
Abstract
Aim
to provide a detailed description and multimodal imaging (MMI) including retro-mode imaging of acute posterior multifocal placoid pigment epitheliopathy (APMPPE).
Methods
Case report of a young male patient presenting with APMPPE picture. Initially, visual acuity testing was performed, followed by biomicroscopic and fundus examinations along with MMI including Optical Coherence Tomography (OCT), fundus autofluorescence (FAF), fluorescein angiography (FA), Indocyanine Green (ICG) angiography, and Retro-mode imaging. The patient was then monitored over a duration of two months.
Results
visual acuity was 20/20 with normal biomicroscopic examination; fundus examination detected multiple pale placoid lesions. MMI was consistent with typical APMPPE. Notably, Retro-mode imaging revealed numerous crater-like round lesions that corresponded to those observed on angiography.
Conclusion
Retromode imaging in APMPPE can serve as a non-invasive tool that highlights the number and distribution of lesions as well as on angiography.
Introduction
Since its initial description by Gass in 1968, acute posterior multifocal placoid pigment epitheliopathy (APMPPE) has been clinically identified as a rare inflammatory disorder characterized by cream-colored lesions scattered throughout the posterior pole, often accompanied by painless visual impairment. 1 Once thought to originate in the retinal pigment epithelium (RPE), it was shown to most likely develop primarily in the choriocapillaris with a secondary disruption of the photoreceptors and RPE. 2
APMPPE demonstrates an equal distribution between sexes among young individuals, predominantly affecting Caucasians.3,4
Patients usually complain of bilateral visual loss, photopsias, or paracentral scotomas. The lesions gradually diminish within a few weeks with resulting chorioretinal atrophy. There may also be papillitis and retinal vasculitis.3–5 The disease has been linked to presumed infectious and inflammatory diseases, such as tuberculosis, 6 psoriasis, sarcoidosis, and erythema nodosum. 7
While various imaging modalities have been employed to describe the findings in APMPPE, we present a case wherein retro-mode imaging was utilized to further describe the distinctive characteristics of these lesions in both the acute and cicatricial phases.
Case presentation
We present a case involving a 23-year-old male who visited our emergency department with a chief complaint of bilateral scotomas persisting for a duration of two weeks. The patient described these scotomas as fixed, darkened spots that exhibited exacerbation during the morning hours. No additional symptoms were reported, and there was no subjective decrease in visual acuity.
The patient had an unremarkable ophthalmic history. Approximately three months prior to the current presentation, he had been admitted to the hospital for observation following a blunt head trauma. Subsequently, he was discharged shortly after with a normal neurological, motor, and cognitive examination. In terms of his social background, the patient maintains an active lifestyle, does not smoke, has no history of medication or substance abuse, and frequently engages in hiking activities within the forests of north-central France. The patient described being bitten by ticks several months prior to presentation, but without the development of any subsequent rash or symptoms.
On examination, visual acuity was 20/20 in both eyes with normal intraocular pressures, pupillary reactions, and ocular motility. The anterior segment examination was unremarkable, with a quiet anterior chamber in particular.
On fundus examination, several pale placoid lesions were noted scattered throughout the fundus, but mostly concentrated in the posterior poles in both eyes.
Fundus autofluorescence (FAF) showed similarly distributed hypoautofluorescent patchy spots in both eyes (Figure 1(b) and (e)).
