
Abstract
Purpose
To recognize prognostic factors for better final visual acuity (VA) in patients presenting with submacular hemorrhage (SMH) secondary to exudative age-related macular degeneration
Methods
This retrospective study included patients who presented to a tertiary ophthalmology department between 2012 and 2019 with SMH and were treated by pars plana vitrectomy (PPV) or injection of tissue plasminogen activator (tPA) with pneumatic displacement. Baseline characteristics included demographic data, VA and optical coherence tomography (OCT) characteristics of the SMH. Patients were divided into groups by improvement of at least 2 lines in BCVA (best corrected visual acuity), and by having a final BCVA better than 20/200.
Results
Forty-three eyes of 43 patients were included. Mean age was 86.72 ± 7.18. Prognostic factors for final VA better than 20/200 included better VA at presentation (1.25 vs 1.90 logMAR, p < 0.001), smaller area of SMH in the infra-red image (19.47 mm2 vs 38.45 mm2, p = 0.024), and lower height of SMH as measured by OCT (713.5 µm vs 962.5 µm, p = 0.03). Third of the patients improved in ≥2 lines from presentation, all in the group of the pneumatic and TPA displacement.
Conclusion
Smaller SMHs with good VA at presentation have a better chance for improvement and result in a better final VA. These patients may benefit the most from pneumatic displacement of the SMH with intravitreal tPA and gas.
Keywords
Introduction
Submacular hemorrhage (SMH) is defined as the accumulation of blood between the retina and the retinal pigment epithelium (RPE), which can be caused by several etiologies, including age-related macular degeneration (AMD), retinal macroaneurysms, and other causes. 1 SMH can quickly cause irreversible damage to the retina, due to iron toxicity of hemoglobin, diffusion barrier between RPE and photoreceptors (PR) and mechanical damage to PR. 2

A 74 year old female who presented with a relatively small sub-macular hemorrhage (SMH) in her left eye, visual acuity was 20/40. OCT was obtained upon presentation to the emergency room and is presented in image A; the patient presented with a 23.54 mm2 sub-macular bleeding approximately 2 disc-diameters temporally to the optic disc, without a PED. Overall hemorrhage height was 511 microns and retinal thickness above the bleed was 398 microns. After pneumatic displacement her visual acuity improved to 20/25 and the SMH has shrunk (image B); There was no disorganization of the inner retinal layers and there was an apparent continuity of the external limiting membrane and ellipsoid zone. An OCT image obtained nearly two years after the sub-macular hemorrhage demonstrates a relatively normal foveal contour with an intact photoreceptor layer (image C).

A 98 year old male presented with a large sub-macular hemorrhage in his right eye, visual acuity was 20/70. He had a large 32 mm2 hemorrhage with a 592 micron PED (image A). Overall hemorrhage height was 627 microns, retinal thickness above the hemorrhage was 211 microns and there was disorganization of the inner retinal layers. Additionally, intra-retinal fluid was present and hyperreflectivity can be seen in the outer retinal layers. The patient underwent pars plana vitrectomy with tPA injection, three months after initial presentation the hemorrhage was visibly smaller as can be seen in image B; overall hemorrhage height was 222 microns, retinal thickness above the hemorrhage was 425 microns and PED was also slightly smaller and measured 574 microns. However, there was apparent discontinuity in the ellipsoid zone layer and the patient's visual acuity was 20/200.
Currently two main treatment options for SMH displacement exist. The first is pars plana vitrectomy (PPV) with direct visualization of clot displacement from the fovea and subretinal injection of tissue plasminogen activator (tPA).3,4 The second treatment option is intravitreal injection of tPA followed by pneumatic displacement of the SMH.5,6 Both treatments were compared extensively over the last decades, with recent studies showing comparable anatomical and functional outcomes.7,8
Still, despite prompt treatment and subsequent resolution of the hemorrhage, functional outcomes in these patients often remain poor, due to the abovementioned causes.2,9 Previous studies have explored this topic, searching for prognostic criteria that will help the surgeon inform the patient of expected visual outcomes in their specific case.10–12 However, these studies mainly focused on the cause of hemorrhage, presenting visual acuity and time to treatment.
