
Abstract
Purpose
To assess the clinical outcomes of symblepharon release in patients with ocular surface chemical injury using Gore-Tex as a novel treatment option.
Methods
This was a retrospective analysis of 23 eyes of 22 chemical injury patients done during a period of January 2014 to December 2021 at a tertiary eye care centre in South India. All patients underwent symblepharon lysis along with Gore-Tex application over the sclera with minimum 1 year follow up. The patients were assessed for demographic details, visual acuity, intraocular pressure, anterior and posterior segment details, photographic documentation, preoperative diagnosis, previous surgical details in recurrent cases, surgical procedures, final visual acuity, surgical outcomes, and complications. The clinical outcomes were assessed and outcomes were defined as success, partial success, or failure.
Results
The median age was 17 years (IQR, 12–39 years). Among them 10 eyes with symblepharon had grade 3 length, 12 eyes grade 3 width and 12 eyes had grade 3 loss of palisades of Vogt. The success was achieved in 52.2% of the patients; partial success in 34.8% and 13.3% had failure. The mean duration of recurrence was 6.75 ± 3.6 months. Failure was noted in young patients with mean age 9.75years and with grade 3c symblepharon. There was no sight threatening complications noted.
Conclusion
The study showed very good results with Gore-Tex as a novel treatment option for chemical injury patient with symblepharon formation. It can be easily employed to prevent the symblepharon recurrence of various ocular surface disorders.
Key messages:
Symblepharon and pterygium are known for recurrence after surgical removal.
Many ocular surface procedures exist to reduce the recurrence such as, AMG, Lr-CLAL, CLAG, and SLET- but associated with unpredictable results.
Gore-tex acts as an adjuvant for such ocular surface procedure to reduce the inflammatory and the proliferative phase and thereby recurrence is reduced.
Gore-tex has been used to seal corneal perforations, multirecurrent pterygium cases previously but its role has been clearly defined in our study with long term results.
Introduction
Ocular chemical injury represents 10–22% of all ocular traumas and is the second most common cause of workplace-related eye injuries (12%). 1 Among ocular emergencies, chemical injuries constitute 0.1–15% and comprise 22% of all ocular injuries. Among them, two-thirds are due to alkali burns and one-third are due to acids and alcohol.2,3 The clinical course is classified as immediate phase, acute phase (initial 7 days), early reparative phase (8–20 days), and late reparative phase. Symblepharon, a pathological adhesion between the bulbar and palpebral conjunctiva is the sequel of the late reparative phase of ocular chemical injury. The severity depends on the agent causing chemical injury, duration of contact, extent of limbal ischaemia, and the amount of loss of corneal epithelial stem cells.1,2 In severe cases fibrovascular pannus can grow to cover the ocular surface with the development of sub epithelial fibrosis, superficial and deep scarring, tenons fibrosis and contracture, corneal vascularisation, nerve damage and progressive symblepharon with cicatrising lid deformities. The undesirable effects of symblepharon include eyelid malposition, inadequate blinking, dry eyes, extraocular motility restriction, and cosmetic disfigurement.4,5 Various surgical approaches with tissue substitutes exist to prevent the recurrence of growth after symblepharon lysis such as conjunctival graft, Amniotic membrane graft(AMG), oral mucosa, and nasal mucosa. 6 The adjunctive measures to prevent readhesion include symblepharon rings, silicone sheets, mitomycin C, anchoring sutures, bevacizumab, and beta irradiation.7,8 However, despite all the possible measures, it is difficult to achieve satisfactory results in eyes with fleshy and bulky pterygium (Figure 1(a) and (b)), thick symblepharon, and eyes with recurrent growth, especially in the younger age group. Since the pathogenesis of wound healing of conjunctiva and tenons following excision is unpredictable, and prevention of recurrence is challenging with a high recurrence rate (6.2% to 40%).1,6,7 Kim KW et al. had previously used Gore-Tex as an effective novel adjuvant in eyes with multi-recurrent pterygium with symblepharon to prevent a recurrence. 9 Gore-tex is a synthetic, bio-compatible, expanded polytetrafluoroethylene sheet, previously used in vascular grafts in cardiac surgeries. 9 It resists infection, inflammation and acts as a barrier for fibrous regrowth. We evaluated the clinical outcomes of patients with symblepharon due to chemical injury managed with Gore-tex as a novel adjuvant along with stem cell transplant and AMG to prevent the recurrence of growth, with a long-term follow-up in the south Indian context.
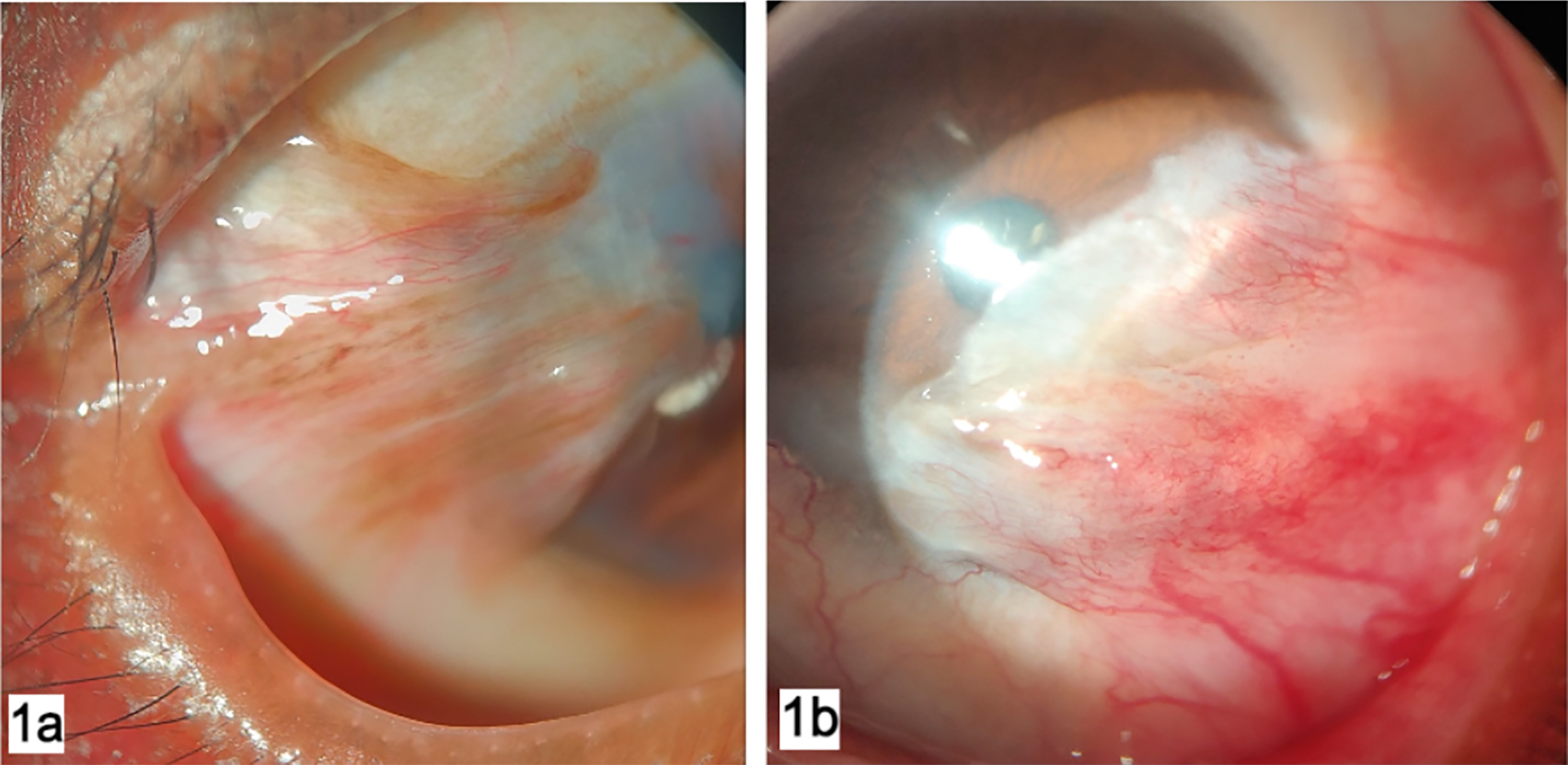
Image showing primary and recurrent pterygium cases grade 3 and 4.
