
Abstract
Purpose
To report a challenging Descemet Membrane Endothelial Keratoplasty (DMEK) case, complicated by intraoperative aqueous misdirection and spontaneous anterior chamber fibrin reaction.
Methods
A 70-year-old female affected by corneal edema due to Fuchs endothelial dystrophy underwent a triple procedure (cataract extraction - IOL implantation - DMEK surgery) in her left eye. This report illustrates the management of the intraoperative complications of aqueous misdirection syndrome and anterior chamber fibrin reaction.
Results
Despite the optimal management of the posterior pressure and the thorough removal of the fibrinous reaction during the case, the DMEK graft was not completely unfolded and centred at the end of the surgical procedure. Nonetheless, the patient showed good long-term anatomical and functional recovery: at the last follow-up (2 years after surgery), central corneal thickness was 526 µm with a best corrected visual acuity of 20/25 and an endothelial cell density of 1112 cell/mm2.
Conclusion
Early recognition and prompt management of intraoperative aqueous misdirection syndrome and anterior chamber fibrin reaction during DMEK surgery is essential to ensure good functional and anatomical outcomes.
Introduction
Descemet Membrane Endothelial Keratoplasty (DMEK) is still a challenging procedure that can frequently incur in intraoperative complications, such as difficulty in graft unfolding or positioning, anterior chamber haemorrhage, increased intraocular pressure and upside-down graft placement. 1 The DMEK learning curve appears longer compared to Descemet Stripping Automated Endothelial Keratoplasty (DSAEK),2–4 and some surgeons still avoid performing DMEK due to its technical difficulty, lack of experience and risk of complications.5–8 Herein, we report a particularly challenging case involving complicated DMEK management, requiring a great deal of effort but providing a notable learning experience.
Case report
A 70-year-old female presented to the clinic complaining of blurred vision, glare, and halos in her left eye, particularly in the morning. She had previously been diagnosed with Fuchs endothelial corneal dystrophy (FECD) and had undergone a combined surgical procedure (Phaco-DMEK) in her right eye. Best corrected visual acuity (BVCA) in her left eye was 20/40. Slit lamp examination revealed mild stromal oedema, guttae, and nucleo-cortical cataract (N2C2) in her left eye. A combined DMEK and cataract removal with intraocular lens (IOL) implant procedure was planned.
Surgery was performed under local anaesthesia. After successful phacoemulsification with IOL implantation in the capsular bag, an 8-mm descemetorhexis was performed with a reverse Sinskey hook. Acetylcholine (Miochol, Laboratoire Chauvin, Montpellier, France), was injected into the anterior chamber to induce miosis. Despite this, the pupil remained dilated. An 8-mm preloaded endo-out F-marked DMEK graft with an endothelial cell density (ECD) of 2400 cell/mm2 was inserted through the 3.2-mm corneal incision at the temporal limbus (DMEK rapid device).9,10 Initially, we unsuccessfully tried to unfold the graft by tapping on the corneal surface with a cannula (Figure 1A). Then, after trying to unfold the DMEK graft with short bursts of BSS, we observed a shallowing of the anterior chamber (AC), seemingly without underlying triggers. Despite trying to inject balanced salt solution (BSS) (Figure 1B), we were unable to re-establish the AC volume or to unfold the graft and decided to remove it from the AC. We found a considerable flattening of the AC with anterior iris displacement and increased posterior pressure. There was no evidence of a suprachoroidal haemorrhage. However, as a result of the manipulations performed attempting to deepen the anterior chamber, we observed a significant AC fibrin reaction. Next, we tried to remove the fibrin clot with the I/A probe, which proved unsuccessful. We subsequently cut the fibrin adhesions using vitro-retinal scissors (Figure 1C) and then the clot was further cut down and aspirated with the anterior vitrector (Figure 1D). Despite the AC flattening and fibrinous reaction, we attempted to inject the DMEK graft again. After numerous attempts, we managed to insert the graft while deepening the AC by injecting BSS. The graft unfolding proved to be exceptionally challenging in this case. We tried several approaches, such as tapping on the corneal surface, injecting short bursts of BSS, inserting an air bubble between the graft and the cornea (Figure 1E), and pulling the graft using vitreoretinal forceps (Figure 1F). After achieving a partial unfolding, with the DMEK graft unfolded in the pupillary area but not completely in the periphery, we filled the AC with an air bubble. We sutured and concluded the procedure (see also Supplementary Video). Post-operative therapy included chloramphenicol four times per day and prednisolone acetate 1% every 2 h. On the following day, slit lamp examination revealed that the bandage contact lens was in place, and that the DMEK graft was attached centrally but detached inferiorly and temporally, with 20% air in the AC and the pupil moderately dilated. The patient was rebubbled up to an 80% air fill after aqueous release and dilated with tropicamide and phenylephrine.