The purpose of our study was to search for factors predicting improvement in visual acuity in patients presenting with submacular hemorrhage secondary to AMD, specifically on optical coherence tomography (OCT) scans at presentation.
Methods
This retrospective study included consecutive patients who presented to the Retina Unit of Rabin Medical Center between 2012 and 2019 who had been diagnosed with sub-retinal hemorrhage secondary to AMD and treated by PPV or intravitreal injection of tPA with pneumatic displacement as their first intervention. The study was approved by the Rabin Medical Center Institutional Review Board and was performed in accordance with the Declaration of Helsinki. Informed consent was waived due to the retrospective nature of this study.
Study design and participants
Inclusion criteria for this study were SMH secondary to exudative AMD involving the fovea, diagnosed both clinically and by OCT, age above 50 years and duration of symptoms of 14 days or less. Patients were treated either by PPV or by pneumatic displacement of the SMH, according to the discretion of a retina specialist at presentation. Significant cataract or vitreous hemorrhage affecting the view of the posterior pole, or factors affecting patient's ability to maintain face-down head positioning after the procedure were considered as indications for primary PPV. VA at presentation, SMH size or chronicity were not considered as decision criteria. All OCT images were acquired using Spectralis spectral domain OCT (Heidelberg Engineering Inc., Heidelberg, Germany) scanning the central 6 mm * 6 mm scan area.
Exclusion criteria were previous vitreoretinal surgeries, presence of pre-existing macular scarring or any other ocular pathologies including glaucoma and retinal artery or vein occlusion.
Patients treated with intravitreal tPA and subsequent pneumatic displacement of sub-macular hemorrhage were injected with 25 µg/0.1 ml of tPA intravitreally. 1 h later they received another intravitreal injection of 0.4 ml – 0.5 ml of pure gas, either Sulfur hexafluoride (SF6) or Octafluoropropane (C3F8). Patients were examined the next day, and in case the surgeon decided the sub-macular hemorrhage was not displaced sufficiently, the patient was scheduled for PPV within 48 h.
Patients who did not undergo pneumatic displacement underwent 23 or 25-G vitrectomy with subretinal injection of 25 μg/0.1 ml tPA using a 41-G needle until a good subretinal bubble was formed, including most of the hemorrhage area. Intravitreal tamponade at the end of surgery was achieved by air or SF6 gas in non-expansile concentration.
Study endpoints
Data gathered included demographic data, any ocular and systemic history, etiology of SMH, and BCVA (best corrected visual acuity) data at all study visits. All patients had their baseline BCVA extracted from their most recent visit to an ophthalmologist, either at the hospital or at a community clinic, up to one year prior to presentation. The primary intervention chosen by the retina specialist at presentation was also documented, and the time from presentation to intervention.
The criteria we reviewed on OCT included the location of SMH and its dimensions on the infra-red image, central retinal thickness and the retinal thickness above the central hemorrhage area. Other OCT characteristics included the presence of pigment epithelial detachment (PED) and its height, Disorganization of Retinal Inner Layers (DRIL), continuity of the external limiting membrane (ELM) and ellipsoid zone (EZ) and presence of intraretinal or subretinal fluid. Analysis of the images was performed by a retina specialist who was blinded to the patient data or disease course.
Statistical analysis
Patient demographic and clinical data were analyzed using descriptive statistics to compare baseline and follow-up characteristics. The normal distribution of the variables was tested by visual methods (histograms and probability graphs) and analytical method (Shapiro–Wilk tests). The Mann-Whitney U test and Kruskal-Wallis test or paired samples Wilcoxon signed-rank test were applied for continuous variables, and the chi-square or Fisher's exact test when appropriate for nominal variables. All statistical analyses performed were two-sided. Statistical significance was set at a p-value of 0.05. Statistical analysis was performed with Prism version 7 and R version 3.4.2 (R Development Core Team 2017).
