
Abstract
Purpose
To compare the safety and efficacy of micropulse laser (MP-TSCP) and slow coagulation transscleral cyclophotocoagulation (TSCP) with a diode laser for reducing intraocular pressure (IOP) in patients with refractory childhood glaucoma (CG).
Methods
Patients with CG and at least 12 months of medical chart data were included. Data on preoperative and postoperative outcomes were analyzed. The primary outcomes were an IOP of 6–21 mmHg and/or ≥ 20% reduction in the baseline value.
Results
A total of 17 eyes were included. The preoperative mean IOP was 28 mmHg in the MP-TSCP and 29.9 mmHg in the TSCP. The mean IOP decreased significantly to 17.26 ± 3.27 mmHg in the MP-TSCP and 14.68 ± 5.79 mmHg TSCP at the last medical record. Three anti-glaucoma meds were administered to the eyes preoperatively in both groups. A mean of 1.02 eye drops was administered to the MP-TSCP and 2.06 to the TSCP. The number of medications decreased by 2.38 ± 1.55 in the MP-TSCP and 0.82 ± 1.68 in the TSCP. The median preoperative visual acuity (logMAR) was 1.51 ± 1.06 in the MP-TSCP and 1.87 ± 0.74 in the TSCP. The variation in mean visual acuity (logMAR) was −0.027 ± 0.05 in the MP-TSCP and −0.40 ± 0.58 in the TSCP. The most frequent complication was corneal decompensation (one - MP-TSCP and two - TSCP).
Conclusion
Both techniques were effective and relatively safe for reducing IOP. These techniques appear to extend the indications of cyclophotocoagulation in CG eyes and improve the functional prognosis.
Keywords
Introduction
Managing childhood glaucoma (CG) remains a challenge due to the complexity and rarity of the disease, changes in tissue behavior compared to adults due to abnormal development of the trabecular meshwork and anterior chamber angle, the potential long-term effects, and difficulties encountered during the postoperative course.1,2
CG is most common glaucoma in infancy. The incidence and management of outcomes vary among populations and studies. 2 The introduction of new diagnostic tools, intraocular pressure (IOP)-lowering drugs, and improved surgical techniques have improved the prognosis of this devastating disease and preserved the vision of affected children. 3
CG treatment for children with glaucoma is primarily surgical, except when the child cannot travel to undergo a surgical procedure due to clinical disability. 3 The preferred initial management is angle surgery, such as goniotomy or trabeculotomy, which improves the poor prognosis of CG. Trabeculectomy and glaucoma drainage devices are secondary options in refractory cases.3–9
Cyclodestructive procedures are used when surgery fails. 1 °Cyclophotocoagulation (CPC) is a cyclodestructive procedure that has been the mainstay treatment for ciliary destruction in pediatric glaucoma cases. CPC uses a diode laser wave to destroy the ciliary epithelium. The number of sessions required to achieve adequate IOP control is difficult to predict.10,11 This technique is traditionally applied using continuous laser energy. 11 Complications of CPC in children are similar to those in adults. The most serious complications include hypotony, phthisis, and decreased or loss of vision. 12 Alternatives with lower morbidity include micropulse transscleral cyclophotocoagulation (MP-TSCP), which uses a laser intermittently, and slow coagulation transscleral cyclophotocoagulation (SC-TSCP). 13
MP-TSCP delivers a series of short, repetitive pulses of laser energy to the ciliary body separated by rest periods. Periods without laser activity reportedly allow for thermal dissipation, and thus reduce collateral damage and adverse effects.11,13 However, SC-TSCP delivers a continuous pulse of thermal energy, but with lower energy and over a longer period, thereby avoiding damaging the ciliary body and thus reducing the inflammatory response.
MP-TSCP has shown promising results and a good safety profile. However, its effects in the pediatric population remain unclear.14,15 Only a few small studies have been conducted on MP-TSCP for childhood glaucoma, and these had short follow-up periods and involved multiple previous ophthalmological procedures. The purpose of this study was to compare the safety and efficacy of MP-TSCP and SC-TSCP in patients with CG.
Material and methods
Ethics
The Institutional Review Board of HCLOE Clinica de Oftalmologia Especializada approved this study, which complied with relevant data protection and privacy guidelines. The patients’ information was anonymized. The study adhered to the Declaration of Helsinki and the requirement for informed consent was waived due to its retrospective, non-interventional design.
Study design and population
This retrospective multicenter study compared the efficacy and safety of MP-TSCP and SC-TSCP using a diode laser in patients with CG and accompanied during the first year after the laser procedure. All data were collected from December 2020 to February 2021. The surgeries were performed at four tertiary referral ophthalmic surgery centers in Brazil (HCLOE Opty Group Brazil-São Paulo, SP; Oculare Hospital de Oftalmologia-Belo Horizonte, MG; HR Oftalmologia-Curitiba, PR; and VisionOne-Hospital de Olhos CBV, Brasilia). All of the surgeons were highly experienced with the various types of lasers used. The parameters described by the Brazilian Glaucoma Society were used as a reference. One eye of each patient diagnosed with CG and treated with the MP-TSCP or SC-TSCP technique was included. Definition of CG was based on the Childhood Glaucoma Research Network (CGRN) classification system [that obtained consensus agreement at the Ninth World Glaucoma Association Consensus]
Outcomes
We collected data on visual acuity, tonometry, the number of eye drops used, associated comorbidities, and previous surgeries before the laser procedure. Medical chart data during the first year after the laser procedure were analyzed for intraoperative and postoperative complications, IOP, visual acuity, the need for additional glaucoma surgery, repeat MP-TSCP or SC-TSCP, and the number of topical medications used.
