
Abstract
Purpose
To describe a rare case of vision loss due to bilateral edema of the optic nerve in a patient with Hereditary Angioedema, treated with prophylactic C1-esterase inhibitor.
Methods
A 60-year-old Caucasian male affected by Hereditary Angioedema with unknown genetic defect (HAE- UNK) was admitted to our hospital presenting bilateral vision loss (best corrected visual acuity of 20/32 in the right eye and hand motion in the left eye) during an HAE attack. Intravenous administration of C1- esterase inhibitor (C1-INH, 1500 IU, Berinert, CSL Behring) determined the resolution of facial and periorbital swelling, however visual impairment persisted, in contrast with previous attacks experienced by the patient. Fundus examination revealed a vital optic disc without papilledema in both eyes. Magnetic resonance imaging (MRI) of the head and orbits showed bilateral edema of the optic nerve sheath. Treatment with intravenous and oral steroids was ineffective. Subsequently, a prophylactic treatment strategy with subcutaneous C1-esterase inhibitor was started (7000 IU every four days).
Results
Complete regression of edema of the optic nerves was observed by imaging at two months of follow-up after chronic treatment with C1-esterase inhibitor (7000 IU every four days). Complete restoration of visual acuity was achieved (BCVA 20/20 in both eyes) and multimodal imaging of the optic nerves demonstrated the absence of anatomical and functional damage.
Conclusion
Patients affected by HAE may show atypical presentation with edema of the optic nerves without involvement of the optic nerve head. They may significantly benefit from prophylactic and chronic treatment with C1-esterase inhibitor.
Introduction
Hereditary angioedema (HAE) is a rare hereditary condition, transmitted as an autosomal dominant trait, caused by deficiency/defect of C1 inhibitor (C1-INH) or other mechanisms. Different forms of HAE are currently identifiable: HAE due to C1-INH deficiency (Type 1 HAE); HAE due to C1-INH dysfunction (Type 2 HAE) and other forms of HAE with mutations in different genes (factor XII, angiopoietin-1, plasminogen, kininogen-1, myoferlin, heparan sulfate 3-O-sulfotransferase 6). In addition, some patients have HAE due to unknown mutations (HAE-UNK). 1 This disease is characterized by episodic bouts of swelling of subcutaneous and submucosal tissues affecting mainly skin, bowel and genitalia. Edema can be life-threatening if it causes swelling of the larynx with obstruction of the airways. Patients with HAE commonly report headaches, visual impairment, periorbital pain and swelling during flare-ups of the disease, usually resolving within minutes or hours with the administration of C1-INH. Central nervous system may be involved in limited number of cases. Few case reports reported recurrent headaches, cerebral infarcts or transient ischemic attacks, status epilepticus, prolonged migraine and rare cases of cerebral edema.2–4 However, no reports are available about optic nerve involvement. We discuss a rare case of bilateral edema of the optic nerve without papilledema in a patient affected by HAE.
Case Report
We report the case of a 60-year-old Caucasian male affected by HAE, since the age of 33 years. Two members of his family were also affected. HAE-UNK with normal C1-INH was diagnosed through blood tests and genetic test for known pathogenic mutations was negative. His general medical history also included pituitary microadenoma previously treated with bromocriptine and type II diabetes mellitus, diagnosed around 5 years ago and treated with metformin and dulaglutide. He has suffered from several (around 10 per year) bouts of angioedema characterized by swelling of the face, eyelids and neck, periorbital pain and unilateral or bilateral visual impairment. Each episode usually lasted a few hours with complete resolution after intravenous administration of C1-INH (Berinert CSL Behring, 1500 IU). Almost twenty years ago, he had been admitted to the Emergency Department of “Cannizzaro Hospital” of Catania for coma due to cerebral edema, which promptly regressed after the intravenous administration of C1-INH. Ten months ago, he presented to the Emergency Department of our Hospital “Policlinico Gaspare Rodolico” of Catania for sudden acute angioedema presenting swelling of the upper airways, face and periorbital region associated with vision loss in both eyes (more severe in the left eye). Intravenous administration of C1-INH (1500 IU) caused the resolution of edema, but visual impairment persisted, contrary to previous attacks. At presentation ocular examination revealed normal ocular motility without diplopia, best-corrected visual acuity (BCVA) was 20/32 in the right eye and hand motion in the left eye. Anterior segment biomicroscopy showed no signs of inflammation. Intraocular pressure was within normal limits in both eyes. Fundus examination of both eyes revealed a vital optic disc with physiological excavation and without papilledema, a healthy macula, absence of diabetic retinopathy signs (Figure 1). Fluorescein angiography confirmed the absence of papilledema or any alteration of the optic nerve head in both eyes (Figure 1). Magnetic resonance imaging of the head and orbits showed the enlargement of the optic nerve sheaths of both eyes, without any sign of intracranial hypertension. Morphology, intensity of signal and course of the optic nerves were normal. (Figure 1). Visual field test showed bilateral large scotoma (Figure 1).