Results
Forty-three eyes of 43 patients with SMH were included in the analysis. Mean age of all participants was 86.72 ± 7.18 years (range 70–98 years). Twenty were males and 23 were females. The etiology for SMH in all participants was AMD. Thirty-one patients (72%) had systemic hypertension, 14 (33%) had diabetes mellitus, and 13 (30%) had a history of ischemic heart disease. Nineteen patients (44%) had been treated with anti-platelet treatment, and no patients in the study were on any other anti-coagulation treatment.
Out of the entire study population, 25 (58%) were treated with pneumatic displacement of SMH and 18 (42%) with primary PPV. Median follow-up time was 2.8 years (IQR [1.7, 4.8]).
Mean baseline BCVA of all patients before presenting with SMH was 0.33 ± 0.31 logMAR (equivalent to 20/42). Mean BCVA at presentation was 1.42 ± 0.67 logMAR (equivalent to 20/520) and improved to 1.05 ± 0.65 logMAR (equivalent to 20/224) logMAR at the last follow-up.
Sixteen patients (37.2%) improved by 2 lines or more in the Snellen chart, from the presenting BCVA to the last follow-up visit, and were compared to the other 27 patients in the study (Table 1). Demographic data of the two groups did not differ significantly, and no significant differences in systemic disease was found. All patients who improved by 2 lines or more underwent pneumatic displacement, additional 9 (33.3%) patients who underwent this procedure and all 18 patients in the vitrectomy group improved by less that 2 lines. The location of the SMH and its dimensions did not differ significantly between the groups, although a trend was noted of a smaller area of SMH on the IR image (median 22.89 mm2 vs 31.50 mm2, p = 0.511, Table 1). CMT and the retinal thickness above the hemorrhage were also noted to be higher, and a higher proportion of patients in the improved BCVA had PEDs, this trend was not statistically significant. No difference between the groups was noted regarding the continuity of inner or outer retinal layers.
