
Abstract
Objectives
To evaluate the validity and reliability of the new Fast Assessment of the Ocular Surface Trouble (FAST®) questionnaire for identifying glaucoma or ocular hypertension (OHT) patients at risk of ocular surface disease (OSD).
Methods
A multicenter, international, cross-sectional, epidemiological survey evaluated the most accurate interview items and ocular signs on the initial 14-item version of FAST® to develop a shorter version for routine, quick clinical use. Rasch analysis and least absolute shrinkage and selection operator (LASSO) method was used to reduce the number of items on the questionnaire. Sensitivity and specificity of FAST® were assessed with receiver operating characteristic (ROC) curves for the detection of OSD with the questionnaire and ophthalmic assessment.
Results
A total of 2308 eyes (1154 patients) were analyzed in this study by 92 ophthalmologists. The initial version of the FAST® indicated 60% of the subjects had OSD. Rasch analysis allowed removal of some clinical signs. The LASSO method allowed elimination of some items from the original questionnaire for a 9-item and a 6-item version of FAST®. For the 6-item questionnaire, the sensitivity and specificity were 71.9% and 74.3% respectively and the area under the curve was 0.815.
Conclusions
The FAST® questionnaire is a valid and reliable tool for use in routine clinical practice and in clinical trials. The short versions of the questionnaire allow quick detection of the majority of patients with OHT or glaucoma at risk of dry eye.
Keywords
Introduction
Most glaucoma patients are prescribed one or more topical drops. However, topical therapy is associated with ocular surface abnormalities, that reduce drop tolerability and patient adherence to therapy thereby increasing the risk of progression of glaucoma. 1 Ocular surface disease (OSD) is associated to preservatives in glaucoma medications.2,3 Additionally, the risk of dry eye and ocular toxicity increases with longterm use of preservative-containing topical medications.1–6
Clinically significant dry eye is reported in up to 52% of open angle glaucoma patients and tear film disruption in up to 78% of glaucoma patients.7,8 Despite the high prevalence, little attention is paid to this issue due to the perception that detecting OSD in glaucoma patients requires extensive workup with a low yield. 6 Given the longterm use of topical glaucoma therapy, timely detection of OSD may increase patient adherence, potentially leading to better clinical outcomes.9–11
The Fast Assessment of Ocular Surface Trouble (FAST®) questionnaire was developed to detect the risk of abnormal ocular surface in patients with glaucoma or ocular hypertension (OHT) in routine clinical practice. This questionnaire was designed by a group of glaucoma experts and OSD experts as a rapid screening tool for detecting OSD.
Initially a 14-item version of the FAST® questionnaire was developed that consisted of a patient interview component to identify risk factors and symptoms related to OSD. The other part of the questionnaire was filled out after clinical examination by highlighting abnormal ocular signs. The idea was to perform only a limited number of procedures that could be used for screening or follow-up.
However, the introduction of any new patient questionnaire requires validation and clinical use may warrant changes to reflect the experience in real world settings. During initial testing of the original FAST® questionnaire, ophthalmologists suggested developing a shorter version that could be performed in less than 2 min and reliably detect patients at risk for OSD. The current study includes the validation study of the initial 14-item questionnaire that was used to determine the most accurate questions for developing a shorter version for use in routine clinical practice for assessing the risk of OSD in glaucoma or OHT patients.
Methods
This multicentre, international, cross-sectional, epidemiological survey evaluated the most accurate items on the initial FAST® questionnaire to develop a shorter version. Clinical research guidelines specific to each country were followed and this study adhered to the tenets of the Declaration of Helsinki. Each study site received research ethics committee approval.
The initial (original) version of the FAST® questionnaire (Figure 1A) contains 14 items in 2 parts. Part 1 is a 9-item patient interview with binary or ordinal responses. Part 2 is a 5-item clinical exam section related to OSD diagnosis that is completed by an ophthalmologist. Part 1 consists of short essential questions to identify risk factors and ocular symptoms between instillations.

