
Abstract
Purpose
To compare the efficacy of gonioscopy-assisted transluminal trabeculotomy (GATT) versus micropulse transscleral diode laser cyclophotocoagulation(MP-TDLC) combined with GATT in the treatment of advanced glaucoma.
Methods
This retrospective comparative study study included 82 patients (82 eyes) with a diagnosis of advanced glaucoma: 36 patients underwent GATT, and 46 underwent GATT + MP-TDLC. Intraocular pressure (IOP) changes in patients who underwent GATT and GATT MP-TDLC were analyzed retrospectively at regular intervals during the 6-month follow-up period.
Results
For the 82 patients included in this study, the mean ± SD IOPs before the procedures were 27.2 ± 8.5 mmHg in the GATT group and 26.6 ± 6.9 mmHg in the GATT + MP-TDLC group (p = 0.866), and the numbers of glaucoma medications used were 3.41 ± 0.5 in the GATT group and 3.36 ± 0.4 in the GATT + MP-TDLC group (p = 0.605). The mean IOP after GATT was 13.6 ± 3.9 mmHg at day 1, 13.9 ± 3.7 mmHg at week 1, 14.6 ± 4.0 mmHg at month 1, 15.3 ± 4.3 mmHg at month 3, and 14.7 ± 3.3 mmHg at month 6. In the GATT + MP-TDLC group, the postoperative day 1, week 1, month 1, month 3, and month 6 IOP values were 12.4 ± 2.5, 11.8 ± 1.8, 12.1 ± 2.0, 11.8 ± 1.09, and 11.8 ± 1.5 mmHg, respectively.
Conclusion
GATT was found to be effective in the treatment of patients with advanced glaucoma, and results closer to the targeted low teens IOP values were obtained with GATT + MP-TDLC.
Keywords
Precis
GATT alone was successful in reducing intraocular pressure in patients with advanced glaucoma. GATT + Micropulse transscleral diode laser cyclophotocoagulation provides a lower intraocular pressure target without serious complications in patients with advanced glaucoma.
Introduction
In the diagnosis and follow-up of glaucoma, progressive visual field defects are the most serious risk factor for permanent vision loss. 1 The current options for glaucoma treatment include using topical medication, surgery, or laser treatment to attempt to reach the target intraocular pressure (IOP).2,3 According to the International Classification of Diseases, glaucoma is considered advanced when there is advanced damage to the optic disc, a visual field defect, and/or 5° fixation with glaucoma in both the superior and inferior hemifields. 4 Patients with advanced glaucoma require disproportionately frequent follow-ups and serious interventions compared to other glaucoma patients. Glaucoma treatment guidelines suggest that surgery may be an appropriate primary option in patients with advanced glaucoma.5,6 Currently, IOP reduction is the most effective treatment known to prevent glaucoma progression and visual field loss. 7 The Advanced Glaucoma Intervention Study (AGIS) demonstrated that visual field loss was minimal when patient IOPs were below 18 mmHg at all follow-up periods. 7 In the same study, visual field defects were reduced in patients with IOPs below 14 mmHg in the early postoperative period. Based on this finding, aggressive IOP reduction (i.e. below 14 mmHg) is targeted in the treatment of advanced glaucoma.