Comparison according to visual acuity improvement.
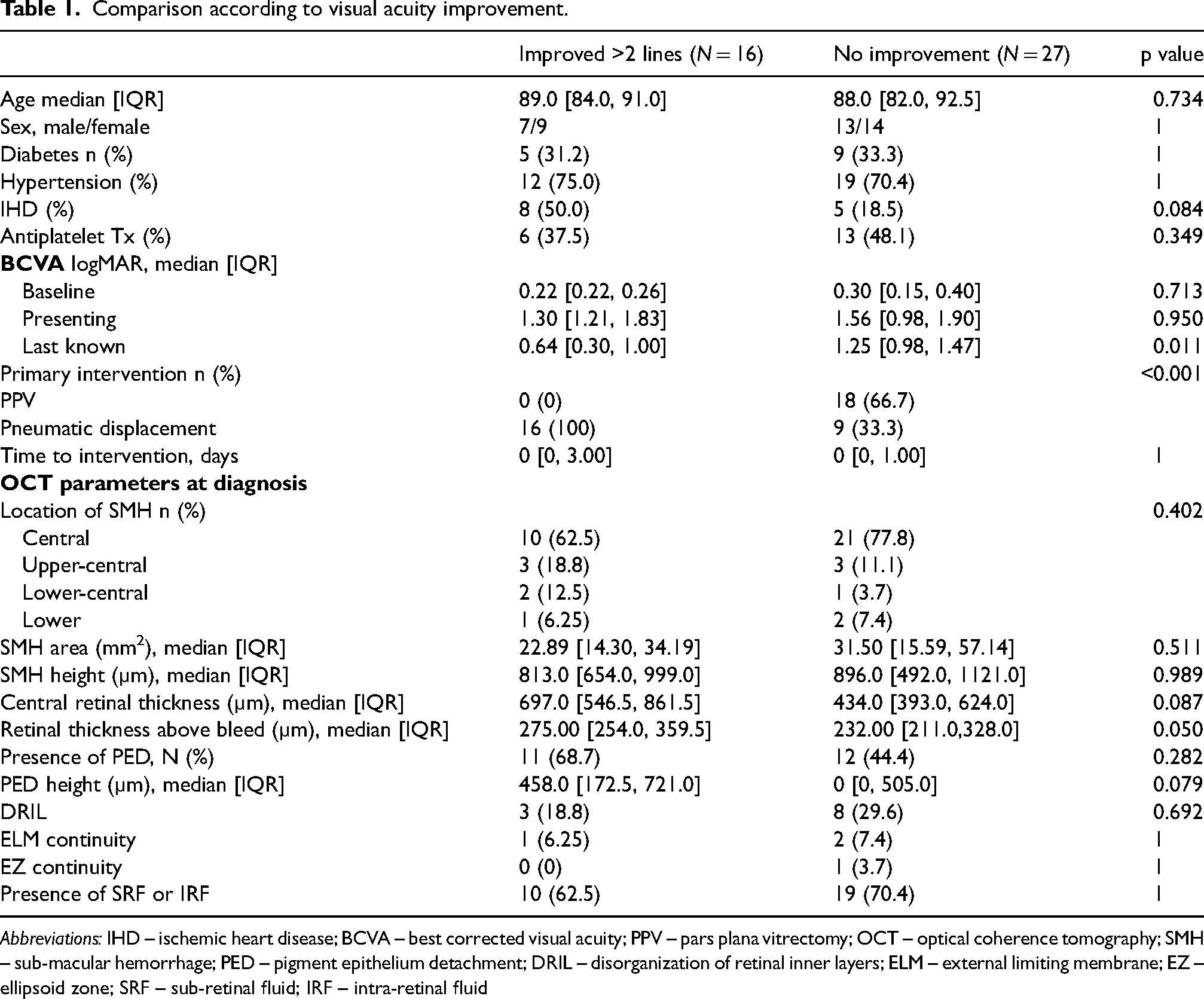
Abbreviations: IHD – ischemic heart disease; BCVA – best corrected visual acuity; PPV – pars plana vitrectomy; OCT – optical coherence tomography; SMH – sub-macular hemorrhage; PED – pigment epithelium detachment; DRIL – disorganization of retinal inner layers; ELM – external limiting membrane; EZ – ellipsoid zone; SRF – sub-retinal fluid; IRF – intra-retinal fluid
A second analysis was performed to compare the 21 patients (48.8%) with a final VA better than 20/200 with the rest of the study participants. While the baseline VA was similar between the groups (0.22 vs 0.30 logMAR, p = 0.318, Table 2), the VA at presentation was significantly better at the group with better final VA (1.25 vs 1.90 logMAR, p < 0.001). More patients in the group with better final VA underwent pneumatic displacement as the primary intervention (81% vs 36.4%, p = 0.005). As can be seen in Table 2, both the SMH area as measured in the IR image (median 19.47 mm2 vs 38.45 mm2, p = 0.024), and the SMH height (median 713.5 µm vs 962.5 µm, p = 0.03) were lower in the group with better VA. No difference between the groups was noted regarding the presence of PED. Continuity of outer retinal layers was demonstrated in 4 patients (19%) in the PD group and was not demonstrated in any of the patients in the PPV group, however this was not statistically significant. Disorganization or inner retinal layers also did not significantly differ between the groups.
Analysis according to patients with visual acuity better than 20/200.