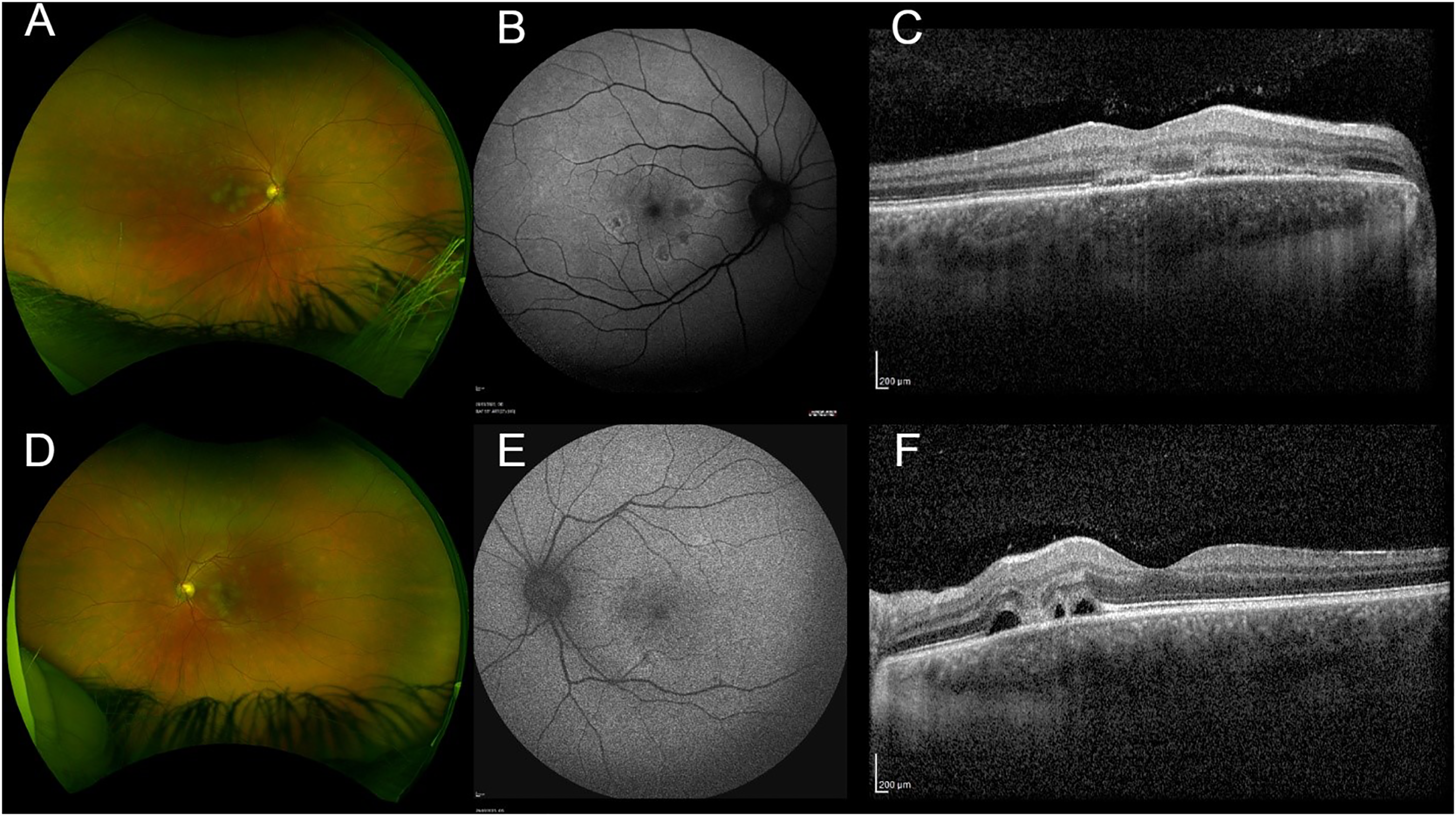
Right and left eye wide field (a, d), with the corresponding fundus autofluorescence (FAF) images (b,e) and the respective Spectral-Domaine Optical Coherence Tomography (SD-OCT) (c,f).
On spectral-domain optical coherence tomography (SD-OCT, Heidelberg, Germany), there was choroidal thickening with blurring of the ellipsoid line at the areas corresponding to the placoid lesions. (Figure 1(c) and (f))
Fluorescein angiography (FA) showed more numerous early hypofluorescent placoid lesions than visible on fundus examination that remained hypofluorescent in the later phases in the right and left eyes (Figure 2(a), (e), (i) and (c), (g), (k), respectively).