First described by Grover et al. in 2014 as a minimally invasive glaucoma surgery technique, gonioscopy-assisted transluminal trabeculotomy (GATT) is a conjunctival-sparing trabeculotomy technique with an rapid efficacy and safety profile. 8 GATT is a minimally invasive glaucoma surgery technique with a more favorable safety profile. This procedure provides aqueous humor from the circumferentially opened dysfunctional trabecular meshwork to reach the collecting ducts and episcleral vessels. To date, GATTs have been performed to treat glaucoma of varying severity, including advanced glaucoma.9,10 Transscleral diode laser cyclophotocoagulation (TDLC) is a cyclodestructive treatment option for the treatment of refractory glaucoma in particular. 11 Previous reports indicate that the surgical success rate of TDLC in achieving target IOP ranges from 40% to 80%.12,13 Unlike conventional TDLC, micropulse transscleral diode laser cyclophotocoagulation (MP-TDLC) delivers a series of repetitive short-energy pulses with specific rest periods between pulses. MP-TDLC has been an important option for the treatment of advanced glaucoma, demonstrating significant success in targeting and minimal collateral damage while significantly reducing postoperative complications. 14 The technique effectively ensures that the thermal reaction is confined to the absorbing tissue and eventually crosses the coagulative threshold. With intermittent cooling, nonpigmented structures adjacent to the target tissue do not cross the coagulative limit, thereby minimizing collateral tissue damage. 14 Previous studies have shown that MP-TDLC is effective in achieving the target IOP and has a lower risk of complications for the treatment of advanced glaucoma.15,16 However, little is known about the risks and efficacy of GATT and MP-TDLC for patients with advanced glaucoma, and complications and success factors according to glaucoma type have not yet been determined. To the best of the our knowledge, no studies have provided data on the efficacy of MP-TDLC with GATT in achieving the target IOP in patients with advanced glaucoma. Therefore, we aimed to compare the efficacy of GATT with that of GATT + MP-TDLC in the treatment of advanced glaucoma.
Method
This retrospective comparative study was approved by the Başakşehir Çam and Sakura City Hospital Ethical Committee and Review Board, and it was conducted in accordance with the Declaration of Helsinki.
Patients
Patients with primary open-angle, pseudoexfoliation, pigment dispersion, uveitic/inflammatory, steroid-induced, or lens-induced glaucoma were included in the study. Using the two Swedish interactive threshold algorithm standard 24-2 visual field examinations (Humphrey Field Analyzer; Carl Zeiss Meditec, Dublin, CA) and retinal nerve fiber layer evaluation (Topcon DRI OCT Triton; Topcon, Corp., Tokyo, Japan), patients who were found to have advanced glaucoma and whose glaucoma progressed despite maximum medical treatment were included in the study. Advanced disease was classified as ‘severe’ visual loss based on the Hodapp glaucoma severity classification. 17 Surgery was performed on these patients. For this reason, a cut-off IOP value for surgery was not established. The results of two surgical groups, GATT and GATT + MP-TDLC, were analyzed. All patients underwent a complete eye examination including best corrected visual acuity, IOP measurement with Goldmann applanation tonometry, evaluation of anterior and posterior segments, and gonioscopy before surgery and on the postoperative 1st day, 1st week, 1st month, 3rd month, and 6th month. The visibility of the trabecular meshwork was carefully performed by gonioscopy before surgical application. Patients with incomplete 360-degree trabeculotomy, angle-closure glaucoma, corneal decompensation, corneal opacity that prevents visualization of the angle, intraocular lens dislocation, neovascular glaucoma, or uncontrolled bleeding parameters were excluded from the study.
Surgical technique
GATT procedure
All surgeries were performed under general anesthesia. All patients were prepared under routine antisepsis using an eyelid speculum, and 5% povidone iodine was administered for 3 min. A 23-gauge needle incision was made in the temporal or superior quadrant to enter the anterior chamber.
The anterior chamber was deepened by inserting viscoelastics through this incision. To maximize the imaging conditions with the Swan-Jacob gonio lens, the patient's head was rotated 30° away and the microscope was positioned accordingly. A 2 mL goniotomy was prepared through a temporal incision by using a microsurgical blade. A blunted 6-0 Prolene suture was used for catheterization in all surgeries. This suture was directed at an angle in the nasal region by using a superior incision and then used to provide a circumferential trabeculotomy. A blunt-tipped Prolene suture held with vitreoretinal forceps was inserted into Schlemm's canal through the goniotomy incision. This suture was passed all the way through, and its blunt end was captured using a microsurgical forceps. The blunt end was held with a vitreoretinal forceps, and the other part of the suture was gently pulled to complete the 360° trabeculotomy. The irrigation and aspiration method was used to wash the anterior chamber.