Methodology
Subjects
A retrospective review of data involving 23 eyes of 22 patients from January 2014 to December 2021 was performed in a Tertiary eye care centre in South India, Tamil Nadu. The study approval was obtained from the local Institutional Ethics Committee of Institutional Review (AEH, TVL-IEC/R/CS/2021/001) and adhered to the tenets of the Declaration of Helsinki. All patients who underwent symblepharon release surgery following moderate to severe chemical injury with Gore-tex material, with a minimum follow-up of 12 months, were included in our study. Patients with trauma, glaucoma, previous squint surgeries, refractive surgery, cataract surgery, scleral thinning, viral disease, eyes with acute inflammation, systemic comorbidities, and autoimmune disorders were excluded. Preoperatively, informed consent was obtained from all the patients, and the data were retrieved retrospectively from the medical case records and entered into an Excel sheet. The data were analyzed for demographic details, visual acuity, anterior and posterior segment details, preoperative diagnosis, and previous surgical details in recurrent cases, surgical procedures, final visual acuity, surgical outcomes, and complications, if any. The intraocular pressure (IOP) was recorded with a non-contact Tonopen XL (TPA; Reichter Inc., Depew, New York, USA), or I care (I-Care Finland Oy, Finland). The Ultrasound B scan was performed in all the eyes with extensive Symblepharon and conjunctivalisation, in whom the fundus was not visible.
All the patients underwent detailed slit-lamp evaluation (D-SLN-Topcon-26) and photographic documentation of symblepharon before and after the surgical procedure (image taken with a Topcon DC3 model camera). Symblepharon was graded based on the length, width, and loss of palisades of Vogt in the ocular surface based on standard photographs of symblepharon as per a previous study done by Kheirkhah et al., 10 and the surgical intervention was planned subsequently (Table 1).
Depicts grading of symblepharon based on length, width and loss of palisades of Vogt. 10
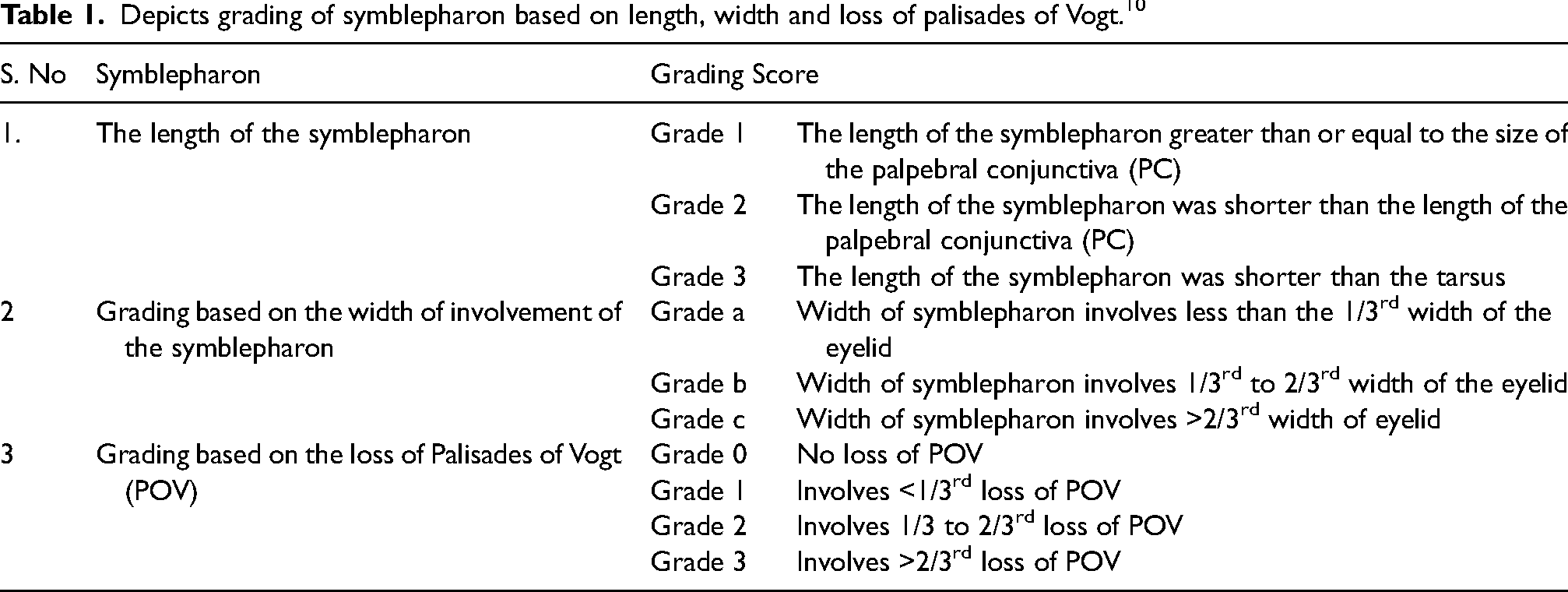
Grading based on the Length of the Symblepharon: Grade 1: The length of the Symblepharon was equal to or > than the size of the palpebral conjunctiva (PC), Grade 2: the length of the Symblepharon was shorter than the length of the PC, Grade 3: the length of the Symblepharon was shorter than the tarsus.
