
Abstract
Aim
There have been a number of clinical trials in glaucoma research published in the past two decades. Most of these trials were designed to evaluate very specific issues in selected populations placing them in the explanatory end of the pragmatic-explanatory continuum. The purpose of this study was to assess the level of pragmatism of published randomized controlled trials in glaucoma.
Methods
A PubMed search using ‘glaucoma’ from 1995 to 2022 and randomized controlled trial (RCT) article type was done. Each study was assessed by three independent examiners using the Pragmatic-Explanatory Continuum Indicator Summary version 2 (PRECIS-2) toolkit. Scores were calculated for each study to determine the level of pragmatism. A summed score ≥36 was indicative of a very pragmatic study.
Results
Thirty-two different articles were included in the analysis. These papers represented 13 different landmark trials. The median PRECIS-2 score was 32 (range, 25 for the Early Manifest Glaucoma Trial (EMGT) to 34 to the Collaborative Normal Tension Glaucoma Study (CNTGS) and the Ocular Hypertension Treatment Study). The Treatment of Advanced Glaucoma Study (TAGS), was considered very pragmatic and scored 33 points.
Conclusion
Despite the number of RCTs in glaucoma, there is still a need for more pragmatic studies.
Keywords
Introduction
Randomized controlled trials (RCTs) provide clear results to help healthcare providers in decision making and to deliver evidence-based treatment towards patients as well as help policy-makers and regulators plan clinical care on a population level. Glaucoma research ranks second in the number of published randomized controlled trials in all of ophthalmology. 1 These RCTs have helped to promote an evidence-based approach to glaucoma management shaping the care to its current status. 2
Most of RCTs in glaucoma research test interventions in selected patient populations under explicitly protocol-defined settings. These explanatory trials are designed to optimize conditions to test the safety and efficacy of specific interventions. Nevertheless, strict inclusion criteria for eligibility of participants limit the external validity or generalizability of the study results in wider clinical settings.
The concept of pragmatism for RCTs was introduced more than 50 years ago. 3 Pragmatic trials aim to provide information on the relative merits of real-world clinical alternatives in routine care. Besides, a pragmatic RCT focuses on maximizing generalizability of the results to many real-world settings, at the same time it tries to preserve as much internal validity as possible. 4 It is currently accepted that explanatory and pragmatism are the extremes of a continuum in the sense that many RCTs have both explanatory and pragmatic features. 5
Pragmatic trials are particularly important in glaucoma. Intraocular pressure (IOP) is the only modifiable risk factor and new therapeutic interventions are continuously being developed. Pragmatic RCTs are useful to reveal the effectiveness of therapeutic interventions in ‘real-world’ conditions and to elucidate barriers to their implementation. Hence, the purpose of this study was to assess the level of pragmatism of published RCTs on glaucoma to ascertain the general need for increased pragmatism in glaucoma research.
Methods
The institution ethics committee waived the need for approval given the nature of the study—not involving human beings. This was neither a systematic review nor a meta-analysis study so that PRISMA reporting guidelines were not followed. A PubMed search using ‘glaucoma’ as keyword and choosing only RCT as article type written in English, published from 1995 to 2022, was done to identify all possibly eligible studies. One of the authors conducted the title, abstract and full text screening and a second check was conducted by another researcher. Disagreements between the two researchers during full text screening were reviewed by a third researcher, and a consensus on inclusion reached following discussion. Only RCTs comparing treatment with observational groups, two different forms of treatments, either medical or surgical therapy or comparing two surgical techniques considered to have relevance and great impact in clinical practice were chosen for analysis. Some articles reporting secondary outcomes from larger landmark RCTs were not included but only one reporting the baseline data, a second reporting the initial results, and third article reporting long-term results were selected. These articles were merged according to each respective landmark trial and evaluated as pragmatic or explanatory using the Pragmatic-Explanatory Continuum Indicator Summary, version 2 (PRECIS-2) by three independent examiners.