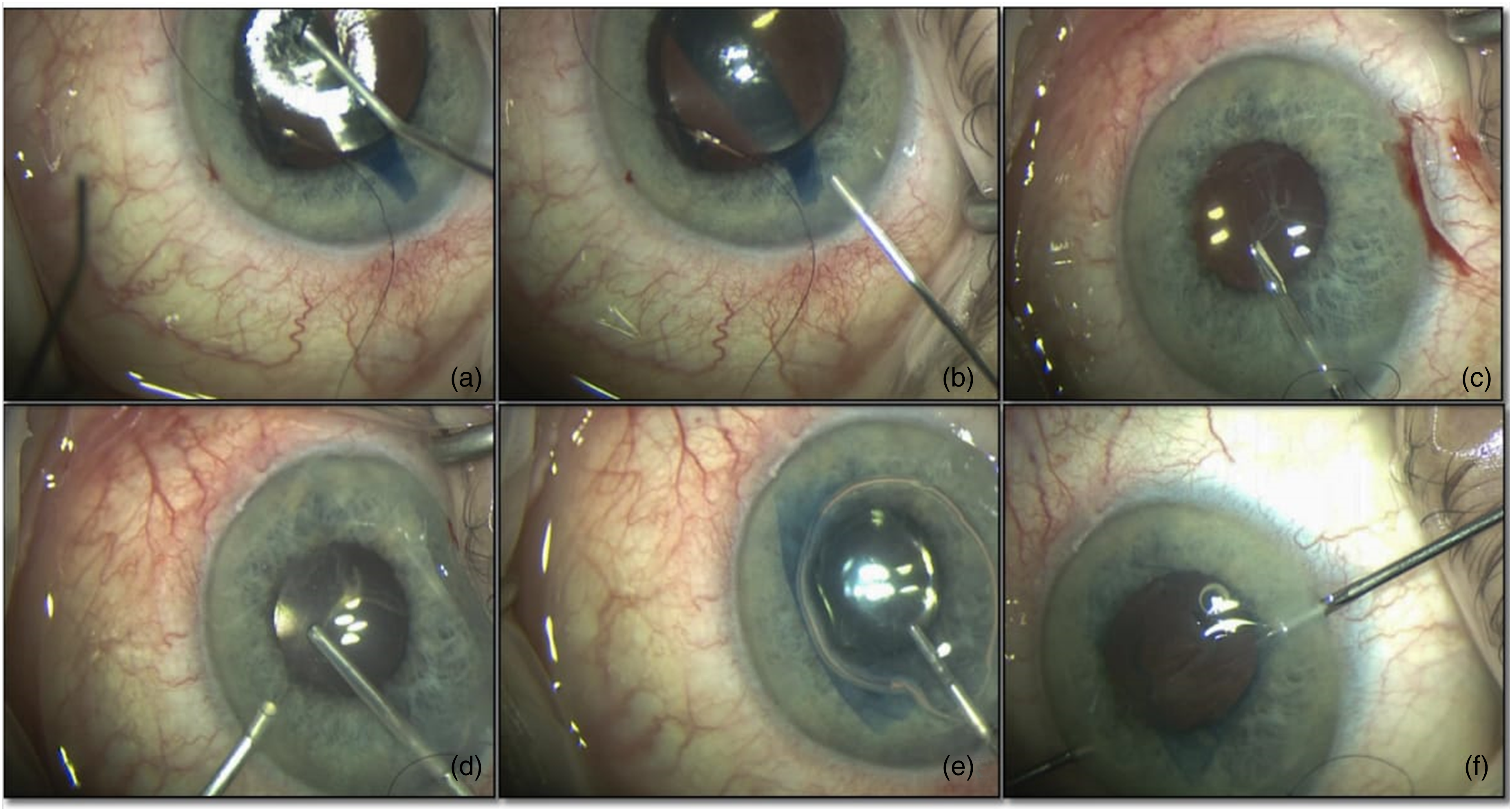
a-b) unsuccessful DMEK unrolling in an eye with very shallow anterior chamber. Multiple attempts have been made to unroll the graft and to deepen the AC by injecting BSS. c-d) After taking out the DMEK graft, fibrin was removed with vitro-retinal scissors and the anterior vitrector. e-f) Successful yet partial unroll of DMEK graft with the help of an air bubble first and then with vitreoretinal forceps and spatula.