The criteria for a successful operation were a decrease of > 20% in the preoperative IOP (criterion A) and/or IOP of 6–21 mmHg at the last visit (criterion B), with or without medication. The need for other types of anti-glaucoma surgery to reduce IOP following MP-TSCP or the SC-TSCP, such as fistulizing surgery, drainage implants, or traditional cyclodestructive procedures, was considered to indicate surgical failure. However, multiple MP-TSCP or SC-TSCP procedures were not considered to indicate failure. All repeat MP-TSCP and SC-TSCP procedures were conducted in the same manner as in the initial operation.
Surgical procedure
SC-TSCP was performed by experienced glaucoma specialists using an IRIS Medical infrared diode laser (810 nm; OcuLight SLx; Iris Medical Instruments, Inc., Mountain View, CA, USA), after peri or retrobulbar block with 2% xylocaine. The G-probe was positioned 1.5 mm from the limbus, and the initial power was set to 1,500 mW for 4 ms, preserving the regions at 3 and 9 o’clock. Three quadrants were usually treated (e.g., 180° superiorly, and 90° in the inferonasal or inferotemporal quadrants). The treatment was delivered at six or seven points per quadrant (total of 18–21 points). The energy level was adjusted to avoid the popping sound characteristic of ciliary body destruction.
MP-TSCP was performed with the IRIDEX Cyclo G6 laser (Iridex Corp., Mountain View, CA, USA). The infrared diode laser was applied at 2,000 mW, with a duty cycle of 31.3% (0.5 ms of “on time” and 1.1 ms of “off time”). The MicroPulse P3 probe was firmly applied perpendicular to the sclera, with the edge of the probe on the limbus at all times. The probe was moved in a continuous sliding motion in the upper and lower quadrants, avoiding the 3 and 9 o’clock meridians. The treatment time ranged from 100 to 320 s.
After the procedure, a topical corticosteroid was applied every 4 h, with gradual tapering and cessation after 30 days. Then, 1% atropine was administered every 12 h for 2 weeks.
Data collection and eligibility
We included CG patients who had already been treated with traditional surgery, but for whom clinical control was not achieved even with the maximum topical therapy that they could tolerate. When both eyes were affected, the first operated eye was selected. A minimum of 12 months of medical chart data during the first year after the laser procedure were required for study inclusion. The need for other types of anti-glaucoma surgery to reduce IOP following MP-TSCP or the SC-TSCP, such as fistulizing surgery, drainage implants, or traditional cyclodestructive procedures, was considered to indicate surgical failure. However, multiple MP-TSCP or SC-TSCP procedures were not considered to indicate failure. data were required for study inclusion. The participants were divided into group A (MP-TSCP) and group B (SC-TSCP).
Inclusion criteria
Patients were eligible to be enrolled in this study if they had been diagnosed with refractory childhood glaucoma, previous glaucoma surgery, and uncontrolled IOP (defined as IOP > 21 mmHg despite maximal tolerated anti-glaucomatous drugs).
Definition of childhood glaucoma – 2 or more required:
- IOP > 21 mmHg - Optic disc cupping: a progressive increase in cup-disc ratio, cup-disc asymmetry of ≥ 0.2, when the optic discs are similar size, or focal rim thinning. - Corneal findings: Haab striae or diameter > or = 11 mm in newborn, > 12 mm in child < 1 year of age, > 13 mm any age. - Progressive myopia or myopic shift coupled with an increase in ocular dimensions out of keeping with normal growth. - A reproducible visual field defect that is consistent with glaucomatous optic neuropathy with no other observable reason for the visual field defect.
Exclusion criteria
Patients who had undergone previous cyclodestructive maneuvers and eyes with significant scleral thinning (thinning of more than one clock hour noticed by scleral transillumination) were excluded from the study
Statistical analyses
Categorical variables are presented as numbers and percentages and were analyzed with Fisher's exact test. Continuous variables are expressed as mean and standard deviation (SD) or median and interquartile range. A p-value < 0.05 was considered significant. Stata software (release 13; StataCorp, College Station, TX, USA) was used for the analyses.
Results
A total of 17 eyes from 17 patients underwent the procedures. Eight eyes underwent transscleral MP-TSCP, and nine underwent SC-TSCP. The mean age was 22.3 years in the MP-TSCP group and 26.4 years in the TSCP group (p = 0.34). There were four females in each group, and four and five males in the MP-TSCP and SC-TSCP groups, respectively. The need for other types of anti-glaucoma surgery to reduce IOP following MP-TSCP or the SC-TSCP, such as fistulizing surgery, drainage implants, or traditional cyclodestructive procedures, was considered to indicate surgical failure. However, multiple MP-TSCP or SC-TSCP procedures were not considered to indicate failure. 12 months of medical chart data were collected for all eyes. CG was the diagnosis in all cases.
