
Abstract
Background
To report the outcomes of “our modified Jensen technique” for treating esotropia in cases with complete sixth cranial nerve (CN VI) palsy.
Methods
This study is a 30-year case series of isolated complete CN VI palsy who underwent combined medial rectus recession and our modified Jensen operation. We modified the original technique by anchoring the muscle-unifying sutures to the sclera near the equator using a non-absorbable suture. Major outcomes such as postoperative diplopia, face turn, horizontal and vertical eye deviations, and abduction limitation were assessed. Successful surgery was defined as orthotropia or esotropia equal to or less than 8 prism diopters (PD) and the absence of any vertical deviation.
Results
Fifty-three cases with a mean age of 28 years old were included in this study. The male-to-female ratio was 3 to 1. Forty-five cases (85%) presented with unilateral palsy, whereas 8 patients (15%) had bilateral palsy. Trauma was the most common etiology (85%). Diplopia or face turn, presented in 42 patients before the operation, remained in seven cases after the operation. Primary position esotropia, which was the main complaint in all patients, decreased from 49 PD to 4 PD in unilateral palsy and from 101 PD to 10 PD in bilateral palsy. The mean reduction of abduction deficit was 1.78 in unilateral and 1.75 in bilateral palsy. The success rate was 76% in unilateral and 62% in bilateral palsy.
Conclusion
Our modified Jensen operation was effective in treating patients with complete CN VI palsy, producing no significant permanent complications.
Background
Sixth cranial nerve (CN VI) palsy is the most common cranial nerve palsy encountered by ophthalmologists. The etiology includes trauma, ischemia, compression, infection, autoimmune, congenital, and idiopathic causes.1,2 Patients with CN VI palsy present with esotropia and abduction deficiency. 3 Spontaneous resolution occurs within six months in most of the acquired cases. 2 Surgical approaches for correcting persistent esotropia include full-tendon and partial-tendon double vertical rectus muscle transposition (full and partial double VRT), single vertical rectus transposition (single VRT), and vertical rectus union (Jensen muscle union). Various modifications of these surgical techniques, such as augmentation sutures, resection of the transposed tendons, and simultaneous medial rectus muscle (MR) recession or chemo denervation, have been made to improve the outcomes. 3 The rectus muscle union that Jensen first described in 1964 became one of the standard transposition techniques. 4 The Jensen technique effectively resolved the ocular deviation and induced a low risk of anterior segment ischemia (ASI).5,6 However, this procedure has recently lost its popularity among ophthalmologists, and many surgeons prefer vertical rectus muscle transposition for correcting esotropia in patients with complete CN VI palsy. In this study, we reported the outcomes of “our modified Jensen technique” in patients with complete CN VI palsy drawing back attention to this transposition procedure.
Materials and methods
All medical records of patients with isolated complete CN VI palsy who were primarily treated with our modified method of Jensen technique during 30 years in our referral centre were retrospectively reviewed. Operations were all performed by a single surgeon (the senior author). By the Jensen technique, the superior and lateral rectus muscles, as well as the inferior and lateral rectus muscles, were sutured together over the equator using a non-absorbable suture.4,6,7 As shown in Figure 1, we modified the original technique by anchoring the muscle-unifying sutures to the sclera near the equator (12–14 millimetres posterior to the limbus) using a non-absorbable Mersillene 5.0 suture. We performed simultaneous ipsilateral MR recession (4.5 to 7 mm) in patients with unilateral palsy and simultaneous bilateral operation in patients with bilateral palsy.
