
Abstract
Purpose
This literature review aims to provide a comprehensive overview of the current understanding, indications, techniques, outcomes, and complications of Müller muscle-conjunctival resection (MMCR) surgery. It also addresses areas of debate with MMCR such as predictability concerning Phenylephrine response as well as the amount of muscle resection required.
Method
This literature review was compiled based on the available evidence from PubMed from 1975 to August 2023.
Results
The success rate of MMCR ranges from 72% to 95%, with high patient satisfaction reported in most studies. The exact range of eyelid elevation after MMCR is variable, with a reported average of 2.1 mm MRD1 elevation.
Conclusion
MMCR is a well-established surgical technique used to correct upper eyelid ptosis that results from dysfunction or attenuation of the levator aponeurosis. MMCR proved to be a safe and effective procedure with a high patient satisfaction rate and low risk of complications.
Keywords
Introduction
Upper eyelid ptosis is a common condition in which the upper eyelid margin is situated lower than normal, leading to visual field obstruction and cosmetic concerns. The primary cause of ptosis is dysfunction or attenuation of the Levator Palpebrae Superioris aponeurosis (LPS). Ptosis may be classified based on the degree of ptosis and etiology such as congenital, aponeurotic, mechanical, traumatic, and neurogenic. The retractors of the upper eyelid are the LPS muscle and the Müller muscle. The Müller muscle originates from the inner aspect of the LPS and inserts at the upper edge of the tarsus receiving its innervation from the sympathetic nervous system. 1 Among the various surgical techniques used to correct ptosis, Müller muscle-conjunctival resection (MMCR) is known for its relative simplicity and excellent outcomes, especially in cases of mild to moderate ptosis with good LPS function. 2
Methodology
A comprehensive search of the PubMed database was conducted using the following keywords: “Müller muscle-conjunctival resection,” “MMCR,” “ptosis surgery,” and “upper eyelid ptosis.” Studies published from 1975 to August 2023 were included in this review. All relevant articles in English were included in our review with a total of 73 cited articles. We summarized the total surgical outcomes of this procedure including all surgical modifications documented. The predictability of the pre-operative phenylephrine test was analyzed in all relevant studies as well as the predictability of the amount of Müller muscle resection. Other parameters such as conjunctival changes, dryness, and postoperative complications were also discussed. This was approved by the IRB board and scientific committee at King Khaled Eye Specialist Hospital.
History & mechanism of action
Müller Muscle-Conjunctival Resection (MMCR) was first introduced in 1975. Prior to that, the Frasnella-Servat procedure was a common practice, which was a similar procedure that included Müller muscle resection with the conjunctiva and part of the tarsus. Putterman and Urist modified that and introduced the MMCR surgery to exclude any alteration to the tarsal tissue. MMCR has the appeal of being an internal approach avoiding an external wound and does not classically require additional lid crease reformation after this procedure. 3
The MMCR procedure's rising recognition is largely due to its straightforward approach and simplicity in addressing ptosis. Yet, the exact mechanism in which it addresses ptosis has been a topic of discussion for many years. Putterman originally believed that the procedure's efficacy came from fortifying Müller's muscle through its resection and advancement 3 In contrast, Buckman et al examined the Müllerectomy's extent in the Fasanella-Servat procedure and found that even with minimal smooth muscle presence, the outcome of ptosis correction was as effective as in cases with a larger amount of Müller's muscle. Thus indicating that Müller's muscle resection might not be crucial for the procedure's effectiveness. 