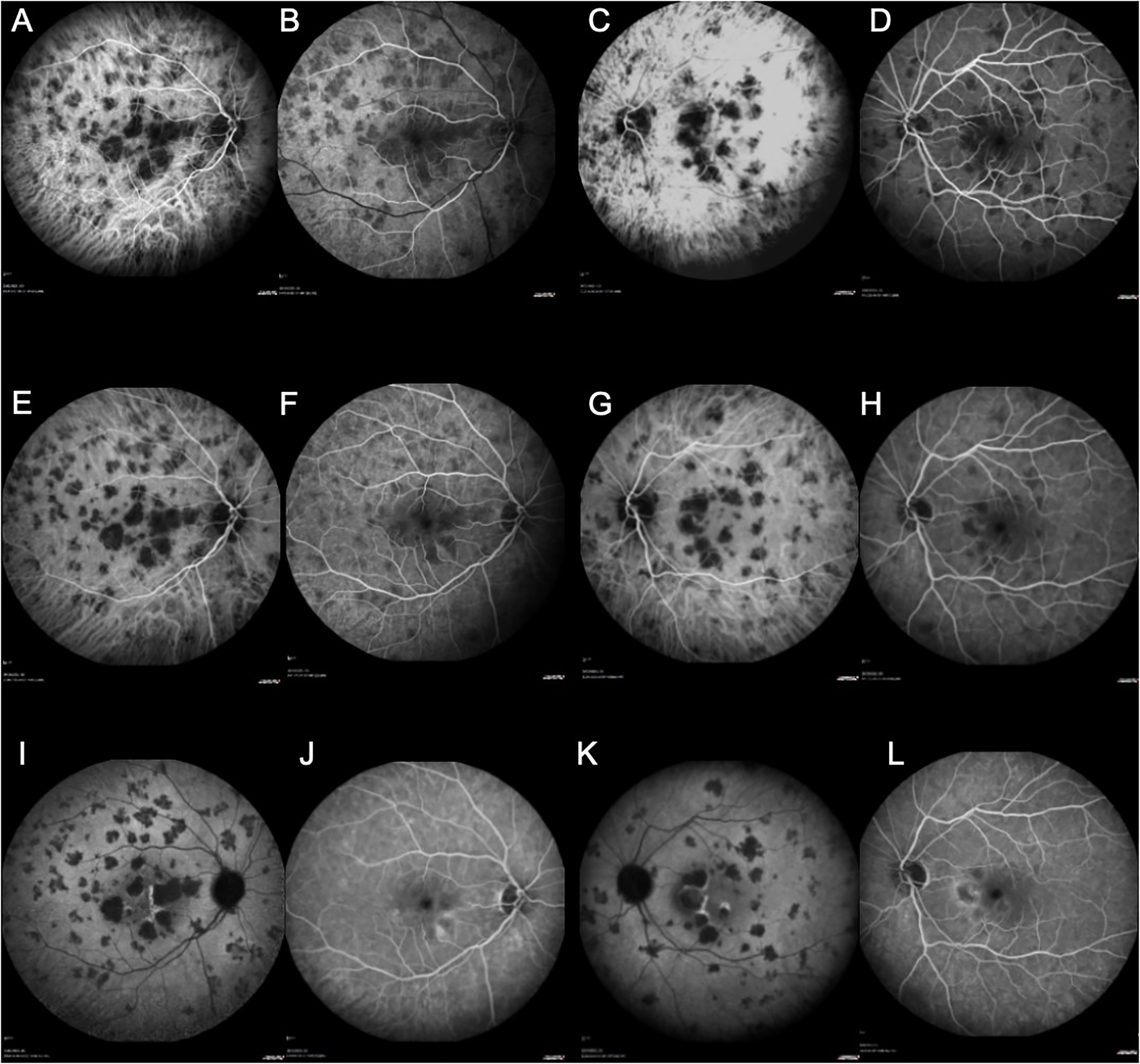
Indocyanine Green (ICG): Early times (a and c), later times (e and g), latest phases (i and k); Fluorescein angiography: Early times (b and d), Arteriovenous phases (f and h) and venous phases J and L) (FA) of the right eye and left eye.