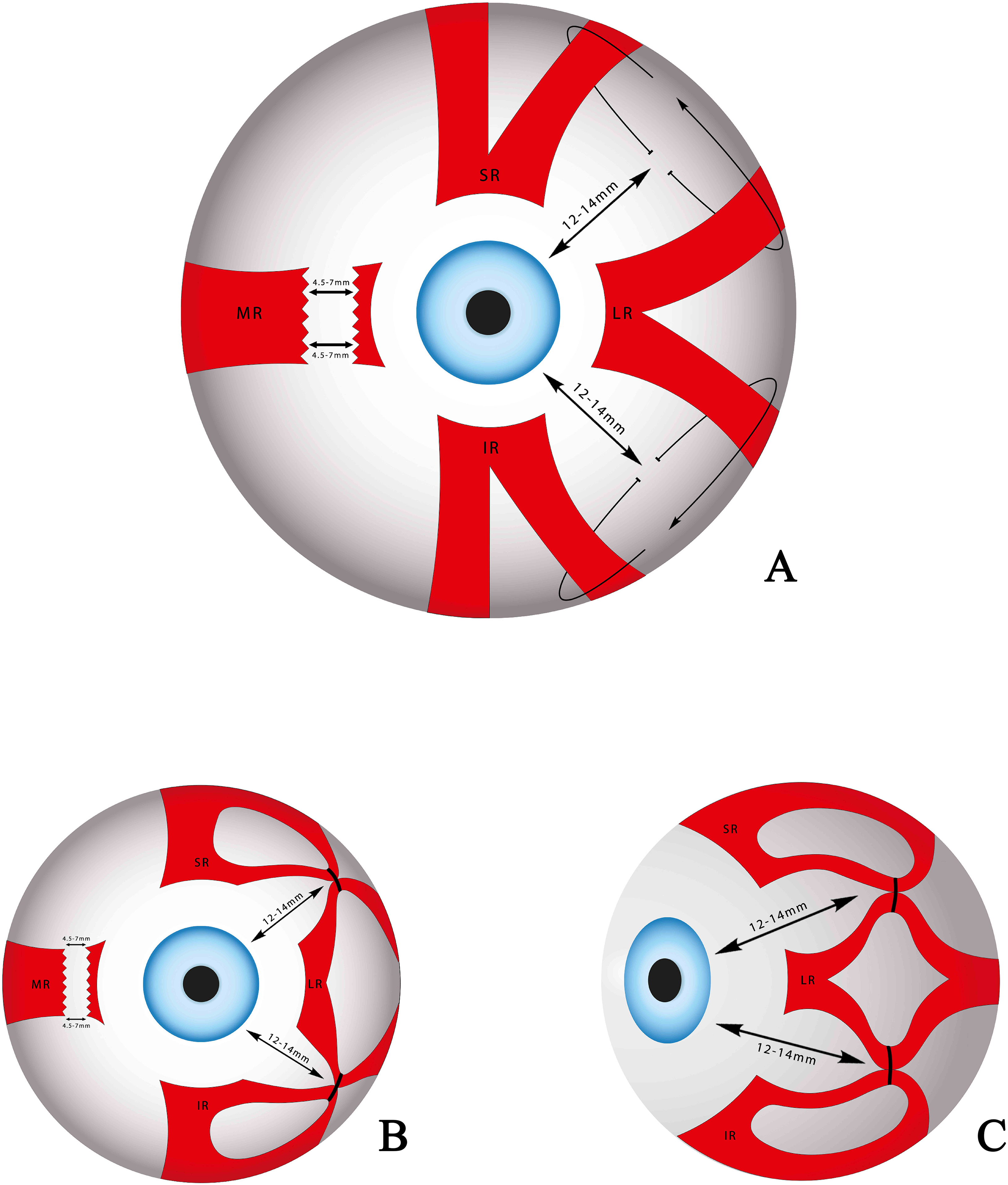
Illustration diagram of modified Jensen procedure. Note: A. Frontal view while suturing. B. Frontal view at the end of the procedure. C. Lateral view at the end of the procedure.
