
Abstract
Purpose
To report spontaneous choroidal hemorrhage with the expulsion of intraocular contents in an elderly female as a complication of microbial keratitis.
Methods
Retrospective case report along with imaging.
Results
A 60-year-old female on treatment for microbial keratitis, presented with protrusion of intraocular contents and no perception of light in the right eye. Ophthalmic ultrasound demonstrated choroidal hemorrhage with coexistent retinal detachment and vitreous hemorrhage. She underwent uneventful evisceration for her condition.
Conclusion
Microbial keratitis needs aggressive medical treatment to prevent associated stromal infiltration and corneal weakening. In cases of microbial keratitis, if spontaneous choroidal hemorrhage occurs, due to thinning of the cornea and compromised integrity of the eyeball, it can lead to the complete expulsion of intraocular contents with unsalvageable loss of vision.
Introduction
Suprachoroidal hemorrhage is a disastrous ocular condition more commonly associated with intraocular surgery. 1 It can occur as limited (ocular contents remain within eye coats) or the more dramatic expulsive type in which intraocular contents are expulsed through the defect in the anterior eye wall structures. Still rarer is the spontaneous occurrence of expulsive choroidal hemorrhage in association with perforation of the cornea or limbus. 2
We report a case of this rare event in an elderly female undergoing medical treatment for microbial keratitis resulting in the expulsion of intraocular contents and permanent loss of vision.
Case report
A 60-year-old Indian female presented to the emergency department of a tertiary care setting with complaints of protrusion of ocular contents in the right eye for the last three days. She was diagnosed with microbial keratitis ten days ago elsewhere and has been treated with topical antimicrobial eye drops (Moxifloxacin and Natamycin 6 times/ day) for the last seven days. She was not suffering from any other ocular infection. There was no history of any surgical intervention or trigger for expulsion like chronic cough or minor trauma.
She did not get much relief and noticed a sudden expulsion of ocular contents with associated pain and minimal bleeding which stopped spontaneously. She sought consultation in the emergency three days after the event. She denies having any systemic illness or intake of systemic medication, nor is there any history of preceding trauma. The cornea and anterior segment of the other eye were normal, with no evidence of thinning/ infection in the other eye. There was no record of thinning or descemetocele of the involved cornea prior to admission.
On ophthalmic examination, vision in the right eye was no light perception. A large, irregular globular reddish-brown hemorrhagic mass consisting of clotted blood admixed with intraocular tissues was found protruding through a large corneal defect with a small rim of peripheral infected corneal tissue adjacent to limbus all around (Figure 1, arrow denoting small peripheral rim of infected corneal tissue). There was no active bleeding. B-scan ultrasound through a closed upper eyelid showed a shrunken globe and choroidal detachment with high internal reflectivity pointing toward the presence of blood with retinal detachment and breakthrough vitreous hemorrhage (Figure 2). Prothrombin time was 10.50 s with an International normalized ratio (INR) of 0.71. Other systemic blood investigations were normal. The left eye had normal fundus and best corrected visual acuity of 6/6 using +1.25 DS and near vision of N.6 using + 2.50 DS.

Extruded intra-ocular contents admixed with clotted blood through a large corneal defect. (Arrow denoting small peripheral rim of infected corneal tissue).
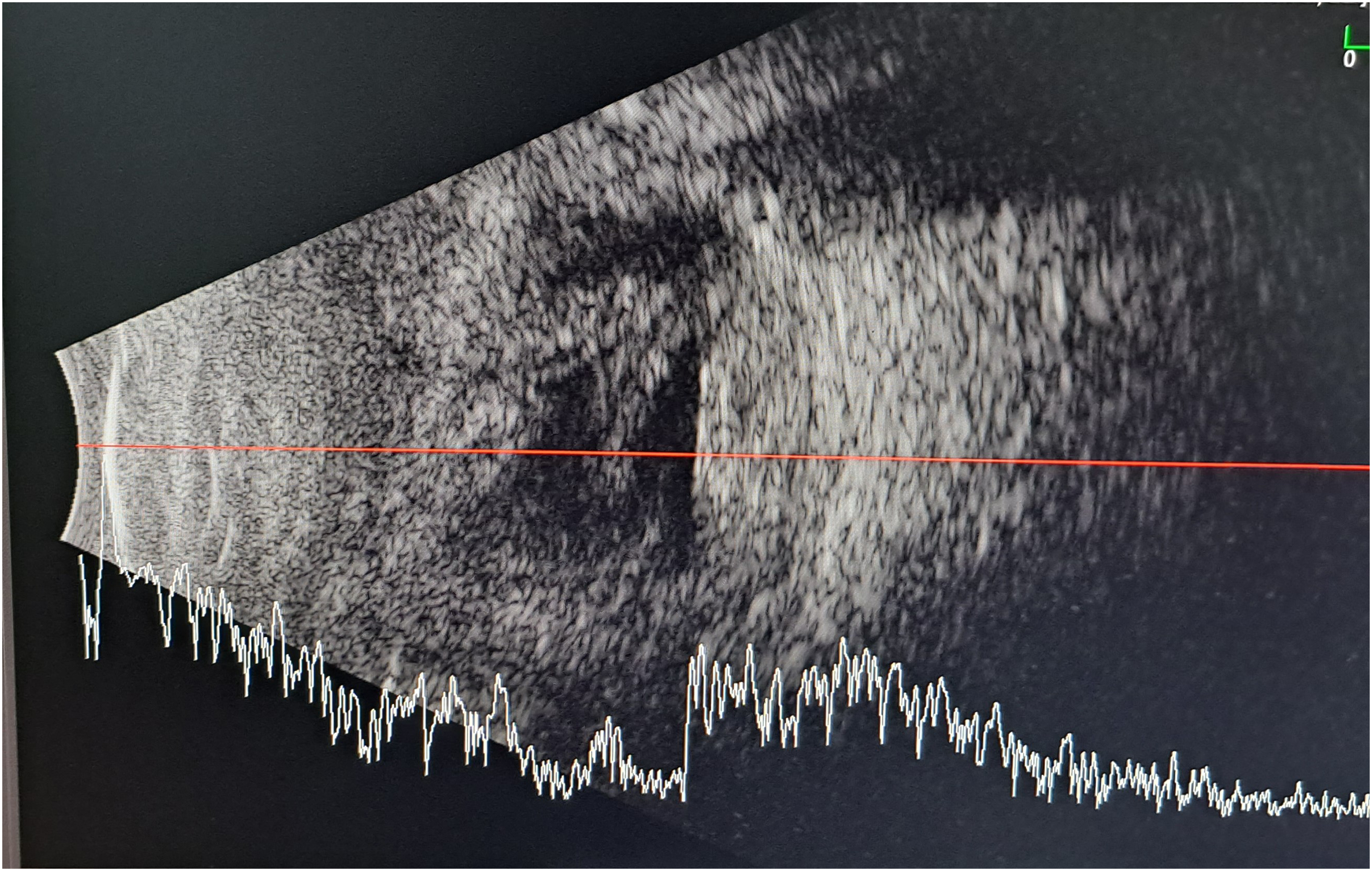