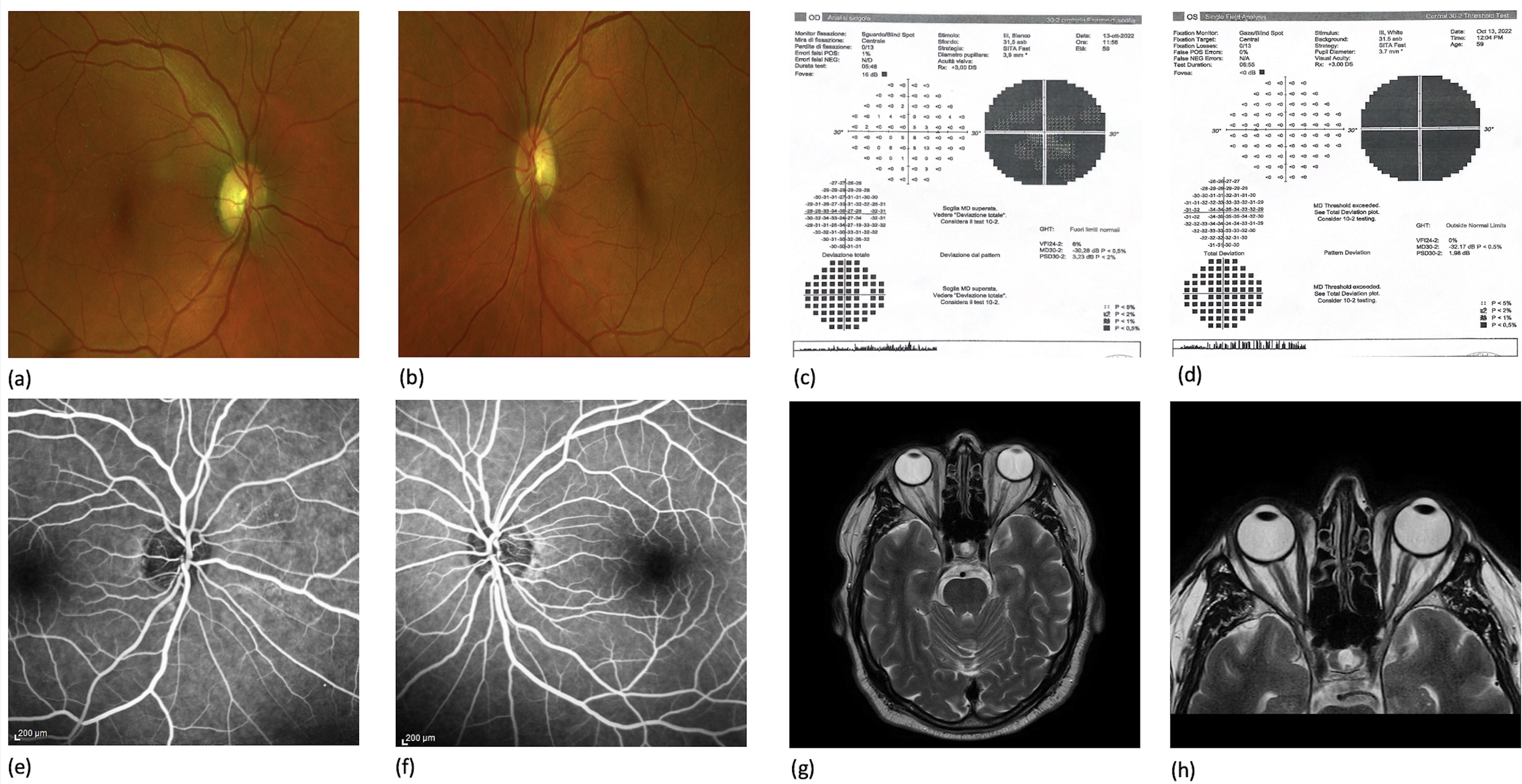
Fundus examination showed a vital optic disc without papilledema in both eyes (a and b). Visual field test demonstrated bilateral large scotoma (c and d). Fluorescein angiography confirmed the absence of papilledema in both eyes (e and f). MRI showed bilateral enlargement or optic nerve sheaths, without any sign of intracranial hypertension (g and h).
