
Abstract
Purpose
To compile real-time data on the preferred mydriasis practice patterns for retinopathy of prematurity (ROP) screening in Europe.
Methods
A cross-sectional online survey was conducted from December 2022 to January 2023, using a self-report online questionnaire which was distributed via email to the members of the European Pediatric Ophthalmological Society and the Greek National ROP Task Force. A six-week period of recruitment was determined, and a reminder email was sent after two weeks. Descriptive statistics were used to explore the data, which was summarized with frequencies and percentages.
Results
Sixty-six responses were recorded (response rate: 29.5%), representing practices in 55 Neonatal Intensive Care Units from 21 European countries. In 94.5%, the applied mydriatic regimen consists of phenylephrine with at least one muscarinic antagonist, either tropicamide or cyclopentolate. The concentration of phenylephrine ranges from 0.5% to 5%, of tropicamide from 0.25% to 1%, and of cyclopentolate from 0.2% to 1%. The most commonly used regimen (43.6%) contains phenylephrine 2.5% and tropicamide 0.5%, administered either combined or separately. About 54.5% of the reported mydriatic solutions are non-commercial, in-house preparations. Systemic adverse events, including oxygen desaturation, bradycardia and cardiopulmonary arrest were reported in 14.5%.
Conclusion
There is considerable heterogeneity in the applied mydriatic regimens for ROP screening in Europe, reflecting the absence of universal guidelines. The wide use of in-house preparations underlines the gap in the pharmaceutical industry. Concern should be raised against the wide use of undiluted commercial drugs, that reach adult dose, in the fragile population of preterm infants.
Introduction
An efficacious screening policy for the timely detection of retinopathy of prematurity (ROP) incorporates repeated eye examinations of infants at risk, on a scheduled basis. 1 International guidelines on ROP screening underline the need for a sufficiently dilated pupil to achieve adequate visualization of the periphery.2–4 Pupil dilation is accomplished using mydriatic eye drops containing either adrenergic or antimuscarinic agents, while a combination of them can also be used due to their synergistic effect. 5 Repeated instillations may be recommended since poor pupillary dilation can occur in patients with darkly pigmented irises or in advanced stages of the disease. 3
Mydriatic efficacy should not jeopardize the clinical condition of infants belonging to this fragile population and being particularly susceptible to complications, so caution should be taken in minimizing systemic adverse events. This has been attempted by amending concentrations, doses, and intervals of instilled eyedrops, or by using alternative mydriasis techniques. 6 A large variation of mydriatic regimens have been reported in the literature, 7 and most complications have been attributed to the systemic absorption of the instilled drugs. 8
Despite mydriasis being an integral part of ROP screening, the optimal mydriatic regimen has not been established yet. The purpose of the present survey was to compile real-time data on the preferred practice patterns of mydriasis for ROP screening in Neonatology Departments and Neonatal Intensive Care Units (NICUs) across Europe. Primary objectives were to identify the mydriatic regimens used and the most frequently administered regimen. Secondary objectives were to ascertain the occurrence of severe adverse events and the frequency of applying alternative mydriasis techniques as routine practice.
Materials and methods
Study design
The reporting of this cross-sectional online survey was guided by the standards of “A Consensus-Based Checklist for Reporting of Survey Studies (CROSS)”
Ethics approval
All procedures were in accordance with the 1964 Helsinki declaration and its later amendments. The study was reviewed and approved by the Institutional Bioethics Committee of Papageorgiou General Hospital of Thessaloniki, approval number 360/12–10-2022. Participation in the survey was voluntary. Filling in the questionnaire indicated the voluntary agreement to participate. The responses remained confidential.
Data collection methods
An online, self-report questionnaire was designed via Google Forms using a combination of open and closed questions, including multiple choice questions, checkboxes, and free-text options (Appendix 2). The questionnaire was composed of six sections, i.e., geographic location, mydriasis technique, lower conjunctival fornix packing, microdrops, instilled mydriatic solution, adverse events. Participants could be directed to some of the sections sequentially, depending on their initial answers; for instance, if someone did not perform ROP screening, they were directed to the end of the questionnaire straight away, if they reported using an alternative mydriasis technique they were directly forwarded to the relevant section. The survey was pre-tested by six pediatric ophthalmologists experienced in ROP screening and their feedback was used to optimize the questionnaire.