The PRECIS-2 is a tool to help researchers make design decisions consistent with the intended purpose of their trial. 5 The instrument has nine domains: eligibility criteria (who is selected to participate in the trial), recruitment (how are participants recruited into the trial), setting (where is the trial being done), organization (what expertise and resources are needed to deliver the intervention), flexibility delivery (how should the intervention be delivered), flexibility adherence (what measures are in place to make sure participants adhere to the intervention), follow-up (how closely are participants followed), primary outcome (how relevant it is to participants), and primary analysis (to what extent are all data included). The scoring system is based on a 5-point Likert scale. For each domain, the score can range from 1 (very explanatory) to 5 (very pragmatic) in order to facilitate domain discussion and consensus. Scores are input in the PRECIS-2 website (http://www.precis-2.org/) where a ‘wheel’ can visually represent how explanatory or pragmatic a trial is on the pragmatic to explanatory continuum. Trials that take an explanatory approach produce wheels nearer the hub whereas those with a pragmatic approach are closer to the rim. Although initially developed to focus on RCT design choices, it has been used in systematic review and meta-analysis of published trials also.6,7
For each domain, the score given in agreement by at least two independent examiners was used as the defined value. The examiners were young ophthalmologists currently enrolled in a glaucoma fellowship program. In the case of no agreement by at least two examiners, a 4th independent examiner (a senior glaucoma clinician-scientist), serving as tiebreaker, evaluated that particular item and defined the final score. Whenever an information was not clearly stated in the article, a score 3 (equally pragmatic/explanatory) was given for that specific domain. Different from the PRECIS-2, scores data for each domain were not plotted to create a wheel; instead, they were summed to have a total score. This was done in order to have an actual figure for quantitative comparison. Lower scores were indicative of more explanatory study (9 as the lowest score possible) whereas higher scores were indicative of a high level of pragmatism (45 was the highest score possible).
Passably, the scores of all 9 domains of a pragmatic RCT should be on or close to the pragmatic extreme (scores ≥4), in order for a trial to be labeled as pragmatic. 4 Hence, in this study, a summed score ≥36 was indicative of a very pragmatic study. However, it has been suggested that trials with scores ≥4 in 4–5 domains could be labeled as such provided the scores of the remaining domains are 3. 4
The proportion of variance of the scores due to between-rater variability was estimated using intraclass correlation. An intraclass correlation coefficient (ICC) above 0.90 was considered indicative of excellent conformity among examiners; between 0.75 and 0.90 good; between 0.50 and 0.75 moderate; and below 0.50 it was considered poor. 8
Results
The PubMed search retrieved 2,296 documents. After review of the articles, 32 articles were chosen for relevance and impact in clinical practice and included in the analysis. Many of the articles were sliced reports belonging to the same RCT and were analyzed as parts of 13 landmark glaucoma trials identified as follow: Advanced Glaucoma Intervention Study (AGIS), Collaborative Normal Tension Glaucoma Study (CNTGS), Collaborative Initial Glaucoma Treatment Study (CIGTS), Early Manifest Glaucoma Trial (EMGT), Ocular Hypertension Glaucoma Study (OTHS), European Glaucoma Prevention Study (EGPS), Tube Versus Trabeculectomy Study (TVT), Ahmed Versus Baerveldt Study (AVB), Effectiveness of early lens extraction for the treatment of primary angle-closure glaucoma (EAGLE), Laser in Glaucoma and Ocular Hypertension Trial (LiGHT), Primary Tube Versus Trabeculectomy (PTVT), Zhongshan Angle Closure Prevention Trial (ZAP), and Treatment of Advanced Glaucoma Study (TAGS).9–40
Five studies compared treatment – either medical or surgical – with observational groups (CNTGS, EMGT, OTHS, EGPS, and ZAP).11–13,16–22,30,39 Four trials compared two different surgical techniques (TVT, AVB, EAGLE, and PTVT).23–30,34–36 Other three studies compared medical therapy versus surgical – either laser or incisional – intervention (CIGTS, LiGHT, and TAGS).14,15,31–33,37,38 One last study (AGIS) evaluated the longterm outcomes of sequences of interventions involving trabeculectomy and argon laser trabeculoplasty in eyes that had failed initial medical treatment for glaucoma.9,10
Table 1 displays the PRECIS-2 scores for each landmark clinical trial. No study reached the minimum score to be label as very pragmatic. The median score was 32, ranging from 24 (EMGT) to 34 (CNTGS and OHTS). The TAGS, self-labeled as a pragmatic trial scored 33 points; even though, it was considered very pragmatic because it scored 4/5 in five domains and 3 in the other four domains. The ICC for agreement among raters was good for most studies except for the EMTG (0.136), OHTS (0.296), TAGS (0.459), and PTVT (0.563).
