with her orbital inflammation appearing well-controlled, so we did not plan to restart Remicade at the time. However, periorbital pain recurred in 7/2017, and we restarted Remicade 800 mg every 4 weeks. Her pain symptoms greatly improved 3 months later on this regimen. She had blunt impact trauma OD in 3/2018 causing pain, but her periorbital inflammation did not worsen.
While we were pleased with her improvement on Remicade and intended to have her continue this medication, between 3/2018 and 10/2018, Remicade had been replaced with Inflectra 800 mg every 4 weeks, though she temporarily stopped Inflectra in 9/2018 to treat an episode of shingles in her right V2 dermatome with right-sided Bell's Palsy. We found her right orbital inflammation had re-flared on that 10/2018 visit, and we slowly restarted Inflectra at 200 mg every 4 weeks with antiviral therapy. However, on her second reinfusion of Inflectra, she developed severe respiratory stress and diffuse hives, prompting termination of this medication. Further immunomodulatory therapies, including cyclophosphamide and Actemra were either ineffective or caused intolerable nausea among other side effects. We eventually tried to reinitiate Remicade, but her initial dose induced shingles recurrence with triggering of her asthma, so she was taken off this medication. Given that she had improvement of her orbital inflammation without side effects from Remicade before she was started on Inflectra, we suspect the intractable course of her inflammation with intolerable sensitivity to Remicade was caused by Inflectra.
Case 3
A 27-year-old woman with history of retinal vasculitis, oral and genital ulcers, and erythema nodosum presented to us in 2011 with anterior and posterior ocular inflammation seen on FA. Her constellation of symptoms satisfied the International Criteria for Behçet's Disease, 14 and we diagnosed her with this condition. We started her on our Remicade protocol (300 mg) in 9/2011, and FA showed marked improvement in inflammation two weeks after her first loading dose. While her ocular and skin symptoms improved after several infusions on this regimen, we noted mild, persistent, peripheral vasculitis in the left eye (OS) and boosted her Remicade to 400 mg per infusion. To further control inflammation, we added 10 mg oral MTX once a week to her regimen, and we eventually converted this to a subcutaneous injection as FA showed little improvement after 2 months on oral medication. FA then showed further improvement in vasculitis; so, we slowly tapered Remicade by stretching out the interval with multiple cycles at 4-, 6-, 8-, 9-, 10-, and 12 weeks to allow her immune system to adjust to new doses of medication given retinal vasculitis on FA in her otherwise asymptomatic eye OS. After a couple of doses at a 12-week interval with no evidence of significant posterior ocular or systemic inflammation, we discontinued Remicade in 3/2017.
However, in 7/2017, she had a recurrence of oral and genital ulcers without any notable ocular findings. FA and OCT finding were also found to be normal. As we were concerned that her recurrent skin inflammation could herald intraocular inflammation, we decided to restart her on Remicade as soon as possible. In 8/2017, she reported additional shortness of breath, though CT scan was negative. She restarted Remicade 400 mg every 8 weeks in 9/2017, and all of these systemic inflammatory symptoms remitted. As she remained on this regimen without issue for nearly 2 years, we decided to slowly decrease her dose to 300 mg in 2019 but continue scheduled infusions. On 3/25/2020, she reported new oral and genital ulcers that had developed a week prior to her infusion. FA and OCT were stable with no active inflammation on examination. Given her systemic symptoms, we shortened her infusion interval to once every 4 weeks, and her symptoms resolved over the next few infusions.
While her inflammation was well-controlled on her regimen at the time, she changed her insurance in 2021, and her new insurance required her to trial Inflectra before they could approve Remicade. On 11/18/2021, we acquiesced and had her begin Inflectra at the same dose and interval as her Remicade (300 mg every 4 weeks). Eight weeks into this regimen, she reported worsening recurrence of oral and genital ulcers, similar to the flare she experienced when she stopped Remicade in 2017. This was surprising to us, as she had no gap in her infusion intervals and no reduction in the amount of medication she received. As we were concerned that her inflammatory symptoms could eventually involve her eyes, we urged her insurance to have her restart Remicade once more. She eventually resumed Remicade infusions of 300 mg every 4 weeks in 2/2022. By 4/2022, her oral and genital ulcers resolved. She had one further oral ulcer that resolved on same therapy between 5/2022 and 7/2022, and she has been free of ocular flares since restart of Remicade.