At six weeks of follow-up, the DMEK graft was attached, and the cornea was clear, with no corneal oedema (Figure 2). Central corneal thickness in the left eye was 526 µm (RE 525 µm), the anterior chamber was deep and quiet, and the IOL was well placed in the capsular bag. BVCA was 20/40.
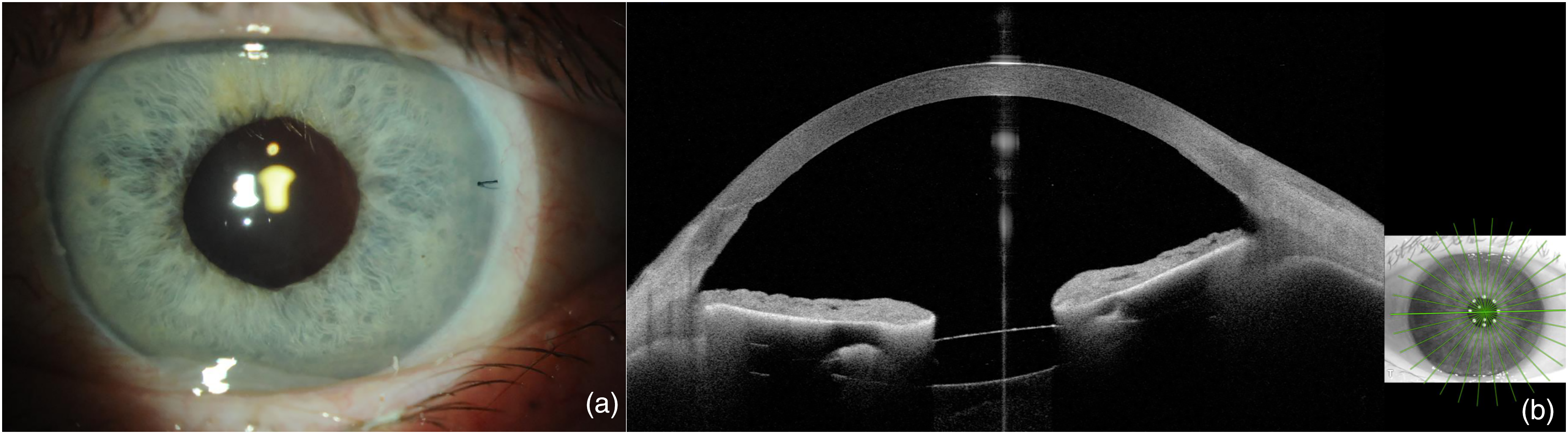
a) Slit-lamp colour photography showing clear cornea; b) OCT-SA image showing graft adhesion.
The BCVA trend at follow-up is shown in the graph in Figure 3.
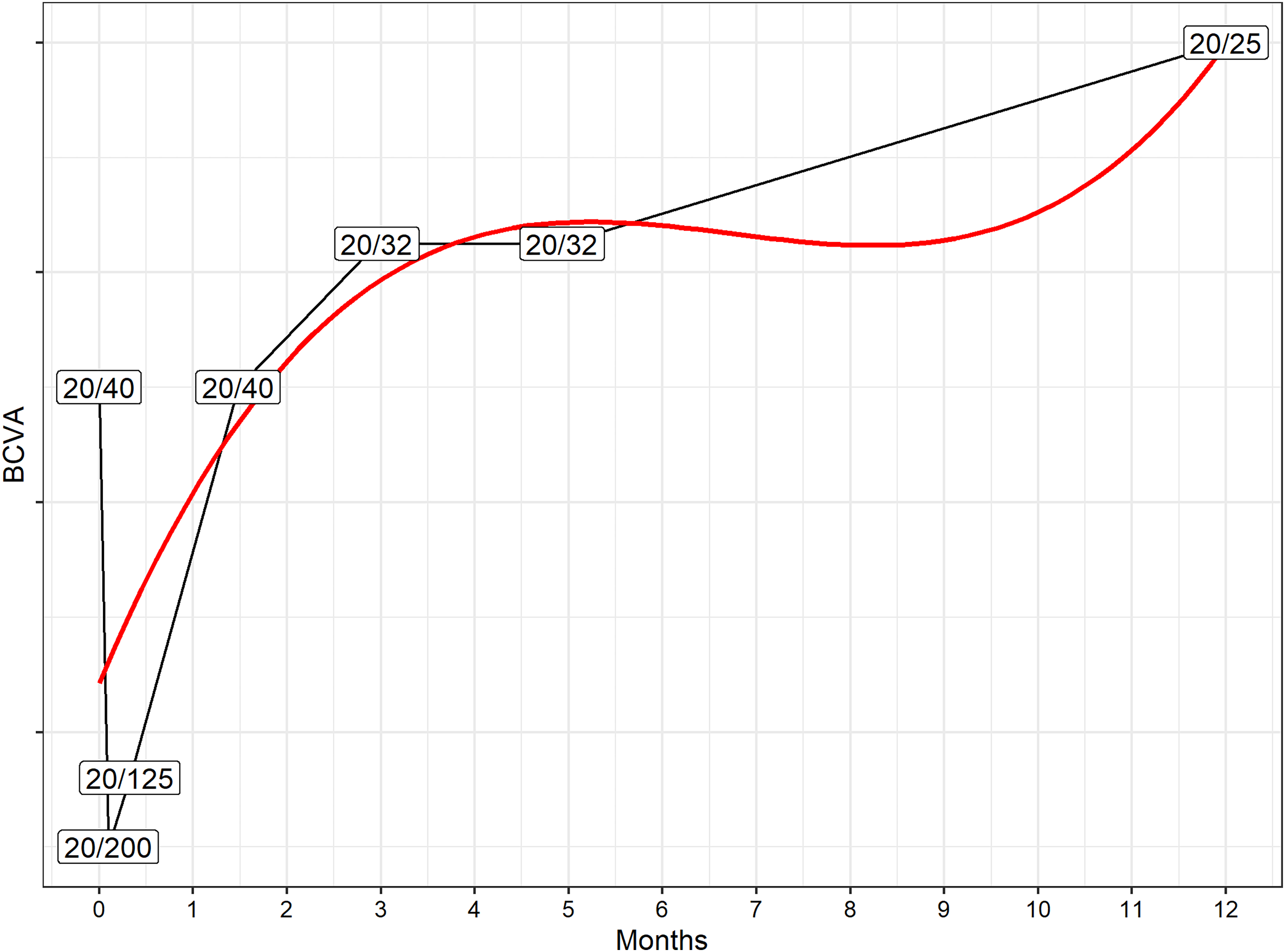
BCVA trend over 1 year of follow-up. The solid red line describes a 3rd degree polynomial relationship between time after surgery and BCVA. The visual acuity recovery rate was somewhat slower in this case compared to what usually reported for DMEK surgery, 2 which we hypothesize might be related to endothelial cell trauma due to the long, difficult unfolding and subsequent need for rebubbling.
At the 1-year follow-up, BVCA was 20/25, central corneal thickness at thinnest point was 497 µm, and ECD was 1112 cell/mm2. Corneal topography (Oculus, Germany) showed no signs of edema or subclinical edema (Figure 4). 11
