
Abstract
Background
Intermittent exotropia (IXT) is one of the most common forms of strabismus usually seen in the pediatric age group, the prevalence of IXT is higher in Africa and the Middle East. IXT treatment strategies include both surgical and non-surgical methods, non-surgical management is preferred in general as it is less invasive and avoids the risks associated with surgery and anesthesia.
Aims
This study aims to determine the effectiveness of patching therapy for the treatment of IXT in different age groups and to compare the success of patching therapy in preventing surgery in IXT patients in different age groups.
Methodology
A retrospective chart review was conducted from September 2022 until February 2023 at King Abdulaziz University Hospital in Riyadh. The data was collected retrospectively from electronic medical records from 2016 to 2021 of all patients diagnosed with IXT and were managed by patching therapy fitting the inclusion criteria.
Results
A total of 76 patients with IXT enrolled in the study with 56.5% of the participants were older than 7 years old. Overall, there was no improvement in the angle of deviation but 34% of patients had improved control over the follow-up period. 55.3% of the participants didn't require surgery. Younger age, longer duration of patching per month, and good compliance were significantly associated with treatment success.
Conclusion
Younger age groups were more likely to benefit from patching therapy than older age groups, and good compliance to patching therapy is an important factor in preventing the need for surgery.
Introduction
Strabismus is a common ocular condition seen usually in pediatric age group and refers to any misalignment of the eye and may be referred to as squint. 1
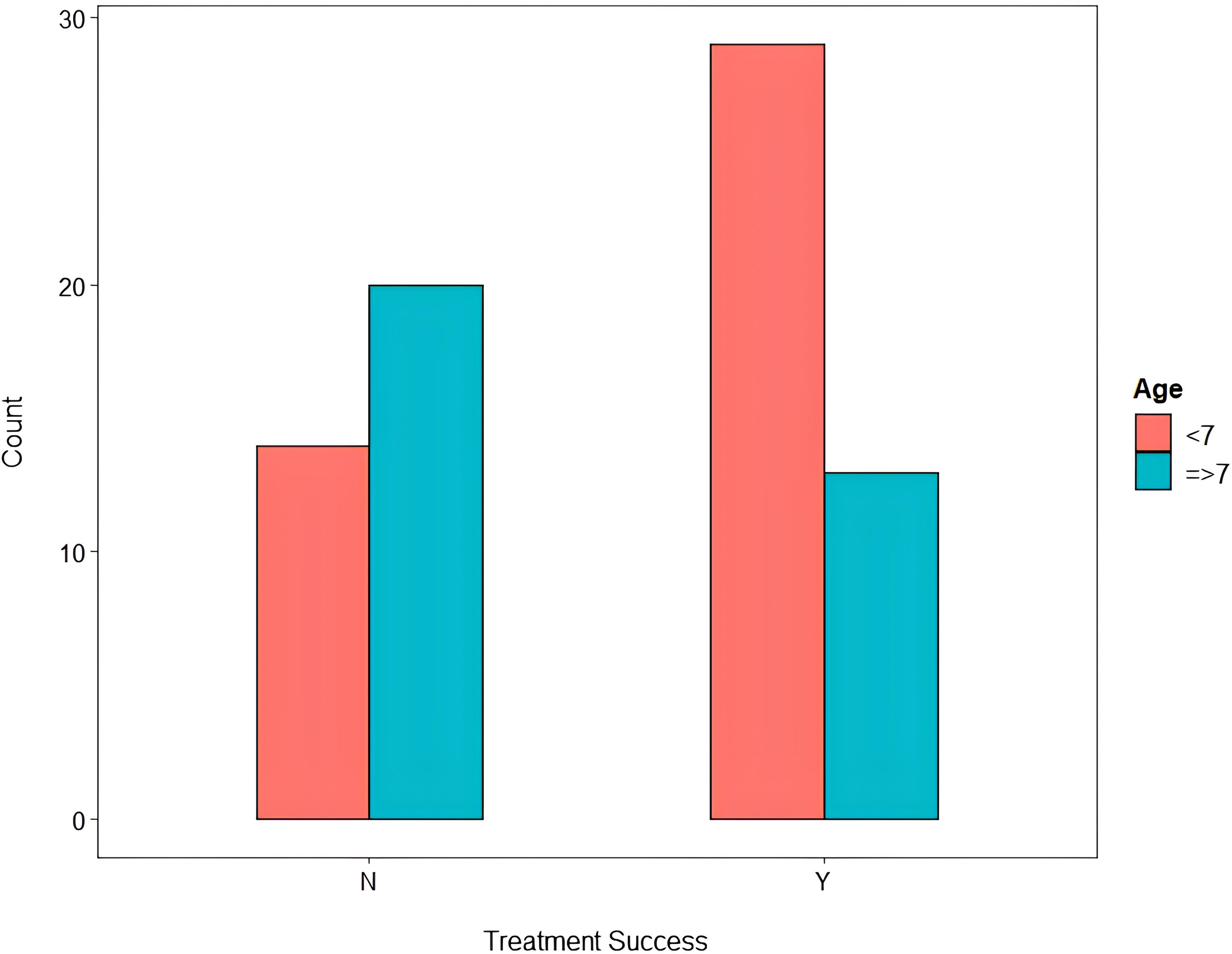
Distribution of treatment success according to age groups.
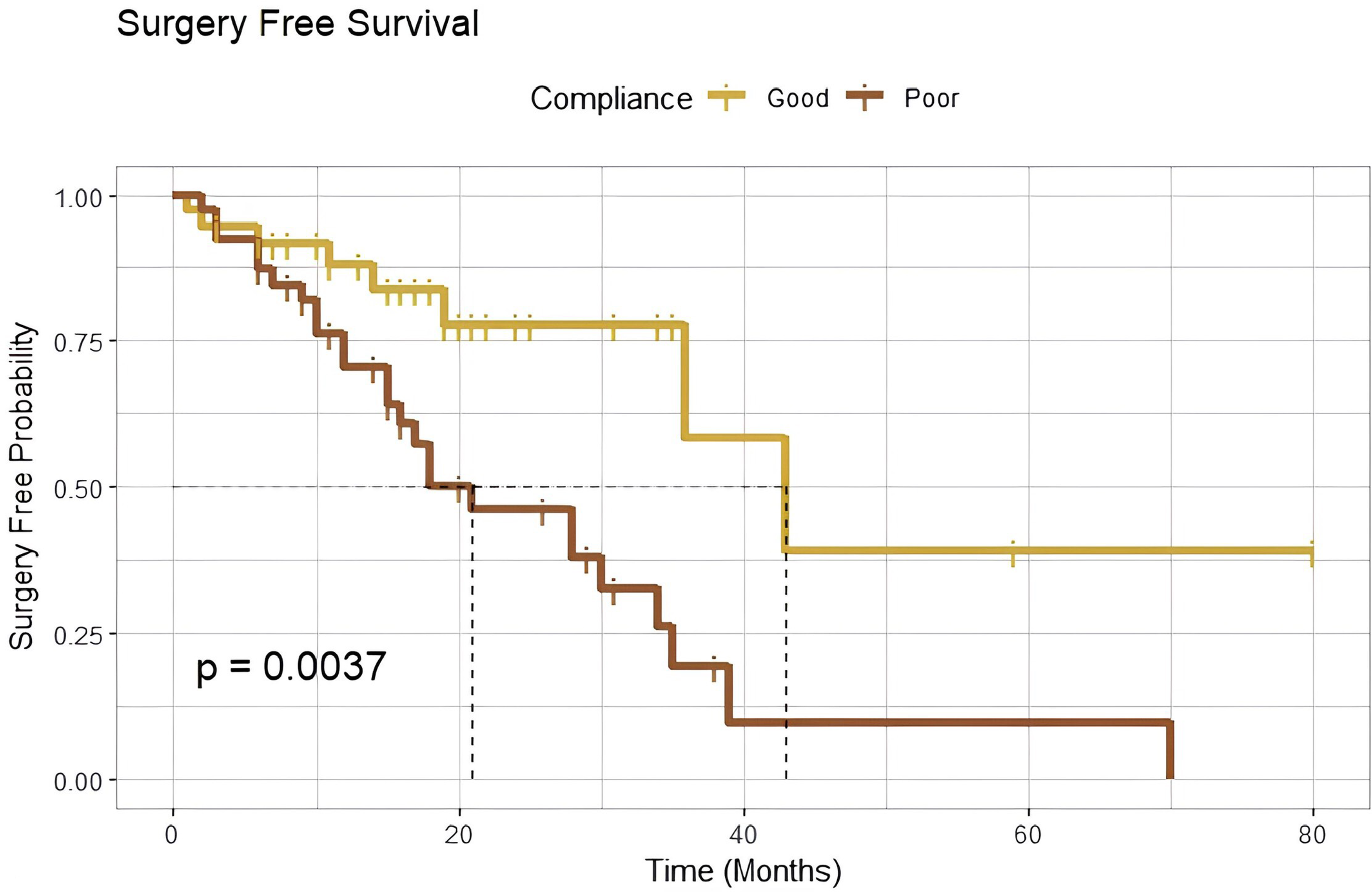
Kaplan-Meier curve of differences in surgery free survival based on compliance.
Strabismus affects approximately 5% of children with normal development and 25% of them being exotropia. 2
Intermittent exotropia (IXT) is the most common form of strabismus with females nearly twice more affected than males.3,4 A large meta-analysis study estimated that the prevalence of strabismus to be 1.9%, with exotropia the most common form with the prevalence of 1.23%. 5 The prevalence of IXT is higher in Africa, Middle east and East Asia in comparison to the USA and central Europe, sun exposure is believed to be a factor that explains that variance.2,6
Patients with IXT are usually asymptomatic, however sometimes they can present with occasional horizontal diplopia or vague discomfort feeling when their eyes are deviated. 7
The treatment strategy for IXT is determined by the angle of deviation and the patient's ability to control it. 8
IXT treatment strategies include both surgical and non-surgical methods, the latter is preferred in many patients with smaller angle of deviation or better control, non-surgical methods are also preferred in very young children who may develop amblyopia due to the possibility of overcorrection during surgical procedures.8–10