4 Similarly, Zauberman et al suggested that shortening the vertical posterior lamella coupled with the scarring effect is pivotal to providing post-operative eyelid elevation. 5 Another suggested mechanism is the tightening of Müller's smooth muscle-LPS complex on the tarsus. This theory gained support after a cadaveric study by Marcet et al found the LPS to be plicated in all cases with some residual Müller muscle fibers. This emphasized the importance of LPS muscle functionality in predicting the procedure's success, much like in LPS plication methods. 6 Reinforcing the idea that MMCR's efficacy doesn't solely rely on Müller's muscle is its success. In cases of Horner's syndrome, this is particularly noteworthy because Müller's muscle lacks innervation in these instances yet MMCR was still effective. 7 Furthermore, to analyze the amount of Müller's muscle excised in the total tissue resected, Zauberman found it to be 21 ± 19% of total tissue. The percentage of muscle within total tissue excised did not correlate to final MRD1; further supporting that mechanism is not directly related to Müller muscle resection. 5
Surgical technique and variations
MMCR with sutures
The standard procedure is performed under local anesthesia consisting of 1–2% Lidocaine with 1:100,000 epinephrine injected subconjunctivally. Variations documented have included adding 0.5–0.75% Bupivacaine. A Desmarres retractor is used to evert the eyelid then a caliper or ruler is used to measure 2 mm superior to the peak of the tarsal plate. The use of 4-0 silk traction sutures to grasp conjunctiva and Müller muscle tissue can be used. Then a Putterman's clamp or any equivalent T-shaped clamp is used at the desired area depending on the amount of resection planned. A running horizontal mattress 6-0 or 5-0 absorbable suture is then placed just below the clamp edge which can be buried or tied. The clamped conjunctiva-Müller tissue is then excised with a #15 blade. The clamp is then released, and the eye is then covered with an antibiotic-steroid combination ointment or drops with or without the use of a Bandage Contact Lens (BCL) over the cornea. 3 Mangan et al, suggest using Bandage Contact Lens (BCL) routinely after MMCR to reduce corneal abrasions, and postoperative pain and irritation thus facilitating a quicker return to normal daily activities. 8 To date, there has been no study comparing the complication rates with or without the use of BCL. Different variations of using non-absorbable sutures like 6-0 prolene are preferred by some surgeons.5,9,10
MMCR with a single suture
A single suture technique was described by placing a single horizontal suture at the midpoint of the clamp. The authors found this technique to be as effective as the traditional MMCR. The single suture technique did not eliminate the risk of post-operative corneal abrasion. It is advocated as a safer approach to avoid multiple needle entries which may risk direct cornea injury as well as being more time-effective. 11
MMCR with tarsectomy
Other surgical variations include the addition of a tarsectomy. A study compared the addition of 1 mm tarsectomy to 2 mm tarsectomy in a standard 8 mm MMCR. The postoperative MRD1 improved by an average of 1.66 mm with the addition of 1 mm tarsectomy versus 2.72 mm with the 2 mm tarsectomy. This encourages the addition of tarsectomy in different lengths based on the desired outcome required for each case especially when the desired elevation is more than 2.1 mm. 12
MMCR without sutures