(A) Original 14-item version of the FAST® (fast assessment of ocular surface trouble) questionnaire for the evaluation of risk of ocular surface disease in patients with glaucoma or ocular hypertension. (B) Nine-item version of the FAST® (Fast Assessment of Ocular Surface Trouble) questionnaire for evaluation the risk of ocular surface disease in patients with glaucoma or ocular hypertension. (C) Six-item version of the FAST® (Fast Assessment of Ocular Surface Trouble) questionnaire for evaluation the risk of ocular surface disease in patients with glaucoma or ocular hypertension.
Risk factors were queried with binary (yes/no) responses for: existing OSD unrelated to glaucoma; use of artificial tears or anti-allergy agents; history of halting topical glaucoma therapy due to medication intolerance; possibility of surgery in the following months/years; (yes/no) and the number of preserved glaucoma drops per day (0, 1, 2, 3 or more). Questions on ocular symptoms between instillations with ordinal assessment (No/Mild/Moderate/Severe) included: itching/irritation, dry eye, burning, eyelid crusts or secretions.
Clinical measurement of ocular signs
An ophthalmologist noted ocular signs from clinical examination for each eye as: No/Mild/Moderate/Severe for conjunctival hyperemia, eyelid redness, fluorescein corneal staining, fluorescein conjunctival staining. Corneal and conjunctival fluorescein staining was graded with National Eye Institute criteria. 12 Tear production was assessed with the Schirmer 1 test. Tear film break up time (TBUT) was graded as: normal > 10 s; abnormal < 10 s; dry eye < 5 s.
Global score
Using the variables from the original and shorter versions of FAST® questionnaire, composite respective OSD scores were generated to determine OSD status.
Study sample
Patients were enrolled by 92 ophthalmologists from Belgium, France, Italy, Poland, Spain and UK. Consecutive patients with glaucoma or OHT were enrolled if they were ≥18 years, presenting for routine ophthalmic consultation and signed a written informed consent for study participation. Patients with corneal ulcers or severe ocular pathology were excluded.
Statistical methodologies
A – Rasch analysis (graded response model)
Originally, Rasch analysis was performed to determine whether the items in the ocular signs section provided good psychometric properties for measuring OSD and whether some clinical exams required modification, removal or graded responses. The graded response model was used for data from each country and on pooled data from all countries.
B – LASSO method (least absolute shrinkage and selection operator method)
Development of shorter versions of the FAST® questionnaire
Subsequently, the LASSO method was used to reduce the number of items in the questionnaire with the objectives of maintaining sensitivity and specificity for identifying patients at risk of OSD. To reduce the items of this predictive model, the aim was to eliminate variables that were not associated to OSD. OSD was defined based on binary (yes/no) responses on the presence/absence of risk factors, ocular signs and symptoms. Eleven variables were evaluated including two clinical exams, conjunctival hyperemia and eyelid redness (‘clinical exams’ in the rest of the manuscript refers to only these exams). Multiple models were tested based on differing clinical criteria.
LASSO was used to select the best model using the area under the curve (AUC) of receiver operating characteristic (ROC) graphs. In this method, less important coefficients were assigned a zero value in order to select the best model. A further modification of the LASSO model (LASSOlite) allowed selection of variables based on AUC ± standard error. This method determined the most highly correlated variables for inclusion in the shorter questionnaires.
Each eye of a patient was considered an independent unit. Eyes were randomized to training and test sets and a 2-fold cross validation test was used to determine mean AUC.
Reliablity
Cronbach α, a measure of internal consistency, was used to test the reliability of the original and short versions of FAST®.
Validity
Validity of the original and short versions was evaluated by assessing for significant differences in OSD detection between the questionnaire and ophthalmologist assessment. ROC curves allowed evaluation of the sensitivity and specificity of the original and short versions for detecting OSD with the questionnaire and ophthalmologist assessment.
Results
There were 1278 patients enrolled in this study as follows: Belgium (185 patients); France (96 patients); Italy (161 patients); Poland (434 patients); Spain (302 patients); United Kingdom (100 patients). Some missing data reduced the sample to 2308 eyes (1154 patients) for the analysis. The outcomes of the original version of the FAST® questionnaire indicated 60% of the glaucoma or OHT patients had OSD.