There is a wide variety of non-surgical methods used to treat IXT which include patching therapy, correction of refractive errors (myopia or very high hyperopia), overcorrecting minus lens therapy, prism therapy, and orthoptics/binocular vision therapy. 8
Patching therapy is one of the non-surgical approaches to IXT management. There are many different patching therapy techniques, including alternate or monocular patching. Alternate patching is used when there is no dominant eye, while monocular patching is used when there is a dominant eye. 9
The mechanism by which patching helps in intermittent exotropia is not completely understood. It is suggested that it disrupts binocular stimulation thus reducing suppression to prevent diplopia and could additionally promote motor fusion,9,11 moreover the angle of deviation could be reduced by patching therapy, turning it from exotropia to exophoria. 9
Purpose of the study
This study aims to determine the effectiveness of patching therapy for the treatment of intermittent exotropia in different age groups. It also aims to compare the success of patching therapy in preventing surgery in IXT patients in different age groups. Lastly, it measures the factors that lead to treatment success of patching therapy by preventing surgery.
Methodology
Study location
A retrospective chart review that was conducted in King Abdulaziz University Hospital (KAUH), Riyadh, Saudi Arabia over a 6-month period from September 2022 to February 2023. It was conducted among all patients diagnosed with intermittent exotropia and managed with patching therapy. The study was approved by The Institutional Review Board (IRB) and Ethical Committee of King Saud University (E-22-6953).