Sample characteristics
The target population was pediatric ophthalmologists who perform ROP screening in Neonatology Departments and NICUs across Europe. A purposive sampling technique was used. The sample was composed of all members listed in the 2021 to 2022 directory of the European Pediatric Ophthalmological Society (EPOS), as well as the members of the Greek National ROP Task Force (GR-ROP group). The latter consists of pediatric ophthalmologists who perform ROP screening in 16 public and private NICUs in Greece. After the distribution of the survey, responses from EPOS members that perform ROP screening in non-European countries were excluded. The eligible EPOS members are based in 30 European countries, thus constituting a highly representative sampling frame.
Survey administration
The online questionnaire was distributed via email among the EPOS members (n = 209), as well as the GR-ROP group members (n = 15). A six-week period of recruitment was determined, and a reminder email was sent after two weeks. Although the survey was anonymous, we asked the participants to report their email and which NICU they screen at in order to avoid duplicate responses from the same centre and to email respondents a query, if necessary.
Statistical analysis
Data were collected in an Excel spreadsheet and analysis was conducted using R version 4.0.3. Descriptive statistics were used to explore the data, which was summarized with frequencies and percentages.
Results
Respondent characteristics
From 2nd December 2022 to 14th January 2023, 66 responses were recorded (response rate: 66/224 = 29.5%). About 13.6% (n = 9) of the respondents do not perform ROP screening, while 4.5% (n = 3) perform ROP screening in non-European countries so they were excluded. According to the declared NICU, 6.1% (n = 4) of the responses were counted as duplicates, with no discrepancies between responses from the same NICU, while 4.5% (n = 3) of the respondents perform ROP screening in more than one NICUs. Therefore, the herein reported data concern practices in 55 Neonatology Departments and NICUs in 21 European countries
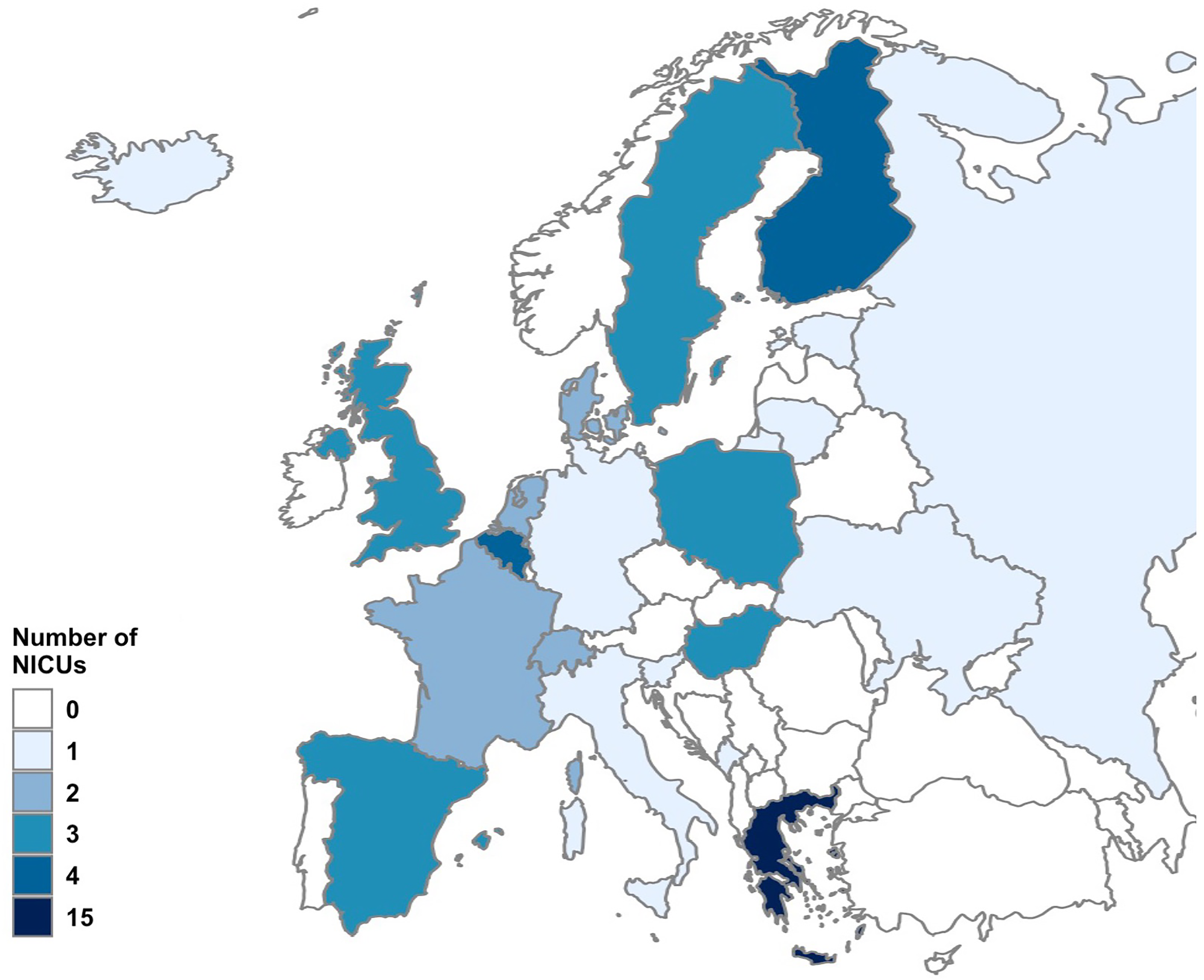
Map of Europe indicating the number of included Neonatal Intensive Care Units (NICUs) per each European country.
Main findings
The mydriatic regimens currently used for ROP screening across Europe are summarized in
Mydriatic regimens for retinopathy of prematurity screening across Europe.
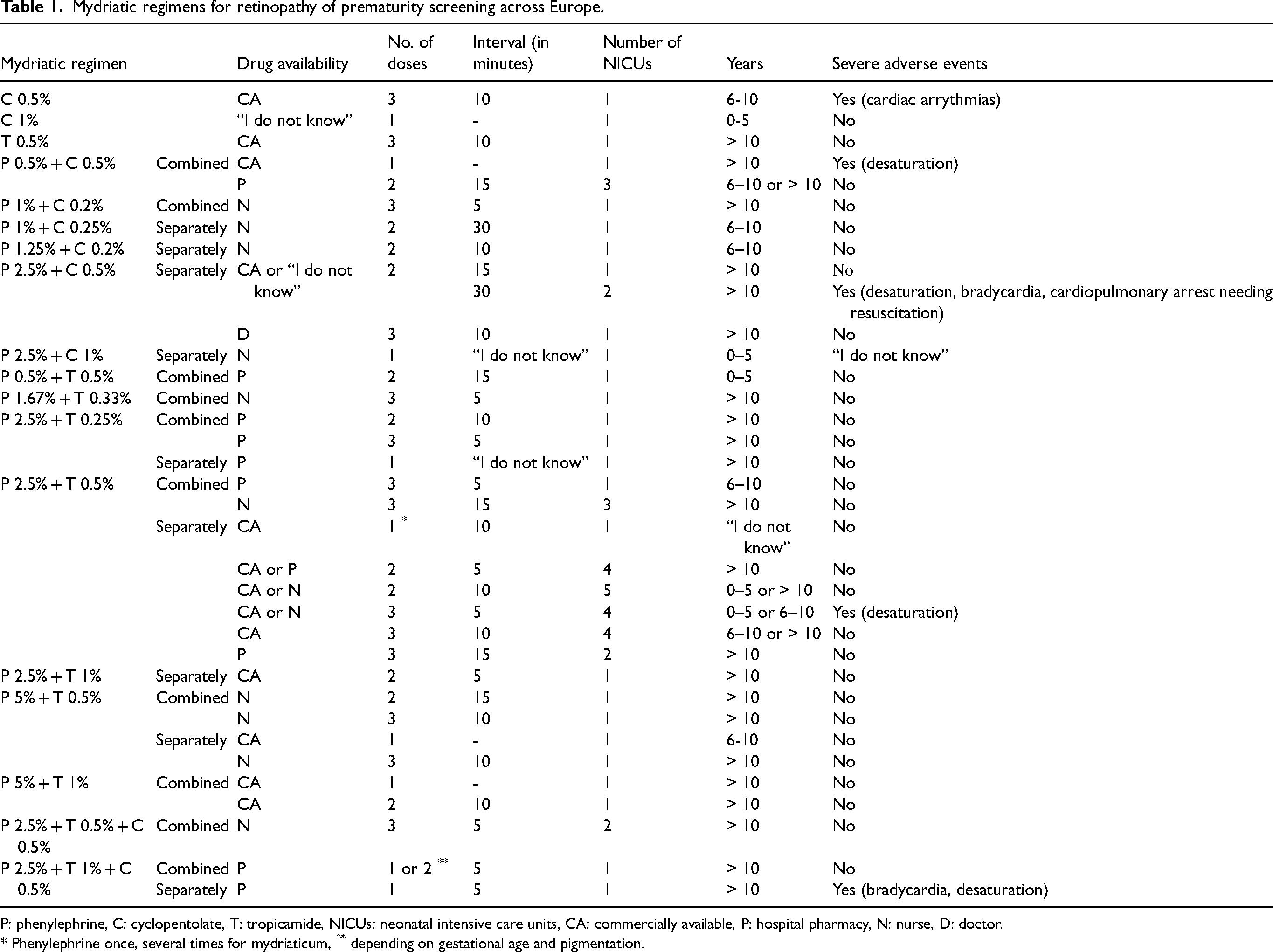
P: phenylephrine, C: cyclopentolate, T: tropicamide, NICUs: neonatal intensive care units, CA: commercially available, P: hospital pharmacy, N: nurse, D: doctor.
* Phenylephrine once, several times for mydriaticum, ** depending on gestational age and pigmentation.
The drugs’ concentration varies vastly. The concentration of phenylephrine ranges from 0.5% to 5%, of tropicamide from 0.25% to 1%, and of cyclopentolate from 0.2% to 1%. The most commonly used mydriatic regimen [43.6% (24/55)] contains phenylephrine 2.5% and tropicamide 0.5%, administered either combined or separately. The number of doses also varies, with two [40% (22/55)] or three [43.6% (24/55)] doses being more common, and the interval in-between ranges from 5 to 30 min, with 5 [31.0% (17/55)] and 10 [32.7% (18/55)] minutes interval being more common.