Indocyanine green angiography (ICGA) similarly showed hypofluorescent lesions throughout the angiographic sequence, potentially corresponding to areas of choriocapillaris ischemia mainly concentrated in the macular area, but that extend outwards towards the periphery in the right and left eyes (Figure 2(b), (f), (j) and (d), (h), (l), respectively). Retro mode imaging (Mirante, Nidek, Japan) demonstrated corresponding crater-like round lesions that were as numerous as those seen on FA (Figure 3).
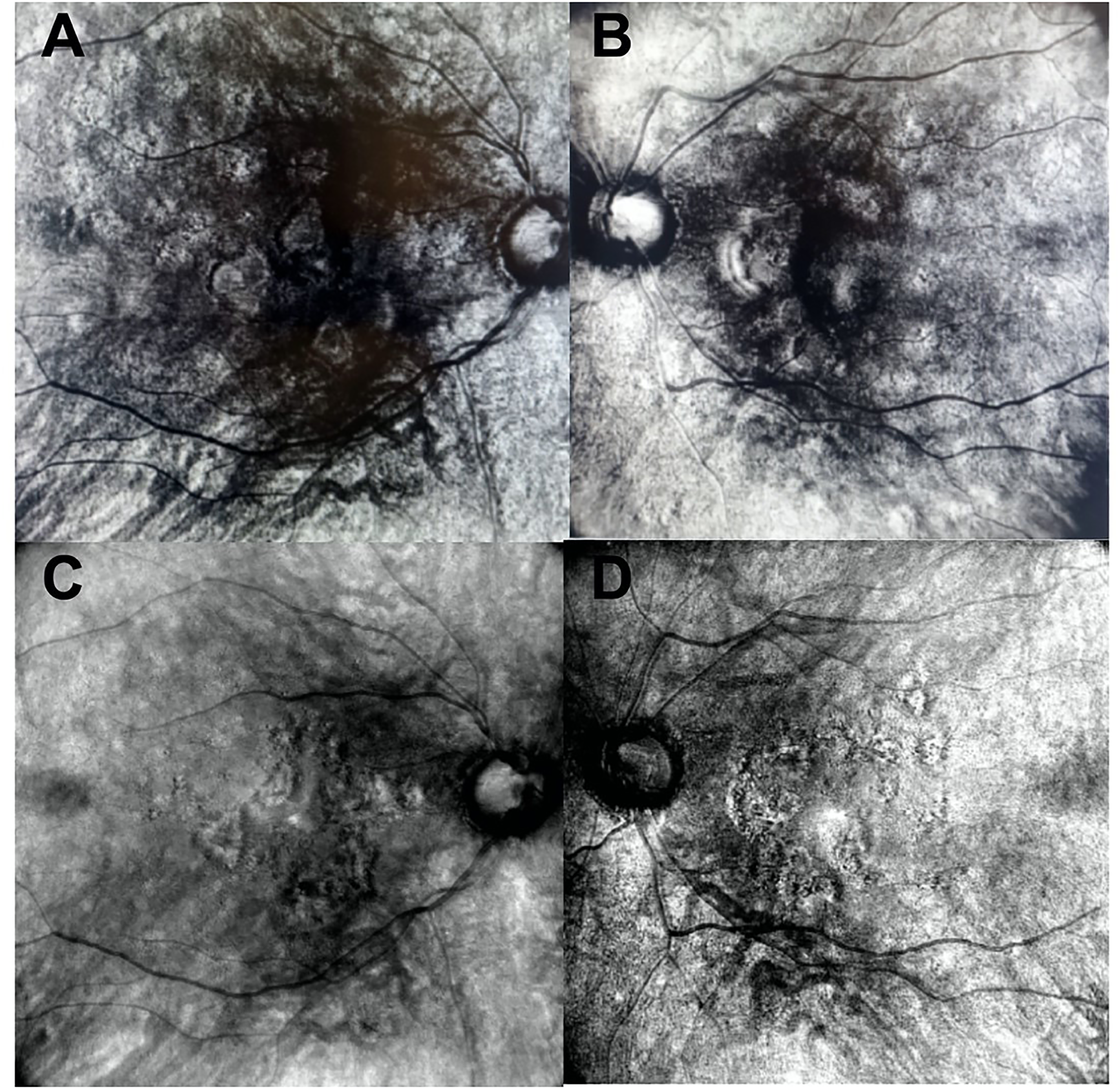
Retro-mode imaging of the right and left eye at presentation (a-d).