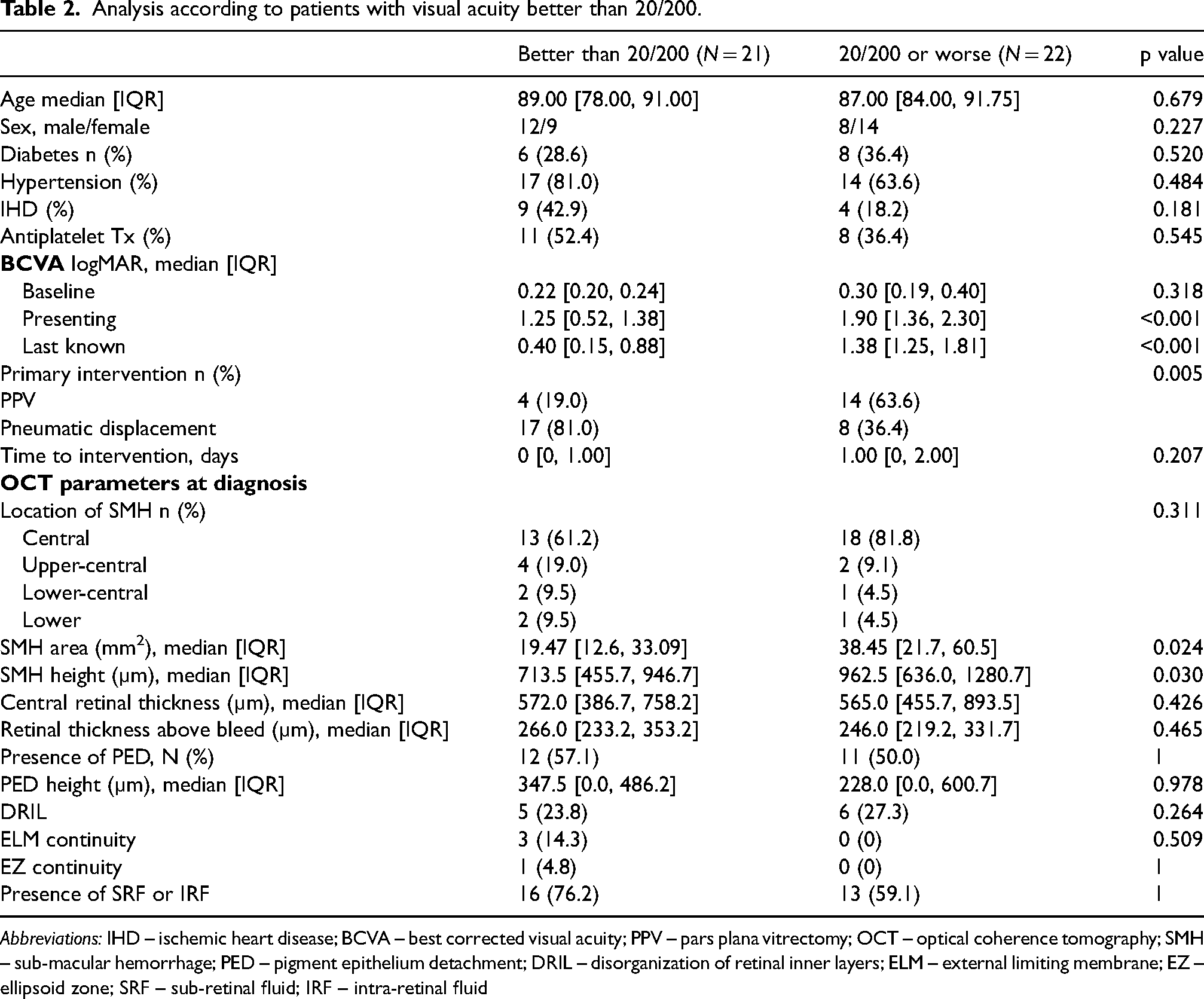
Abbreviations: IHD – ischemic heart disease; BCVA – best corrected visual acuity; PPV – pars plana vitrectomy; OCT – optical coherence tomography; SMH – sub-macular hemorrhage; PED – pigment epithelium detachment; DRIL – disorganization of retinal inner layers; ELM – external limiting membrane; EZ – ellipsoid zone; SRF – sub-retinal fluid; IRF – intra-retinal fluid
We performed a separate analysis comparing the group of patients who underwent PPV with the group that had PD. Comparison of the demographic and other baseline characteristics is shown in Table 3. VA at presentation and final VA were significantly lower in patients who were referred for PPV, although an improvement in VA was shown in both groups (median 1.30 vs 1.85 logMAR, p = 0.008 and 0.87 vs 1.30, p = 0.002, respectively).
Pneumatic displacement vs. Pars plana vitrectomy.