MP-TDLC procedure
Following the routine GATT procedure, a Supra 810 nm diode laser (Quantel Medical) with 2000 mW power at 31.3% duty cycle was irradiated 0.5 ms. The MicroPulse G probe was placed perpendicular to the sclera at the limbus border, and the laser power was applied to the upper and lower hemispheres with a sliding motion, excluding the 9 and 3 o'clock positions. An application time of 180 s was valid in all cases of advanced glaucoma.
Both groups were administered postoperative moxifloxacin and dexamethasone drops four times daily. The primary outcome is surgical success, with secondary outcomes including IOP levels and the number of glaucoma medications. Surgical success is defined as achieving an IOP of 18 mmHg or less and an IOP reduction exceeding 20% from baseline, while maintaining the same or fewer medications. Cases with IOP higher than 18 mmHg compared to baseline or requiring more medications were deemed failures only if persisting after the third postoperative month. Any further surgery for IOP control or instances of loss of light perception at any time were considered as failures.
Statistical analysis
In the study, statistics related to continuous variables were reported as mean ± standard deviation/median (minimum - maximum) values, and descriptive statistics related to categorical variables were reported as numbers and percentages. Intergroup comparisons were performed using an independent groups t-test or Mann–Whitney U test depending on the distribution structure. Pre- and post-treatment comparisons were performed using a paired two-sample test or Wilcoxon test depending on the distribution structure. The relationships between categorical variables were analyzed using a chi-square test. Kaplan Meier survival analysis was used to analyse the cumulative probability of success between the groups. Kaplan-Meier analysis findings were evaluated for statistical significance by Log-rank test. IBM SPSS Statistics (Version 28) software was used for statistical analyses. The analyses were performed considering a 95% significance level, and p ≤ 0.05 was considered statistically significant.