The sample size was determined to be 76 participants, we included all patients that fit the inclusion criteria described below.
Data collection
The data was collected retrospectively from electronic medical records, and we included all patients diagnosed with intermittent exotropia and were managed by patching therapy between 2016–2022 in King Abdulaziz University Hospital (KAUH) in Riyadh. We excluded those who had undergone ocular surgery, anyone with sensory deprivation exotropia, and patients with poor vision in one eye (e.g., amblyopia, anisometropia). Participants anonymity was assured by assigning each participant with a code number for the purpose of analysis only.
Data collected from the study participants’ medical records were divided into four categories, patient demographics (Age, gender, diagnosis, and visual acuity), factors related to patching therapy, factors related to disease severity, and factors related to treatment outcomes.
Factors related to patching therapy included duration of patching in months from the visit that patching therapy was prescribed to the patient until the patient stopped patching or the last available visit, it also included the daily duration of patching (in hours) along with the patched eye (either left, right or alternate patching), compliance to patching was also collected and divided into either good or poor compliance according to the treating physician's documentation.
Factors related to disease severity included deviation angle at near and distance, it was measured using prism alternate cover test (PACT) by the treating physician and documented in Prism Diopters (PD), it also included deviation control score at near and distance (excellent, good, fair, and poor) documented by the treating physician according to Kushner's classification. 12 These factors were collected in three different visits (baseline visit, second follow-up visit at 3–6 month past the baseline visit, and final follow-up).