In this study, demographic data such as sex, age at the time of diagnosis, etiology of palsy, laterality of the involved eye, palsy to operation interval, and follow-up intervals were recruited from medical records. A prior history of botulinum toxin injection into the MR was also recorded. We collected pre- and post-operative data regarding diplopia, face turn, abduction deficit, and ocular deviations. The abduction limitation was graded on a scale from −5 to 0: −5 for inability to reach the midline, −4 for a limitation up to the midline, −3 for 75% deficit in full abduction, −2 for 50% deficit in full abduction, −1 for 25% deficit in full abduction, and 0 for no abduction limitation. 8 The ocular deviation in the primary position was measured using an alternate prism cover test in most cases. In patients with poor cooperation, the results of the Krimsky test were recorded. Our data were analyzed using SPSS Statistics for Windows, version 16.0 (SPSS Inc., Chicago, Ill., USA). Successful surgery was defined as orthotropia or esotropia equal to or less than 8 prism diopters (PD) and the absence of any vertical deviation that remained for at least six months. 3
Results
Sixty-one patients have undergone our modified Jensen technique over 30 years. Eight cases were excluded from this study due to simultaneous CN III or IV palsy, orbital fracture with extraocular muscle entrapment, or simultaneous traumatic muscle injury. Therefore, 53 patients were included in this case series. The mean age of patients at the time of presentation was 28 years (ranging from 1 to 75 years old). The male-to-female ratio was 3 to 1. Eight patients (15%) had bilateral CN VI palsy, whereas the other 45 cases (85%) presented with unilateral palsy. The left eye was involved in 25 patients (56%) with unilateral palsy. The most common cause of CN VI palsy in our series was trauma (45 cases); 44 patients had a history of a car accident (83%), and one patient (2%) had developed sixth cranial nerve palsy after falling down. Other causes of CN VI palsy included brain tumour (4 patients; 7%), vascular (1 patient; 2%), and congenital palsy (3 patients; 6%). All patients were initially observed for at least six months following the presentation and a decision for surgery was made in cases with no evidence of spontaneous recovery. The mean palsy to surgery interval was 18 months (ranging from 6 to 96 months) in unilateral cases and 14 months (ranging from 8 to 24 months) in bilateral patients. All patients were followed up for at least six months after the operation, and the mean follow-up period was 14 months (ranging from 6 to 90 months). Postoperative results remained stable in patients who were followed for more than six months.
The major outcomes of all patients, unilateral cases, and bilateral cases are summarized in Table 1. Diplopia or face turn, was present in 42 patients before the operation and remained in seven cases after the operation. All patients complained of esotropia in the primary position before the operation. Esotropia decreased from 49 PD to 4 PD in unilateral cases and from 101 PD to 10 PD in bilateral cases. The mean reduction of abduction deficit was 1.78 in unilateral and 1.75 in bilateral palsy. In the unilateral group, three patients (6.6%) developed post-operative vertical deviation (two had 5 PD hypertropia and one had 5 PD hypotropia) and two other patients (4.4%) developed ASI. One of them was a 75-year-old man with a history of hypertension and atherosclerosis and the other was a 22-year-old man with no remarkable past medical history. Both cases were successfully treated with topical and systemic steroids. After a few weeks, only mild pupil irregularity remained in both cases.