PRECIS-2 scores and ICC coefficients for landmark randomized controlled trials in glaucoma.
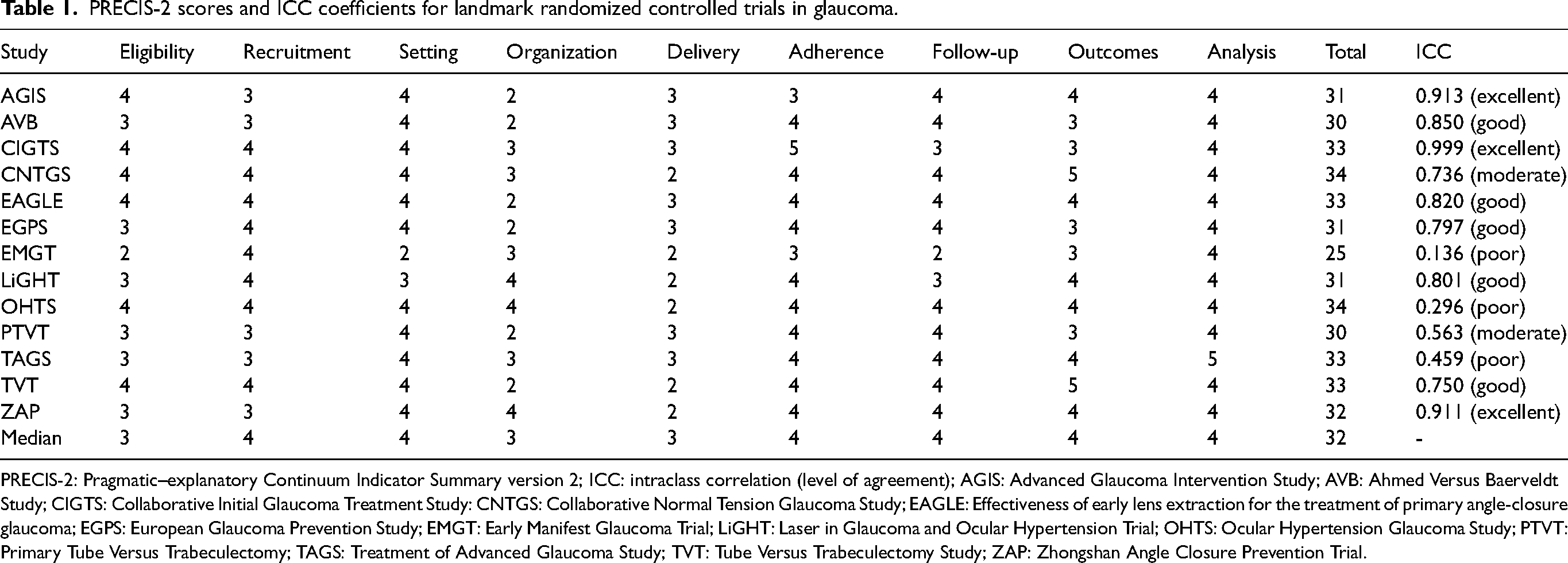
PRECIS-2: Pragmatic–explanatory Continuum Indicator Summary version 2; ICC: intraclass correlation (level of agreement); AGIS: Advanced Glaucoma Intervention Study; AVB: Ahmed Versus Baerveldt Study; CIGTS: Collaborative Initial Glaucoma Treatment Study: CNTGS: Collaborative Normal Tension Glaucoma Study; EAGLE: Effectiveness of early lens extraction for the treatment of primary angle-closure glaucoma; EGPS: European Glaucoma Prevention Study; EMGT: Early Manifest Glaucoma Trial; LiGHT: Laser in Glaucoma and Ocular Hypertension Trial; OHTS: Ocular Hypertension Glaucoma Study; PTVT: Primary Tube Versus Trabeculectomy; TAGS: Treatment of Advanced Glaucoma Study; TVT: Tube Versus Trabeculectomy Study; ZAP: Zhongshan Angle Closure Prevention Trial.