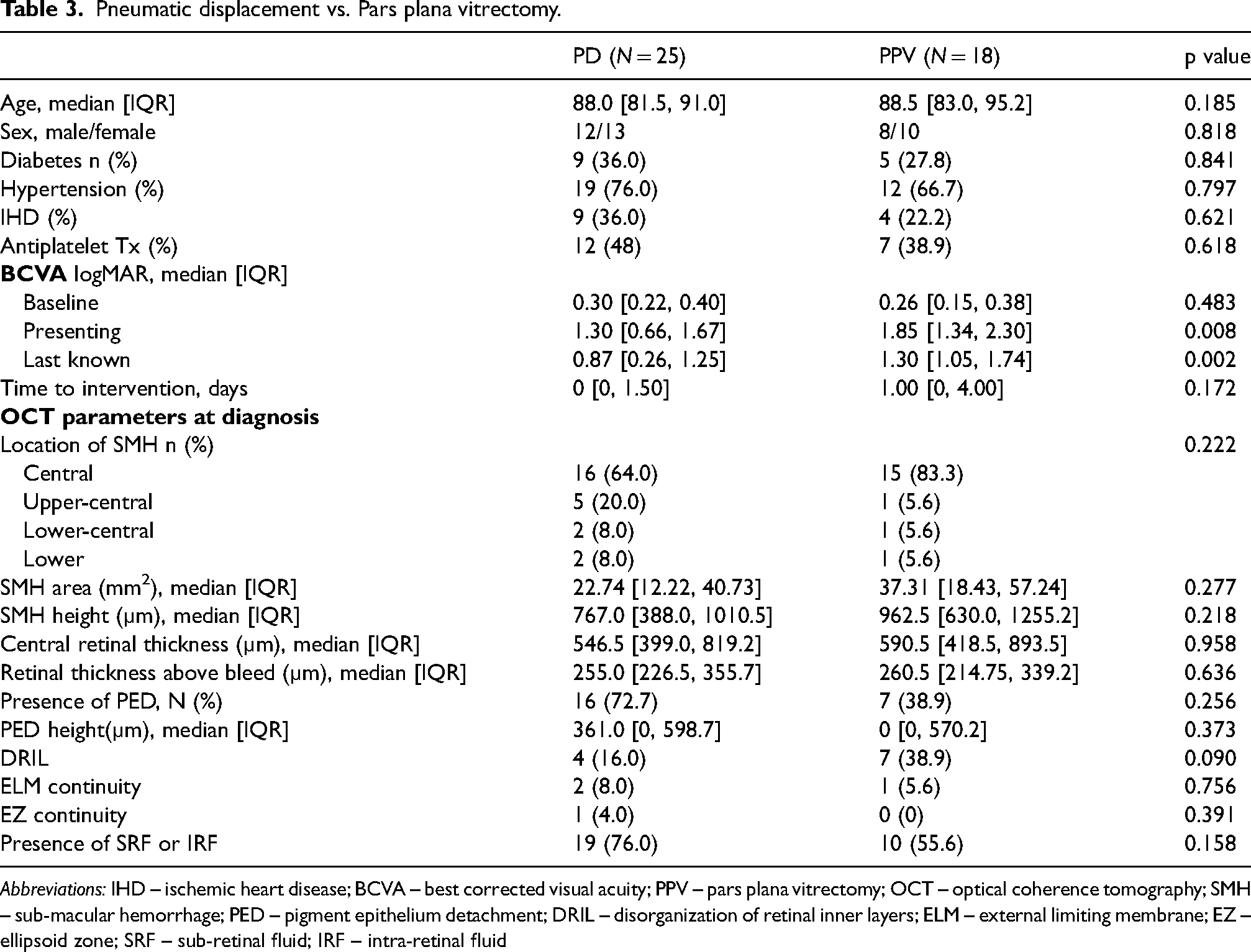
Abbreviations: IHD – ischemic heart disease; BCVA – best corrected visual acuity; PPV – pars plana vitrectomy; OCT – optical coherence tomography; SMH – sub-macular hemorrhage; PED – pigment epithelium detachment; DRIL – disorganization of retinal inner layers; ELM – external limiting membrane; EZ – ellipsoid zone; SRF – sub-retinal fluid; IRF – intra-retinal fluid
Discussion
We found that patients with sub-macular hemorrhage secondary to exudative AMD who had better VA at presentation and smaller SMH size were more likely to turn out with a final VA better than 20/200. Additionally, in our cohort patients who underwent pneumatic displacement with tPA were more likely to improve their VA by at least 2 lines, and to reach a final VA better than 20/200, in comparison to patients who underwent surgical treatment. Our results are in accordance with previous published studies, implying that pneumatic displacement could be beneficial for a specific patient population with good outcome. Such an example can be seen in Figure 1.