Factors related to treatment outcomes were angle difference between the last and first visit (at near and distance), and most importantly treatment success which was defined as those who did not require surgery throughout the observation period.
Statistical analysis
Statistical analyses were conducted using Rstudio (version 1.4.1717). Continuous variables were described using mean and standard deviation (SD), while categorical variables were described using counts and percentages. Paired t-tests were used to compare continuous variables between paired observations, and Cochrane’s Q test was used for categorical variables. The assumptions of each test were carefully checked to ensure the validity of the analyses. The Kaplan-Meier method was used to explore factors associated with surgery-free survival (treatment success) by the final visit, and significance was tested using the log-rank test. Cox proportional hazards models were used to identify and adjust for factors associated with surgery-free survival. A significance level of 0.05 was used for all statistical tests. If any data were missing, they were excluded from the analysis.
Results
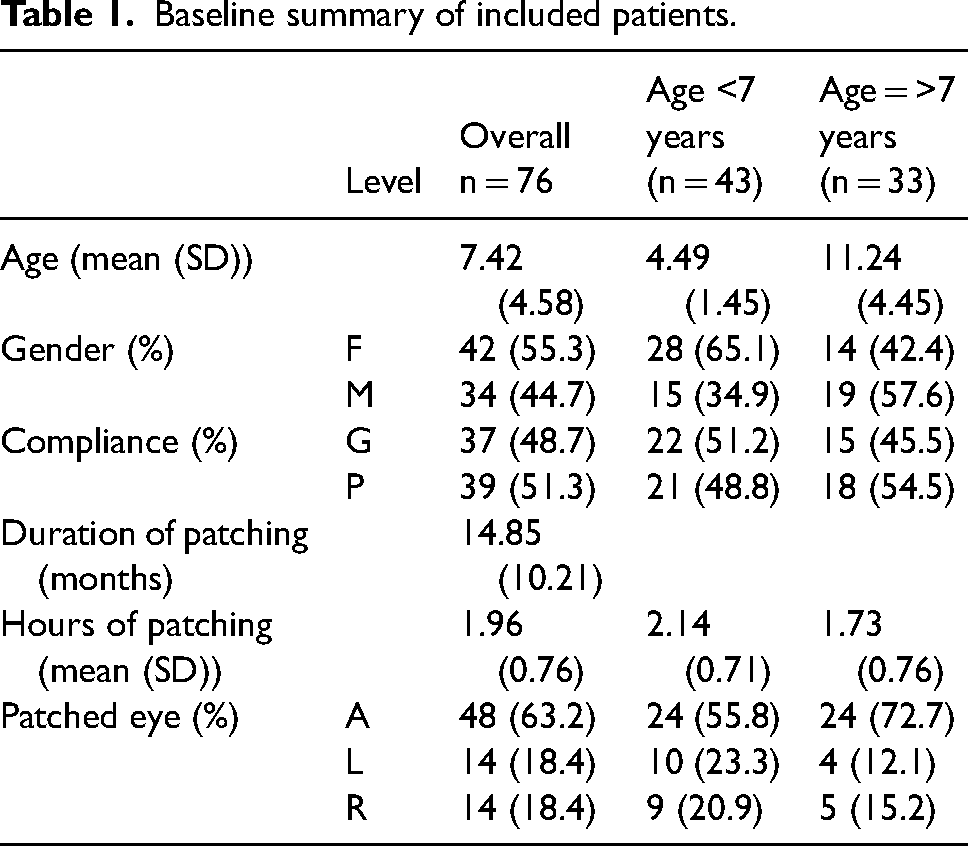
A total of 76 patients were enrolled in the study, the mean age was 7.42 (SD = 4.58) years. 56.5% of the participants were younger than 7 years old. And most of the patients were females (55.3%). The average duration of patching was 14.85 (SD = 10.21) months, and most patients were undergoing patching therapy for 2 h per day. Approximately half of the patients (51.3%) had poor compliance to patch therapy. Baseline characteristics are summarized in (Table 1).
Baseline summary of included patients.