Discussion
The results of this analysis revealed some level of pragmatism in the majority of studies although only one was considered very pragmatic. Even older studies as the AGIS and the CNTGS achieved some degree of pragmatism.9–13
The less pragmatic and more explanatory study was the EMGT (score 24 out of 45).16,17 The EMGT was designed to evaluate the effectiveness of IOP reduction in early untreated open-angle glaucoma. The treatment protocol involved betaxolol 0.5% twice daily and argon laser trabeculoplasty in the treatment group – an unusual option therapy even at that time. The study scored lower in eligibility (2), setting (2), delivery (2), and follow-up (2).
The higher scores were obtained by the OHTS and CNTGS (34 out of 45). Even though, they did not scored high enough to be considered very pragmatic. The OHTS was designed to evaluate the safety and efficacy of topical ocular hypotensive medications in preventing or delaying the onset of visual field loss and/or optic disc damage in patients with ocular hypertension at moderate risk of developing glaucoma. 19 The study scored 4 on all domains, except for delivery (score 2).
The CNTGS purpose was to determine if IOP plays a part in the pathogenic process of normal-tension glaucoma. One hundred-forty eyes of 140 patients were randomized either to be untreated as a control or to have IOP lowered by 30% from baseline. 11 The means to achieve that IOP reduction included both surgery and topical therapy. However, neither beta-adrenergic blockers nor adrenergic agonists could have being used and since prostaglandin analogues were not available at that time, medical options were very limited and different from usual care. Hence, the study scored low on delivery.
The TAGS, a self-labeled pragmatic study did not achieve a very high score (33 out of 45); however, the study scored ≥4 in five domains (setting, adherence, follow-up, outcomes, and analysis) and the remaining four (eligibility, recruitment, organization, and delivery) scored 3, being considered very pragmatic. The trial was designed to compare clinical and cost-effectiveness of primary medical management compared with primary surgery for patients with advanced open-angle glaucoma.37,38 As such, the generalizability of the results can be applied to different populations.
Eligibility – the first of the nine PRECIS-2 domains – analyses to what extent the trial participants are similar to those who would receive an intervention if it was part of usual care. A low score characterizes a very explanatory approach with lots of exclusions (e.g., those who do not comply/respond to treatment, or are not at high risk for primary outcome, are children or elderly), or uses many selection tests not used in usual care. 5 The median score was 3 and the EMGT scored the lowest (2). The study enrolled only newly detected and untreated chronic open-angle glaucoma patients with repeatable visual field defects and many exclusion criteria (visual field loss with mean deviation <16 dB or threat to fixation, mean IOP > 30 mmHg or any IOP > 35 mmHg in at least one eye, visual acuity >0.5 in either eye and any condition precluding reliable fields of photos, use of study treatment or 4-year follow-up).16,17 As a study to assess a very specific primary aim, the authors were understandably restricted to strict eligibility criteria making it difficult to design a more pragmatic study. All the other studies were considered either equally pragmatic/explanatory or rather pragmatic.
Recruitment evaluates the extra effort made to recruit participants over and above what that would be used in the usual care setting to engage with patients. A score 5 for very pragmatic study would recruit participants through usual appointments or clinic, whereas a score 1 for a very explanatory approach would use strategies not used in usual care, e.g., targeted invitation letters, advertising in newspapers, radio plus incentives and other routes. 5 The median score was 4 and, in this domains, all studies were considered either equally pragmatic/explanatory or rather pragmatic.