A provisional diagnosis of APMPPE was established, and the patient's treatment regimen commenced with oral Prednisone at a daily dosage of 60 mg for a duration of two weeks, primarily due to the proximity of the lesions to the perifoveal area (Figure 4).
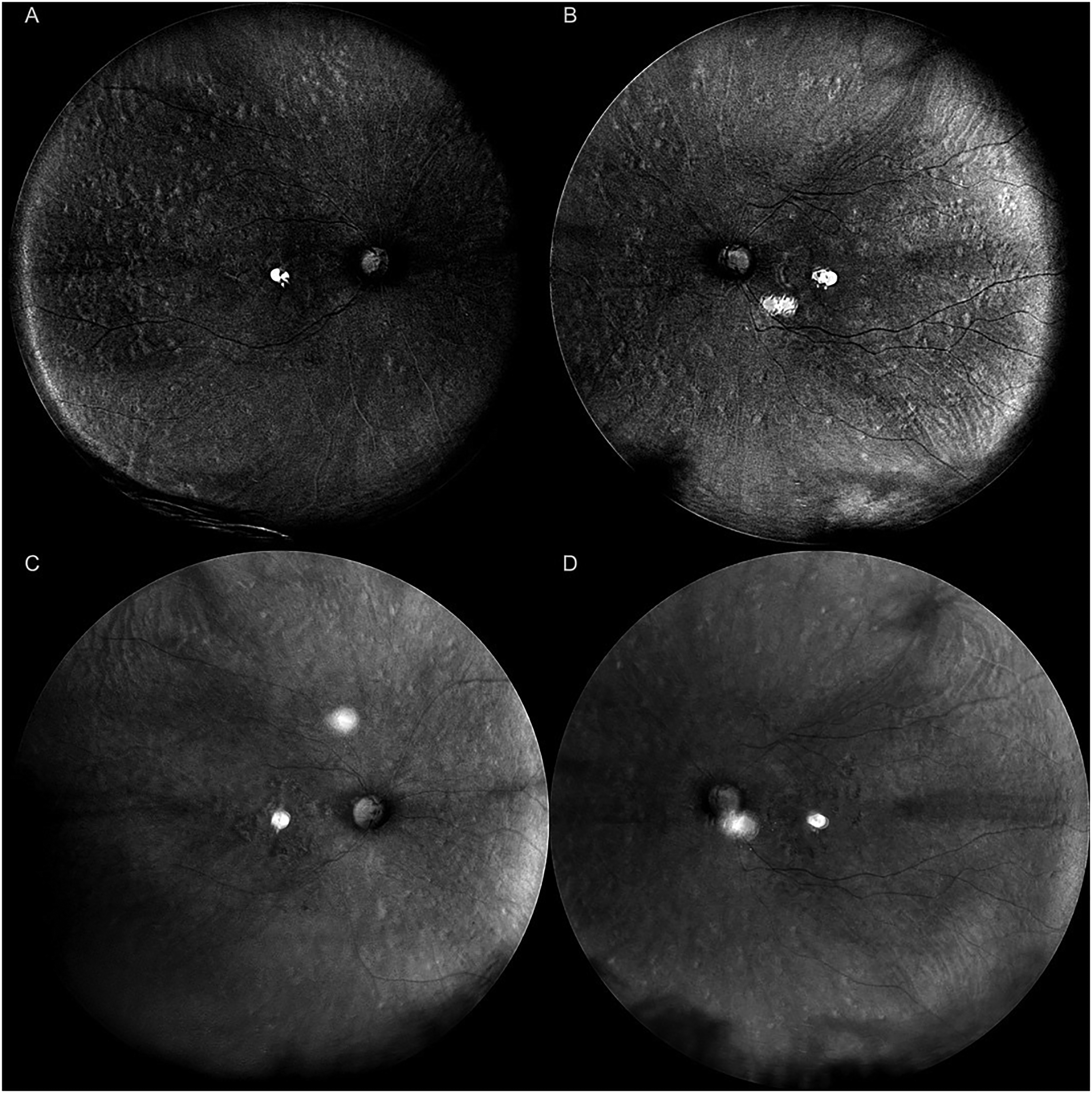
Wide-field Retro-mode photos of the right and left eyes, and the respective photos two months after presentation. Note the attenuation of the furrows over time, not only in the posterior pole, but also on the peripheral retina.
In order to conduct a comprehensive evaluation of uveitis, several diagnostic investigations were initiated. These included serological testing for Toxoplasmosis, Cytomegalovirus, Tuberculosis, Herpes Simplex, Varicella, Human Immunodeficiency Virus type I and II, Syphilis (TPHA VDRL), Borreliosis (Lyme). Additionally, we performed a complete blood count, C-Reactive protein, protein Electrophoresis, electrolytes and liver function tests. Furthermore, Brain MRI and MRA were performed to exclude any associated central nervous system vasculitis. Among the aforementioned investigations, the Borreliosis (Lyme) serology yielded positive results, with a recorded IgM anti-Borrelia level of 1.4 Ua/mL, while the IgG values were within the normal range. These serology tests were repeated two weeks later and yielded the same results, with no conversion of IgM. Due to the high false-positive rates of anti-Borrelia IgM, a confirmatory Western blot test for Lyme disease was conducted and effectively returned negative. None of the other serological, blood tests or imaging found anything pathological. Due to a cutaneous reaction, potentially due to the high-dose prednisone, the patient was started on an oral course of Doxycycline treatment for 1 month by his general practitioner, with the argument that it would effectively treat a potential co-existing Lyme disease.
During the patient's second follow-up visit, which took place two weeks later, he reported a subjective stabilization of the visual symptoms. Over the course of a two-month period, on SD-OCT there was a reduction of external retinal disruptions. The latter manifested as increasingly flattened elevations of the RPE, with a nearly complete restoration of the ellipsoid zone. The placoid lesions diminished and remained discernible only within the posterior pole. On the Retro-mode tool, the corresponding crater-like lesions attenuated were visible within the posterior pole, albeit undergoing complete disappearance in the peripheral regions.
Consequently, his treatment plan was appropriately tapered during subsequent visits, and he reported a symptomatic improvement at his third visit, two months after initial presentation.
Discussion
We presented a detailed case report of a young male patient who exhibited bilateral lesions of acute posterior multifocal placoid pigment epitheliopathy (APMPP).