Major surgical outcomes.
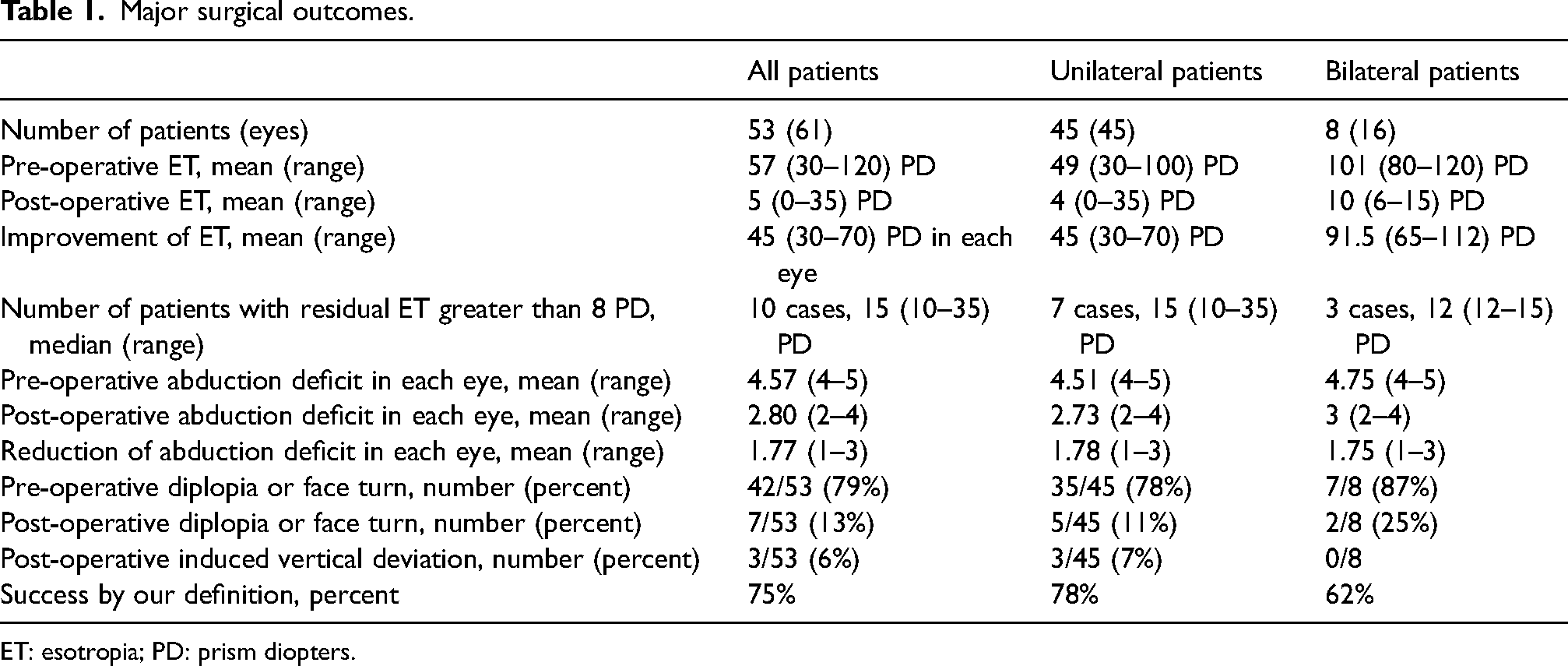
ET: esotropia; PD: prism diopters.
Seven patients in the unilateral group had a history of botulinum toxin injection into the MR at least five months before the operation. We compared the pre-and post-operative data of these patients (7 patients) with other 38 unilateral cases. No significant differences were found (Table 2).
Discussion
In this study, we reported the surgical outcomes of a large case series of isolated complete CN VI palsy who were primarily treated by our modified method of Jensen technique combined with MR recession. Our series included more young men compared to the previous reports.1,9,10 Trauma was the most common cause of CN VI palsy in our series, which was similar to other studies,6,8 although car accident was the major mechanism of trauma in this study.
Spontaneous recovery of CN VI palsy occurs in most cases within the first six months of presentation. 2 In our strabismus centre, patients with no spontaneous recovery were referred for further evaluation regarding surgical correction. The palsy to operation interval was much longer than 6 months in our case series (mean 14 months and 18 months in unilateral and bilateral cases, respectively). The traumatic cases with bilateral involvement underwent surgery slightly sooner than those with unilateral palsy.
Various surgical techniques have been employed to correct diplopia, head turn, primary position esotropia, and abduction deficiency in cases with complete CN VI palsy. Results of full or partial double VRT, as well as single VRT, and their augmentations such as simultaneous muscle resection, posterior fixation suture (PFS) of the transposed tendons, and MR recession or chemo denervation have been evaluated in several articles.1,5,8–20 Sen et al. in a review of all published studies till September 2018 calculated the weighted average of esotropia correction for each patient and abduction improvement in every specific transposition surgery. 3 They reported 0.39–1.62 grades of abduction improvement in full double VRT and its modifications, 0.29–2.72 in partial double VRT and its modifications, and 0.4–1.87 in single VRT and its modifications. 3 We recalculated the weighted average of esotropia correction in each eye, which could be a better estimation for the effectiveness of every specific procedure. The weighted average of esotropia correction in each eye following full double VRT, full double VRT with PFS, and full double VRT with MR chemo denervation was 33, 38, and 40 PD respectively. The weighted average of esotropia correction after partial double VRT, partial double VRT augmented with PFS, and partial double VRT augmented with MR recession was 25, 43, and 47 PD respectively. The weighted average of esotropia correction was calculated as 27, 44, and 43 PD in single VRT augmented by PFS, single VRT segmented with MR recession, or a combination of both.