Rasch analysis of the 14-item FAST® questionnaire
Rasch analysis simplified the questionnaire by decreasing the number of variables in the questionnaire and retaining only the presence/absence of the ocular signs and symptoms with severity grading. Pooled data analysis indicated considerable overlap of category characteristic curves for corneal fluorescein staining (FCORN) and conjunctival fluorescein staining (FCONJ) (Figure 2A). The curves for moderate and severe grading for each category were poorly separated (Figure 2). Item response category curves for grading of the ocular signs and symptoms show the curves for RED and CONJ were superimposed (Figure 2B). Similarly, the curves for FCORN and FCONJ were superimposed (Figure 2B). Hence only one test was retained and then only the presence/absence of the retained variable was noted. Analysis indicated differences in data from UK and Italy that excluded both countries from the pooled analysis. Language translation difficulties and differing clinical practices resulted in data exclusion of both countries.
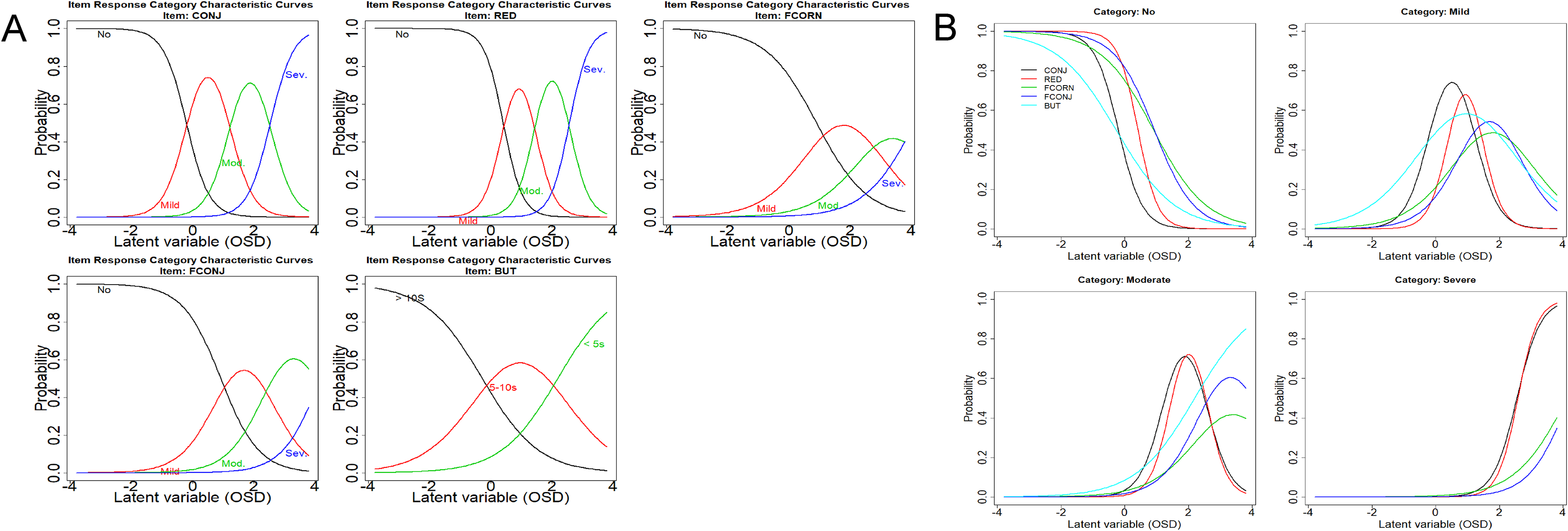
RASCH analysis: (A) Item response category curves of 5 ocular signs and symptoms of ocular surface disease (OSD), conjunctival hyperemia (CONJ), eyelid redness (RED), fluorescein staining of the cornea (FCORN) and fluorescein staining of the conjunctiva (FCONJ) and tear film break up time (BUT). OSD denotes ocular surface disease; black curves plot a response of no ocular signs/symptoms; red curves plot mild grade ocular signs/symptoms; green curves plot moderate (Mod) signs/symptoms; blue curves plot severe (Sev) signs/symptoms; s denotes seconds. (B) Item response category curves for grading of 5 ocular signs and symptoms of ocular surface disease (OSD), conjunctival hyperemia (CONJ), eyelid redness (RED), fluorescein staining of the cornea (FCORN) and fluorescein staining of the conjunctiva (FCONJ) and tear film break up time (BUT). Black curves plot a response of no ocular signs/symptoms; red curves plot mild grade ocular signs/symptoms; green curves plot moderate (Mod) signs/symptoms; blue curves plot severe (Sev) signs/symptoms; s denotes seconds.