Another variant method is the suture-less approach. Leapman introduced this method following the initial surgical procedure described by Putterman with the utilization of a direct hemostat instead of a continuous suture. This technique yielded successful results with an average of 1.45 mm eyelid elevation. Leapman advocates for this suture-less approach, mentioning benefits like the absence of suture-related complications like foreign body granuloma as well as reduced surgery duration. He also claims that it eradicates tarsal irregularities stemming from inconsistent suture placements. However, there has been no direct comparison of eyelid contour and the tarsal margin between the suture-less method and the classic technique. Yet, the technique's straightforwardness and easier learning curve seem promising. 13 In a single study comparing the suture-less technique to the traditional MMCR, Van Philips et al noted a statistically significant variance in the MRD1 alterations. The suture-less MMCR had an average improvement of 3.27 mm in MRD1 compared to 2.39 mm in the conventional MMCR. 14
MMCR with fibrin sealant glue
Wound closure using fibrin sealant (Tisseel) was also introduced as a suture alternative. This method achieved adequate eyelid elevation as it is a low-tension wound with no residual material after 1-week post-operative. 15 It had similar success rates to traditional suture-MMCR which had more pain, suture granuloma, and corneal issues with 13% needing further procedures.16,17 With lower rates of suture-related complications and corneal abrasion in the fibrin sealant group, it is advised for cases with recurrent corneal erosions, previous refractive procedures, and ocular surface disease. Nonetheless, the cost of the Tisseel kit is high with unknown safety profiles in pregnancy and pediatric age groups.15,17
Conjunctiva-sparing MMCR
While all these variations have proved successful, concern over the loss of conjunctiva tissue remains. A conjunctiva-sparing Müller muscle resection technique was presented and found efficacious results. No corneal irritation or abrasion was reported with this method. 18 This technique involves incising the conjunctival to directly visualize the Müller muscle and then using the Mancini Keenum bipolar forceps to cauterize the muscle. The free conjunctiva flaps were then left open for primary healing intentions. Despite the additional step of conjunctival incision, this method was recorded to be quicker than traditional MMCR with an average of 4.42 min versus 8.45 min respectively. They also reported 1 mm higher post-operative MRD1 with this method. 19 The “Open Sky Müller Muscle Resection” was another similar technique that involved the addition of 1 mm tarsectomy. The aim is to increase eyelid elevation as well as direct visualization of the Müller muscle. This allows for direct subtotal stripping of Müller muscle from LPS. It is described by adding 3 double-armed 5-0 silk sutures through the conjunctival edge and exiting through the skin crease while incorporating residual Müller muscle and the upper edge of the tarsus. Successful eyelid elevation to the desired level was reached in 92% with significant over-correction reported in only one case. The authors also advocate this technique to cause eyelid eversion consequently avoiding upper eyelid entropion. 20 Attention must be given to the eyelid shape and contour with multiple tarsal sutures as one study of a similar technique found medial eyelid flare in one eye. 21
External MMCR
An external approach to Müller muscle alteration has been presented, in an external Müller muscle tucking procedure. This requires a skin crease incision and exposure of the tarsus then fixing Müller muscle to tarsal tissue in a similar manner to LPS advancement. This technique had a higher rate of revision when compared with the external levator advancement procedure. 22
Ultimately the selection of the MMCR method is influenced by the surgeon's expertise, patient characteristics, and degree of ptosis.
Indication and patient selection