Comparison of pre-and post-operative data of unilateral patients with or without a history of Botulinum toxin injection.
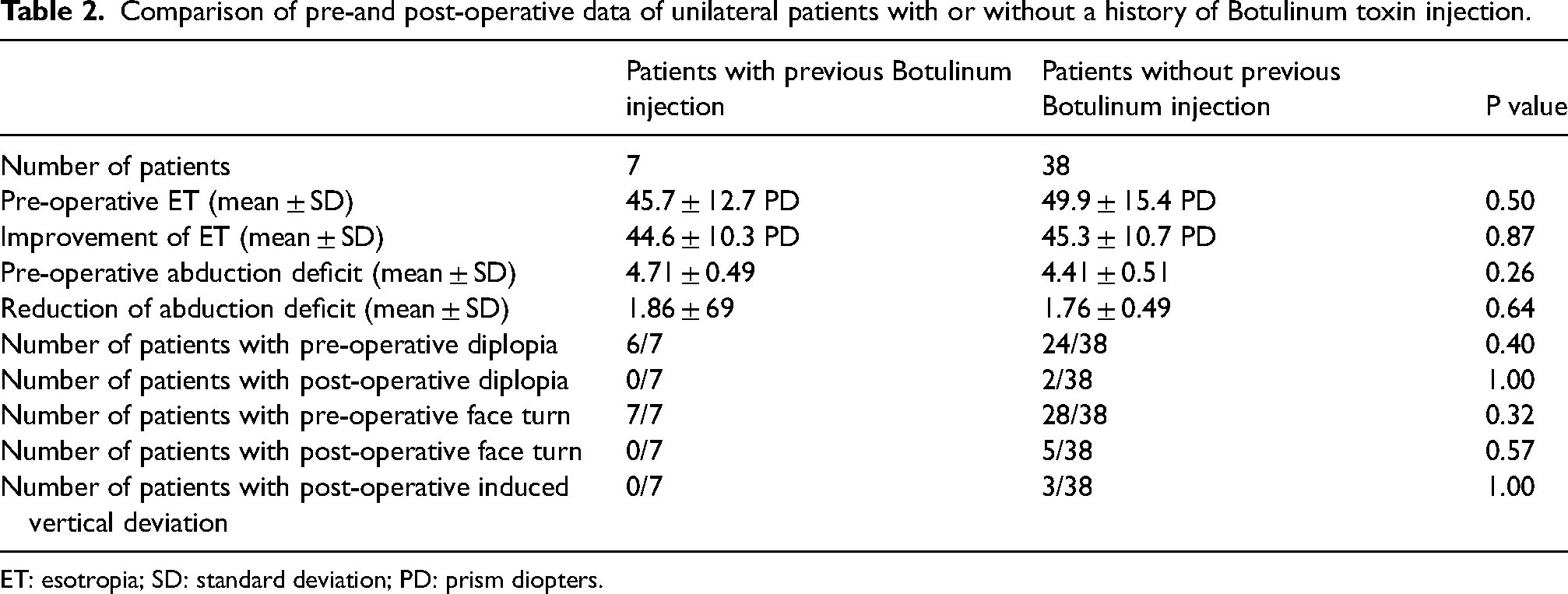
ET: esotropia; SD: standard deviation; PD: prism diopters.
Nishida procedure, which was introduced in 2003, soon became a popular technique for treating complete sixth cranial nerve palsy. Multiple studies reported 29–38 PD of esotropia correction in patients with unilateral palsy with this procedure. A combination of Nishida procedure and MR recession successfully corrected 50–62 PD of esotropia in patients with unilateral palsy and 55–79 PD of esotropia in patients with bilateral palsy.7,21–23
Various studies reported the results of the Jensen muscle union procedure, its modifications, and its combination with MR recession for correcting diplopia, face turn, primary position esotropia, and abduction deficiency in cases with complete CN VI palsy.4,6,24–28 We summarized the results of these articles in Table 3. The weighted average of esotropia correction in the Jensen procedure combined with MR recession was 44 PD. Jensen procedure combined with MR recession and vertical rectus augmentation suture (which is somewhat similar to our modification) resulted in 45 PD of esotropia correction and 1.5 grades of abduction improvement.