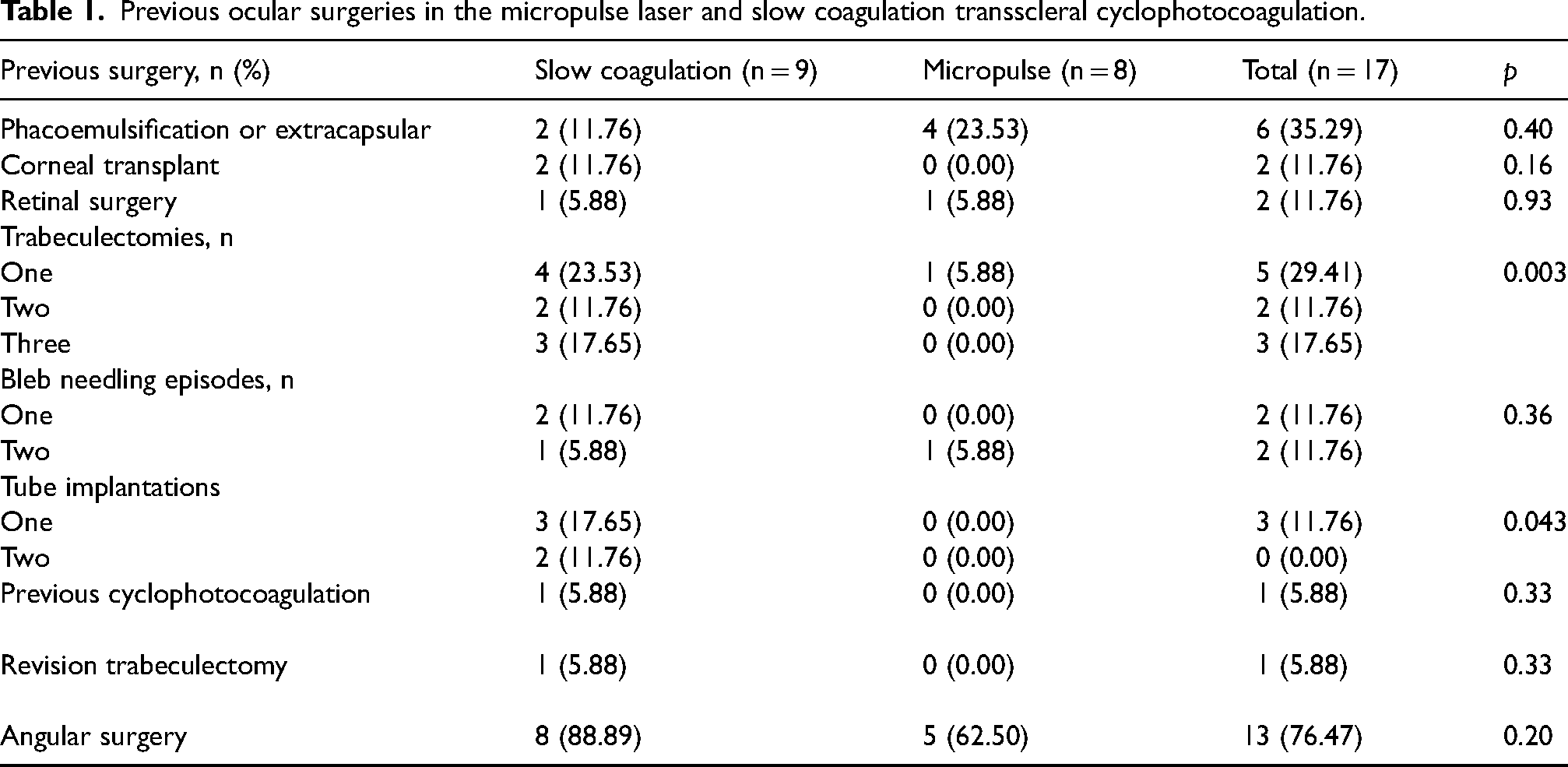
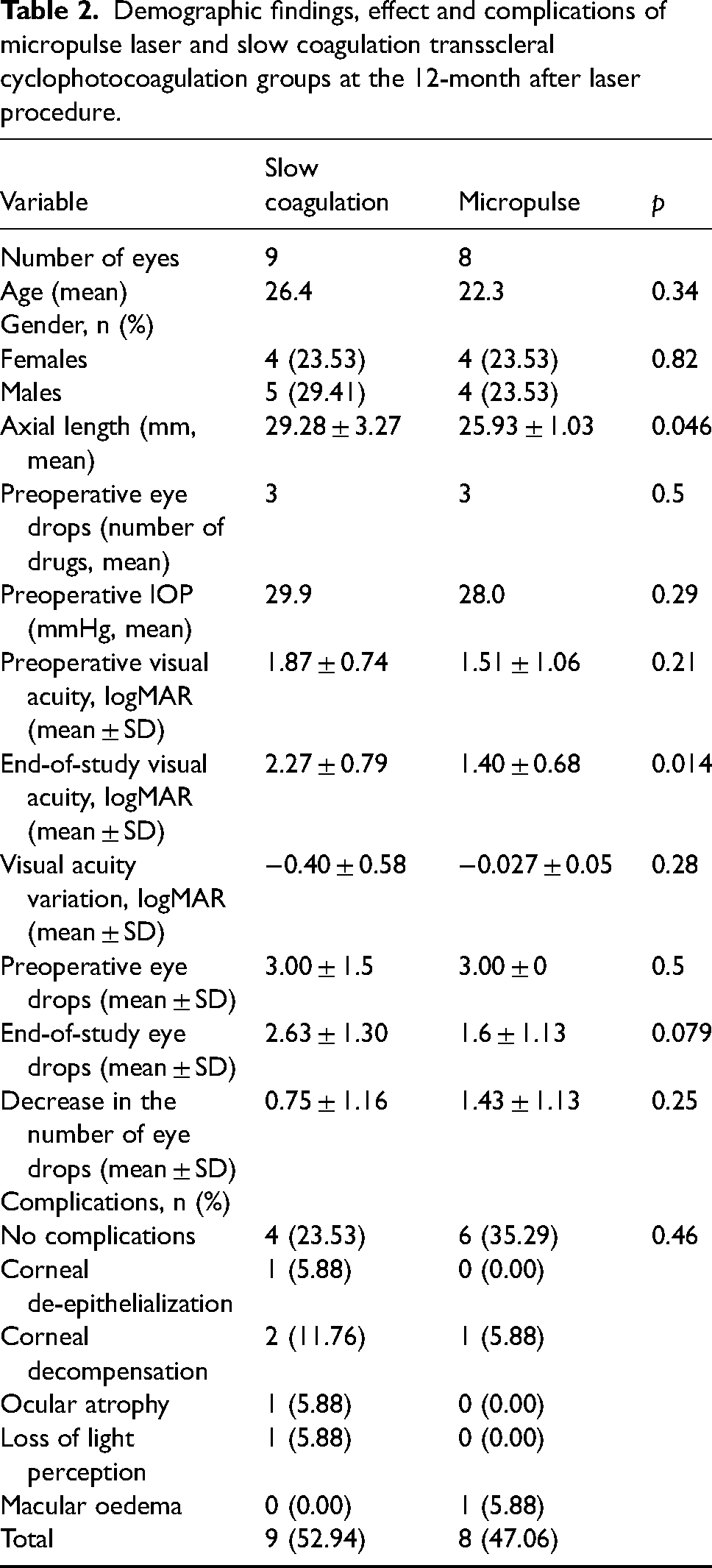
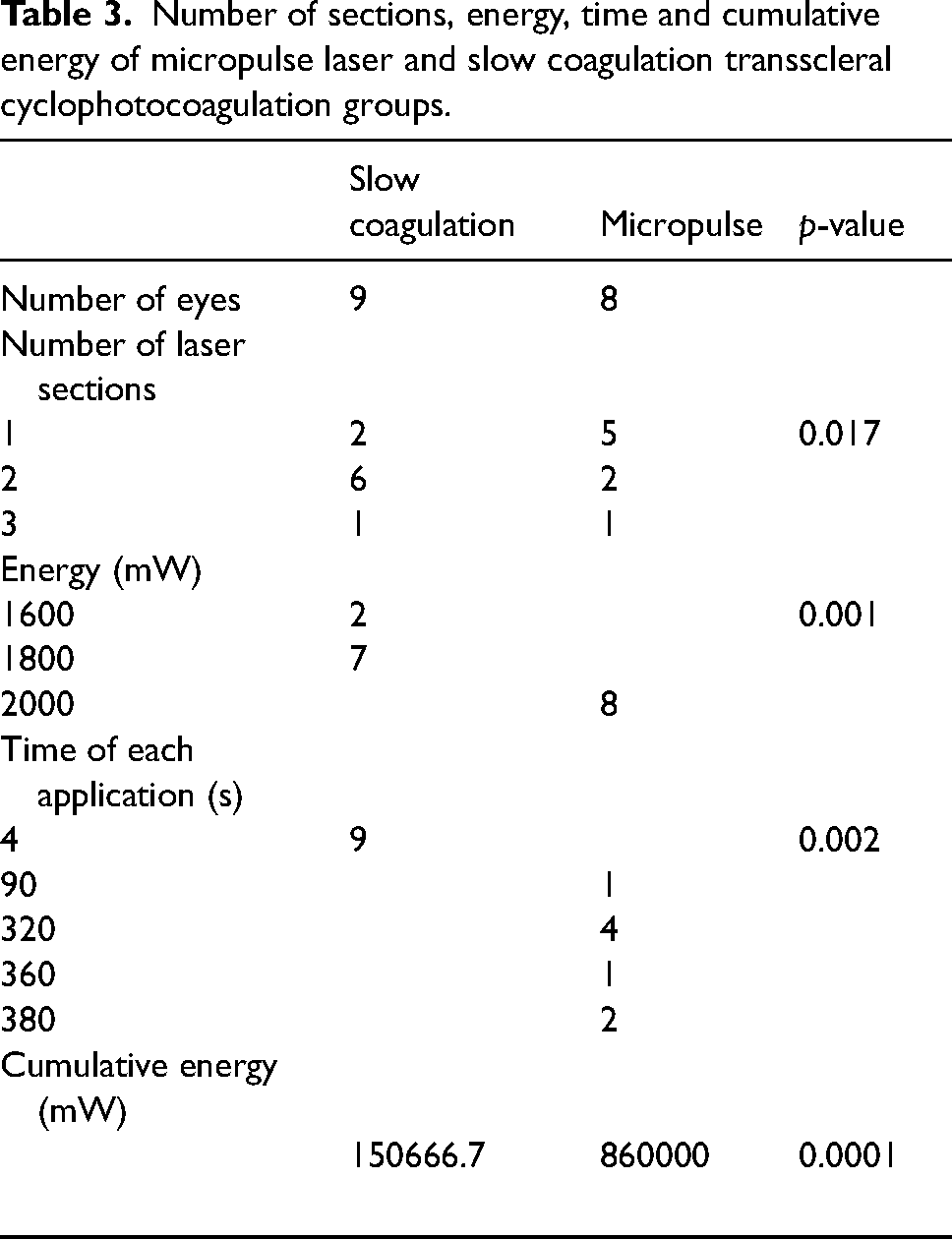
The mean preoperative IOP was 28 and 29.9 mmHg in the in MP-TSCP and SC-TSCP groups, respectively (p = 0.29). The mean number of preoperative eye drops was 3 in both groups (p = 0.5). The preoperative visual acuity (logMAR) was 1.51 ± 1.06 in the MP-TSCP group and 1.87 ± 0.74 in the SC-TSCP group (p = 0.21). Mean axial length was 29.28 ± 3.27 mm in the SC-TSCP group and 25.93 ± 1.03 mm in the MP-TSCP group (p = 0.046). The previous ocular surgeries are described in Table 1. Demographic findings, effect and complications of each technique are described in Table 2. Number of laser applications, energy (mW), time for each application and cumulative energy are described in Table 3.