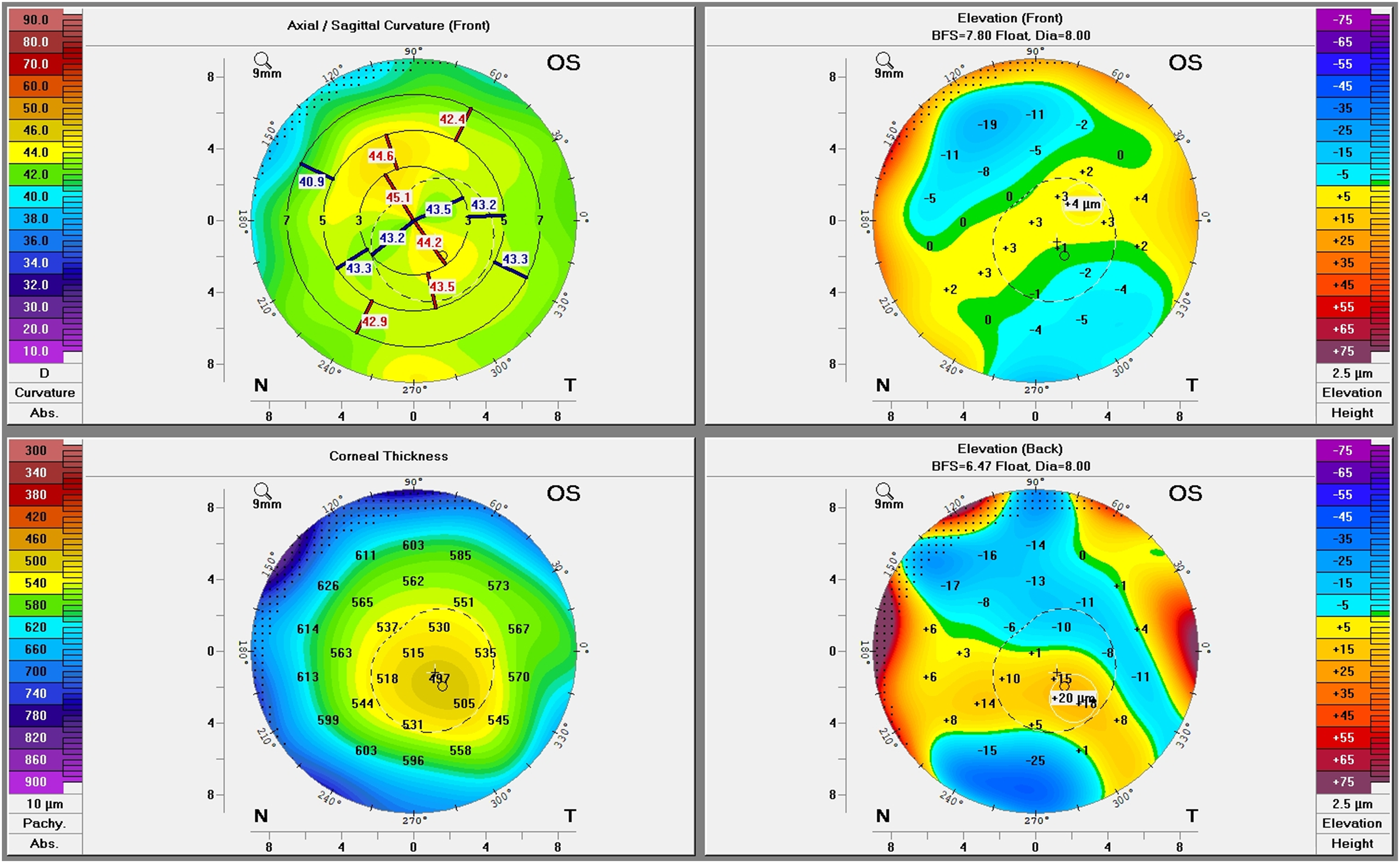
Corneal topography showing no signs of overt or subclinical oedema.
Discussion
Intraoperative aqueous misdirection syndrome (IAMS) is a challenging surgical complication characterized by intraoperative anterior segment volume loss due to misdirection of infusion fluid into the posterior segment.12,13 It presents as central and peripheral shallowing of the anterior chamber with anterior displacement of the iris-lens diaphragm, in absence of suprachoroidal effusion or major pathologies affecting the iris–lens complex.13,14 The main known risk factors for IAMS are small hyperopic eyes with shallow AC and a short axial length, and lax zonular fibres.14,15Additionally, there are other suggested potential risk factors, such as a history of IAMS in the fellow eye, nanophthalmos, plateau iris syndrome, larger natural lenses, and elevated intraocular pressure before surgery. 16
The exact comprehension of the pathophysiology behind IAMS remains elusive. Initially, one hypothesis proposed that penetration into the AC, particularly under elevated IOP, causes swift decompression of the AC, resulting in the displacement of the ciliary body and lens. 17 Another hypothesis suggests that the vitreous might play a bigger role in the development of IAMS. This theory gained support from early treatment endeavours aimed at deepening the AC by extracting the lens, which were effective only in cases where vitreous loss was present. 16
Shaffer and Hoskins proposed that physical misdirection of anteriorly rotated ciliary processes shunts the produced aqueous into the vitreous rather than the posterior chamber. 18 Ultrasound biomicroscopy (UBM) studies confirmed the alteration in the position of the ciliary bodies during a misdirection syndrome attack, as well as their correct repositioning after resolution. 19 Additionally, during the attack, the formation of aqueous pockets in the vitreous was confirmed. 16 Critically, the absence of evidence for a one-way valve allowing aqueous entry into the vitreous and preventing its exit prompted reconsideration of these theories, leading to the exploration of alternative hypotheses.