Grading based on the width of involvement of the Symblepharon: Grade a: width of Symblepharon involves < the 1/3rd width of the eyelid, Grade b: width of Symblepharon involves 1/3 to 2/3rd width of the eyelid, Grade c: width of the Symblepharon involves >2/3rd width of the eyelid.
Grading based on the loss of Palisades of Vogt (POV): Grade 0: no loss of POV, Grade 1: involves < 1/3rd loss of POV, Grade 2; involves 1/3 to 2/3rd loss of POV, Grade 3; involves >2/3rd loss of POV. All the surgeries were performed by a single experienced surgeon (AV) with a minimum of 10 years of experience. The procedure was performed under general anaesthesia for patients under 20 years of age after obtaining systemic fitness and in peribulbar anaesthesia for the rest.
Outcomes
The study aimed to evaluate the clinical outcomes of Gore-tex as an adjuvant along with limbal cell replacement procedures for the prevention of recurrence of symblepharon after its lysis surgery—primary outcomes in terms of success, partial success, and failure and secondary outcomes such as the demographic data, visual acuity, complications, and safety were assessed.
Surgical technique
Preparation of Gore-Tex
Multi-microporous e-PTFE (GORE PRECLUDE Pericardial membrane, Gore, Flagstaff, Arizona, USA) was obtained from Novo med Incorporation Pvt Ltd, Mumbai, and Maharashtra. It is available as a white 0.1mm thick, flexible membranous sheet that can be cut to the desired size to fit the defect area. Before the procedure, the sheet was made microporous with the 26 G needle to allow oxygen diffusion to the surgical wound, preventing hypoxia-induced scar formation during the proliferative phase of wound healing. Before placing the Gore-tex, AMG was secured over the bare sclera with fibrin glue (Tisseel Lyo, Fibrin Sealant, Baxter AG, Austria) Figure 2(b) and (c). Next, Gore-tex was placed over it, sutured over the episclera with 10-0 nylon, then covered with AMG with 10-0 vicryl sutures, and anchored to the episclera.
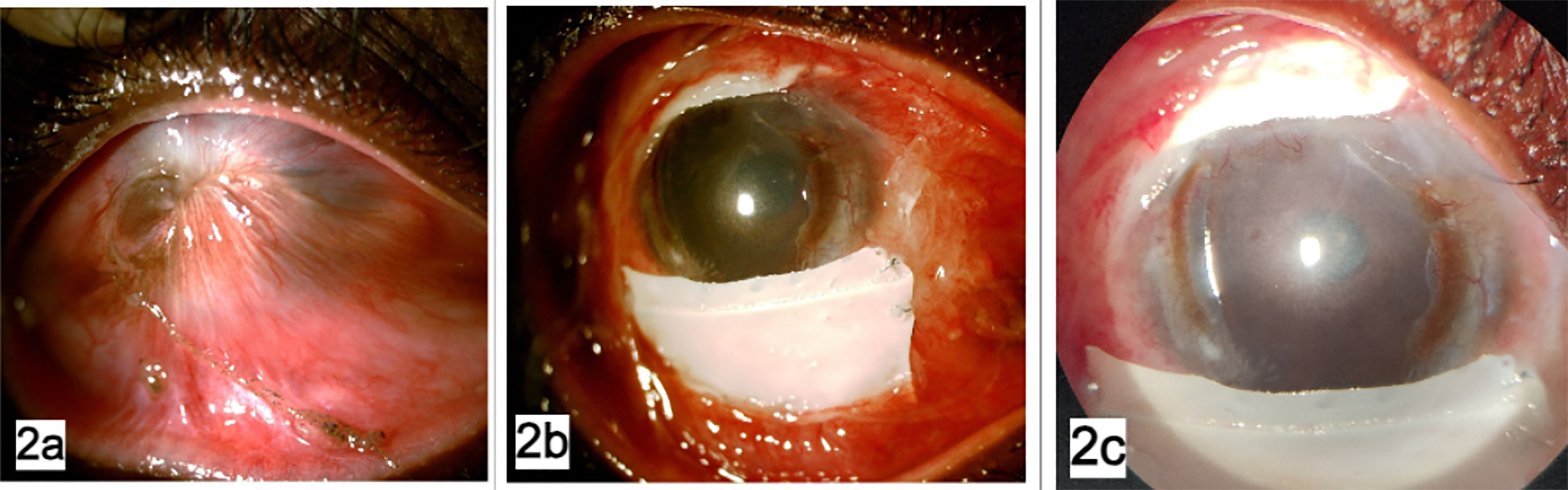
(a) Image showing total symblepharon following chemical injury, (b) image showing immediate postoperative period of symblepharon release and Gore-tex with AMG done, (c) image of five weeks postoperative period of Gore-tex in the same patient.
Altered methods of surgical techniques were chosen, depending upon the length, width, and loss of palisades of Vogt.
For eyes with grade 1 length of the Symblepharon: Resection of the growth was done away from the fornix, and the fibrotic tissue was dissected and cut to expose the underlying sclera. Nasally, careful dissection was done to prevent iatrogenic injury to the medial rectus in eyes with nasal growth. AMG was placed on the exposed bare sclera with the basement membrane (BM) side up, anchoring 10-0 vicryl sutures. A 4 × 2 mm conjunctival limbal tissue from the fellow eye (CLAG) or the same eye was harvested and placed circumferentially along the limbus with fibrin glue. In both conditions, multi-micro porous Gore-Tex is placed over the AMG in the bulbar surface, separating the raw surface of the palpebral and tarsal conjunctiva. If needed, fornix-forming sutures with 4-0 silk were placed to reconstruct the fornix.