- Effect of the techniques on IOP
Previous ocular surgeries in the micropulse laser and slow coagulation transscleral cyclophotocoagulation.
Demographic findings, effect and complications of micropulse laser and slow coagulation transscleral cyclophotocoagulation groups at the 12-month after laser procedure.
Number of sections, energy, time and cumulative energy of micropulse laser and slow coagulation transscleral cyclophotocoagulation groups.
The mean IOP decreased significantly to 17.26 ± 3.27 mmHg in the MP-TSCP group and 14.68 ± 5.79 mmHg in the SC-TSCP group after 12 months (p = 0.14). The mean decrease in IOP at 12 months was 10.74 ± 8.36 mmHg in the MP-TSCP group and 15.21 ± 6.59 mmHg in the SC-TSCP group (p = 0.12) (Figure 1).
- Effect of the techniques on the anti-glaucoma drug doses
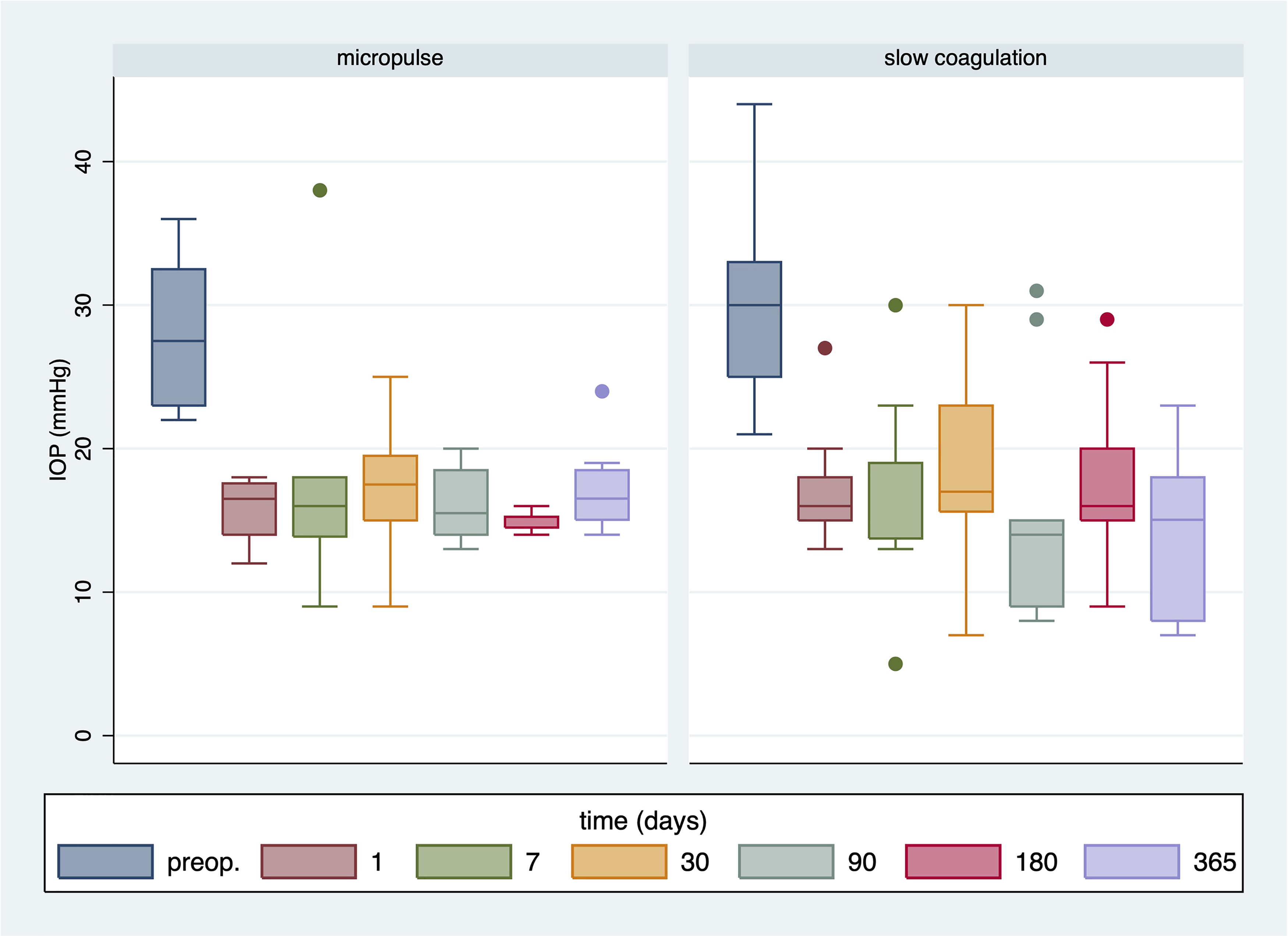
Variations in intraocular pressure over time in the micropulse laser and slow coagulation groups.
The mean number of eye drops administered at the end of the study was 1.6 ± 1.13 in the MP-TSCP group and 2.63 ± 1.30 in the SC-TSCP group. The decrease in the number of eye drops administered was 1.43 ± 1.13 in the MP-TSCP group and 0.75 ± 1.16 in the SC-TSCP group (p = 0.25).