Good preoperative VA has been previously shown to predict better final VA,13–15 as was smaller SMH size.9,13,14 For example, Figure 2 shows a case with a very large SMH size and high PED on presentation, with subsequent poor final VA. Although preoperative integrity of outer retinal layers was described in previous studies as a predictor for better final VA,14,16 we did not find that to be the case in our study. We also recognized a trend that higher retinal thickness above the hemorrhage and higher PED in the preoperative OCT were related to a better chance for improvement in 2 lines or more of BCVA.
The question of efficiency of surgical intervention for SMH has been vastly explored in the literature. Moisseiev et al. and Chang et al. have shown in 2 relatively large retrospective cohorts of 31 and 101 patients with SMH, that achieved prompt anatomical displacement of the hemorrhage after PPV with subretinal injection of tPA but had very poor visual acuity outcomes, with a mean final VA of counting fingers and 20/1150, respectively.15,17 These unfavorable results were repeatedly shown in smaller publications in recent years.4,9,16 On the contrary, recent publications exploring intravitreal injection of tPA and gas showed relatively favorable outcomes even in these difficult cases.18,19 Hassan et al. 5 reported a final visual acuity of 20/80 or better in 40% of 15 patients treated with PD, and Papavasileiou et al. 20 reported a median final VA of 20/32.
Several recent medium sized retrospective cohorts comparing the two treatment modalities showed that improvement in VA and final VA was slightly better in PD patients.7,21 A recent publication by our group that compared 107 patients with SMH, 51 of which were treated with tPA-and-gas and 56 with PPV, also found better final VA in the PD group. 8 Moreover, one randomized control trial comparing 24 patients with SMH who were treated with PD vs PPV demonstrated better mean BCVA in the PD group after treatment. This was despite slightly worse preoperative BCVA in these patients. 22
As most of these studies were retrospective, a possible selection bias could partially explain these differences. Patients with more significant underlying retinal conditions, larger SMH or delayed presentation, could have been more likely to be referred for PPV than pneumatic displacement by their treating ophthalmologists. Additionally, as PD requires patients to maintain face down positioning, it is possible that patients who were less likely to adhere to a strict follow-up regimen were also referred for PPV, thus contributing to the less favorable outcomes in this group.
Still, as these results seem to be consistent among different study group over different continents, populations and hospitals, a possible explanation could be related to the subretinal injection of tPA or other factors related to the PPV procedure itself. Fujikawa et al. showed in a relatively large group of 68 patients, that treatment with tPA did not add an adjuvant effect over injection of pure C3F8 gas, 23 and dose dependent retinal toxicity of tPA has been previously shown in vivo and in vitro. 24 However, in most studies comparing PPV with or without intravitreal or subretinal injection of tPA, the groups who did not receive tPA achieved worse final VA results.21,25,26 It is possible that tPA is more toxic when injected into the subretinal space, via higher concentrations of the substance staying for a longer time closer to the photoreceptors. Other possible explanations are the retinotomies sometimes done in these cases, and other maneuvers in the subretinal space, including drainage of the hemorrhage and forced attachment of the retina. In addition, it might be that since PD is an office procedure, patients are treated earlier and subsequently get better VA outcome.
The two main limitations in our study are its retrospective design and medium cohort size. As mentioned previously, allocation bias could partially explain the results. However, as our data represent real world data, we believe that our results are important for clinical decision-making. As SMHs are a relatively uncommon presentation of exudative AMD, and as it was important for us to have high quality OCT images of all study participants, the study cohort is smaller than a previous study done by our group that compared VA outcomes only. However, even with this medium sized cohort, our results are in line with previous published data, providing important data.
In conclusion, our data suggest that smaller SMHs with good VA at presentation have a better chance for improvement and better final VA. These patients may benefit the most from pneumatic displacement of the SMH with tPA and gas. Further large prospective studies are needed to reassure our findings.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.