He was then admitted to the Neurology Unit of “Gaspare Rodolico” Hospital. During hospitalization, he suffered a progressive visual acuity worsening in both eyes (20/100 in the right eye and hand motion in the left eye). Angioedema attacks were treated with on-demand intravenous C1-INH (Berinert, CSL Behring, 1500 IU) during the hospital stay. Empirical therapy with intravenous methylprednisolone (500 mg/day for three days) followed by oral prednisone (50 mg/day) was administered, without any improvement of the visual acuity. Accordingly with the specialists of the Regional Referral Center for Angioedema and Rare Diseases of “Policlinico Gaspare Rodolico”, the patient was discharged with a treatment regimen based on subcutaneous prophylactic-chronic C1-INH (Berinert, CSL Behring, 7000 IU every four days). Since then, a significant improvement in BCVA and a reduction in the number and severity of angioedema attacks have been documented. Surprisingly, after two months of prophylactic treatment with C1-INH, BCVA reached 20/20 in both eyes, visual field test showed substantial bilateral improvement and MRI of the head and orbits demonstrated complete resolution of the optic nerve edema in both eyes (Figure 2).
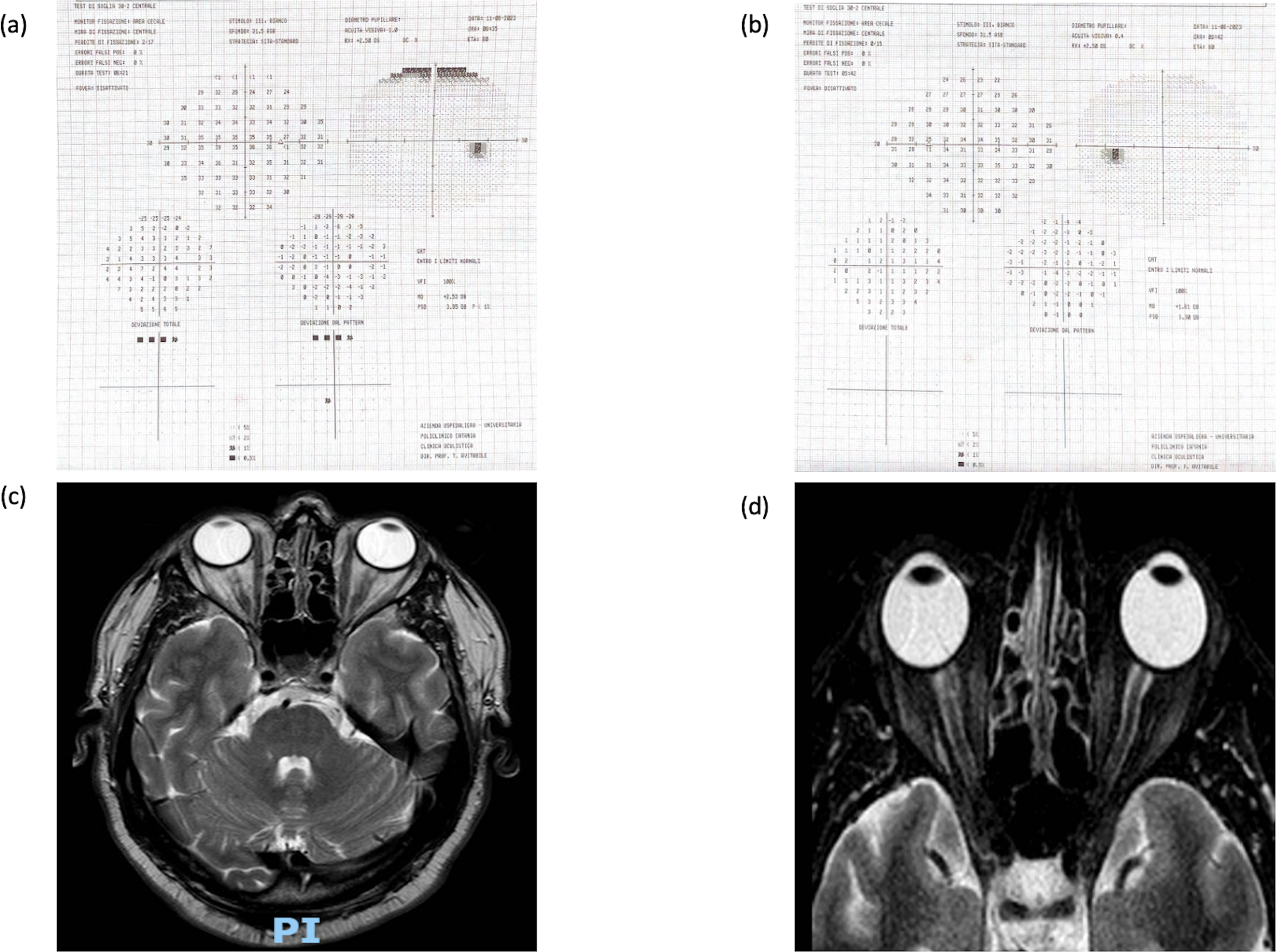
After two months of prophylactic treatment with C1-esterase inhibitor (7000 IU every four days), visual field test demonstrated a significant improvement in both eyes (a and b). MRI of the head and orbits showed resolution of the optic nerve edema in both eyes (c and d).
Fundus examination was unchanged, showing a vital optic disc without papilledema in both eyes (Figure 3). Radial peripapillary capillary plexus on optical coherence tomography angiography (OCT-A) and retinal nerve fiber layer (RNFL) thickness on optical coherence tomography (OCT) were within normal limits in both eyes, demonstrating the absence of anatomical damage to nerve fibers and vascularization of the optic nerve head (Figure 3). The patient is still on prophylactic treatment with C1-INH and at 1-month follow-up visit, visual acuity is stable.
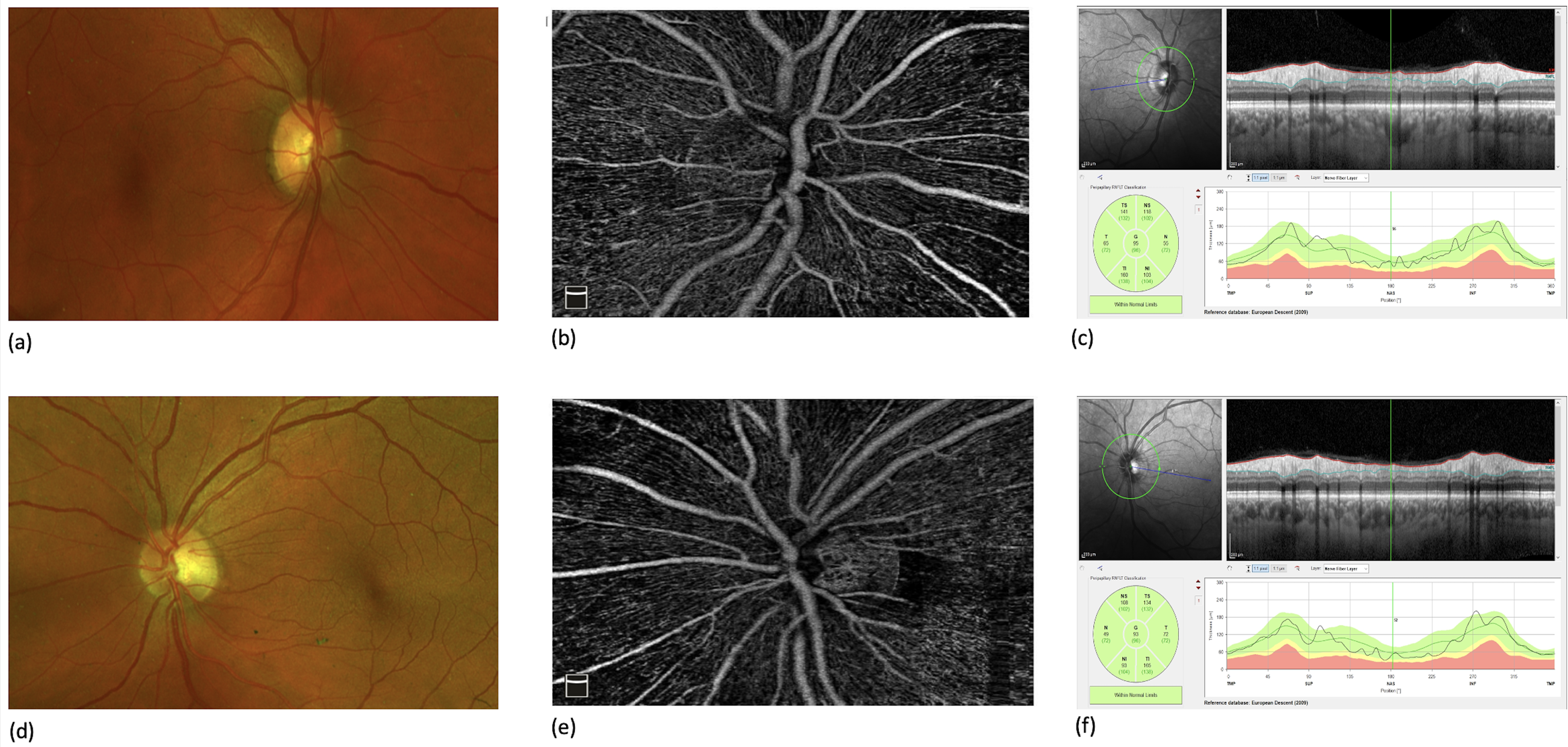