- Success rate, retreatments, and complications
The mean variation in visual acuity (logMAR) was −0.027 ± 0.05 in the MP-TSCP group and −0.40 ± 0.58 in the SC-TSCP group (p = 0.28). Criterion A was met with similar frequency in both groups after 12 months. Six eyes (75%) in the MP-TSCP group and seven (77.77%) in the SC-TSCP group achieved a decrease in IOP of ≥ 20% (p = 0.89). There was a trend toward a significant group difference in the frequency of meeting criterion B (IOP of 6–21 mmHg; four eyes [50%] in the MP-TSCP group and seven eyes [77.77%] in the SC-TSCP; p = 0.079). Kaplan–Meier curves representing the probability of treatment success over time are shown in Figure 2 (Criterion A) and Figure 3 (Criterion B).
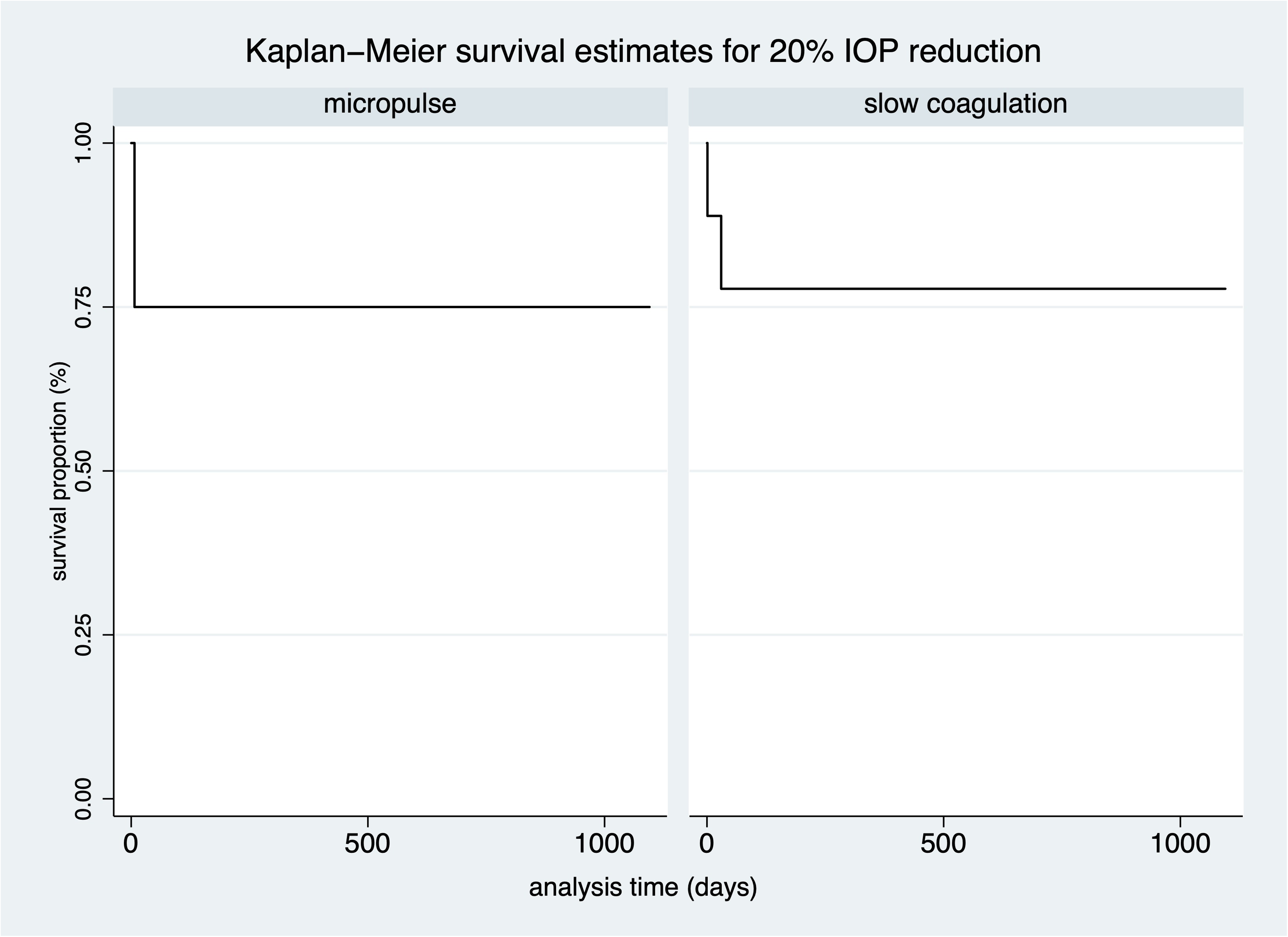
Kaplan–Meier curves representing the probability of treatment success over time. Criterion A: 20% IOP reduction.