B scan is suggestive of hemorrhagic choroidal detachment with retinal detachment and vitreous hemorrhage.
The diagnosis of spontaneous expulsive choroidal hemorrhage with nil prognosis for vision was explained to the patient. She underwent evisceration with non-implantation of an acrylic ball after informed consent which was uneventful. Histopathological examination of the dissected specimen showed a pigmented epithelial layer and subepithelial stroma showed pigment with numerous dilated and congested blood vessels. Extensive areas of hemorrhage were present. No atypical cells/evidence of malignancy was seen. No microbial organisms could be identified.
Discussion
Spontaneous expulsive choroidal hemorrhage is a catastrophic event that can occur due to predisposing risk factors like older age, atherosclerosis, glaucoma, corneal ulcer 3 with thinning of the diseased eyeball, and intraocular malignancies. 4
Underlying pathophysiological mechanisms postulated in such cases include sudden decompression of the eye leading to ischemia of posterior ciliary arteries precipitating their rupture, 2 hemorrhage in posterior ciliary arteries resulting in raised intraocular pressure and rupture of previously weakened cornea 5 or lastly acute necrosis of the wall of choroidal vessels preceded by breach of corneal barrier.6,7
Microbial keratitis due to Pseudomonas infection has been indicated to show a correlation with spontaneous expulsive choroidal hemorrhage. 8 The patient reported in this study had chronic glaucoma and hypertension as other associated factors with inflammation of choroidal vessels.
Patient-reported in our case study had microbial keratitis for which she received empirical treatment and had not undergone culture or microscopic testing for the underlying infectious cause prior to presentation. Her infection had progressed, as is evident with the involvement of the peripheral cornea up to the limbal area, thus weakening the corneal tissue, which made it vulnerable to perforation or dehiscence in case intraocular pressure rises acutely. It seems that suprachoroidal hemorrhage occurred in this old lady with breakthrough continuous vitreous bleeding resulting in the rupture of the diseased tissue and subsequent expulsion of intraocular contents through the large defect in the cornea. The B-scan picture corroborates the preceding theory in the absence of any mass lesion. Perforation of the cornea, which was localized and leading to the sudden decompression, anterior displacement of the retina and choroid with focal ischemia of posterior ciliary arteries, though plausible, seems less likely. Risk factors like glaucoma, hypertension, use of anticoagulants, and systemic abnormalities were absent in this case.
This case emphasizes the need for appropriate and timely treatment of microbial keratitis to stop the progression of infection and thinning of the cornea. Lack of adequate treatment can result in a thinned cornea predisposed to rupture.
Spontaneous choroidal hemorrhage in an eye with microbial keratitis can lead to the complete expulsion of intraocular contents due to compromised integrity of the eyeball, rendering the eye unsalvageable. Complete expulsion of intraocular contents can potentially be prevented if intensive, adequate, and timely treatment is given in this rare scenario which can improve the visual prognosis and save the eye of the patient.
Declaration of patient consent form
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient has given her consent for her images and other clinical information to be reported in the journal. The patient understands that her name and initials will not be published and due efforts will be made to conceal her identity, but anonymity cannot be guaranteed.
Footnotes
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.