We found no significant changes in deviation angle at near (p = 0.24), deviation angle at distance (p = 0.84), after comparing the angle difference at the three visits. However, 55.3% of patients did not require surgery (treatment success) (Figure 1), which was our primary outcome for this study. The average angle difference at near was −2.12 (SD = 9.12) (which means the angle on average deteriorated over time), while the average angle difference at distance was 0.09 (SD = 8.49). Twenty-six (34.2%) patients exhibited improvement of control over time, however, there was no significant difference between groups stratified by age. (Table 2).
Main outcomes of the study.
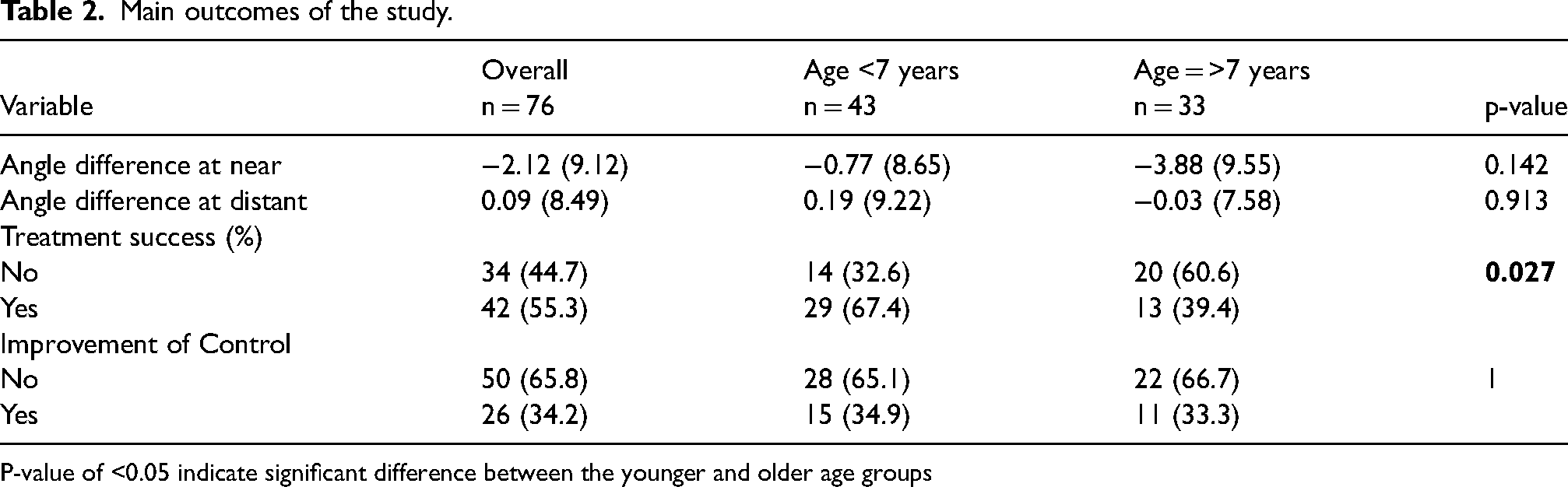
P-value of <0.05 indicate significant difference between the younger and older age groups
Regarding survival analysis, we applied the Kaplan-Mier method and found that duration of patching in months (log-rank test = 0.019), daily duration of patching in hours (log-rank test = 0.017), and compliance (log-rank test = 0.0037) were statistically significant (Figure 2). For cox regression we found consistent results. We found that patients with poor compliance to patching therapy were more likely to undergo surgery compared to patients with good compliance (HR = 3.11, 95% CI [1.39, 6.93], p = 0.006). Patients who had a duration of patching ≥12 months were less likely to undergo surgery, compared to patients with a duration of patching <12 months (HR = 0.43, 95% CI [0.21, 0.88], p = 0.02). Patients who had one hour of patching per day were more likely to undergo surgery compared to those who had more than one hour of patching per day (HR = 2.5, 95% CI [1.15;5.43], p = 0.02). (Table 3).
Cox regression model for predicting the need for surgery.
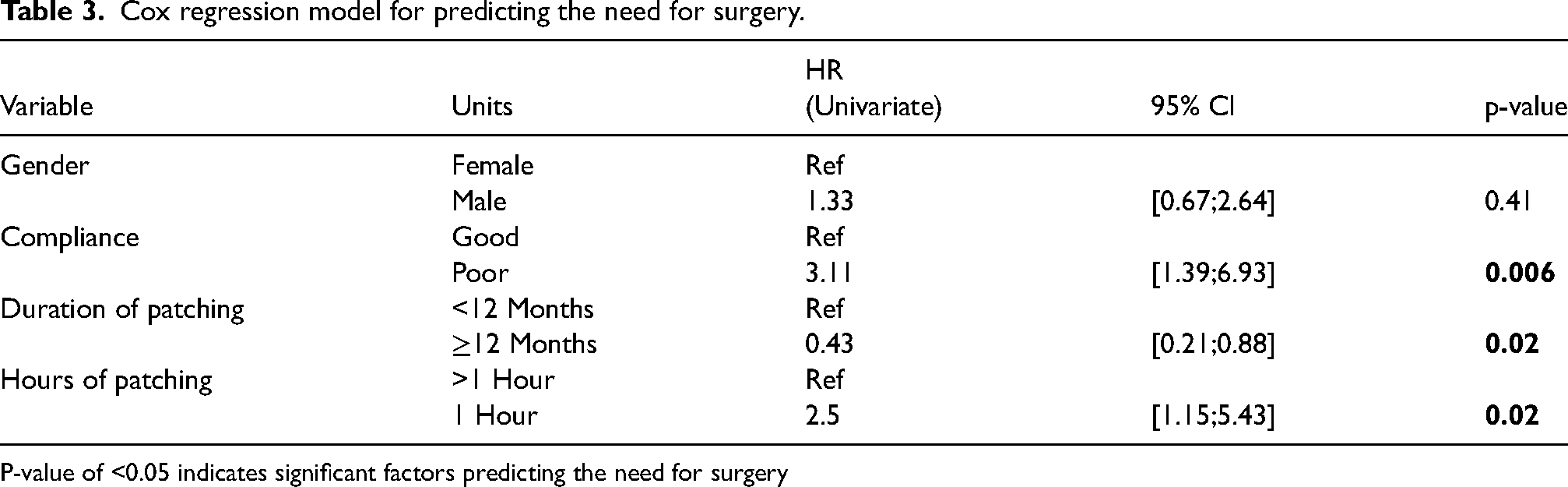
P-value of <0.05 indicates significant factors predicting the need for surgery
Younger age (OR = 2.81, p = 0.03) and good compliance (OR = 6.47, p = 0.0003) were associated with less need for surgery, and this was statistically significant in the logistic univariate regression analysis. (Table 4).