Discussion
In our retrospective case series, we discussed the outcomes of 3 patients who were initially on Remicade and underwent non-medical biosimilar switch to Inflectra. In our clinical experience, we have had limited success with Inflectra in controlling inflammation while avoiding intolerable side effects such as paresthesia, respiratory distress, and thrombocytopenia.
Our patient in case 1 had JIA-associated uveitis, the most common form of ocular inflammation in children and a difficult-to manage condition with multiple complications including uveitis, glaucoma, cataracts, macular edema, and band keratopathy. Early intervention with non-steroidal IMTs is essential for preventing blindness and the above complications in affected individuals. 15 This patient had a significant breakthrough flare on Inflectra, severe subsequent panuveitis after stopping this medication that had not been seen with cessation of other biologics, and difficulty with controlling ocular inflammation with Remicade. As she had not experienced similar symptoms on the rest of her regimen, we suspect her infliximab biosimilar was the cause of these complications. One possible reason for her complicated course upon restarting Remicade is that she may have developed anti-infliximab antibodies while on Inflectra. One study analyzing multiple reports of ulcerative colitis and Crohn's disease patients on biologics showed wide variability in the development of anti-biologic antibodies with an average incidence rate of about 35–40% across all studies with patients on infliximab biologics. Such anti-drug antibodies may dampen the therapeutic effect of biologics. 13 While it is possible our patient in case 1 may have developed such antibodies, we have low suspicion of this as she did not develop a reaction to her original Remicade and had been on the recommended dose of Inflectra at 5 mg/kg. In addition, this patient developed paresthesias while on Inflectra that resolved with resumption of Remicade. A report by Xue et al. 16 discussed two patients who developed similar polyneuropathy after switching from Remicade to an infliximab biosimilar with resolution after restarting Remicade. Together, these findings suggest that the non-biomedical switch to biosimilar induced these side effects in these patients.
In case 2, our patient exhibited substantial dyspnea and hives while on Inflectra and had intolerable asthma and recurrence of shingles when she resumed Remicade. We recognize that she had been on a lower dose of Inflectra to prevent recurrence of a recent shingles infection, and this may have provoked anti-infliximab antibody development. A similar reaction of angioedema to Inflectra was described by Xue et al., 16 though it resolved after resumption of Remicade, unlike our patient who developed this kind of reaction after Inflectra was stopped. Alternatively, our patient may have developed autoantibodies from Inflectra due to the interval in infusions due to patient non-adherence to therapeutic recommendations. Notably, our patient had not developed anti-infliximab antibodies to Remicade with similar non-adherence. This suggests that Inflectra may have a greater potential for formation of anti-infliximab antibodies than Remicade. However, we recognize that our insights are restricted by a small sample size and that further work will be necessary to determine the extent of anti-infliximab antibody formation in biosimilar switching.
In case 3, our Behçet's disease patient experienced worsening of joint pain and an increased number of oral and genital ulcers after she was switched to Inflectra, despite being stable on Remicade. These symptoms subsided once she was switched back to Remicade. Another case series described similar symptoms in 3 patients with Behçet's disease that were switched from Remicade to a biosimilar. Each of these patients demonstrated systemic symptoms that developed after starting an infliximab biosimilar and remitted after switching to subcutaneous adalimumab. 17 Notably, our patient's Behçet's flare occurred while on a similar dose and interval of Inflectra as her original Remicade, so it is unlikely that she developed anti-drug antibodies on her Inflectra regimen. Instead, we propose that her disease recurrence was due to an intrinsic property of her infliximab biosimilar.