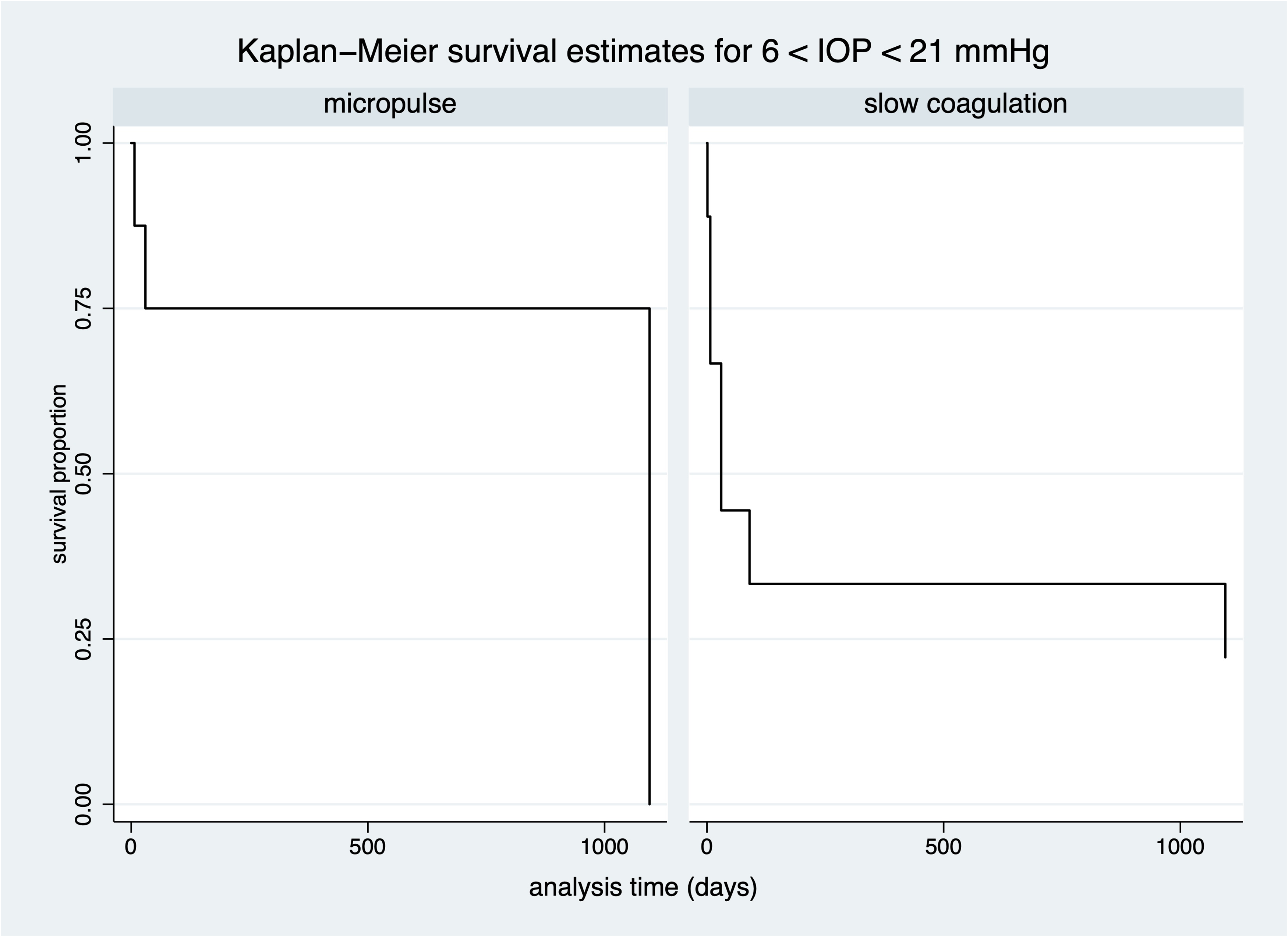
Kaplan–Meier curves representing the probability of treatment success over time. Criterion B: IOP 6–21 mmHg.
Three eyes (42.85%) in the MP-TSCP group required a retreatment session, compared with seven eyes (77.77%) in the SC-TSCP group. The complications reported are described in Table 2. Corneal decompensation occurred in one eye in the MP-TSCP group and two in the SC-TSCP group. One case of vision loss was observed and there was also one case of phthisis, both in the SC-TSCP group.
Discussion
Managing CG presents many challenges. Initial surgical treatments include goniotomy and trabeculotomy. However, in up to 50% of patients with CG, these initial procedures fail such that further surgical intervention is required. 5 Trabeculectomy and valve implants are often the next steps in these patients. However, despite high success rates in adults, the results [of these filtering surgeries] have been less impressive in the younger population. 16 Cyclodestructive procedures are alternative methods to lower IOP in these patients. The use of these procedures to reduce IOP was first described by Beckman et al. and Beckman and Sugar.17,18 Transscleral infrared light is absorbed by pigmented epithelial cells in the ciliary body, which destroys the ciliary body epithelium.
Traditional cyclophotocoagulation is associated with severe complications such as hypotony, progression to vision loss, retinal detachment, and phthisis. 19 Therefore, this treatment is usually reserved for cases with a poor outlook because of the failure of multiple surgeries. MP-TSCP and SC-TSCP lasers were recently introduced for use in cyclodestructive procedures, and showed a superior safety profile and satisfactory efficacy. However, the effects are transient and repeated sessions are thus necessary.20–22
In our study, both MP-TSCP and SC-TSCP were highly effective for lowering IOP. In terms of meeting success criterion A (decrease of > 20% in the preoperative IOP), MP-TSCP and SC-TSCP showed similar performance (75% vs. 77.8%). However, SC-TSCP may be more effective in terms of meeting success criterion B (IOP 6–21 mmHg at the last visit); 50% in MP-TSCP vs. 77.8% in SC-TSCP).