MMCR is primarily indicated for patients with mild to moderate ptosis and good LPS muscle function (≥5 mm).3,6 It has been recommended that patients undergo the phenylephrine test as a part of their clinical assessment of ptosis. The phenylephrine test assesses the Müller muscle's sympathetic tone, which is believed to be a useful preoperative tool to predict the surgical outcome. 23 Generally, patients with positive phenylephrine test results are considered suitable candidates for MMCR.9,24 However, not all authors agree on the usefulness of preoperative phenylephrine testing as will be discussed in the upcoming segment. 25 MMCR is often classically done for aponeurotic ptosis but successful outcomes in congenital ptosis have also been reported.21,26–28 To extend the selection criteria for MMCR, Sweeney et al compared outcomes of MMCR vs External Levator resection (ELR) for patients with severe ptosis in 142 eyes. Severe ptosis in this study was MRD of 0 or less. In fact, they found a higher success rate in the ptosis correction for the MMCR group 97.2% vs 77.4% in the ELR group supporting its efficacy in severe ptosis. 29 One possible explanation for this finding is the abnormal fatty infiltration of LPS muscle in cases of severe ptosis thus resulting in suboptimal results with ELR. 30
The patient's ethnic variability did not appear to result in different outcomes despite different anatomy of septal/LPS insertions. There was no statistically significant difference in surgical outcome of MMCR between Caucasian and Asian eyelids. 31
Müller Muscle Conjunctival Resection has an additional role in shortening the fornix. Thus maximal MMCR can be seen as a procedure of choice for cases of Giant Fornix Syndrome with ptosis.32,33 In addition to correcting the large superior fornix, reports of post-operative improvement of chronic discharge were also noted in a small series. 34 The theory behind this improvement is related to the excision of inflamed conjunctiva, bacterial reserve, and minimizing dead space for coagulum formation with better response in maximal MMCR. 32 Caution must be taken in anophthalmia to avoid further damage to the conjunctiva resulting in socket contraction. The conjunctiva-sparing technique was studied in patients with anophthalmia and reported good MRD1 elevation of an average of 2.8 mm. One case of significant over-correction (5.5 mm elevation) was reported but the adjustment of the prosthesis was sufficient to overcome it. 35 Interestingly, another indication for MMCR was advised by Saonanon et al in Thyroid Eye Disease (TED). He hypothesizes that Hering's phenomenon can help alleviate unilateral retraction by elevating the contralateral eye despite the lack of ptosis. The surgical outcome was comparable to their preoperative 10% phenylephrine test. MMCR in TED yielded promising results by elevating the operated eye and lowering the retracted eyelid to achieve symmetry without compromising contour. 36
The phenylephrine test
The Phenylephrine test is a clinical test by instilling 2.5%, or 10% Phenylephrine drops in the ptotic eye and observing the difference of MRD-1 before and 5–10 min after. It is believed that the sympathetic effect of phenylephrine works on contracting the Müller muscle which consequentially elevates the eyelid. A comparison between 2.5%-10% phenylephrine revealed no notable disparity in the elevation of the upper eyelid. 37
It has been classically reported that to achieve the same elevation as the phenylephrine drops, 8.25 mm of Müller muscle resection should be performed. 23 While the majority of surgeons avoid performing MMCR in ptosis cases that don’t respond to Phenylephrine drops, the debate about the test accuracy stands. Studies have found varying results on the accuracy and predictability of the pre-operative Phenylephrine test (Table 1).
A summary of the documented results on the predictability of pre-operative phenylephrine test.
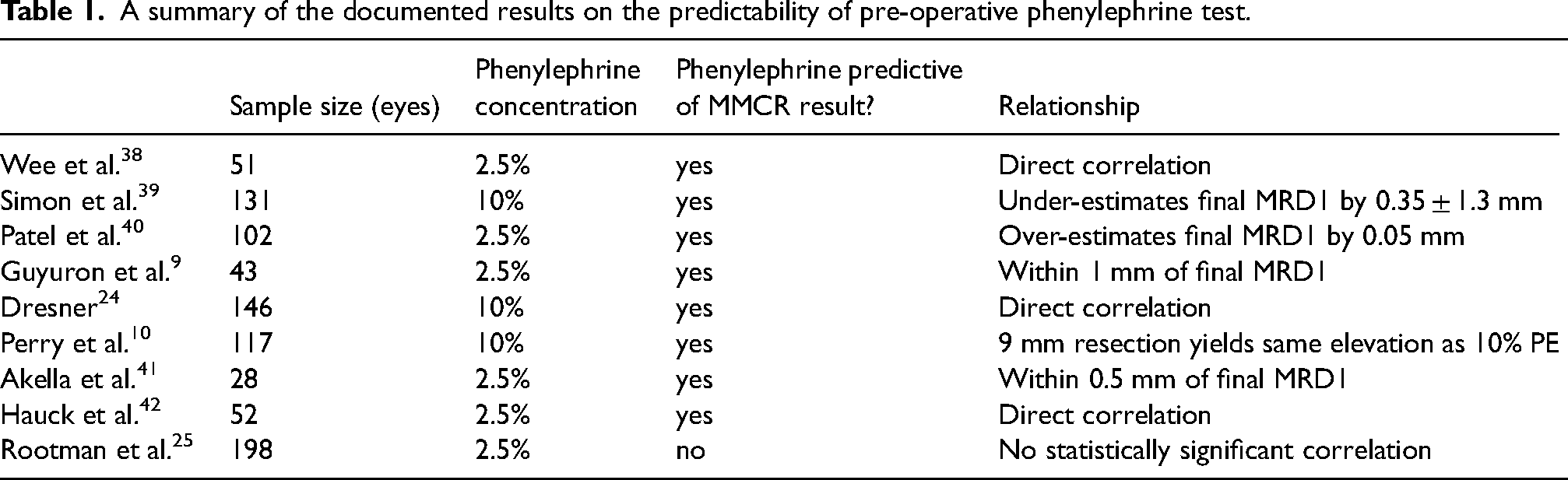