Our results are particularly important as several adalimumab biosimilars become available in the United States. While Humira has been the only form of adalimumab available through the end of 2022, its patent protections ended in 2023 with the arrival of adalimumab-atto, marketed as Amjevita (Amgen; Thousand Oaks, CA), with several other adalimumab biosimilars launching later in 2023. 18 Recent reports suggest these biosimilars may be good additions to the uveitis treatment armamentarium. A group out of Bristol found that Amjevita could treat uncontrolled or recurrent cases of non-infectious uveitis previously-treated with Humira with no significant differences in the number of patients who flared before and after the switch. 19 Another group out of Italy showed that another adalimumab biosimilar, Imraldi (Biogen; Barr, Switzerland) could treat refractory cases of non-infectious uveitis. 20 While these results support medically-relevant biosimilar switching to treat uncontrolled uveitis, recent data does not necessarily support non-medical biosimilar switching for patients with uveitis controlled on a biologic originator. For instance, one study showed that for patients with controlled uveitis on originator anti-TNF-a drug, nearly 1/5 of them had a relapse after switching to a biosimilar. 21 Given these results and our patient cases described herein, we advocate against non-medical biosimilar switching.
Conclusion
In our case series herein, each of our 3 patients who underwent non-medical infliximab biosimilar switching showed less optimal control of ocular and systemic inflammation than they had before their switch. Based on our experience and the results of our case report, we recommend that patients that have been well-controlled on Remicade should remain on this medication unless it is deemed medically-necessary to change therapy. Non-medical infliximab biosimilar switching not only may disrupt our ability to control ocular inflammation but may also result in recurrence of systemic symptoms, failure of previously-effective therapy, and other medication-related side-effects. These complications adversely affect patient quality of life, unduly increase the cost of care, and unnecessarily deplete resources from our medical community. In summary, we recommend that non-medical infliximab biosimilar switching be discouraged, and physician input should be valued and heeded in tailoring an appropriate treatment therapy for ocular and systemic inflammatory disease.
Supplemental Material
sj-docx-1-ejo-10.1177_11206721231199778 - Supplemental material for Effects of non-medical infliximab biosimilar switching in ocular inflammatory diseases: A case series from a tertiary care center
Supplemental material, sj-docx-1-ejo-10.1177_11206721231199778 for Effects of non-medical infliximab biosimilar switching in ocular inflammatory diseases: A case series from a tertiary care center by Andrew H Dolinko, Diana Edem Morvey, Shimy Apoorva, Max Chikovsky, Stephen D Anesi and C Stephen Foster in European Journal of Ophthalmology
Footnotes
Acknowledgements
Many thanks to our patients, without whom this work would not be possible. Special thanks to our research coordinators whose invaluable contributions allow our work to be shared with the medical community through publications.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This report was made possible with funding from the Ocular Immunology and Uveitis Foundation (OIUF, Waltham, MA).
Financial disclosures
Andrew H Dolinko, MD, PhD – Grant support from OIUF. Diana Edem Morvey, MD – Grant support from OIUF. Shimy Apoorva, MD – Grant support from OIUF; Employed by MERSI. Max Chikovsky, MD – Grant support from OIUF; Employed by MERSI. Stephen D. Anesi, MD – Co-owner of MERSI (Co-owner); Grant support from OIUF; Speaker honoraria from Bausch & Lomb, Mallinckrodt Pharmaceuticals, and Eyepoint; Independent Contractor with Santen, Mallinckrodt Pharmaceuticals, Allakos, Eyepoint, and Takeda. C. Stephen Foster, MD, FACS, FACR – President of MERSI; Speaker honoraria from Alcon, Allergan, and Mallinckrodt Pharmaceuticals; Stock options in Eyegate Pharma; Independent Contractor with Aldeyra Therapeutics, Allakos, Bausch & Lomb, Eyegate Pharma, Genentech, Novartis, and pSivida; Current and pending grant support from OIUF, Aciont, Alcon, Aldeyra Therapuetics, Bausch & Lomb, Clearside Biomedical, Dompé Pharmaceutical, Eyegate Pharma, Mallinckrodt Pharmaceuticals, Novartis, pSivida, and Santen.
Credit statement
Andrew H Dolinko: Investigation, Writing – Original Draft, Writing – Review and Editing, Supervision. Diana Edem Morvey, MD: Writing – Original Draft, Writing – Review and Editing. Shimy Apoorva, MD: Conceptualization, Investigation, Writing – Original Draft, Writing – Review and Editing. Max Chikovsky, MD: Conceptualization, Investigation. Stephen D. Anesi, MD: Conceptualization, Writing – Review & Editing, Resources, Supervision, Funding acquisition. C. Stephen Foster, MD, FACS, FACR: Conceptualization, Writing – Review & Editing, Resources, Supervision, Funding acquisition.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.