
Abstract
Purpose
Scleral fixation of intraocular lenses constitutes a surgical option in cases where there is inadequate capsular support or zonular insufficiency. Knotless techniques, such as the z-suture technique, avoid suture-related complications, such as conjunctival erosion or exposure. The purpose of this study was to evaluate the visual outcomes and postoperative complications of patients who underwent scleral z-suture fixation of the Akreos AO® intraocular lenses.
Methods
A retrospective, observational study was conducted, including 22 eyes of 20 patients who underwent Akreos AO® intraocular lenses using the z- suture scleral fixation technique.
Results
The mean age of the patients was 55,64 ± 28,47 years old, and the mean follow-up time was 25,64 months. The most common indication for surgery was previous complicated cataract surgey. The mean postoperative spherical equivalent was +0,058D ± 0,79D, with values ranging from - 1,50D to +1,00D. Mean best-corrected visual acuity was 0,178 ± 0,15 logMAR. Intraocular pressure was 15,07 ± 2,56 mmHg on the day after surgery, and 16 ± 2,15 mmHg 1 month after. No suture-related complications were observed in any patient postoperatively. One patient had a slight inferonasal lens dislocation and another patient had a severe case of herpetic keratitis posoperatively.
Discussion
The knotless z-suture technique appears to be a reliable and safe way to fix an intraocular lens in the sclera, regardless of the patient's age. Our results show good visual results and predictable refractive outcomes. Decades of follow-up may be necessary to assess the long-term risk of lens dislocation.
Introduction
The surgical approach to intraocular lens (IOL) implantation in patients with inadequate capsular support is complex. There are several reasons why it may not be possible to implant an IOL into the capsular bag, the most common being capsular disruption during complicated cataract surgery, or dislocation of the lens-zonules complex due to pre-existing pathology or following trauma.1–3 Several surgical techniques and different types of IOLs have been developed for use in these cases, such as angle-supported anterior-chamber IOLs (ASIOLs), iris-claw IOLs (ICIOLs), and scleral fixation of IOLs.4,5
Scleral fixation of IOLs in the ciliary sulcus constitutes a safe option that places the IOL in a more physiological position, closer to the natural lens plane, and avoids the drawbacks associated with anterior chamber lenses, namely the proximity to the corneal endothelium.1,6 However, it is a technically challenging procedure, with a steep learning curve, that may be associated with specific short and long-term complications such as suture erosion or breakage.7,8 Classic techniques for the scleral fixation of IOLs require a suture knot, that cannot be placed directly under the conjunctiva due to the risk of conjunctival erosion, infection, and consequent endophthalmitis. For this reason, additional maneuvers to protect the knot, such as the creation of a scleral flap, are generally recommended.9–11 However, late atrophy of the scleral flap with exposure of the suture may occur in the long term. 12 Alternative methods involve the creation of a scleral pocket or a scleral groove, but although less invasive, have similar complications.13–16 The z-suture technique, first introduced by Szurman, 17 is a knotless technique for transscleral suture fixation of IOLs, in which a needle is passed through the ciliary sulcus, and the suture is secured in the sclera with a zig-zag-shaped intrascleral suture, which is then cut without any knot.17,18
The purpose of this study was to evaluate the visual and refractive outcomes of patients who underwent scleral fixation of the Akreos AO® (Bausch & Lomb, New York) IOL with the z-suture technique and to report the associated postoperative complications associated with this procedure.
Methods
A retrospective, observational, single-center study of consecutive eyes was conducted, including 22 eyes of 20 patients, who underwent implantation of the Akreos AO® IOL (Bausch & Lomb, New York) using the z-suture technique for scleral fixation.
All consecutive cases with a minimum follow-up of 1 year were included. Clinical records were analyzed for demographic data, indication for surgery, postoperative refractive error, slit-lamp examination, spherical equivalent (SE), best-corrected visual acuity (BCVA), intraocular pressure (IOP) measured by Goldmann applanation tonometry, fundus examination, and intra- and postoperative complications were reviewed. Concomitant ophthalmological disease and prior ophthalmologic surgery were noted. Spectral-domain optical coherence tomography (OCT) with Avanti RTVue XR, Optovue® was performed, when necessary, to exclude cystoid macular edema. The adopted outcome measures were postoperative BCVA, SE, IOP, and postoperative complications.