The prevailing etiological hypothesis proposes choroidal expansion as the primary mechanism pushing the vitreous forward. 20 Factors like intraoperative inflammation or hypotony are suggested as potential triggers, causing breakdown of the blood-choroid barrier and protein exudation, expanding the extravascular choroid, and increasing posterior vitreous pressure. 21 Support for this theory includes findings of choroidal effusions in acute angle-closure glaucoma and narrow angles. 22 Studies further revealed thicker choroids in angle-closure patients compared to healthy control and open-angle glaucoma patients, indicating susceptibility to choroidal expansion. 23 This hypothesis potentially explains the observed prevalence of uveal edema in misdirection syndrome cases. 24
Although IAMS has been described as a complication mainly related to trabeculectomy and cataract surgery, 16 several cases associated with endothelial keratoplasty (EK) have been reported.15,25,26 In EK procedures, IAMS most frequently occurs during irrigation with BSS while maintaining the AC during DSAEK graft insertion or unfolding the graft during DMEK. 15
Currently, the best intraoperative management approach for IAMS is still subject to debate. Before proceeding with the surgery, suprachoroidal haemorrhage must always be excluded. 27 In a review of existing literature, Grzybowski and Kanclerz suggested a pars plana decompression using a small-gauge trocar/cannula vitrectomy cutter (23-, 25-, or 27-gauge), finding this procedure safer and more effective than a decompression performed with a straight needle. 14 However, Gregori et al. proposed a simple aspiration of retrolental fluid with a short 25-gauge needle on a medium-size syringe, suggesting an immediate normalization of IOP with no additional expensive instrumentation, with lower risks of cutting the posterior capsule and traction on the vitreous base compared to a vitreous cutter. 13 This management agrees with the cases reported by Lau et al., who managed IAMS with pars plana needle aspiration, suggesting no association with adverse visual outcomes. 28 Moreover, Ang et al. proposed a similar approach in the handling of IAMS during DMEK, inserting a 27G needle through the pars plana to release the gas that had migrated in the anterior vitreous, behind the IOL. 25
Intraoperative spontaneous anterior chamber fibrin reaction during DMEK is a rare complication with few reported cases in the literature, which makes the intraocular manipulation of the DMEK graft more challenging for the cornea surgeon.29–32
As fibrin in anterior chamber is not always visible, especially early during its release, intraoperative injection of trypan blue can help increase visibility. However, in our case, fibrin was evident without the aid of dye. The underlying mechanisms for fibrin formation are still not established. According to Trinh et al., this phenomenon occurs more frequently after long repeated tapping movements on the corneal surface, leading to microtrauma of the iris, and long graft unscrolling time, consistent with the dynamics of our case. 32 Risk factors are not clear either. Benage et al. proposed anticoagulation therapy, haemorrhaging during iridectomy and intraoperative hypotony as possible explanations for fibrin formation. 31 However, Trinh et al. did not confirm this hypothesis, finding no correlation between these occurrences and the fibrin reaction. 32
Tissue plasminogen activator is a protease that promotes the conversion of plasminogen to plasmin. 33 Since it plays a key role in fibrinolysis, intracameral recombinant tissue plasminogen activator (rtPA) has been proposed as a possible strategy for management of severe fibrin reaction.33–36 Rocha Lima et al. described a case of severe fibrin effusion after phacoemulsification treated with intracameral injection of rtPA (25 µg/0.05 cc), showing complete dissolution of fibrin within 30 min. 33 These results are in agreement with reports from Mehta et al., showing effectivity and safety of rtPA at a dose of 25 µg for treating fibrinous membranes following paediatric cataract extraction. 37
Although rtPA use has also been advocated in prevention of fibrinous effusion,38,39 it is not a cost-effective treatment as prophylaxis. Thus, prevention of fibrin formation by blocking the coagulation cascade pharmacologically may represent a more effective strategy for anterior chamber fibrin reaction prophylaxis in selected cases. 40 In this respect, low-molecular-weight heparin (LMWH) intraocular infusion showed reduced anterior chamber inflammatory response aided in preventing intraocular fibrin formation and was not associated with increased risk for intraoperative or postoperative complications.40–44
In conclusion, we report here a challenging case of DMEK complicated by IAMS and intraoperative anterior chamber fibrin reaction. We present our experience in the management of this uncommon surgical event and report the evidence in the literature about the most appropriate handling of this event.
Patient consent
The collection of data was performed with approval of the patient. Written consent to publish this case report was obtained. This case report does not contain any personal information that could lead to the identification of the patient.
Supplemental Material
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.