The literature on MP-TSCP and SC-TSCP for childhood glaucoma is limited to a few studies with small sample sizes. Short-term follow-ups are typically seen in studies of traditional cyclophotocoagulation. Kraus et al. reported a 28.6% reduction in IOP using traditional transscleral cyclophotocoagulation for pediatric glaucoma, with a pre-interventional mean IOP of 26.9 mmHg and mean IOP at the last medical record of 18.8 mmHg. 23 The mean IOP was 28.0 mmHg in our MP-TSCP group and 29.9 mmHg in the SC-TSCP group. The mean IOP decreased significantly in the MP-TSCP and SC-TSCP groups, by 38.35% and 50.86%, respectively.
Elhefney et al. reported a 37.5% decrease in the mean IOP, and a decrease in the mean number of eye drops used, at the follow-up visit of children with glaucoma treated with MP-TSCP. 24 In another study, MP-TSCP was effective for lowering the IOP of children with refractory glaucoma, similar to continuous wave transscleral cyclophotocoagulation. The decrease in IOP was 63% in the MP-TSCP group and 67% in the continuous wave transscleral cyclophotocoagulation group. However, the complication rate was lower in the former group, indicating that it is a safer alternative. 14 Aquino et al. concluded that MP-TSCP has similar efficacy to continuous wave transscleral cyclophotocoagulation, but a more predictable effect on IOP and lower incidence of vision-threatening complications. 20
A retrospective study compared traditional transscleral cyclophotocoagulation and SC-TSCP for treating refractory glaucoma and showed an equivalent decrease in the IOP at 12 months postoperatively. The mean decrease in the IOP in the SC-TSCP group after 12 months was 35%. 25 Diode laser cyclophotocoagulation has been utilized in many cases of pediatric glaucoma, but reports suggest that the response in children is poorer than in adults. It has been hypothesized that younger eyes might recover faster from treatment than older ones.25,26 In our study, improvements persisted for over a year, although retreatment sessions were necessary for both groups.
Advantages of SC-TSCP and MP-TSCP include their repeatability and titratability. Some surgeons prefer to increase the duration of laser application over repeat sessions to enhance its efficacy, whereas others prefer to increase the power in eyes with severe hypertension and poor vision. In this study, we applied the lasers for the same duration as in previous protocols, in all retreated eyes.
A retreatment session was required in 42.85% and 77.77% of the MP-TSCP and SC-TSCP cases, respectively, for almost complete IOP control. Refractory pediatric glaucoma treated with continuous wave transscleral cyclophotocoagulation is associated with a high retreatment rate (70%), where failures mainly occur during the first 6 months. Most studies reported using up to three sessions; however, there is no clear consensus on the number of sessions that should be completed.
In a previous MP-TSCP study, the mean number of glaucoma medications decreased significantly from 2.6 ± 0.5 pretreatment to 1.7 ± 0.6 during month 15. 20 The average number of glaucoma medications in our patients who underwent SC-TSCP decreased from 3.9 ± 0.68 to 2.6 ± 1.6 after 12 months in this study. However, despite the decrease in number of post-treatment medications, neither treatment allowed for complete discontinuation of topical medications in any patient.
The main concern with procedures involving ciliary body destruction is the risk of complications such as hypotony, corneal decompensation, choroidal detachment, macular edema, and inflammation. Because of the risk of vision-threatening complications, there is a tendency to apply such procedures only in eyes with impaired vision or a poor prognosis. Severe complications, such as phthisis and blindness, occurred in our study at similar rates to those reported in previous studies. Phthisis has a prevalence of 0–9.9%, and visual acuity decreases by 5–47%.14,27,28 The vision loss may be due to more than just treatment, however; the progression of glaucoma may also play a role. 29 In our study, even though we did not detect a statistical difference between the groups, we observed more serious complications in the SC-TSCP than MP-TSCP group, such as blindness, phthisis, and corneal decompensation. The lack of statistical significance may be due to the small sample size. Moreover, the SC-TSCP group had poorer preoperative visual acuity and more previous surgeries than the MP-TSCP group, which may reflect more advanced disease, a worse prognosis, and higher risk of serious complications. Given the severity and refractory nature of glaucoma, both techniques may be useful, and should not necessarily be reserved only for patients with end-stage disease.
Our study had some limitations. First, because of its retrospective nature, the patients were not randomized to the MP-TSCP and SC-TSCP groups, which may have led to selection bias. The techniques were selected according to their availability at each center, and no specific variable predisposing a surgeon to choose one treatment over another was identified. Second, our study had a small sample size, which may have limited the power of the statistical analysis. The reason for the small sample was that childhood glaucoma (CG) is rare. In our glaucoma subpopulation, axial length was statistically significant higher in SC-TSCP group than in MP-TSCP, and that means cases in SC-TSCP group could be more advanced, what could also influence in success rate and in the increased number of severe complications. Further prospective clinical studies with larger samples are required to address the lack of data regarding the success rates, efficacy, and postoperative complications of these laser procedures in CG patients.
We conclude that both MP-TSCP and SC-TSCP were effective for treating CG but frequently required a repeat session. SC-TSCP was more effective than MP-TSCP in terms of achieving an IOP of 6–21 mmHg. There was a tendency toward more serious complications in the SC-TSCP than MP-TSCP group.
Footnotes
Author contributions
RCSS, HAM, HHAR, TSRN, MB, TAPF, and NVAL wrote the manuscript and reviewed the literature. All authors critically reviewed and approved the final manuscript. No conflicts of interest exist for any of the authors.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics and consent to participate
This research was approved by our Institutional Review Board in 2021 (approval number: 48417221.6.0000.0068). A copy of the written consent form is available for review by the Editor-in-Chief of this journal.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.