Patients who responded to Phenylephrine drops by 2 mm or more had higher post-operative MRD-1 with an average of 2.41 mm versus 1.19 mm and 1.21 mm in those who responded less than 2 mm or not at all respectively. 38
Another study of 15 patients demonstrated successful MMCR results despite the failure of elevation on the pre-operative Phenylephrine test. 7
According to Guyuron et al, the predictability of the Phenylephrine test was accurate within 1 mm in 92%. 9 Dresner also relies on the predictability of the 10% Phenylephrine test response to titrate the amount of Müller muscle resection which is discussed in detail in the following paragraph. Dresner also promotes a pre-operative Phenylephrine test to assess contralateral eyelid changes with Hering's law. This allows for better pre-operative planning and reducing the amount of resection to minimize contralateral ptosis. 24
The 2.5% Phenylephrine test was found to be highly predictive of post-operative MRD1 as results fell within 0.2–0.5 mm in 2 different studies.41,42 Additionally, such results were also similar in a study by Patel et al who found Phenylephrine to overpredict postoperative MRD1 by 0.05 mm when 8–9.5 mm resection was undertaken with a study documenting the predictability to OR = 0.40.40,43 In fact, in the largest prospective study of 229 eyelids, Phenylephrine was the only significant predictor of post-operative success (OR = 2.69). 44 Literature reviews have concluded that in cases with ptosis <3 mm and a positive response to phenylephrine test with good LPS muscle function, MMCR is more predictable and reproducible than aponeurotic surgery.45,46
Pre-operative Phenylephrine was also able to predict the cosmetic appearance of skin fold and eyelid contour. 42 Such a claim was not analyzed by an impartial third party through a double-blind masked study. It was noted that a positive Hering's law with a Phenylephrine test cannot predict the post-operative response. Therefore surgical intervention should only be done on the initial ptotic eyelid regardless. 47 In conclusion, the majority of studies agree with the predictability of Phenylephrine to assess postoperative eyelid and advise titration of resection based on the amount of response.
Amount of Müller muscle resection
The average length of the Müller muscle is 10–12 mm. As previously mentioned, when MMCR was first introduced a standard 8 mm resection was advised. Another classic formula was the 4:1 mm which entails that for every 4 mm tissue resected the expected elevation is 1 mm. (48) Other reports quantified that every 1 mm of muscle resection resulted in 0.19 mm elevation while some even reported a higher response of 0.25 and 0.32 mm elevation.9,48–50
Surgeons tried multiple different algorithms in their practice to titrate the ptosis correction level to the desired outcome. (Table 2) Dresener formulated that titration of muscle resection can be based on the Phyelephrine response. If the response was 2 mm or greater eyelid elevation, a 4 mm resection for every 1 mm of ptosis. Higher and lower resection amounts were advised if the Phenylephrine response was less than or greater than 2 mm respectively. 24 The relationship between the exact amount of Müller muscle resection and the resultant eyelid elevation was studied. Rootman et al concluded that the length of tissue resection does not play a direct role in the amount of eyelid elevation post-MMCR surgery despite comparing a wide range of resections (4–9 mm).5,25 Because MMCR is believed to be a dynamic system; in the case of asymmetrical ptosis, the resection amount and surgical technique did not predict postoperative outcomes. 51 Others however did find the amount of resection to be a significant independent predictive factor for the success of MRD-1 similar to the linear relationship described by Dresner et al (Table 2).24,52
The relationship between the amount of müller muscle resection and final eye lid elevation based on different author experiences.