Surgical outcomes of the Jensen procedure and its modifications.
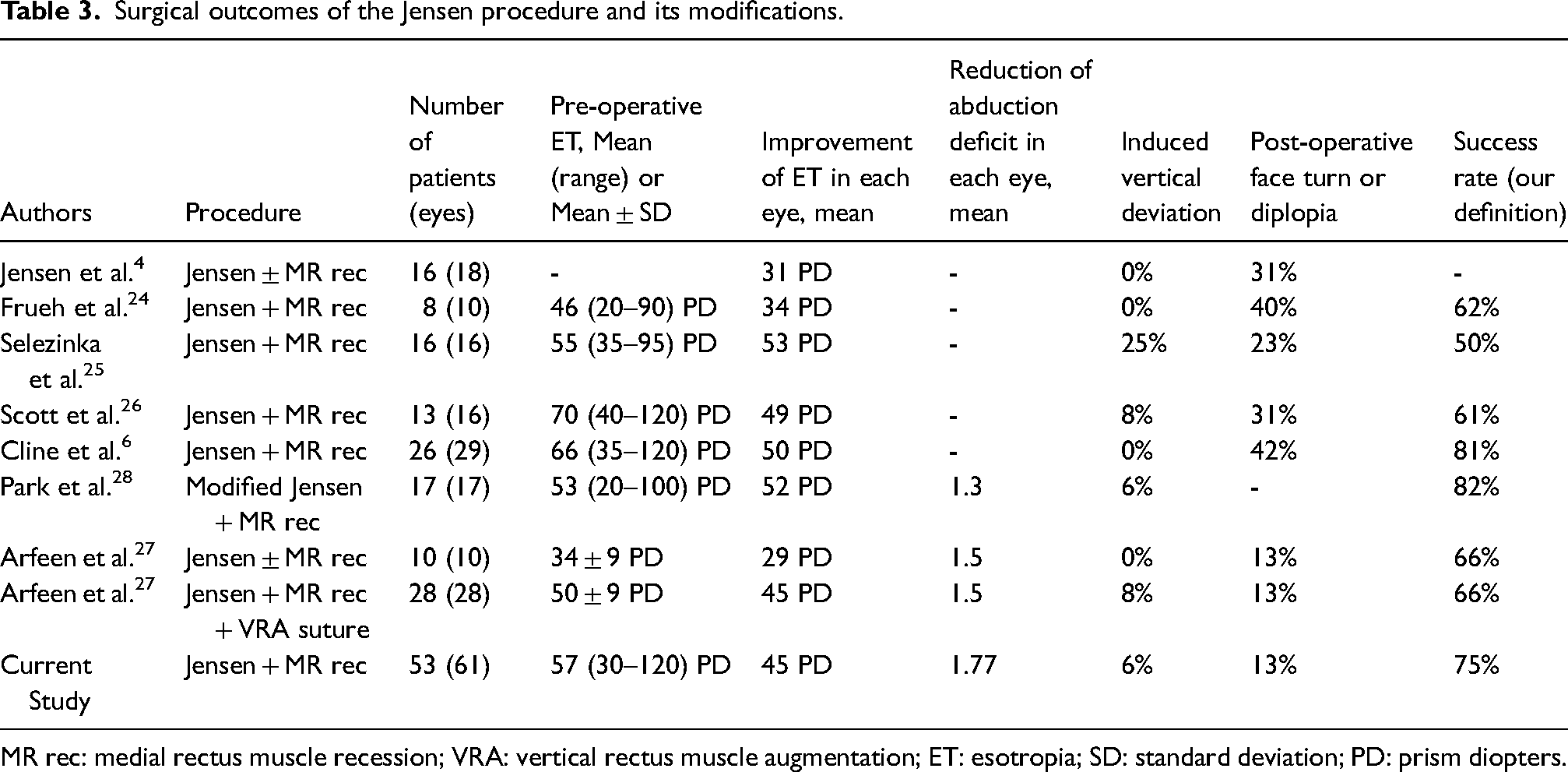
MR rec: medial rectus muscle recession; VRA: vertical rectus muscle augmentation; ET: esotropia; SD: standard deviation; PD: prism diopters.