LASSO method
The LASSO method allowed for binary responses and a penalization method that eliminated some items from the original questionnaire. The LASSOlite method without the inclusion of clinical evaluation then reduced the number of variables to 9 with an associated risk score for OSD. The 9-item version of the questionnaire was comprised of 5 items for a patient interview component and 4 items assessed by clinical evaluation (Figure 1B). The interview section was retained and consisted of questions to identify risk factors. The ocular signs were assessed for each eye by an ophthalmologist and documented as a yes/no response for conjunctival hyperemia, eyelid redness, positive fluorescein corneal staining, positive fluorescein conjunctival staining and break up time <5 s.
Whatever the model, the variable “dry eye” was strongly associated to OSD risk. The symptoms between instillation, itching/Irritation were not related to OSD in the initial questionnaire and thus deleted in the 9-item questionnaire.
With clinical exams of ocular signs (conjunctival hyperemia and eyelid redness), LASSO did not suppress any variables and simplified the process due to the dichotomization of variables.
In the model without clinical evaluation, the equation for generating a score from the 9 variables selected in the LASSO model is presented in the appendix.
Table 1 presents the coefficients and statistics of model accuracy and performance from the LASSO method without inclusion of the clinical evaluation. Tear film break up time (BUT) < 10 s was considered an appropriate ocular sign for this analysis. This model decreased the number of variables to 9 as predictors of OSD. For this model, the AUC was 0.786 and the sensitivity and specificity were 67.9% and 76.6%, respectively.