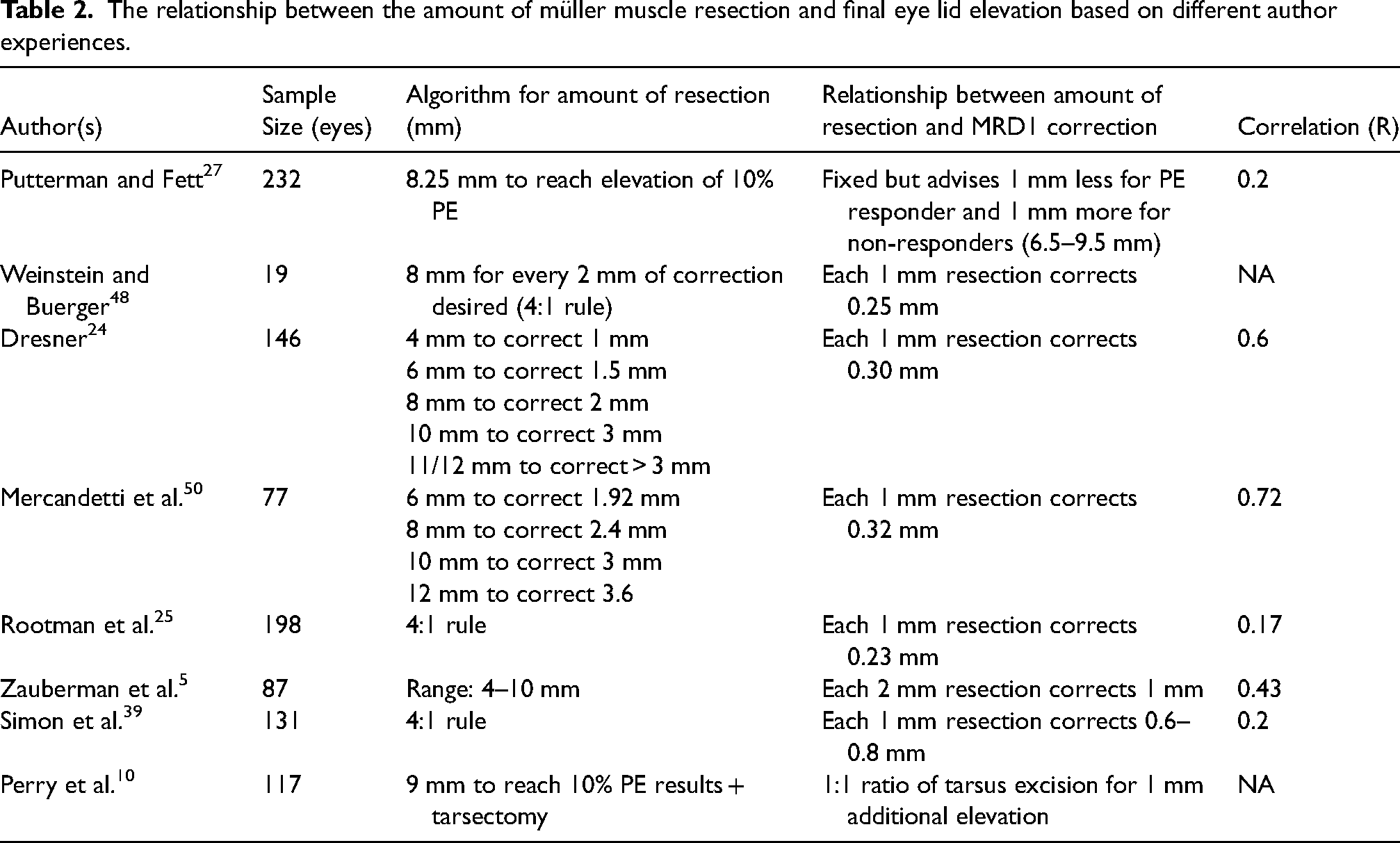
Perry et al concluded that a 9 mm MMCR resection will result in the same eyelid elevation obtained after a 10% Phenylephrine test. For any additional elevation required, he advised the addition of tarsectomy 1:1 mm ratio without exceeding 2.5 mm in order not to compromise eyelid stability. With this formula, Perry was able to achieve 87% outcome predictability. 10 A success rate of 93.1% of eyelid symmetry within 0.5 mm was found using Perry's suggested formula in another study by Karabulut et al. in 58 eyes without the addition of tarsectomy. In this particular study, the amount of resection was purely calculated according to the amount of post Phenyelphrine eyelid symmetry regardless of the amount of ptosis. 53
Final MRD-1 change however was found to relate more directly to the pre-operative MRD-1 (r = 0.5,0.3). It was noted that the higher the initial MRD-1, the lower the amount of eyelid elevation.25,43,50 It can be argued that with higher pre-operative MRD1, the amount of correction planned was minimal thus contributing to this finding. Nevertheless, regression analysis isolating the amount of resection to the amount of change in MRD1 failed to show a strong relationship. 25 It has been estimated that for every 2 mm resection, the MRD1 was elevated by 1 mm when the resection was within the 4–10 mm range. 5 Similarly, Patel et al found no difference in the amount of eyelid elevation with different amounts of resection with an average of 2.30 mm improvement of MRD1 regardless. It is important to note that in this study the resection range was narrow (8–9.5 mm). 40 Roelof et al compared 3 different MMCR surgical algorithms. They compared the outcome in 3 groups: the standard 4:1 ratio, the fixed 7 mm resection, and the 7 mm resection combined with an additional 1 mm tarsectomy. They found no difference between the 3 groups as they had similar outcomes with no direct correlation with the amount of tissue resected. 51 The exact relationship between the amount of tissue resection and the final eyelid elevation after MMCR is still a controversial topic with no uniform agreement amongst surgeons.
Outcome and complications
The success rate of MMCR ranges from 72% to 95%, with high patient satisfaction reported in most studies.3,24,38,39,44,45,49 Success is defined as MRD1 of 2.5 mm or greater. In a single study, the success rate in mild-moderate ptosis was 88% of postoperative MRD-1 ranging from 2.5 to 5 mm. Whereas, the severe ptosis group had a success rate of 70% despite 11 mm resection. The predictive factors for success were pre-operative MRD1 as well as the amount of tissue resection. 52 The lowest success rate reported for MMCR was 65% by Dan et al in a large cross-sectional study of 315 eyes.; Nevertheless, 83% achieved successful eyelid symmetry. This study had a higher sample size and varying pre-operative responses to Phenylephrine. Although different outcome results between males and females have not been commonly reported, Dan et al found female sex to be a positive predictor of MMCR success. 44