The Akreos AO® (Bausch & Lomb, New York) is a 10–11mm, single-piece, four-haptic, hydrophilic acrylic foldable IOL. 19 Each of its haptics has an eyelet that provides a potential fixation point for the suture. All patients had this IOL implanted, using the same surgical technique. The formulas used for the biometric calculation were the SRK-T and the Barret Universal II Formula, with an A-constant of 118.5, as recommended by the manufacturer. 19
All surgeries were performed by the same surgeon in the operating theatre of Hospital Pedro Hispano, under sub-tenon, peribulbar, or general anesthesia. Regarding the surgical technique, patients underwent a 25-gauge pars plana vitrectomy (PPV), using the Stellaris Elite® (Bausch & Lomb, New York) combined phacoemulsification and vitrectomy system, performing lensectomy in cases where the lens was luxated posteriorly. A conjunctival peritomy was performed at the 3 o’clock and 9 o’clock positions along the limbus to expose the underlying sclera. A 2 mm corneal limbal incision was created near the 12 o’clock position, and the anterior chamber was filled with OVD, before implanting the intraocular lens. One of the haptics of the lens was externalized through the main corneal incision, using a forceps. A straight needle 10-0 polypropylene suture was passed through the eyelet of the lens, outside the eye, creating a loop around it. This loop was then secured to the lens by tying a simple knot between the loop and the haptic. This process was repeated twice, to allow a firm anchorage of this end of the suture to the haptic of the lens. Then, the needle was inserted inside the eye through the corneal incision, passed behind the iris and externalized through the sclera at a distance of 2 mm from the limbus, guided by a bent 27-gauge insulin injector needle, at a 3 or 9 o’clock position. Two intrascleral passes, approximately 5 mm long, were then made parallel to the limbus. The procedure was repeated for the opposite haptic, which was fixed to the opposite position, 180° away from the initial location, to ensure correct positioning and centration of the IOL. The remaining two haptics of the lens were left untouched. After 2 intrascleral passes were made on each side, 3 additional passes were made bilaterally, for a total of 5 intrascleral passes on each side, which is recommended number to resist the maximum tensile force of 0,41 Newton, the most that the suture itself can withstand. 17 Finally, the sutures are cut adjacent to the sclera, without knotting. The conjunctiva was then closed with polyglactin (Vicryl®) 8-0 suture, the OVD was removed, and the corneal incision was sealed by hydrating the stroma. Subconjunctival injections of cefuroxime and methylprednisolone were administered. In pseudophakic patients with a posteriorly dislocated IOL, the procedure was adapted by retrieving the dislocated IOL and fixating it to the sclera, according to the same technique. The main surgical steps are shown in Figure 1.

For statistical purposes, BCVA usually labelled as “counting fingers”, “hand movement”, and “light perception” was converted to a decimal scale as 0.01, 0.005, and 0.0005, respectively, following the conversion method developed by C. Lange and colleagues. 20 Additionally, visual acuity (VA) represented using the decimal scale was converted to the equivalent logarithm of the minimum angle of resolution (logMAR).
This work was carried out with the agreement of the ethics committee of Hospital Pedro Hispano. Informed consent was obtained from the study participants, and the guidelines outlined in the Declaration of Helsinki were followed.
Statistical analysis was conducted using Statistical Package for the Social Sciences (SPSS) version 23.0 for Macintosh. The assumption of normality of distribution and homogeneity of variance were tested by the Kolmogorov-Smirnov test. When these assumptions were verified, a t-test for paired/independent samples was used. When those assumptions were not proved, the Mann-Whitney test for independent samples was used. Statistical significance was defined as p < 0,05.
Results
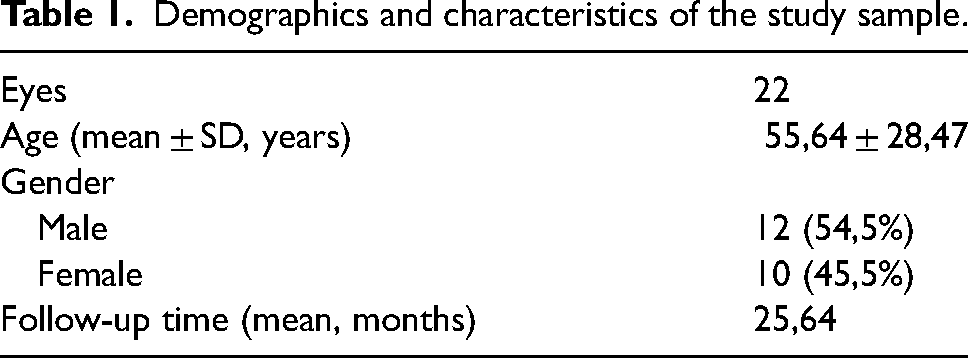
A total of 22 eyes of 20 patients were included in this study. Table 1 shows the demographics and characteristics of the study sample, where 54,5% of the patients were male, and 45,5% were female. The mean age of the patients was 55,64 ± 28,47 years old. The mean follow-up time was 25,64 months, with a minimum follow-up time of 12 months, due to the study design.