Nine-parameter questionnaire. Coefficients of two models of least absolute shrinkage and selection operator methods and statistics of model accuracy for detecting ocular surface disease in patients with glaucoma or ocular hypertension.
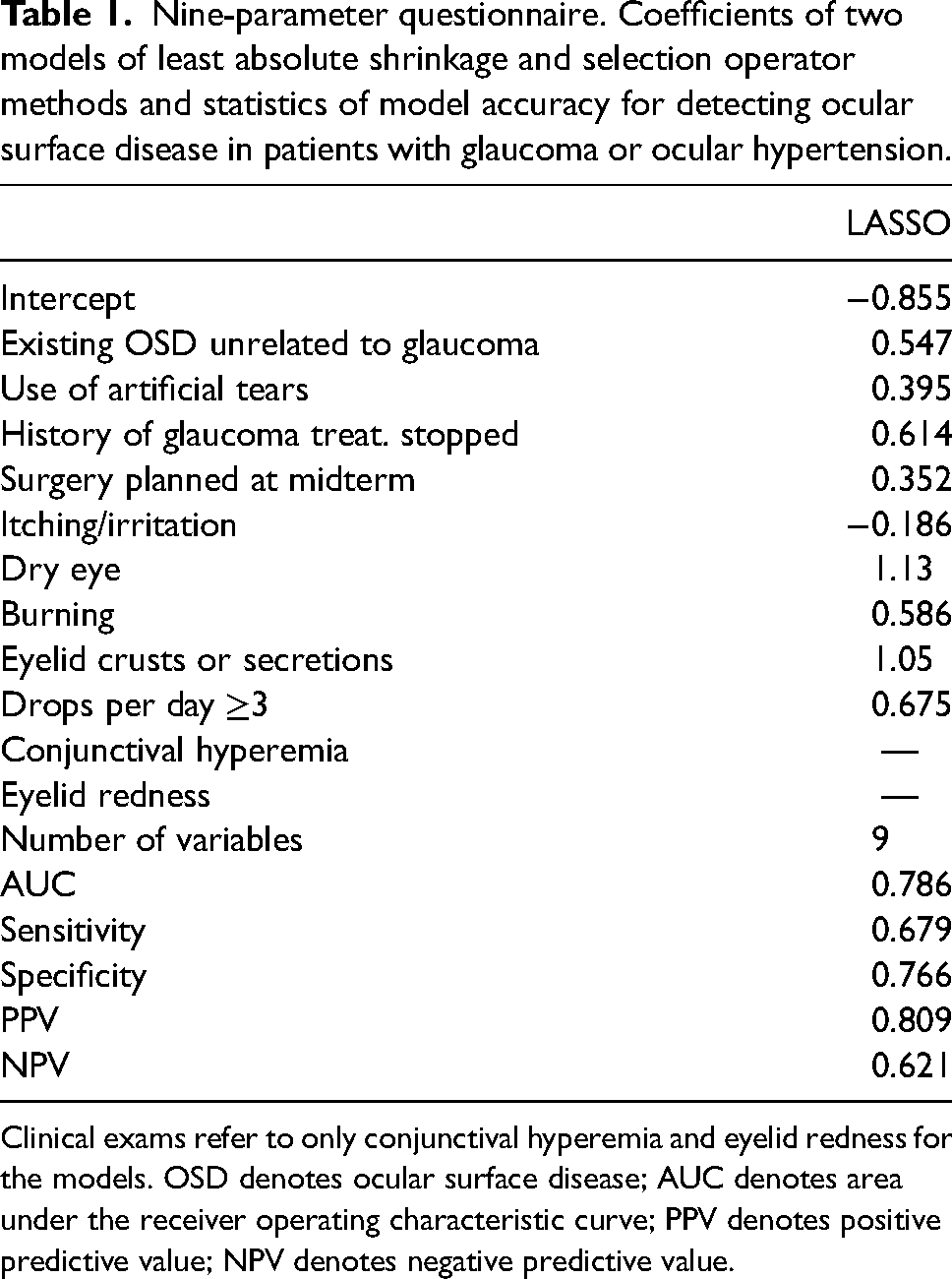
Clinical exams refer to only conjunctival hyperemia and eyelid redness for the models. OSD denotes ocular surface disease; AUC denotes area under the receiver operating characteristic curve; PPV denotes positive predictive value; NPV denotes negative predictive value.
6-Item FAST® questionnaire: the fastest identification of patients at risks of OSD
The LASSOlite method was then performed for eyes with a grade of moderate or severe in one of the following or a mild grade symptom in atleast 2 of the following symptoms: itching/irritation, dry eye, burning sensation on instillation of drops and eyelid crusts and secretion (Table 2). The LASSO method that included clinical exams, eliminated the surgery variable, and reduced the number of variables to 6 as predictors of OSD. With this model, the most important variable was the use of artificial tears followed by conjunctival hyperemia, eyelid redness, instillation of 3 or more drops a day, existing OSD and a history of halting glaucoma treatment. The AUC for this model was 0.815 and the sensitivity and specificity were 71.9% and 74.3%, respectively.
Six-parameter questionnaire. Coefficients for a model of least absolute shrinkage and selection operator method that included only conjunctival hyperemia and eyelid redness and statistics of model accuracy for detecting ocular surface disease in patients with glaucoma or ocular hypertension.