The exact range of eyelid elevation after MMCR is variable. Reports suggesting an average of 1.5 mm, 2.1 mm, or even 3.5 mm MRD1 elevation have been stated.9,25,33,39 Guyuron et al suggest that for each 1 mm resection, the eyelid elevates by 0.25 mm. 9 Mercandetti et al found an average elevation of 2.5 mm and 3.2 mm when a classic 8 mm resection is performed versus a maximal 10 mm respectively. 50 In a 10-year study by Putterman and Fett noted that 82% had an average MRD1 of 2.5 mm postoperatively. Interestingly, 100% of congenital ptosis eyelids achieved 1.5 mm of the level of the opposite eyelid post-MMCR as opposed to only 90% in acquired ptosis. 27
Complications of MMCR are uncommon including over-correction, under-correction, eyelid contour abnormalities, corneal abrasions, and dry eye syndrome. The incidence of these complications can be minimized by careful preoperative assessment and intraoperative adjustments 45 Corneal abrasion was reported to range from 1.3% to 3.80% with the classic suture-MMCR.44,50 Transient post-operative SPKs may also occur and are often believed to be suture-related. 24 The immediate post-operative success does not prevent future recurrences with some ptosis recurrence presenting 1 year after the procedure's success. 39 In severe ptosis cases, the recurrence of ptosis after MMCR occurred at an average of 27 months versus 16.8 months after ELR. 29
While very few discussed lagophthalmos in their post-operative results, Akella et al reported a 21% lagophthalmos in the early postoperative period. Complete resolution was noted and none of these patients developed corneal complications. 41 In a few studies. lagophthalmos was reported to have an occurrence of 0% in traditional MMCR as well as single-suture MMCR technique.11,49,52 Although under-correction is believed to be more often encountered after MMCR, cases of over-correction have also been reported. In one study, one patient with over-correction naturally returned to achieving symmetry over a 2-year follow-up. 9 While some patients with over-correction and significant eyelid retraction did require subsequent recession. 39 In fact, Similar rates of over-correction (6.4%) and under-correction (6.4%) were observed by Karesh et al. Cases of under-correction were treated successfully with a repeat MMCR.29,54 A lower rate of under-correction of 3.4% was reported in a prospective study and they did require additional surgical interventions. 44 Comparable rates of under-correction (2.3–2.9%) have been recorded with the suture-less MMCR.13,19