In our study on a relatively large number of patients with unilateral and bilateral CN VI palsy, we achieved 45 PD of esotropia improvement in every single operated eye, which was comparable with the best-weighted averages previously reported in other procedures. Abduction deficit was reduced by 1.77 grade in each eye of our patients, which is as well as the other reported ones. Post-operative diplopia or face turn was presented in 13% of our patients, which is equal to or less than other studies that reported the results of the Jensen muscle union procedure and its modifications. The success rate of our surgery was 75% (78% in unilateral cases and 62% in bilateral ones), which is comparable with the results of other studies.
Few reports have previously discussed the surgical outcome of patients with bilateral CN VI nerve palsy.1,6,7,11,12,24,26 The results of these reports are summarized in Table 4. The weighted average of esotropia correction was 86 PD in eight previously reported cases of bilateral palsy treated with the Jensen procedure combined with MR recession and 70 PD in nine other cases. Our modified Jensen procedure corrected 92.5 PD of esotropia in eight patients with bilateral CN VI palsy.
Surgical outcomes of patients with bilateral 6th nerve palsy.
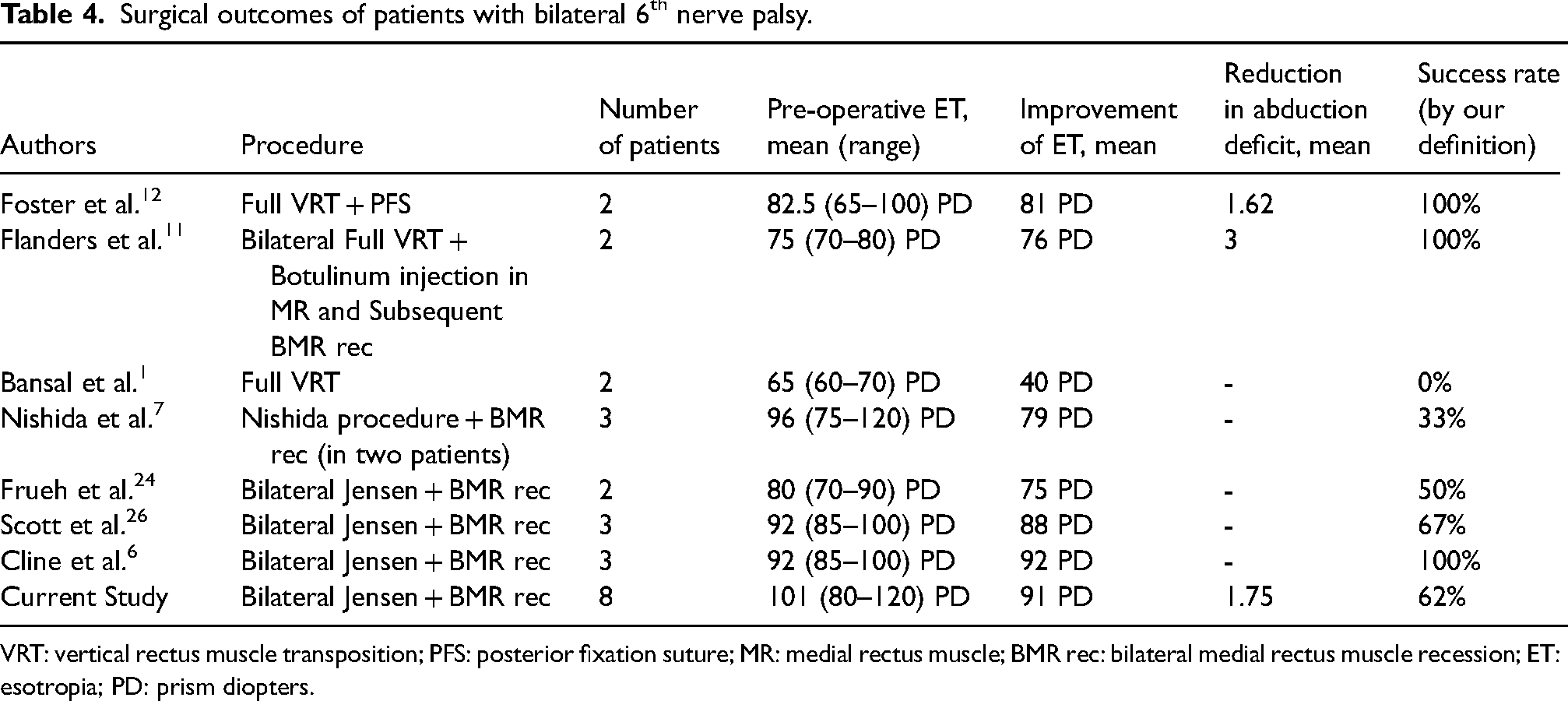
VRT: vertical rectus muscle transposition; PFS: posterior fixation suture; MR: medial rectus muscle; BMR rec: bilateral medial rectus muscle recession; ET: esotropia; PD: prism diopters.