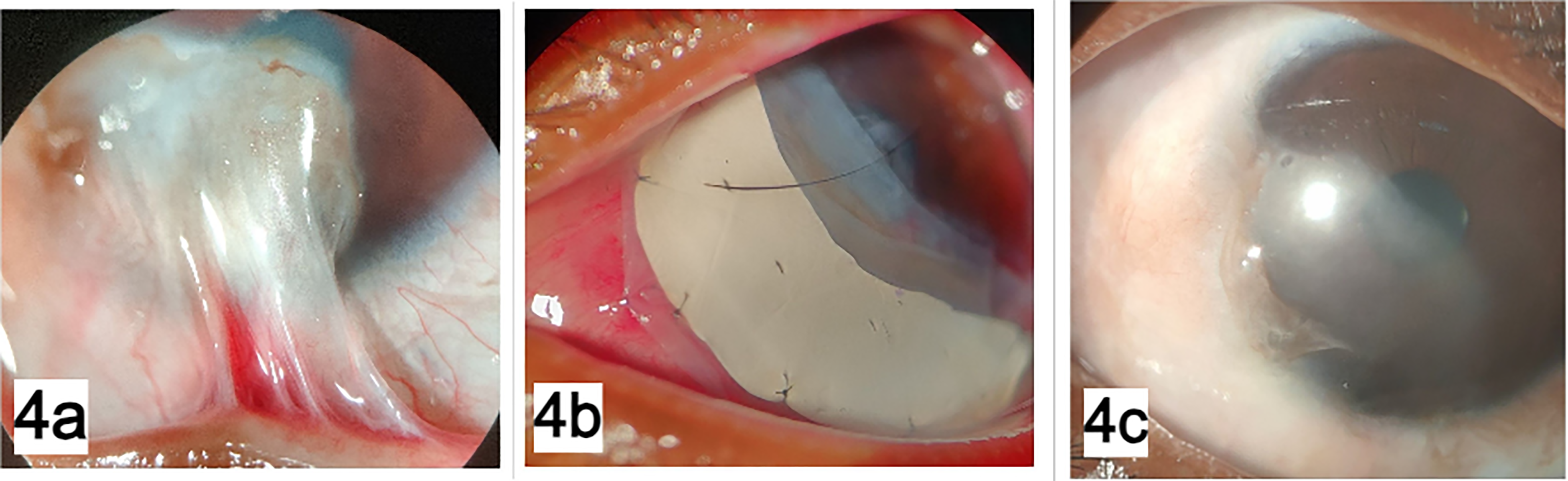
For grade 2 & 3 lengths of Symblepharon: A 360-degree complete peritomy was done. First, Symblepharon was released away from the fornices, and the fibrotic tissue was extensively dissected away from the corneal surface and underlying tenons on the scleral surface. Further, the surgical defect over the sclera was covered with Gore-tex sandwiched between two layers of AMG. If the surgical defect involves the entire surface, Gore-tex was placed over the superior and inferior bulbar conjunctiva, where the chance of recurrences is high due to the apposition of the lids over the ocular surface (Figures 1(a), 2(a), 3(a), and 4(a)). For the limbal stem cell deficiency (LSCD), a small 2 × 2mm biopsy of limbal stem cells from the superior limbus was harvested from the fellow eye or the living-related donor and cut into small pieces. These were placed with the epithelial side up over the AMG, secured with fibrin glue, and covered with another layer of AMG or Lr-CLAL obtained from the healthy donor and placed along the limbus (Figure 3(a)–(c)).
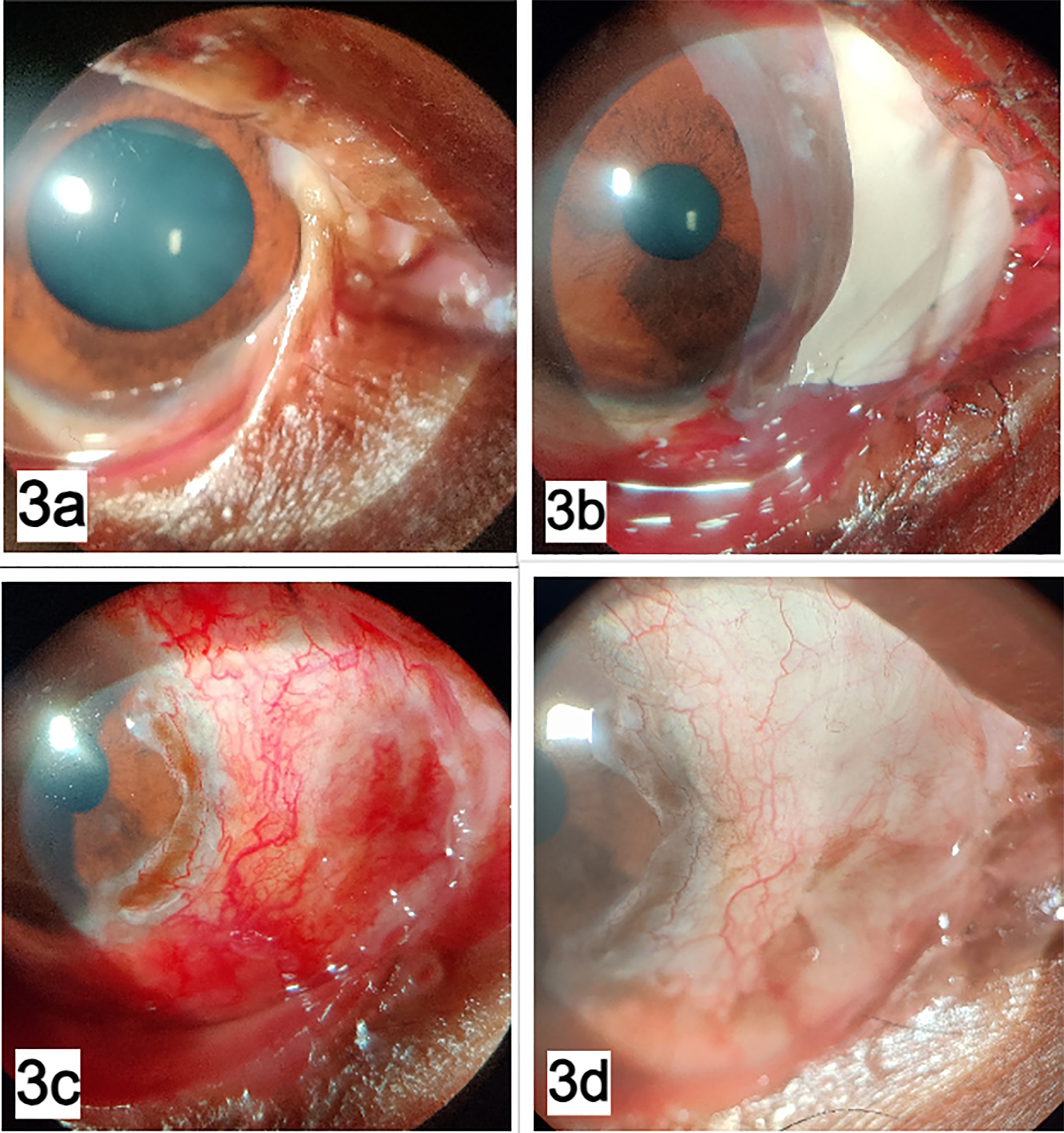
(a) Symblepharon involving 180 degree of the limbus following chemical injury, (b) shows postoperative image of same patient after symblepharon release and Gore-tex, AMG, (c) postoperative image taken after Gore-tex removal, (d) postoperative image showing well epithelised surface after 10 weeks of follow-up.