Setting accesses how the setting of the trial differs from the usual care setting. A score 5 for a very pragmatic study uses identical settings to usual care; a very explanatory approach (score 1) uses only a single center or only specialized academic centers. 5 The EMGT was considered rather explanatory (score 2) since most patients (76.1%) were recruited from population-based screening of specific age cohorts in two cities in Sweden.16,17 Other RCTs that included patients from many different clinics and hospitals were considered either equally pragmatic/explanatory or rather pragmatic.
Organization appraises how the resources, provider expertise and the organization of care delivery in the intervention arm of the trial are different from those available in usual care. A very pragmatic choice uses identical organization to usual care; on the other hand, score 1 for a very explanatory approach if the trial increases staff levels, gives additional training, require more than usual experience or certification and increase resources. 5 The AGIS, AVB, EAGLE, EGPS, and TVT were considered to be rather explanatory. The AGIS had a very complex organization. In addition to clinical investigators in 11 clinical centers (staffed by one or more ophthalmologists, one of whom is clinic director, and by one or more technical staff, one of whom was clinic coordinator), a coordinating center (staffed by an epidemiologist, who was the center director, a statistician, who was deputy director, a data coordinator, a protocol monitor, an administrative coordinator) was responsible for coordinating study activities and communications, maintaining a quality assurance program, randomizing eyes to treatment, and receiving, editing, processing, and analyzing study data, and three committees – Steering Committee responsible for approving changes in policy and procedure, generating scientific publications, and reviewing abstracts and manuscripts submitted for presentation or publication; the Policy and Treatment Effects Monitoring Board, responsible for reviewing and advising on study design and methods, protocol changes, and problems that arose in study conduct, and for reviewing the accumulated data every 6 months for efficacy and safety; and the Operations Committee, responsible for managing the day-to-day conduct of the study.9,10 The other RCTs were similar in their organizations, different from a pragmatic approach.
Flexibility (delivery) weights the flexibility in how the intervention is delivered and the flexibility likely in usual care. Score 5 for a very pragmatic choice has identical flexibility to usual care; score 1 (very explanatory) uses a strict protocol, monitoring and measures to improve compliance, with specific advice on allowed co-interventions and complications. 5 The median score was 3 (equally pragmatic/explanatory) and the CNTGS, EMGT, LiGHT, OHTS, TVT, and ZAP were considered rather explanatory. The EMGT allowed some flexibility in participants who reached progression and followed customary patterns of glaucoma treatment.16,17
Flexibility (adherence) gauges the flexibility in how participants must adhere to the intervention and the flexibility likely in usual care. A very pragmatic approach involves no more than usual encouragement to adhere to the intervention. A very explanatory choice involves exclusion based on adherence and measures to improve adherence if found wanting. 5 The median score was 4 (rather pragmatic). In the AGIS, an interviewer at the coordinating center interviewed study patients by telephone regarding their adherence to medical therapy. Even though the researchers tried to avoid response bias (due to the possible tendency of patients to want to please the doctor or the coordinator), the telephone call might have served as an incentive to improve adherence.9,10
Follow-up examines how different is the intensity of measurement and follow-up of participants in the trial and the likely follow-up in usual care. A very pragmatic approach schedules no more than usual visits. Very explanatory approach schedules arranges more frequent, longer visits, unscheduled visits triggered by primary outcome event or intervening event, and more extensive data collection. 5 The median follow-up score was 4 (rather pragmatic) and the EMGT scored 2 (rather explanatory). In post-screening visits, the ability of the patients to comply with the study interventions and the feasibility of prolonged follow-up was assessed; follow-up visits were scheduled every three months – different from usual care especially for patients with early disease.16,17
Primary outcome grades to what extent the trial's primary outcome is relevant to participants. A high score means there is an obvious importance to participants, whereas a low score for a very explanatory approach uses a surrogate, physiological outcome, central adjudication or use assessment expertise that is not available in usual care, or the outcome is measured at an earlier time than in usual care. 5 In this domain, the median score was 4 (rather pragmatic) emphasizing the important outcomes of all studies, regardless of their degree of pragmatism.