After two months of prophylactic treatment with C1- esterase inhibitor (7000 IU every four days), multimodal imaging of the optic nerve demonstrated the absence of anatomical damage to nerve fiber layer and vascular network in both eyes. A vital optic disc without papilledema was evident on clinical examination, in both eves (a and d). Radial peripapillary capillary plexus on oct angiography (b and e) and RNFL thickness (c and f) were within normal limits in both eyes.
Discussion
Central nervous system involvement was exceptionally described in HAE patients: few case reports described recurrent headaches, transient ischemic attacks, migraine, epilepsy and rare cases of cerebral edema.2–4 However, no reports are available about optic nerve involvement. To the best of our knowledge, this is the only reported case of bilateral edema of the optic nerve in a patient with HAE. A link between hereditary angioedema (HAE) and retinopathy has also been studied. OCT-A documented a reduced vessel density in both superficial and deep capillary plexus and a higher retinal thickness in HAE patients compared to healthy controls. 5 Another study from the same group demonstrated that RNFL thickness (in the nasal superior and temporal quadrants) and the ONH thickness in HAE patients were greater than in controls. 6 Therefore, these studies documented subclinical damage in the retinal microvascular network in type I HAE patients that could be associated with initial mild functional changes. The authors of the last-mentioned studies proposed a physiopathological hypothesis for their findings: C1-INH normally blocks the classic component pathway, the activation of coagulation factor XI and XIIa, kininogen, plasmin and TPA activation. In HAE, its deficiency leads to an increase of kallikrein, which causes liberation of bradykinin, increasing vascular permeability and producing massive local uncontrolled edema. Vasodilatation induced by C1- inhibitor insufficiency and accumulation of bradykinin can hypothetically produce edema in any perivascular tissue. Therefore, it could be hypothesized that recurrent failure of the blood-endothelial barrier of the retina in HAE patients potentially results in chronic damage. 