Results
The study included 36 patients who underwent GATT and 46 patients who underwent GATT + TDLC for advanced glaucoma. The patients in the GATT group had a mean age of 56.8 ± 17.4 years, and 36% of them were male. The patients in the GATT + MP-TDLC group had a mean age of 58.1 ± 12.2 years, and 41.3% of them were male. The baseline demographic characteristics and preoperative Best-Corrected Visual Acuity (BCVA), cup disc ratio, nerve fiber analysis, and visual field index evaluation as well as the glaucoma types of patients in both groups are shown in Table 1. In the GATT group, 19 (52.7%) patients were phakic and 17 (47.2%) were pseudophakic, while 24 (52.1%) patients were phakic and 22 (47.9%) were pseudophakic in the GATT + MP-TDLC group. Cataract surgery was not performed in the patients included in the study.
Demographic data and baseline ocular characteristic.
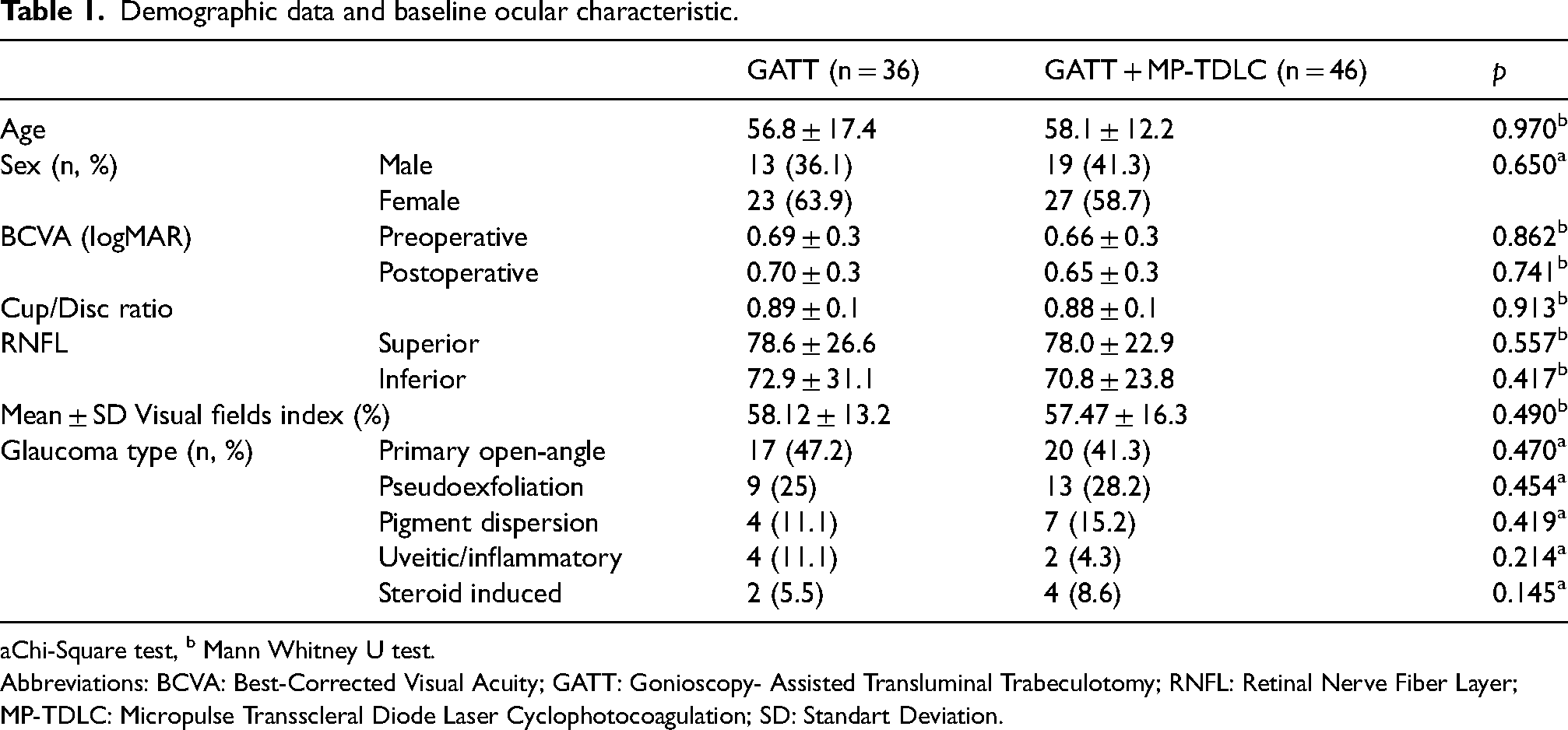
Chi-Square test, b Mann Whitney U test.
Abbreviations: BCVA: Best-Corrected Visual Acuity; GATT: Gonioscopy- Assisted Transluminal Trabeculotomy; RNFL: Retinal Nerve Fiber Layer; MP-TDLC: Micropulse Transscleral Diode Laser Cyclophotocoagulation; SD: Standart Deviation.
The number of preoperative medications was respectively 3.41 ± 0.5 and 3.36 ± 0.4 in the GATT and GATT + MP-TDLC groups, and no significant difference was observed between these groups (p = 0.605) (Table 2). The number of medications at 6 months post-operation was respectively 1.08 ± 1.2 and 0.28 ± 0.5 in the GATT and GATT + MP-TDLC groups; clearly, the number of medications in the GATT + MP-TDLC group was significantly lower (p = 0.002). An analysis of the change in the number of medications used preoperatively and postoperatively revealed a significantly higher decrease in the GATT + MP-TDLC group (p = 0.006) (Table 3).
Comparison of baseline IOPs and number of medications with various postoperative follow-up periods.