(a) Image of a patient with recurrent pterygium associated with symblepharon, (b) showing postoperative image after excision of pterygium and Gore-tex, (c) shows 6 months postoperative image.
Postoperative management and follow-up
Postoperatively, topical 0.5% Gatifloxacin and 0.1% Dexamethasone combination eye drop were given in a tapering dose starting from six times a day for three months along with oral steroids (Tab prednisolone dispersible 1 mg/kg body weight) under strict blood glucose monitoring. Adjuvant topical medications such as topical carboxymethylcellulose 1% eye drops and a tablet of vitamin C 500 mg once daily were given for 30 days. The capsule Doxycycline 100 mg was twice daily for fifteen days and then tapered to once daily for another 15 days. All patients were admitted for three days. During the fourth week, a loose Gore-Tex sheet was removed in the slit-lamp under aseptic precautions with sterile forceps and cornea scissors under topical anaesthesia with 0.5% proparacaine drops. The topical treatment was continued as per schedule.
Success was defined as complete epithelialization of the ocular surface and formation of the fornix. Partial success was defined as epithelisation of the ocular surface with mild conjunctival recurrence of symblepharon and pterygium. Failure was defined as persistent inflammation or the severe recurrence with fast progression of the fornix shortening. All the patients underwent visual acuity testing (Snellen's chart), slit-lamp examination for the anterior segment, posterior segment, and IOP at every visit. The patients were followed up at one week, two weeks, one month, three months, six months, and after four monthly follow-ups for a minimum of one year. The conjunctival and corneal recurrence of the growth was assessed at every visit, and documented drawings were in the case sheet. The patients with only conjunctival recurrence were considered mild, growth reaching the limbus was deemed moderate and corneal recurrence was considered severe.
Statistical analysis
Descriptive statistics were used to report the demographic and clinical findings of the study subjects. The frequencies with percentages were used for qualitative data, and the median with interquartile range (IQR) was used to report the quantitative variables. The association between the categorical variables was assessed using Fisher's exact test. And for continuous variables, the group difference was analyzed using the Wilcoxon rank-sum test. Snellen's equivalent visual acuity was converted and presented in log MAR (logarithm of minimal angle of resolution). The postoperative comparison of visual acuity was made using the Wilcoxon sign rank test. ANOVA test was used to compare the age between the study outcomes. Statistical significance was assessed at the two-sided level of a p-value less than 0.05. The statistical analysis was performed using STATA, version 14.0 software (Stata Corp, Texas, and USA).
Results
A total of 23 eyes from 22 patients were included in the study. The median age of overall study subjects was 17.0(IQR, 12–39) years; among them, 16 (72.7%) were males and 6(27.3%) were female patients (M: F ratio of 8:3). The median follow-up was 36.0(IQR, 12 to 96) months, with the median time interval between the onset of symptoms and first presentation in months being 9.0(1 to 48) months. The demographic data are shown in Table 2.
Demographic details of the patients during the study period.
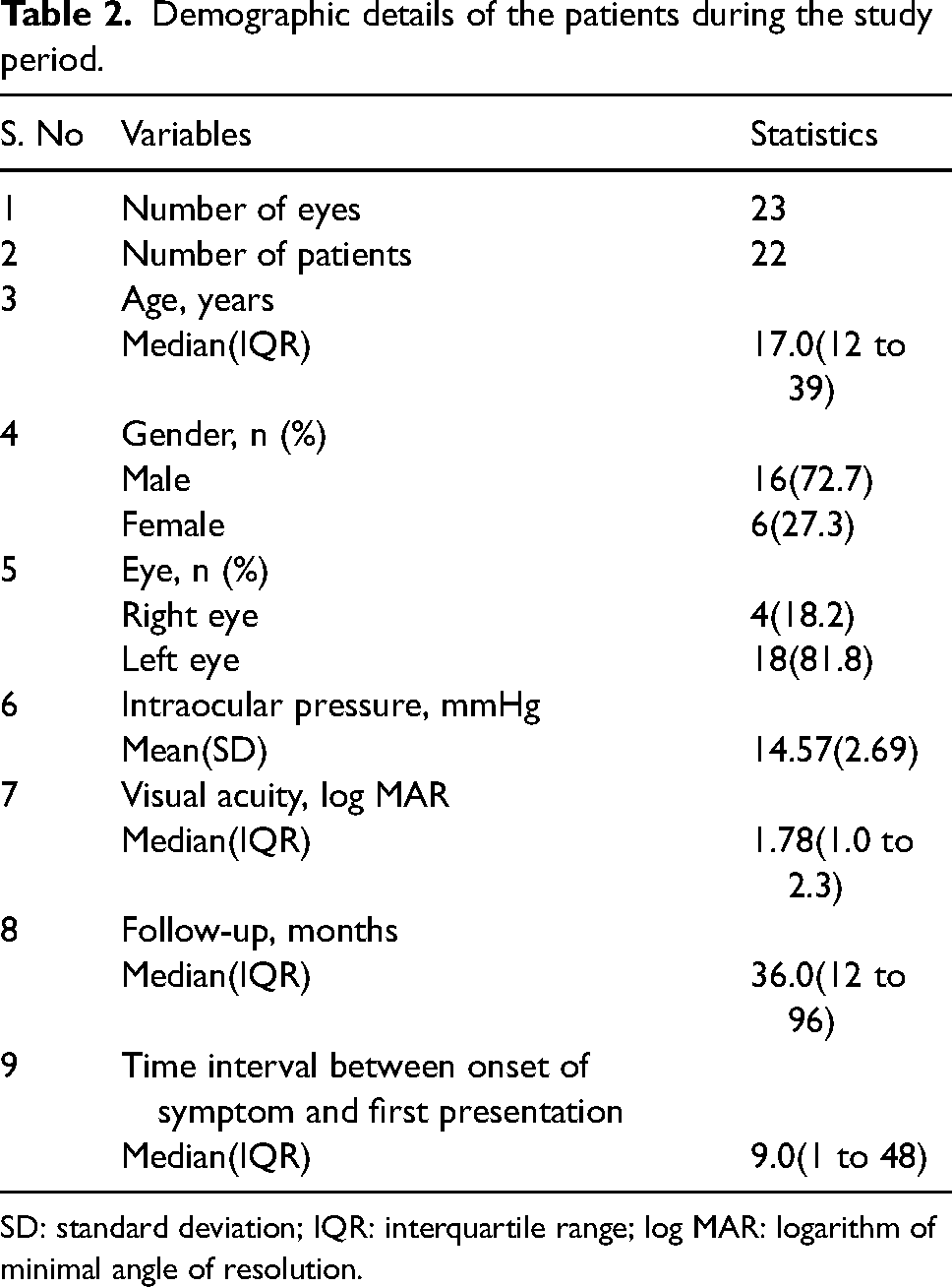
SD: standard deviation; IQR: interquartile range; log MAR: logarithm of minimal angle of resolution.