Logistic regression model for predicting the need for surgery.
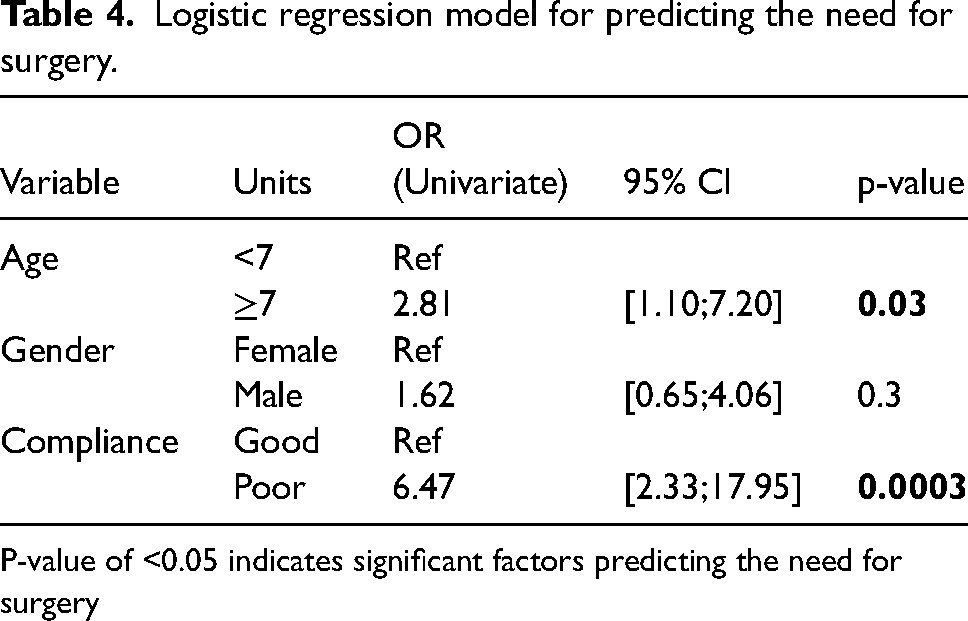
P-value of <0.05 indicates significant factors predicting the need for surgery
Discussion
Strabismus is a common ocular disease typically observed in children and refers to any misalignment of the visual axes. 1 Strabismus has many different types, and it could lead to many different complications, especially in children. It could lead to amblyopia, which is difficult to treat if not treated early.
Intermittent exotropia (IXT) is the most prevalent form of strabismus. A large meta-analysis estimated that the prevalence of strabismus to be 1.9% with exotropia being the most prevalent form at 1.23%. 5
Even though it is the most prevalent form of strabismus in childhood, the most effective conservative treatment modalities in different age groups are still unclear. patching therapy is proven to be effective in the conservative management of IXT, however, there is scarcity of studies comparing the effectiveness of patching therapy in young versus older age groups. Our study aimed to assess the effectiveness of patching therapy between different age groups (<7 and ≥7 years).
Clinical practice of IXT revolves around assessing whether the patient would benefit more from conservative or surgical management. The latter is usually indicated when there is loss of motor control or worsening of sensory fusion.13,14 We defined treatment success as the patient not requiring surgery in the last visit based on the treating physician's decision.