In case the regimen consists of two or more drugs, these are most commonly [61.5% (32/52)] administered separately. In that case, the instilled drugs are usually commercially available (CA) [53.1% (17/32)] but may also be diluted by the hospital pharmacy [15.6% (5/32)] or the nurses [25.0% (8/32)]. On the other hand, in 38.5% (20/52) the two or more drugs are administered as a combined solution, which is usually prepared by the hospital pharmacy [40% (8/20)] or the nurses [45.0% (9/20)] and is less commonly CA [15.0% (3/20)]. Of note, all respondents use standard eye drops, while alternative mydriasis techniques (e.g., microdrops, lower conjunctival fornix packing, Mydriasert®) are not being used as daily practice.
Finally, most respondents state they have used the specific regimen for more than 10 years and report severe adverse events in 14.5% (8/55), including oxygen desaturation, bradycardia, cardiac arrhythmias, even cardiopulmonary arrest needing resuscitation, especially in high-risk infants.
The above results, i.e., the variety in the regimen medications, concentrations, doses, interval, availability and preparation, and the reported adverse events, also apply to the sub-group of GR-ROP group members.
Discussion
This cross-sectional online survey depicts the diverse current mydriasis practices for ROP screening across Europe. The large heterogeneity of pharmaceutical agents, combinations, doses, and intervals is noteworthy, considering that more than 30 different mydriatic regimens are being used in 55 Neonatology Departments and NICUs in 21 European countries. To our knowledge, this is the first study compiling these real-time data in Europe.