Symblepharon grading
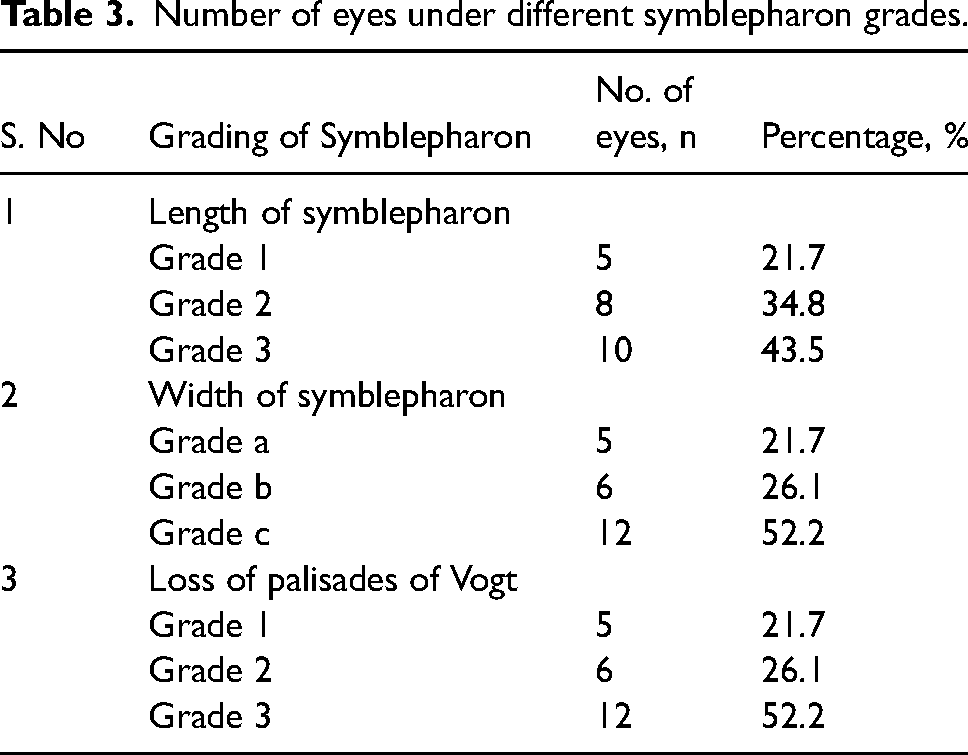
Based on the length of the symblepharon, 5 eyes (21.7%) had lengths equal to or more than the length of the palpebral conjunctiva (grade 1), 8 eyes (34.8%) had lengths shorter than that of the palpebral conjunctiva (Grade 2), and 10 eyes (43.5%) were having a length shorter than the tarsus (Grade 3). The width of the symblepharon was also graded depending on the involvement of the tarsus, 5 eyes (21.7%) was noted to have a symblepharon width less than 1/3rd width of the eyelid width (Grade a), 6 eyes (26.1%) had a width of symblepharon involving 1/3rd to 2/3rd of the eyelid width (Grade b), and 12 eyes (52.2%) had the width of the symblepharon affecting more than 2/3rd width of the eyelid width (Grade c). Based on the extent of loss of palisades of Vogt (POV), symblepharon was graded from 0 to 3, 5 eyes (21.7%) were noted (Grade 1), which had less than 1/3rd loss of POV, six eyes (26.1%) were reported to have 1/3rd to 2/3rd loss of POV (Grade 2) and 12 eyes (52.2%) were having more than 2/3rd loss of POV (Grade 3) (Table 3).
Number of eyes under different symblepharon grades.
The mean duration of epithelisation was 5.27 ± 0.74 weeks. The surgery's success depended on the age, length, width, and loss of POV. Complete success was achieved in 12 eyes(52.2%), 8 eyes (34.8%) had the partial success that is only conjunctival recurrence without forniceal shortening and corneal recurrence, and three eyes (13.0%) had a failure with rapid recurrence of conjunctival recurrence and forniceal shortening. The mean duration of recurrence was 6.75 ± 3.6 months. Failure was noted in cases with grade 3c symblepharon with a severe fibrotic response. The mean age of the eyes which achieved complete success is 23.83 (±7.2) years (Figures 3 and 4), which includes five eyes from grade 1, a; 6 eyes from grade 2, b; and one eye from grade 3, c symblepharon. Partial success with conjunctival recurrence was noted in eyes with grade 3, c symblepharon with mean age of 22.25 (±8.0) years and in patients with a mean age of 9.67 (±2.5) years had both recurrence of both conjunctival and corneal symblepharon in all 3 eyes were with severe grade 3, c symblepharon (Table 4).
Comparison of age with study outcomes.
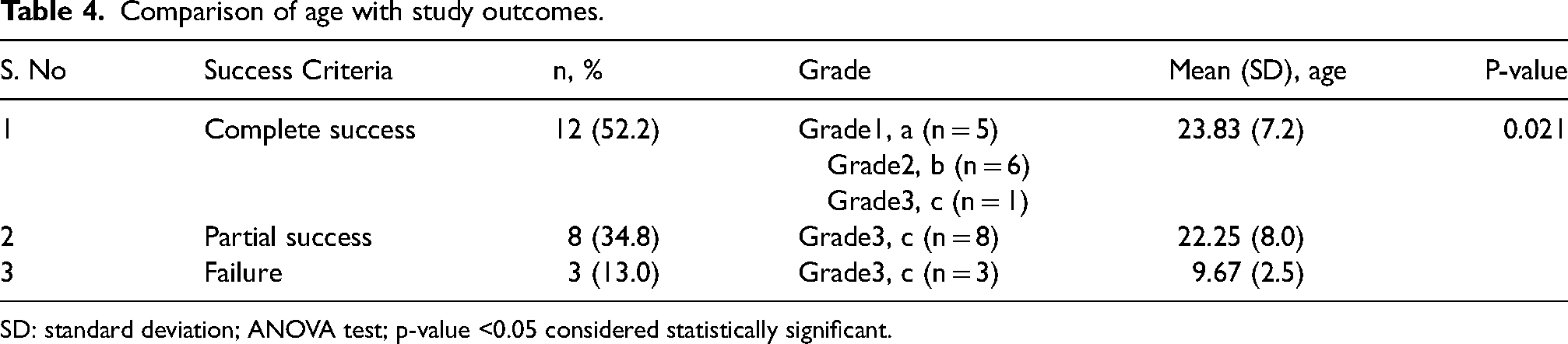
SD: standard deviation; ANOVA test; p-value <0.05 considered statistically significant.