During the initial fundus examination, pale lesions were observed in our case, which aligns with the literature describing such lesions as having a patchy distribution and cream-colored appearance.1,8
The following multimodal imaging revealed a typical APMPPE: FAF exhibited the presence of hypoautofluorescent patches that corresponded to the hyperreflective areas observed on spectral-domain optical coherence tomography (SD-OCT), specifically within the outer retina at the levels of the retinal pigment epithelium (RPE) and the ellipsoid zone.9,10 With regards to FA, active lesions were observed to exhibit hypofluorescence during the early phases, which may subsequently transition to hyperfluorescence in later stages.11,12 ICGA demonstrated a persistent hypocyanescence of active lesions throughout the entire examination duration, indicating impaired perfusion of the choriocapillaris.13,14
The Retro-mode imaging technique (Mirante, Nidek Co., Ltd, Gamogori, Japan) revealed the presence of multiple crater-like excavated lesions distributed in a manner consistent with the findings observed on FA and ICGA. It is worth noting that Retro-mode utilizes infrared laser light, allowing for deeper penetration into ocular layers. This property has proven effective in identifying subretinal deposits and anomalies in the retinal pigment epithelium (RPE), as seen in conditions like drusen and central serous chorioretinopathy. 15 As it acquires images from of the deep retinal layers through the lateral aperture, it creates a final image appearing as a shadow of the silhouetted retino-choroidal details, as well as abnormalities in the deeper retinal layers and choroid.
We hypothesized that the Retro-mode tool could be of use in the setting of investigation of Multiple Evanscent White Dots masqueraders (MEWDS), including APMPPE. The latter disrupts the RPE and outer retina, thus rendering the Retro-mode tool efficient in this specific case. Not only does Retro-mode tool helps in the setting of multimodal investigation when characterizing RPE level disruptions, but it could also replace invasive angiographic examinations.
Consequently, the application of this tool holds promise for characterizing inflammatory retinal disorders that can lead to disruptions at the outer retinal level, such as acute posterior multifocal placoid pigment epitheliopathy (APMPPE).
In the case at hand, Retro-mode imaging provided a non-invasive distinct pseudo three-dimensional visualization of the same numerous lesions observed on angiography.
Moreover, the Retro-mode tool demonstrated diagnostic value in terms of monitoring RPE reconstitution over time. Within a month of treatment, a significant reduction in the depth of furrows and crater-like excavated appearance of the widespread lesions was observed, indicating a positive response to therapy.
While Gass proposed an initial implication of RPE, alternative perspectives posit that early disruption of photoreceptors and the onset of choroidal ischemia may precede, resulting in a subsequent loss of RPE. Additionally, the proposition maintains that the loss of RPE persists throughout the phases of healing and resolution. 16 Using the Retro-mode tool, the RPE / photoreceptor loss is evident in the form of silhouette-like profound excavations. 15 Notably, there is a discernible reduction in the depth of these disruptions, particularly in the peripheral regions as opposed to the posterior pole. Despite the peripheral attenuation, the lesions persist to a relatively greater extent in the posterior pole even after a month, potentially suggesting a more profound ischemic impact within this specific anatomical region.
In addition to the comprehensive multimodal analysis presented in this case report, it is crucial to acknowledge and investigate the potential etiology underlying our patient's APMPPE. In this regard, the serological examination yielded a positive result for Borreliosis, thereby indicating a concurrent presence of this infectious condition. To the best of our knowledge, there have been only a few rare reports documenting the coexistence of confirmed Borreliosis, as indicated by a positive IgM test, alongside a clinical presentation of APMPPE.17,18
In our patient, even though the patient reported a history of tick bites, and IgM values were positive, there was no conversion with positive IgM or positive Western Blot, so a causal relationship between the tick bite and the ophthalmologic manifestations remains unclear.
While the scope of this case is to report the diagnosis and management of APMPPE, it is important to note that the Centers of Disease Control and Prevention (CDC) currently recommend a two-step approach for Lyme disease. If the first step is either positive or indeterminate, the second step is to be be performed. The final result is considered positive only when both tests are positive or equivocal. False positive tests occur in cases with a low prior probability of Lyme disease. Similarly, false negative results may occur in patients who are tested too soon following infection.19,20
In conclusion, Retro-mode imaging can visualize and characterize the type of lesions that appear in the setting of APMPPE. It could be used as an alternative to the more invasive angiography or as a complementary imaging method to study the RPE / photoreceptor changes alongside other investigation modalities.
Footnotes
Additional contributions
We thank the patient for granting permission to publish this information. The patient provided informed consent verbally.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.