It is unfortunate that in most cases, the instilled drugs’ concentration equals to or even exceeds the adult dose, i.e., phenylephrine 5% or 2.5%, cyclopentolate 1% or 0.5%, tropicamide 1% or 0.5%.10–13 In contrast to mydriasis routine in adults, instillation of mydriatics in preterm infants is usually applied more than once, so the total amount of absorbed medication is accumulated. This, combined with the extremely low body mass and the immature metabolizing capacities of preterm infants renders them more vulnerable to the instilled drugs’ toxicity. 8
Moreover, emphasis should be placed on the fact that more than 50% of the reported mydriatic solutions administered for ROP screening are non-commercial in-house preparations. The lack of CA mydriatic solutions in lower concentrations forces clinicians to ask the hospital pharmacy or the nurses either to dilute the commercial solution or to prepare a combined solution. 14 This gap in the pharmaceutical industry should be recognized and not be disregarded, considering the large number of patients that belong to this fragile population worldwide.
Based on the results of this survey, that are in line with relevant surveys in America, Australia, and New Zealand,15,16 most of the applied regimens contain phenylephrine with at least one muscarinic antagonist, either consecutively or in a mixture, presumably due to their synergistic effect. 5 An important advantage of a mixture is the need for reduced number of instillations and therefore less discomfort for the infant, comparing with consecutive administrations of multiple drugs. 15
There are several limitations that need to be acknowledged. First, the relatively low response rate, which can lead to non-response bias. However, response rates to email surveys are known to be highly variable, and usually average at 25% to 30%,17,18 as was the case in our study. Also, efforts were made to maximize participation by addressing a purposive sample and by sending reminders, and indeed 21 out of the 30 European countries, in which EPOS members are based, are represented in our results. Second, as expected from addressing GR-ROP group members in addition to EPOS members, Greece is over-represented in our survey. However, the heterogeneity observed was similar even within this sub-group of Greek responses and this can be attributed to the lack of national guidelines or recommendations for ROP screening. Third, it is difficult to draw safe conclusions regarding the occurrence of severe adverse events, due to the increased possibility of recall bias that is attributed to the nature of the study design, as well as due to the fact that we only addressed pediatric ophthalmologists and not nurses or neonatologists who primarily attend infants after the completion of ROP eye examination screening. However, the primary objective of the study, which was to depict the current mydriasis practices in Europe, could adequately be addressed by the target population, considering that pediatric ophthalmologists are those who prescribe the mydriatic regimen in each case.
In conclusion, there is a wide variety of applied mydriatic regimens for ROP screening in Europe, including undiluted commercial drugs that reach or even exceed adult dose thus exposing infants to dose-related adverse events. It is also remarkable that the majority of mydriatic solutions used are in-house preparations of diluted drugs or mixtures underlining the gap in the pharmaceutical industry. These results call for clinical awareness and highlight the need for a more appropriate standard of care for the vulnerable population of preterm infants.
Supplemental Material
sj-docx-1-ejo-10.1177_11206721241234952 - Supplemental material for Mydriasis for retinopathy of prematurity screening in Europe: A cross-sectional online survey
Supplemental material, sj-docx-1-ejo-10.1177_11206721241234952 for Mydriasis for retinopathy of prematurity screening in Europe: A cross-sectional online survey by Aikaterini K. Seliniotaki, Konstantinos I. Bougioukas, Maria Lithoxopoulou, Stella Moutzouri, Elisavet Diamanti, Nikolaos Ziakas and Asimina Mataftsi in European Journal of Ophthalmology
Footnotes
Acknowledgements
We would like to thank the president of the European Pediatric Ophthalmological Society (EPOS), Dr. Darius Hildebrand, and the members of the EPOS Board, Dr. Christina Gerth-Kahlert, Dr. Manca Tekavčič Pompe, Dr. Catherine Cassiman, Dr. Erika Maka, and Dr. Robert Matthieu, for their approval and their valuable support in conducting this survey. We thank Mrs Alice Hakim for her administrative support and the distribution of the questionnaire. Finally, we thank all the respondents for their contribution in this survey.
Author contributions
AKS, KIB, NZ and AM were involved in the conception and design of the study. AKS and KIB provided methodological expertise. AKS and AM collected the data. AKS and KIB performed data analysis. All authors (AKS, KIB, ML, SM, ED, NZ, AM) were involved in the interpretation of the data. AKS and AM drafted the initial manuscript. All authors (AKS, KIB, ML, SM, ED, NZ, AM) critically revised the manuscript, approved its final version for publication, and are responsible for accuracy and integrity of all aspects of research.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.