5 The same physiopathological mechanism could have been the underlying cause of optic nerve edema in our clinical scenario, but with a substantial difference in the molecular pathway because C1-INH concentration was normal in our patient (HAE-UNK with normal C1- inhibitor). Mutation of a still-unknown pathogenic gene could have determined the accumulation of vasoactive peptides that caused perivascular edema arising from the vessels of the optic nerve sheath, which is formed by meningeal membranes. As a matter of fact, edema arose around the optic nerves, which are the only cranial nerves covered by pia mater, arachnoid and dura mater while the other cranial nerves were spared. We suppose that perivascular leakage of the optic nerve sheath vessels, determined by HAE, could have produced mild and chronic edema of the optic nerve sheaths which caused damage to the optic nerve, possibly by compression of the optic nerve fibers causing interruption of neuronal signal transmission. This mild edema of the optic nerve sheaths was enough to create a disruption of nerve impulses and severe visual loss, but not sufficient to cause ischemic irreversible compression of the feeder vessels of the optic nerve or papilledema. In our case, edema was confined to the intra-orbital part of the optic nerves, without cerebral edema, enlargement of cerebral ventricles or any classical neuroradiological sign of intracranial hypertension (empty sella, tortuosity of the optic nerves, flattening of posterior sclera, intraocular protrusion of the optic nerve head), as confirmed by neuroimaging. It should be pointed out that visual impairment during flare-ups was not transient and no improvement after facial swelling resolution was detected, in contrast with previous attacks experienced by the patient. Indeed, visual acuity in both eyes constantly declined during and between exacerbations of the disease, despite the on-demand treatment. We suppose that the on-demand administration of C1-INH could have caused slow and partial reabsorption of the optic nerve edema but residual fluid represented the trigger for further attacks and continuous vascular leakage. OCTA showed a pivotal clinical role in detecting vascular alteration in patients affected by systemic disorders.7–9 In this case, no morphological alteration of the radial peripapillary vascular network was detected suggesting that the ischemic damage (caused by compression of the feeder