Demographics and characteristics of the study sample.
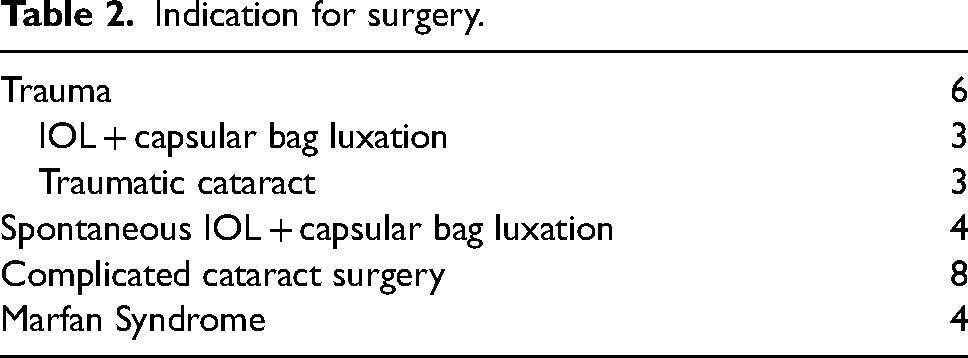
Regarding the indications for surgery, shown in Table 2, all included pathologies where there was a loss of zonular or capsular support, preventing the implantation of the IOL within the capsular bag. The most common indication was complicated cataract surgery, accounting for 36,4% of the patients, due to posterior capsule rupture or zonular dehiscence, in which there were no conditions to place the IOL in the ciliary sulcus. Traumatic injuries were responsible for 27,3% of the cases, due to traumatic cataracts or IOL luxation. Spontaneous IOL and capsular bag luxation occurred in 4 patients, all of them previously diagnosed with pseudoexfoliation syndrome. Finally, there were 4 eyes of 2 patients with lens subluxation due to Marfan syndrome.
Indication for surgery.
The mean postoperative BCVA was 0,178 ± 0,15 logMAR, with values ranging from 0 logMAR to 0,4 logMAR. Final visual acuity was influenced by coexisting ocular pathology in some of the trauma patients. One patient with a BCVA of 0,4 logMAR had a penetrating ocular injury from a car accident. The final mean SE was +0,058D ± 1,46 diopters, with values ranging from −1.50D to +1.00D. Almost half of the patients (45,5%) had a final SE between −0,50D and +0,50D, and 77,3% had a final SE between −1,00D and +1,00D.
Postoperative IOP values measured 1 day and 1 month after the surgery were 15,07 ± 4,79 mmHg and 16,00 ± 2,15 mmHg, respectively. An important bias in this analysis was the fact that some of the patients included in the study had glaucoma, namely pseudoexfoliative glaucoma, and underwent other IOP lowering procedures as well as topical hypotensive medication.
There were no intraoperative complications. Regarding postoperative complications, one patient had a slight inferonasal IOL dislocation, with no effect on the visual function, and a final BCVA of 0,05 logMAR and a SE of +1.00D. Another patient had severe herpetic keratitis in the immediate postoperative period, partially affecting the central cornea and the visual axis. This patient had a BCVA of 0,4 logMAR and a SE of +0,75D. No cases of cystoid macular edema were documented. No suture-related complications were observed in any patient, during the follow-up period.
Discussion
Implantation of intraocular lenses into the capsular bag after phacoemulsification is the gold standard of cataract surgery. However, other strategies must be used when surgical complications, trauma, or concomitant pathologies compromise the integrity of the capsular bag/zonules complex.8,21 Over the last few decades, several options have emerged to avoid prolonged aphakia. These include ASIOLs, ICIOLs, and scleral fixation of IOLs. In recent years, ASIOLs have fallen into disuse due to high complication rates involving damage to the iridocorneal angle and the corneal endothelium. 22 Traditionally, ICIOLs have been associated with complications related to their positioning in the anterior chamber, in close proximity to the corneal endothelium. Retropupillary positioning techniques are usually thought to have a protective effect on the corneal endothelium, but the evidence is not entirely clear. Some studies report no statistically significant differences regarding outcomes and complications.23,24 A recent meta-analysis by Lau et al compared the efficacy and safety outcomes between ICIOLs and scleral fixation on IOLs. 1 The final BCVA was not significantly different between groups, with similar visual improvement regardless of the technique. Absolute changes in spherical equivalent and surgically induced astigmatism were also similar. Some complications may differ between techniques, as ICIOLs may be associated with pupillary distortion due to mechanical manipulation of the iris. Endothelial cell density appears to be more affected in ICIOL implantation, regardless of antero- or retropupillary implantation. 1
Scleral fixation of IOLs in the ciliary sulcus is a safe option, that places the IOL in a more physiological position, closer to the natural lens plane, and theoretically avoids the disadvantages associated with anterior chamber lenses. 6 However, it is a technically challenging procedure with a steep learning curve. Classical complications of the scleral fixation of IOLs are usually related to the lens position and stability, and the suture itself.7,8 Most described techniques require a suture knot, which may be associated with conjunctival erosion, with potentially serious consequences due to the exposure of the underlying sclera and the fact that there is a direct pathway through the suture thread to the interior of the eyeball, with an associated risk of infection. The creation of a scleral flap, pocket, or groove prevents direct contact between the suture and the conjunctiva, minimizing that risk, but these procedures add another layer of complexity to an already delicate surgery, and atrophy of the scleral patch is also a possible long-term complication,9–11 delaying, but not preventing suture exposure. 14 The z-suture technique allows the creation of a transscleral suture fixation without the need for a knot, which is the main factor responsible for the conjunctival erosion, considering that it stands as an irregularity on the scleral surface, and creates a point of friction. As the entire suture course is intrascleral, there is no direct contact with the conjunctiva in its trajectory, thus avoiding irregularities in the scleral surface responsible for erosion. 17