Primary analysis considers whether all data included are in the analysis of the primary outcome. A very pragmatic approach uses an intention-to-treat analysis with all available data. An explanatory analysis excludes ineligible participants after randomization, includes only those that completed the study or those following the treatment protocol (per-protocol analysis). 5 The median score was 4 (rather pragmatic) since all studies used an intention-to-treat analysis of the outcomes.
Organization and Flexibility (delivery) were the two domains which most studies scored low leaning towards the explanatory end of the continuum. In order to improve Organization, researchers should include as investigators professional from free-standing outpatient settings or small community hospitals. A pragmatic trial should include a variety of investigators with a representative mix of experience appropriate to the intervention under study and implement the intervention at a group level incorporating cluster randomization whenever suitable. 41 This might be challenging given the low experience of the staff with academic research. Providers’ expertise and the organization of care delivery in the intervention arm of pragmatic trials should be similar to those available in usual care. As for Flexibility (delivery), pragmatic studies should deliver the intervention just as in normal practice, by staff with typical experience and with the use of routinely available tools. Commonly, pragmatic trials investigate a general approach to treatment and do not dictate specific details of that approach. Adherence to the protocol and delivery of the intervention should be balanced in a pragmatic approach. Investigators should receive training in new glaucoma interventions within the restraints of the hospital where the trial is being conducted and minimum advice on how to achieve good outcomes for participants. 41
This study has some limitations. First, the PRECIS-2 was initially developed to help researchers develop pragmatic studies and not to evaluate the level of pragmatism of published studies. Nevertheless, the instrument has been used in systematic review and meta-analysis of published trials also.6,7 Dal-Ré has suggested that the PRECIS-2 tool is not sensitive enough to clearly discriminate between masked pragmatic RCTs and open-label pragmatic ones and, hence, it should not be used to support placing masked trials in the pragmatic side of the explanatory/pragmatic continuum. 42 Different from this previous study, we scored the RTCs for each of the PRECIS-2 nine domains, whereas Dal-Ré classified RTCs as explanatory, neutral, or pragmatic. Moreover, the author conducted the assessment of the RCTs by himself as in our study we used three raters for the same subjective analysis. Besides, all RCTs included in this study were masked and not open-label.
Second, it has been suggested that the PRECIS-2 instrument should be expanded by including a 10th domain describing the placebo control group. 43 The current version of the instrument contains nine domains and in the analysis of the RCTs we did not assessed the placebo control and blinding aspects of each study. As PRECIS domains have developed over time a revised version of the instrument including a placebo group domain is anticipated for the future. 42 However, since only three RCTs included in this study – EMGT, OHTS, and EGPT – had a matched placebo control groups and as such should be placed in explanatory end, this domain did not interfered in the analysis of most of the studies which leaned towards the pragmatic end.
Third, not all information was clearly stated in the manuscript for an absolute evaluation of each of the 9 PRECIS-2 domains. Whenever an information was not available in the article, a score 3 (equally pragmatic/explanatory) was given for that specific domain. 42 A last drawback was that the ICC for the EMTG, OHTS, TAGS, and PTVT was found to be low. This observation may either represent the inappropriateness of the use of PRECIS-2 as an instrument to evaluate how exploratory/pragmatic the study is or the non-familiarity of the examiners with the instrument – or both. The examiners who participated in the evaluation of the RCTs were young ophthalmologists currently in training of a glaucoma fellowship program and not very experienced in clinical research. Nevertheless, they could well be representative of a general/average reader of clinical articles of scientific journals.
In summary, the results of this study revealed that there is a need for more pragmatic studies in glaucoma research. Explanatory RCTs provide important information about treatment effects in selected populations. These trials are designed to maximize estimates of treatment efficacy and safety of new interventions in glaucoma care, but the findings are often not easily generalized to the broad range of patients seen in clinical settings. More data and information can be gained from properly designed pragmatic RCTs, whose results are more broadly generalizable to routine clinical glaucoma practice.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.