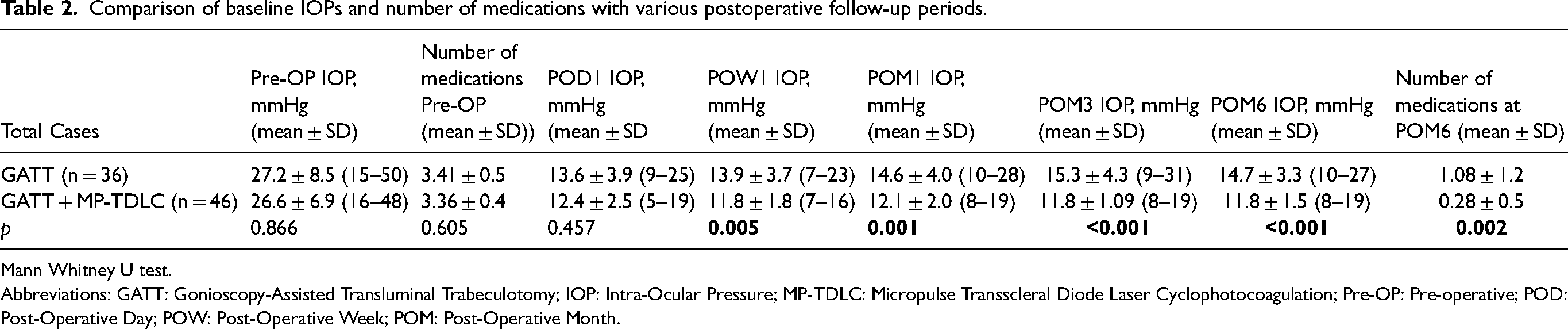
Mann Whitney U test.
Abbreviations: GATT: Gonioscopy-Assisted Transluminal Trabeculotomy; IOP: Intra-Ocular Pressure; MP-TDLC: Micropulse Transscleral Diode Laser Cyclophotocoagulation; Pre-OP: Pre-operative; POD: Post-Operative Day; POW: Post-Operative Week; POM: Post-Operative Month.
Efficacy data for the study population at selected postoperative time points.
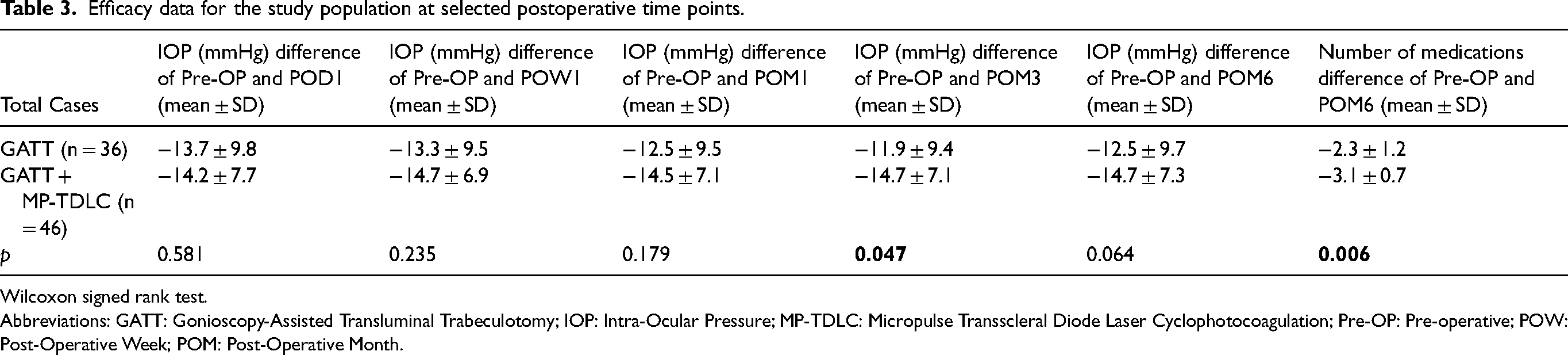
Wilcoxon signed rank test.
Abbreviations: GATT: Gonioscopy-Assisted Transluminal Trabeculotomy; IOP: Intra-Ocular Pressure; MP-TDLC: Micropulse Transscleral Diode Laser Cyclophotocoagulation; Pre-OP: Pre-operative; POW: Post-Operative Week; POM: Post-Operative Month.