Patients with a mean age of 9.67 (±2.5) years were likely to fail even if adequate attention was given to the limbal stem cell regeneration and the barrier effects (p = 0.021). The patients with eyes that had conjunctival recurrence were observed, except for two eyes with grade 2 length and grade b width and grade 3 POV, with progressive conjunctival recurrence of fibrotic growth encroaching on the cornea. Hence repeat procedure was attempted with Lr-CLAL and Gore-tex/AMG. Postoperatively, at four months, mild conjunctival recurrence was noted. In eyes with grade 3 lengths, grade c width, and grade 3 loss of POV, all three eyes had a severe recurrence, and repeat the procedure with SLET from Living related donor and AMG/Gore-tex was attempted. All three eyes had recurrence within three months of surgery. The reasons might be the presence of preoperative inflammation, which was not satisfactorily controlled, the younger age of the patients with the severe fibrotic response, and the severity of the symblepharon. In a 12-year-old child, Gore-tex was repeated at the interval of 12 months, but a complete failure was noted within two months. For a two-year-old male child with less than grade 2/b symblepharon, repeat Gore-tex was done at the interval of 6 months, and partial success was achieved with the stable ocular surface at two years follow-ups.
All the eyes had a stable epithelized ocular surface; no sight-threatening complications were noted in the study patients. Pyogenic granuloma was noted in 6 eyes (27.2%) of patients, for which granuloma excision with intralesional 0.1ml of 0.1% Dexamethasone injection was given; spontaneous extrusion of Gore-tex was noted in 3 eyes, all happened after four weeks of surgery. Hence it did not need repeat procedures. Fungal infection was reported in one eye (4%) over the surface of the infection that did not affect Gore-tex; the underlying sclera; topical Fluconazole (1%) eye drops were given six times a day for two weeks. The use of Gore-tex was relatively safe, even in children. The average preoperative best-corrected visual acuity (BCVA) was 1.78 log MAR units, and the postoperative BCVA was 0.48 log MAR, which was statistically significant (p-value = 0.016, Figure 5).
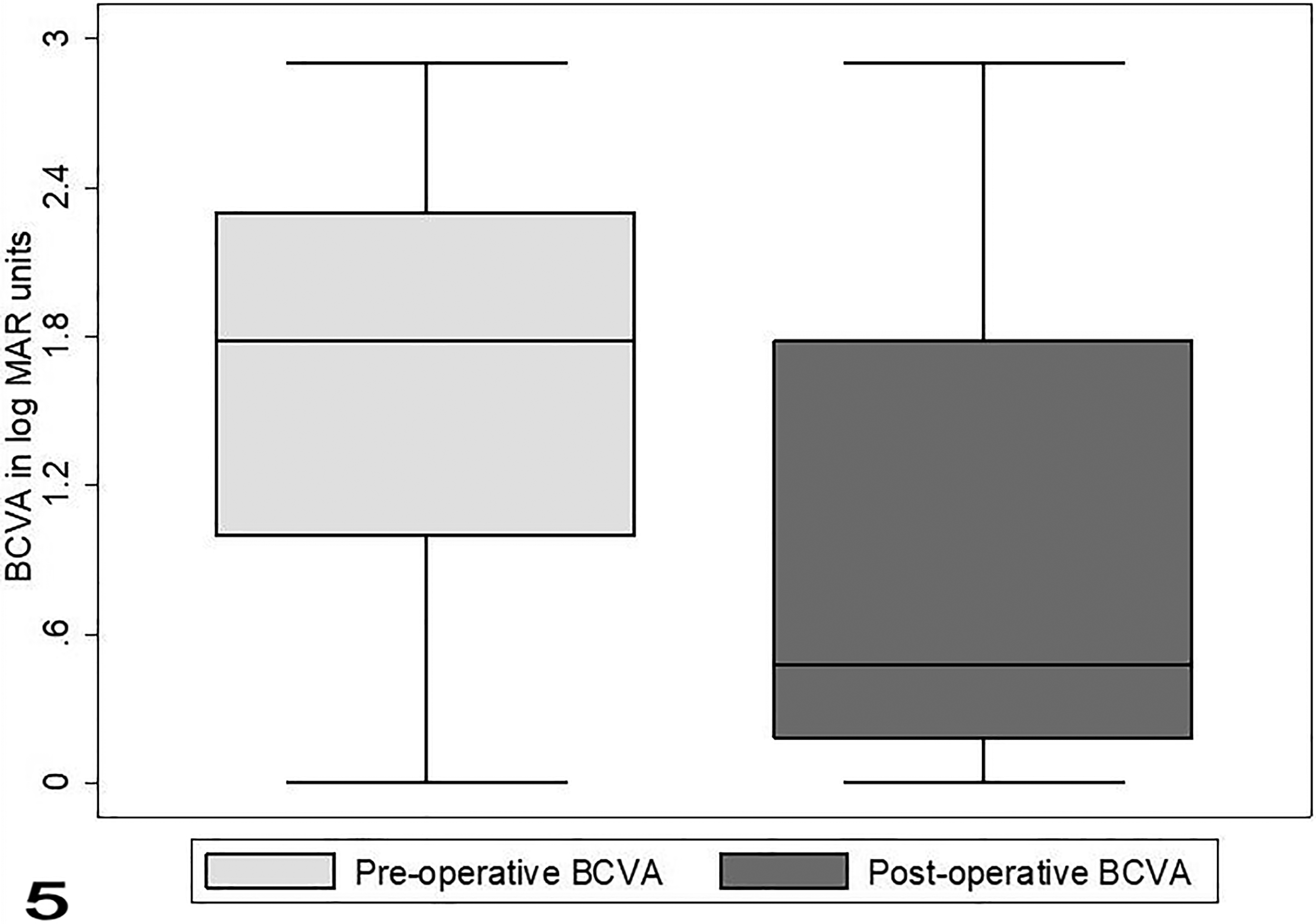
Boxplot showing change in best corrected visual acuity (BCVA) in log MAR units. The box indicates upper and lower quartile values (25th and 75th percentile), whereas the ends of whiskers extend to 1.5 times the interquartile range. The solid line within the boxes represents the median log MAR value (50th percentile).