Many studies in the literature showed that IXT affects females more than males, which was similar to our study where we found that IXT is slightly more common in females than males but that was not statistically significant.3,4,15 The distribution between good and poor compliance in our study was nearly equal, however, the older age group had slightly worse compliance.
Many studies were conducted on IXT patients to determine the effectiveness of patching therapy showed that most of the patients benefited from patching therapy either by improvement of the angle or delaying the need for surgery,12,16–19 on the other hand, our study did not find any significant difference in the angle of deviation at near and distance (p = 0.24 and p = 0.84 respectively) during the observation period. However, there was improvement in control in 34% of patients.
Most patients (67.4%) younger than 7 years of age did not require surgery (treatment success) while only 39.4% of patients older than 7 years did not require surgery which was shown to be statistically significant (p = 0.027, OR = 2.81). Similarly, Kushner et al studied 279 patients with IXT on patching therapy, this study showed that there is a parallel increase of the likelihood of requiring surgery with age. 12 One point to consider is that the older group in our cohort had worse compliance with patching (54.4%) which may have contributed to the physician's decision to the need for surgery.
This shows that patching therapy is an effective management option in deferring the need for surgery in patients with IXT, especially in younger age groups, which is beneficial for many reasons, as some studies mentioned that patients with IXT undergoing surgery at a younger age are more likely to develop complications of overcorrection and worse sensory outcomes, on the other hand patients who undergo surgery at an older age are less likely to have these complications.20–22
To the best of our knowledge, there is nothing in the literature that studies the compliance to patching therapy in patients with IXT patients in preventing the need of surgery as it's a subjective measure that is difficult to assess, we categorized the patients to either poor or good compliance depending on the treating physician's documentation. We found that patients who had a poor compliance to patching therapy were more likely to need surgery (HR = 3.11, p = 0.006) than those with good compliance. Furthermore, being compliant with patching therapy is beneficial even if surgery was needed in the future, Shin et al investigated the effect of preoperative part-time patching therapy on long-term surgical success in IXT and found that preoperative patching therapy increases surgery success rate and reduces the recurrence rate after surgery. 23
Furthermore, in our study there is a statistically significant association between those who had duration of patching >12 months and treatment success. However, it's less likely to be clinically important as it might be attributable to the fact that patients with a stable condition are more likely to continue with patching therapy.
Our findings also showed that patients who had one hour of patching per day were more likely to need surgery than patients who had more than one hour of patching per day (2.5 HR, P-value = 0.02), this suggests that different daily duration of patching results in different outcomes, however more studies are required to assess the optimal daily duration of patching as it is variable in the literature. 19
The results of this study might encourage clinicians to focus more on counseling patients and their parents on the benefits of good compliance once patching therapy is prescribed to the patient. It may also encourage policy makers to make programs for screening and campaigns to raise awareness about IXT and the benefits of its early diagnosis and management.
Further research with a larger sample size from multiple centers is needed to make solid evidence and generalization, as the sample size of this study was relatively small and from a single center. Moreover, the retrospective nature of this study is one of the limitations, therefore future prospective and clinical trial studies under controlled study settings are needed. It's also worth mentioning that our study included all patients with IXT who underwent patching therapy regardless of their initial control status. To the best of our knowledge, no study in the literature compared different conservative management methods in different age groups, therefore we advise future randomized controlled clinical trials comparing the effectiveness of different conservative management methods in different age groups.
Conclusion
In conclusion, patching therapy for intermittent exotropia is an effective method in delaying or reducing the need for surgery in some patients. Younger age groups were more likely to benefit from patching therapy than older age groups, and good compliance to patching therapy is an important factor in preventing the need for surgery.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical statement
The study was approved by The Institutional Review Board (IRB) and Ethical Committee of King Saud University (E-22-6953).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article