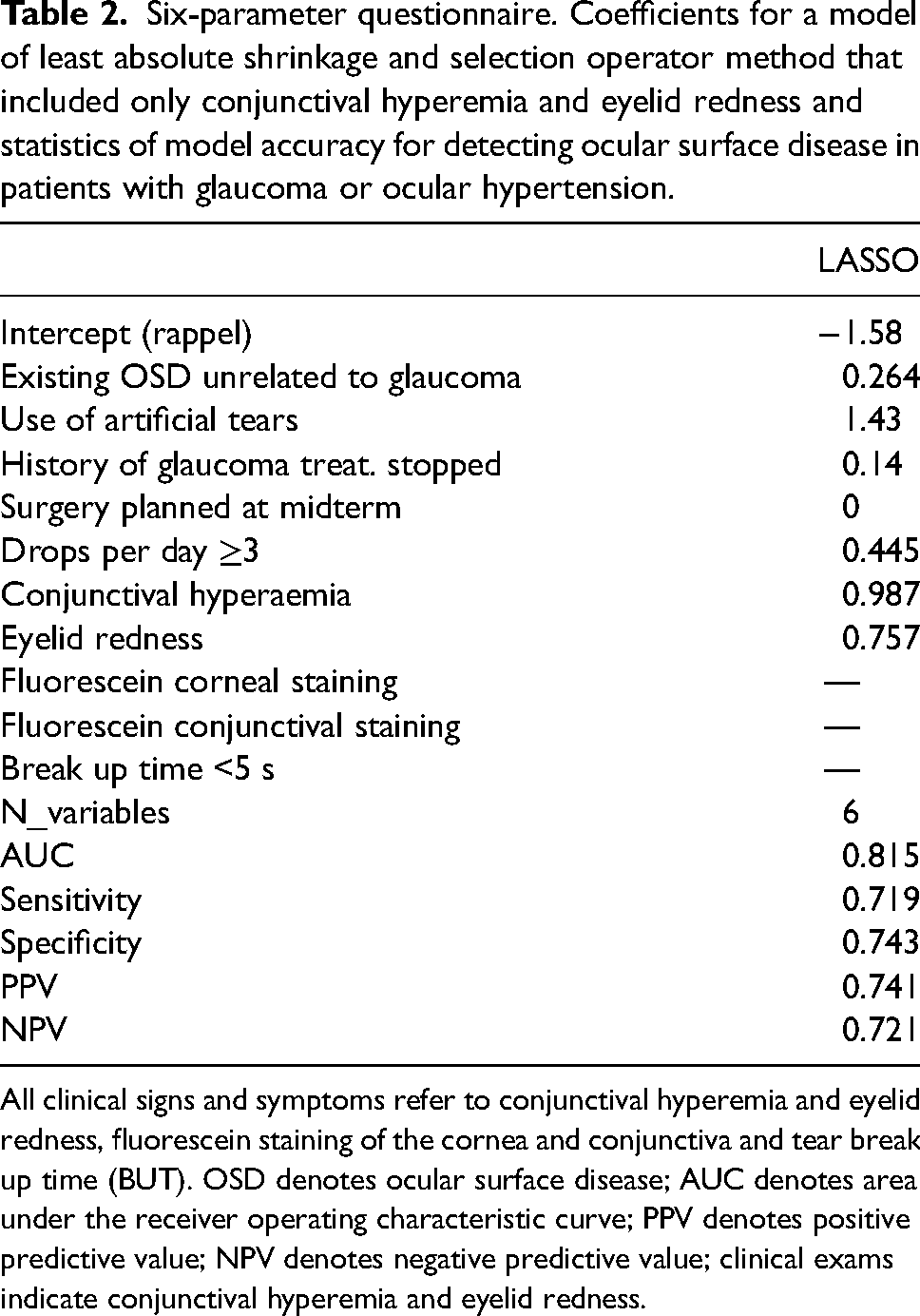
All clinical signs and symptoms refer to conjunctival hyperemia and eyelid redness, fluorescein staining of the cornea and conjunctiva and tear break up time (BUT). OSD denotes ocular surface disease; AUC denotes area under the receiver operating characteristic curve; PPV denotes positive predictive value; NPV denotes negative predictive value; clinical exams indicate conjunctival hyperemia and eyelid redness.
The 6-item version was comprised of 4 items for a patient interview component and 2 items that were assessed through clinical exam (Figure 1C). The patient interview section for identifying risk factors was retained. The ocular signs (clinical exam) were assessed for each eye by an ophthalmologist and documented as a binary yes/no response for only conjunctival hyperemia and eyelid redness.