Discussion
In ophthalmology, the use of Gore-tex was initiated in 1989 by Tawakol et al. 11 Furthermore, in 1990 by Whitmore et al., scleral grafts in rabbits, 12 the experience was limited in humans. In 1991, Legeais et al. initiated the use of Gore-Tex successfully in human eyes to temporarily cover the corneal perforations in 6 eyes until a corneal transplant was done. 13 In 1994, Huang et al. used it in 3 eyes of patients with Mooren's ulcer and Necrotising scleritis as a patch graft. 14 In 2002, Amm M et al. used a Gore-Tex patch for immunological corneal melts in 6 eyes due to Rheumatoid arthritis and found it effective. 15 Rufer F et al. conducted a study with a more extensive case series and longer follow-up of patients with multi-layered Gore-tex for non-infectious corneal defects in 38 eyes. 16 About 5.1 to 50 lakh population are being affected every year worldwide by chemical injuries. 3 The prognosis depends upon the severity of the burns and their impact on the ocular surface. The long-term sequelae include limbal stem cell loss, symblepharon, corneal stromal haze, pseudo pterygium, and persistent epithelial defects leading to permanent vision loss.1–3 Management of symblepharon and LSCD is quite challenging, immediate surgical intervention with AMG following chemical injury in addition to conventional medical therapy reduces the incidence of symblepharon. In our study, only 5 patients (22.7%) had undergone initial AMG before the presentation. Conjunctival wound healing is divided into four stages: 1) Inflammatory phase (1–2 weeks), 2) Proliferative phase (2–4 weeks), 3) reparative phase (after 4 weeks up to 12 weeks), and final remodelling phase. The persistent uncontrolled inflammation and the LSCD cause the growth of sub-epithelial fibrosis, causing adherence of conjunctiva and tenon's capsule leading to recurrence of symblepharon after its excision. 5 Ayse Burcu et al. studied the management of LSCD secondary to more than grade 2 chemical burns, with medical therapy, AMG, and limbal graft transplantation, and subsequent keratoplasty if needed. Success with clear cornea was achieved only in low-grade chemical injuries grade 2(78.6%) compared to grade 3(60%). Hence, the prognosis is guarded for severe chemical burns even with LSCT.17,18 David H K et al., compared AMG alone and AMG with MMC to prevent recurrence after recurrent pterygium excision and observed no additional benefits with MMC to AMG. 19 We have managed every insult that occurred to the ocular surface due to chemical injury. We ensured the adequate release of the fibrous tissue and replaced limbal stem cells, covered the OS with AMG to hasten the epithelial integrity, and finally used Gore-tex as a novel adjuvant, which acts as a mechanical barrier for the recurrent invasion of the fibrous tissue. The authors have also suggested that prognosis in the case of prevention of pterygium recurrence depends upon the age, fleshiness, and morphology of the pterygium.18–20 In a study by Solomon et al., 17 eyes with symblepharon due to various reasons such as OCP, Pterygium, chemical injury, strabismus surgery, SJS & TEN, chronic allergic conjunctivitis undergone AMG for conjunctival fornices in 17 eyes with symblepharon, 70.6% (12 eyes) had success and eyes with symblepharon due to autoimmune and chemical burns observed failure of the procedure with recurrence of the growth. 21 Similarly, Tseng et al. also observed a low success rate in chemical burns with AMG and MMC. Hence, the prognosis of symblepharon due to chemical injury is considered poor compared to all other Aetiologies. 22 To prevent the recurrence, a few synthetic materials 12 have been tried such as Ologen, and e-PTFE in pterygium surgery but not in symblepharon procedures.9,23 Ologen is a spacer separating the subconjunctival tissue and the episclera, thereby preventing fibrosis and the recurrence of pterygium. 23 E-PTFE (Gore-Tex) has good tensile strength, is chemically and biologically inert, non-antigenic, easily cut, moulded, and sutured, and is resistant to infection. In 2013, Kim KW et al., for the first time, used Gore-tex in ocular surface procedures and compared two groups of patients with multi-recurrent pterygium with and without Gore-tex in a total of 62 eyes. He observed that postoperative recurrence of Symblepharon, motility restriction, and conjunctival hyperaemia was less in the Gore-tex group. 9 We have used Gore-tex for severe cases of symblepharon in patients with a mean age of 17 years, complete success was noted in 52.1% of eyes because more than 10 eyes had severe loss of limbal stem cells and had grade 3 symblepharon. Age, loss of palisades, and morphology of symblepharon were the factors influencing the success of our procedure. Since Gore-Tex is an inert material, it acts as a mechanical barrier when kept between the conjunctiva and sclera during the proliferative phase of conjunctival wound healing and acts as a successful adjuvant for the prevention of symblepharon. Kwon and Kim et al. used CLAG alone for 116 eyes with moderate to severe pterygium and observed 12.1% recurrence. 9 Malhotra et al. used AMT alone in 20 eyes with grade 4 symblepharon, which 30% failed. 24 The advantage of this material is that it can be cut into any shape and size, punched with trephines to get the desired shape, and placed anywhere in the bulbar surface and the fornix without difficulty can be easily removed. A 12-year-old child underwent a safe, repeat Gore-tex procedure at the interval of 12 months each but failed even after the second Gore-tex. CLAG/CLAL/Lr-CLAL is used to repopulate the limbal stem cells and acts as an effective limbal barrier preventing the regrowth of conjunctiva over the cornea. Similar to the observation by Huang et al. in his case series, we also had a fungal infection over the Gore-tex in one eye, but in contrast, the infection did not involve the ocular surface or the vitreous. 14 Kim et al. evaluated 62 eyes of 62 patients with recurrent pterygium associated with Symblepharon following AMT, CLAG, MMC 0.33%, divided and compared two groups with (30 eyes) and without Gore-tex (32 eyes). The mean follow-up was 17.2+/-2.3 months. Only 3.3% of the Gore-tex group developed corneal recurrence compared to 25% of the non-Gore-tex group. Even though corneal recurrence occurred in one patient, the growth was stable and limited during the maximal follow-up period. 9 The failure rate was 3.5% even though low, conjunctival recurrence was noted in 34.7% of cases. The recurrence was noted in the young age of our patients and severe limbal stem cell deficiency; associated with extreme fibroblastic response, wound contraction, and angiogenic sprouting. Though we have managed moderate to severe grade chemical injury successfully by preventing symblepharon with Gore-tex as a one-step procedure, we had several limitations, retrospective analysis, small sample size, several steps of surgical technique, the need for suturing, and longer surgical time, which may be inconvenient to some surgeons. In addition, the whitish appearance of the material is of cosmetic concern in a few patients. This is the first series of cases with experience in the usage of Gore-tex to prevent the recurrence of symblepharon in literature with long-term follow-up. Gore-tex seems to be a vital adjunctive treatment option, commercially available for preventing the recurrence of pterygium and symblepharon in advanced cases. It has proven safe in young individuals without sight-threatening complications and can be used in first-line surgery at risk of recurrence. In the future, it can act as a novel surgical option to prevent the recurrence of various ocular surface disorders.
Footnotes
Data availability
Data and material are available with the corresponding author and can be provided on request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Consent
Consent was obtained from all the patients before the surgical procedure.
Ethics
Ethics Committee approval obtained and submitted with the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.