vessels) is a less plausible theory. Accordingly, the reversibility of the visual acuity decline in this case, without neuronal cell death, supports a chronic fluid accumulation in the optic nerve without an acute ischemic event. Visual impairment was totally recovered reaching a BCVA of 20/20 in both eyes, with a vital optic disc on clinical examination. The inefficacy of steroidal treatment excludes inflammatory etiologies such as optic neuritis and further confirms our theory of a non-inflammatory edema of the optic nerves, caused by HAE. Further genetic tests may identify the pathogenic mutation in our patient and, as a consequence, a new genotype-phenotype correlation could be established (a new gene mutation responsible for HAE associated with central nervous system involvement in the form of cerebral edema and optic nerve edema). C1-esterase inhibitor is a life-saving drug for these patients during angioedema attacks affecting the upper airways. Based on the clinical scenario we have discussed, C1-esterase inhibitor can also be considered a sight-saving drug, able to restore visual function in patients affected by edema of the optic nerves, a rare complication of HAE.
Conclusion
The present case describes a rare new complication in patients affected by HAE. Persistent vision loss during and between angioedema attacks should be considered a warning sign of edema of the optic nerve. Prompt ophthalmological assessment is needed and it should be kept in mind that a clinically normal optic disc on fundus examination does not rule out the presence of edema of the optic nerves and functional impairment of the visual pathway. In this clinical scenario, MRI and visual field tests are mandatory to detect morpho-functional alteration of the intra-orbital or intra-cranial component of the optic nerve. Prophylactic chronic treatment with C1-INH may be considered a sight-saving drug in these patients.
Footnotes
Authors’ contributions
NC drafted the manuscript. ED, FL, SN, FG collected patient information. TA, PC, SN, AR, DS and FG reviewed the manuscript. All the authors read and approved the final manuscript.
Consent for publication
Written informed consent was obtained from the patient.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.