In the GATT group, the postoperative 1st day, 1st week, 1st month, 3rd month, and 6th month IOP values were 13.6 ± 3.9, 13.9 ± 3.7, 14.6 ± 4.0, 15.3 ± 4.3, and 14.7 ± 3.3 mmHg, respectively. In the GATT + MP-TDLC group, the corresponding values were 12.4 ± 2.5, 11.8 ± 1.8, 12.1 ± 2.02, 11.8 ± 1.9, and 11.8 ± 1.5 mmHg, respectively. Whereas the preoperative IOP values between the groups did not show a significant difference, the postoperative IOP values in the GATT + MP-TDLC group were significantly lower at the 1st week (p = 0.005), 1st month (p = 0.001), 3rd month (p < 0.001), and 6th month (p < 0.001) (Table 2). An analysis of the preoperative and postoperative IOP changes of the GATT and GATT + MP-TDLC groups revealed that although the decrease was more pronounced in the GATT + MP-TDLC group in all controls, only the change in the 3rd month was statistically significant (p = 0.047) (Table 3).
At the 6th postoperative month evaluation, the radial nerve fiber layer values in the GATT and GATT + MP-TLDC groups were 77.8 ± 26.3 and 77.5 ± 22.3 in the superior, 71.9 ± 31.4 and 70.1 ± 23.7 in the inferior, respectively. There was no statistically significant difference between the groups (p > 0.05). At the 6th postoperative month, the visual field index value was 57.83 ± 13.1 in the GATT group, and in the GATT + MP-TDLC group, it was 57.35 ± 15.8. No significant difference was observed between the groups.
At the 6-month follow-up assessments, the predefined success criteria were fulfilled by 32 individuals (88.9%) within the GATT group, whereas 45 patients (97.8%) in the GATT + MP-TDLC group demonstrated successful outcomes. The cumulative success rate was 0.885 in the GATT group and 0.978 in the GATT + MP-TDLC group. There was no significant difference between GATT and GATT + MP-TDLC groups in terms of cumulative success (survival) (p = 0.088 > 0.05) (Figure 1). IOP spike (IOP ≥ 30 mmHg within one month postoperatively) occurred in 10 eyes (27.7%) in the GATT group and 11 eyes (23.9%) in the GATT + TDLC group. IOP spike was managed with glaucoma medications or through the release of aqueous humor from the paracentesis site. Hyphema occurred in 12 (33.3%) patients within the GATT group and in 14 (30.4%) patients within the GATT + MP-TDLC group. These cases responded favorably to medical interventions, leading to regression without necessitating additional surgical procedures. In the GATT + MP-TDLC group, transient ocular hypotony was observed in two patients on postoperative day 1. No uveitis, phthisis bulbi, or choroidal detachment was observed in the GATT + MP-TDLC group. Fibrin reaction in the anterior chamber was noted in only three patients (6.5%) in the GATT + MP-TDLC group, which resolved with medical treatment, eliminating the need for additional surgical procedures.
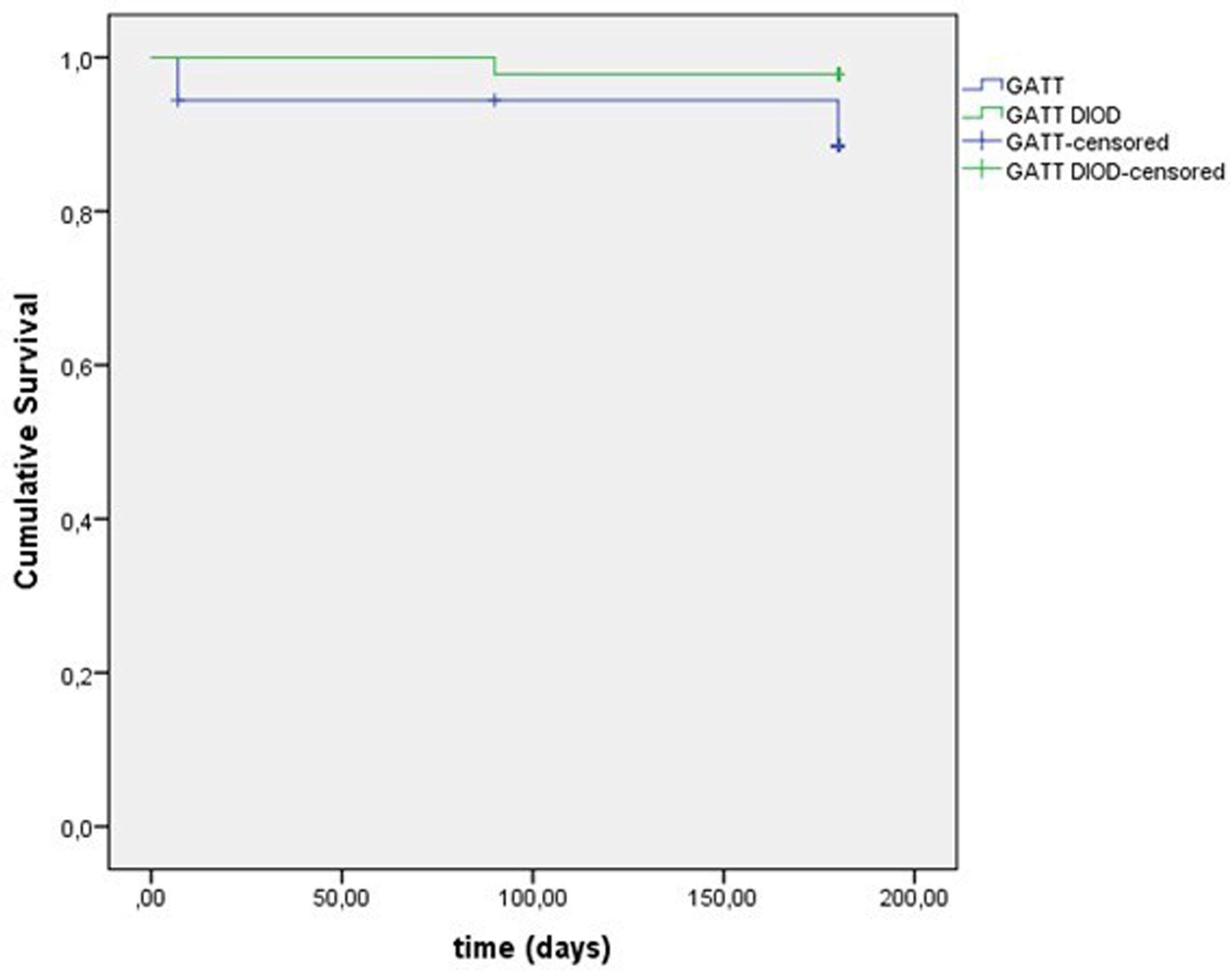
Kaplan Meier survival analysis graph.
Discussion
This study sought to assess the efficacy of GATT and GATT + MP-TDLC in managing advanced glaucoma. The surgical success criteria, defined as meeting predetermined IOP targets without additional surgical interventions, were achieved by a high proportion of patients in both groups. However, the GATT + MP-TDLC group demonstrated a slightly higher success rate compared to the GATT group. The GATT + MP-TDLC group showed a significantly greater reduction in the number of postoperative medications compared to the GATT group. Regarding postoperative complications, both groups experienced manageable adverse events such as hyphema, transient ocular hypotony and fibrin reaction in the anterior chamber within the first three months post-implantation. Notably, these complications were effectively addressed with medical interventions and did not require additional surgical procedures. Importantly, no further complications were reported in any of the patients during the remainder of the 6-month observation period. These findings underscore the potential of both GATT and GATT + MP-TDLC in effectively managing advanced glaucoma with a low incidence of of no serious permanent complications. However, at the end of the six-month follow-up period, four eyes in the GATT group exceeded the target IOP, while only one eye in the GATT + MP-TDLC group had values above the desired threshold, necessitating additional surgical procedures for these patients.