Discussion
This study describes the development and validation of a new short version of a questionnaire called FAST® dedicated to glaucoma and OHT patients for detecting those at risk of OSD during routine visits. All versions of the questionnaire use patient interview and clinical assessment components for calculating a global OSD score (9-item version) or to indicate glaucoma patients at risk for OSD (6-item version). Initially, Rasch analysis was used to determine correlations and reduce variables that essentially gave the same information. Then, LASSO was used to maintain or increase specificity and sensitivity of the questionnaires to reduce the number of items first to 9 then to 6 questions. The 9-item and 6-item versions include the same risk factors, but the calculation of a global score with the 9-item questionnaire allows OSD assessment over time.
The original 14-item questionnaire generates accurate results for detecting OSD in European patients. For example, use of this FAST® questionnaire indicated a 60% prevalence of OSD in the study population. This is consistent with previous published prevalences of OSD in glaucoma patients ranging from 47.6% to 75%.1,4–6,13 Hence prevalence data from this study could be used for the overall European population but this version includes 5 clinical exams that would increase workup time in daily practice.
OSD in glaucoma includes factors such as advanced age, and preservative-containing medications. 14 Due to the longterm nature of glaucoma, patients may be using multiple topical medications daily for decades, exacerbating OSD. Instillation of preservative-containing glaucoma medications may lead to stinging, burning and hyperemia that can increase in severity with the duration of therapy. 2 A 2022 survey of ophthalmologists, reported that 75.6% of glaucoma patients had conjunctival hyperemia. 15 The high prevalence of some form of tear film disruption among glaucoma patients increases with the number of preserved anti-glaucoma medications used daily which increases the daily burden of preservative dosage. 8 The reduced adherence to medical therapy potentially leads to progressive visual field and vision loss. 4 Hence detection of at-risk patients can reduce morbidity and the prevalence of OSD. Clinical implementation of the 6-item questionnaire allows quick detection of at-risk patients and implementation of appropriate treatment for better adherence, potentially leading to better disease control.
The 6-item FAST® questionnaire is ideally suited to work within the constraints of limited patient workup time without affecting the workflow efficiency of the clinic. We used statistical methods and clinician input to determine the most appropriate predictors for OSD. The outcomes of the modeling studies indicated that a 6-item questionnaire with binary responses was ideal for detecting glaucoma patients at risk of OSD. The strength of our combined statistical approach (Rasch analysis and LASSO) is evident based on the statistics of accuracy (sensitivity/specificity/ AUC 71.9%/74.3%/0.815 respectively).
High sensitivity is preferable when the disease is serious and cannot be ignored. 16 To avoid unnecessary treatment, high specificity is preferable when the disease is incurable. 16 The score developed here could be considered an initial detection of OSD and then, the final diagnosis of OSD severity would be confirmed with clinical assessement (TBUT, fluorescein) to mitigate unnecessary treatment. Importantly, this score can identify patients at risk of developing OSD or those at risk of a progressive increase in severity. Hence, the ophthalmologist can select the optimal topical glaucoma regimen by mitigating the risk of OSD. Addressing OSD in glaucoma patients increases patient compliance and presumably, the efficacy of medical therapy.1–3 Notably, the European Society of Glaucoma (ESG) stated that preserved topical glaucoma formulations can cause or aggravate OSD and recommends preservative-free drops in at-risk patients. 17 The European Medicines Agency also suggests avoiding preservative-containing drops in patients on longterm treatment. 17
We found that 6 variables allow detection of 7 out of 10 glaucoma patients at risk of OSD. The six variables, ranked from highest to lowest importance are: artificial tears, conjunctival hyperemia, eyelid redness, daily instillation of 3 or more drops, existing OSD and history of halting glaucoma treatment.
AUC values of 0.5 indicate that the model is no better than chance at detecting the disease. However, our value for AUC (0.815) is well above chance, indicating excellent detection of OSD. The values for sensitivity, specificity and AUC reported in the current study are well within the range reported for commonly used OSD questionnaires for the general patient population. 18 For example, the 12-item Ocular Surface Disease Index (OSDI) has 60%, 83%, 0.83 sensitivity specificity and AUC respectively.12,18 The 19-item Dry Eye Screening for Dry Eye Epidemiology Projects, has a sensitivity and specificity of 0.6 and 0.94 respectively. 19 The 15-item Ocular Comfort Index, has a sensitivity and specificity of 56.7% and 55%, respectively. 20 Commonly used OSD questionnaires routinely contain over 10 items and were originally developed for epidemiologic research that is not suited for routine clinical use. Direct comparison of the shorter versions of the FAST® questionnaire to other questionnaires is tenuous at best as none of the other surveys were specifically designed for detecting OSD in glaucoma/OHT patients. The 9-item and 6-item versions can be used in routine practice or for research studies for identifying patients at-risk patients and to follow the change in score over time or after switching treatment.