Induced vertical deviation is a major concern in the surgical management of CN VI palsy. Undesired vertical deviation occurs after double vertical rectus muscle transposition due to asymmetric restriction of the transposed muscles. 10 The reported rate of this complication was 6–32% in full double VRT and 13–20% in partial double VRT procedures.9,10,14,15 Single VRT surgery puts patients at a higher risk for induced vertical deviation (28–71%) and torsional diplopia.18–20 The rate of induced vertical deviation was 0–25% in the Jensen muscle union and its modifications.4,6,24–28 Three patients (6%) in our case series developed postoperative vertical deviation.
A rare but potentially serious complication of strabismus surgery is ASI. It usually occurs when strabismus surgery is performed on 3 or 4 rectus muscles and is therefore a major potential concern following Jensen muscle union.9,18 Few cases of ASI have been reported after the Jensen operation, and this method still seems to be a safe surgical approach.3,6,27,28 ASI has also been reported following various types of full or partial double VRT procedures combined with MR recession or botulinum injection. 29 Recently, ASI was reported following the modified Nishida procedure. 30 In our study, two eyes (3%) developed this complication, and both were successfully treated with topical and systemic steroids leaving no permanent sequela except pupil irregularities. ASI can range from mild self-limiting inflammation to phthisis bulbi. Multiple methods were recommended over time to avoid this complication. Some surgeons prefer intraoperative botulinum injection into the MR as an alternative procedure to MR recession, and some prefer a staged approach for MR recession.3,9
It is difficult to make a fair comparison among different surgical procedures suggested for complete CN VI palsy due to various reasons. First, the number of patients in some case series was small.11,17–19 Second, patients with various forms of strabismus were included in these studies, such as Duane syndrome, and multiple CN palsy as well as unilateral and bilateral sixth nerve palsy.8,12,13,17–20 Third, some patients had a history of previous strabismus surgery.9,16,28 Fourth, different definitions were utilized for successful surgery. In most studies, exoshift was reported as the main outcome of the surgery. Since postoperative exotropia (overcorrection) is not a desirable outcome, it must be kept in mind that a larger exoshift of a certain procedure is not necessarily equal to a better surgical result.3,4,9 Fifth, the amount of preoperative esotropia varied in different reports. 3 Finally, the postoperative follow-up period was not long enough to ensure the stability of the results.8,16,18
Conclusion
Our modification of the Jensen technique combined with MR recession effectively reduced diplopia, face turn, esotropia, and abduction deficit in patients with isolated unilateral and bilateral complete CN VI palsy. It produced no significant permanent complications. However, until well-designed randomized clinical trials are conducted, it is recommended that surgeons choose their surgical approach based on their own experience and expertise.
Footnotes
Acknowledgements
The study was approved and supported by the institutional review board at Shiraz University of Medical Sciences (Grant number 13539). We would thank Miss Sepideh Saadat for preparing illustrations of the surgical technique.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Shiraz University of Medical Sciences, Grant number 13539.