The current and widespread use of the GATT procedure prompts the necessity for comprehensive evaluation of its efficacy and safety, particularly concerning its application in patients with advanced glaucoma. 18 GATT affords some important advantages over trabeculectomy in advanced glaucoma surgery. The most obvious differences are related to the safety profile; bleb-related complications are not observed, and hypotony is extremely rare. As it is not a conjunctiva-related surgery, it does not pose a limitation for filtering surgeries if necessary, thus providing diverse options in the subsequent treatment of patients. Recent studies have reported that GATT may have a better efficacy than trabecular bypass stents.19,20 Rahmadnejad et al. reported that GATT had a 63% success rate and 44% mean IOP reduction rate after an average of 11.9 months. 10 Grover et al. reported that GATT had mean IOP reduction rates of 37.3% and 49.8% in primary and secondary open-angle glaucoma, respectively, after two years, with glaucoma drugs significantly decreasing from the baseline. 21 MIGS surgery is recommended for patients with mild and moderate glaucoma. Grover et al. reported a higher failure rate of the GATT procedure in patients with advanced glaucoma, with an MD worse than −15. 21 The main reason for the decrease in the success rate may be collector duct atrophy. By contrast, Aktaş et al. did not find a significant relationship between IOP reduction and MD values. 9 Hann et al. estimated that advanced glaucoma itself constitutes the main problem. 22 Advanced glaucoma is not limited to increased distal outflow resistance and collecting duct atrophy. Similar to this theory, Aktas et al. did not report high surgical failure rates after GATT surgery in advanced glaucoma, with only 5.4% of patients needing additional filtration surgery. 23 In one of the most recent studies, Dar et al. reported GATT as a successful surgical option in advanced glaucoma cases. 24 In our study, we observed an IOP decrease of 45% in the GATT group at the 6-month follow-up as well as a significant decrease in the number of medications used.
Although several studies have shown the efficacy of MP-TDLC in advanced glaucoma cases, to the best of our knowledge, no comparison has been reported between the efficacy of GATT and GATT + MP-TDLC in these cases. In the postoperative follow-up of advanced glaucoma patients treated with the GATT + MP-TDLC method, significantly lower IOP values were achieved in the 1st week, 1st month, 3rd month, and 6th month follow-up evaluations compared to those in the GATT group. An evaluation of the preoperative and postoperative IOP change in the GATT + MP-TDLC group revealed that it was higher than those in the GATT group in all postoperative follow-up periods and was significantly higher at the 3rd month. An evaluation of the 6-month follow-up IOP value and number of medications revealed that the GATT + MP-TDLC group was more successful in reaching the target values.
Patients with any intraoperative complications were not included in our study. The data from patients who could not complete the procedure due to any intraoperative complications or for whom the standard procedure could not be performed were excluded from the study. This exclusion was necessary because their data would not yield accurate results for the surgical procedure. Postoperative complications in the GATT group were similar to those reported in the literature.9,25 The most common complications were hyphema, all of which resolved spontaneously, did not require intervention. Among the early postoperative complications, transient ocular hypotony and hyphema were observed in a limited number of patients in the GATT + MP-TDLC group in the 1st week post-operation. In both groups, permanent ocular hypotony with or without phthisis bulbi was not observed in any eye during follow-up. Sympathetic ophthalmia, endophthalmitis, or vitreous hemorrhage were not observed in both groups.
The limitations of this study include the relatively small number of patients, short follow-up time, and inclusion of patients with open-angle but various types of glaucoma between groups. One limitation of this study is its retrospective design, which lacks subsequent randomization. Longitudinal studies with large surgical series may be needed to evaluate the full effects of GATT and additional combined surgeries on patients with advanced glaucoma. The GATT + MP-TDLC group must be evaluated in terms of complications with larger prospective studies.
In conclusion, GATT and GATT + MP-TDLC were found to be effective in patients with advanced glaucoma, with GATT + MP-TDLC providing results closer to the target pressures. In these patients, GATT + MP-TDLC should be considered before subconjunctival surgery. Close postoperative follow-up and prompt and appropriate treatment in terms of complications are critical.
Footnotes
Acknowledgements
The authors did not receive any financial support for this study, and they have no conflicts of interest to declare.
Authors’ contributions
Writing: Murat Karapapak, M.D.; Ali Olgun, M.D.
Data Collection and Processing: Murat Karapapak, M.D.; Ali Olgun, M.D.
Data Sharing: Murat Karapapak, M.D.; Ali Olgun, M.D.
Analysis and Interpretation: Murat Karapapak, M.D.; Ali Olgun, M.D.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed consent
The requirement for informed consent was waived by the local ethics committee.