The binary responses incorporated into FAST® saves time in identifying at-risk patients in routine daily practice. A yes/no answer allows the patient and ophthalmologist to save time because it reduces the task of grading a sign or symptom and/or determining the severity of each item. In fact, one positive response in this questionnaire indicates that the patient warrants further investigation for OSD with the appropriate clinical tests. The methodology used here was extremely beneficial for the objective of reducing the items on the questionnaire yet maintaining reasonable accuracy for routine clinical use. Additionally TBUT less than 5 s is a more appropriate parameter as 10 s is not precise enough to determine OSD given the greater variability in tear film with age. 21 TBUT shorter than 5 s is a definitive marker of dry eye. 22
Some limitations to this study include the enrolment of a European population and further testing may be warranted to ensure validity in other populations. Administering FAST® will add time to the clinical workup however, we have formulated a 6-item version for quick implementation in daily practice. A technician or nurse may administer this questionnaire during pre-screening to alert the ophthalmologist if further testing is warranted. Although the attendant drawbacks of verbal questionnaires may exist when administering FAST®, the 6-item version consists of questions that are routinely asked during clinical assessment. Hence we believe this risk is minimal at best.
To our knowledge, this is the first publication of the new FAST® questionnaire that enrolled the largest study sample of currently available OSD questionnaires. This is the first questionnaire specifically developed for detecting patients at risk of OSD in the glaucoma subpopulation. The 9-item and 6-item versions are useful for identifying patients at risk of OSD. The short questionnaire is a simple and quick tool for incorporation into the routine clinical workup of glaucoma patients for early evaluation of OSD risk. Both versions of the questionnaire provide robust estimations of patients at risk. Avoiding OSD or mitigating the risk of OSD via the use of preservative-free topical glaucoma formulations is an important consideration given the enhanced risk of dry eye and ocular toxicity with longterm use of preservative-containing topical formulations that are common for treating glaucoma. 8
In summary, the adoption of the short versions of the FAST® questionnaire in routine clinical practice will allow the detection of the majority of glaucoma patients at risk of OSD without appreciably generating false negatives. This questionnaire will help ophthalmologists diagnose OSD which may improve adherence to the topical regimen in patients with glaucoma or OHT.
Footnotes
Declaration of conflicting interests
Christophe Baudouin is a consultant for Alcon, Horus Pharma, Oculis, Santen and Thea. Ingeborg Stalmans reported the following commercial relations: Grant/research support: Théa and Santen; Clinical trial participation: Aerie, Bausch&Lomb, Omikron, Théa, Santen; Consultant for: Alcon, Allergan/AbbVie, Bausch&Lomb, Elios Vision, EyeD, Horus, Mona, Omikron, Santen, Théa; and Investments: Mona. John Thygesen is a consultant for Santen and Théa and have given lectures for both companies for which he has received an honorarium. Joanna Wierzbowska and Marta Misiuk Hojło have given lectures for Thea. Jose M. Benitez-del-Castillo is a consultant for Thea, Santen, Brill, and Horus. Alfonso Anton is a consultant for Horus Pharma and Thea. Grant/research support: BrudiLab and Thea Clinical trial participation: Aerie, Omikron, Théa, Santen; Honoraria/Consulting fees: Alcon, Horus, Omikron, Santen, Théa. Jonathan Clarke has consulted for Thea, Glaukos and Santen.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We thank Laboratoires Thea (France) for funding the editing of this manuscript.
Appendix
Equation for generating a score from the 9 variables using the LASSO model.
Ln denotes logarithm, P denotes probability.
A score ≥0.60 indicates that the patient has OSD.