The Akreos AO® (Bausch & Lomb, New York) IOL was implanted in all documented cases. Its design with four haptics, each one with an eyelet, provides support for the suture. The A-constant of 118.5, recommended by the manufacturer for in-the-bag placement, was used for IOL calculation, as the effective position of the lens is similar between both techniques. 19 A possible disadvantage of this procedure is the fact that only two of the four haptics are used to fixate the IOL, which may lead to concerns regarding the stability of the IOL, especially with regard to the risk of lens tilt, which could be an important concern. A small tilt of only 5° may induce a refractive error, and a tilt of more than 15° can lead to severe high-order aberrations, with an important impact on the final visual quality. 25 However, in our series, we had only one case of slight lens dislocation, where the IOL remained within the visual axis, and did not affect the final visual result, with a final BCVA of 0 logMAR. Nevertheless, we acknowledge that a longer follow-up period of decades may be required to assess the long-term risk of tilting or dislocation.26,27 In all cases, a 10-0 polypropylene suture was used for fixation. Some reports mention that this material may lose tension after several years, leading to the long-term possibility of lens decentration or suture breakage with lens subluxation.26,27 In our series, even in the patients with the longest follow-up time of several years, we did not have cases of suture breakage or lens decentration. Again, only a very-long term follow-up would allow this potential complication to be analyzed. A potential disadvantage of using this IOL is the fact that it is hydrophilic, and therefore more prone to opacification, especially after air or gas tamponade, 28 which may have some relevance in this context, taking into account the type of patients who undergo this surgery.
The final visual results in our series were satisfactory in terms of refractive predictability. The mean final SE was +0,058D ± 1,46 diopters, with values ranging from −1,50D to +1,00D, with almost half of the patients having a final SE between −0,50D and +0,50D, and most of them having a final SE between −1,00D and +1,00D. These results are similar to those described in the literature, where a slight tendency towards myopia had been described, with likewise deviations from emmetropy.29,30 In a series by Brunin, 35% of patients had a final refractive error between −0,50D and +0,50D, and 65% within −1,00 and +1,00D, 31 slightly below those obtained in this study. The final BCVA of the patients was satisfactory. One of the patients with a BCVA of 0,4 logMAR had a penetrating eye injury from a car accident, and another with the same BCVA of 0,4 logMAR had a severe herpetic keratitis in the immediate postoperative period with a loss of central corneal transparency. Pre-existing ocular pathology is invariably present in many of the patients submitted to this type of surgery. These comorbidities have an important impact on visual outcomes, and it is important to interpret the results in this context. This technique is often performed in complex patients, and this should be considered regarding the final visual outcome.
The only postoperative complications attributable to the surgery were one case of minor lens dislocation, with no effect on final visual acuity, and one case of severe herpetic keratitis that occurred in the immediate postoperative period. The latter is not specific to this technique and may occur in the postoperative period of any surgical technique, due to the relative immunosuppression caused by postoperative anti-inflammatory medication. There were not reported cases of cystoid macular edema, or prolonged ocular hypertension.
The main important limitation of this study was the follow-up period, which, although relatively long, does not contemplate postoperative complications that may be related to this technique after several years or decades. Other limitations of this study are related to its design, namely the retrospective analysis, the limited sample of patients, and the fact that it is a single-center study of consecutive cases.
The knotless z-suture technique appears to be a reliable and safe way to treat aphakic patients. Our results showed satisfactory visual results and predictable refractive outcomes. A follow-up of decades may be necessary to evaluate the risk of long-term lens dislocation.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.