Repeat MMCR is usually successful with one study reporting a mean MRD-1 elevation of 1 mm after repeat MMCR. 54 A large retrospective study of 409 patients assessed the rate of revision surgery for under-correction post-initial MMCR. The prevalence of under-correction was 4.4%. Successful correction reaching 3.44 mm MRD1 was achieved in repeat MMCR while 2.35 mm was achieved in those who underwent subsequent ELR. Furthermore, patients who underwent repeat MMCR did not require further intervention, but 2 patients from the ELR surgery group underwent a third reoperation for under-correction. Karlin et al concluded that secondary MMCR and ELR had successful outcomes after the initial surgery with comparative results, but the contour differences were not thoroughly compared. 55 Simon et al found no changes in eyelid crease after MMCR. 39
Unlike standard ptosis correction procedures, MMCR was weakly associated with changes in MRD-2. A study analyzing the position of the lower eyelid post-operatively found a slight increase in MRD-2 by an average of 0.51 mm. 56
Post-operative infections are rare with limited mention of their incidence in the literature. A case report of an atypical post-operative Mycobacterium (M. Chelonae) infection was reported 4 weeks after the initial operation.
Remarkably, MMCR has a low rate of reported complications with some studies reporting 0 rate of complication even after undergoing this procedure twice in the same eye. 54 Although there is substantial information on the short- and medium-term effects of MMCR, there is a lack of long-term data.
MMCR versus other blepharoptosis surgeries
MMCR is often compared to other surgical techniques for ptosis correction, such as External Levator Advancement (ELA)/Resection (ELR). Largely, MMCR is viewed as less invasive with a shorter recovery time. Frontalis sling procedures are typically reserved for patients with congenital ptosis or in patients with severe LPS dysfunction. 57 Given this different indication, no comparison between Frontalis sling MMCR has been conducted.
MMCR was compared to traditional external approach LPS procedures including ELA and ELR. In a systemic review, there was no significant difference in post-surgical MRD-1 measurements. MMCR was found to be simpler, more reliable, and less prone to complications, thus strongly recommending it for mild to moderate cases of ptosis that responded well to phenylephrine. On the other hand, ELA had a higher incidence of over-correction and subsequent need for surgical revision. A thorough review by Karam et al summarizes all previous studies comparing ELA with MMC in a table. 46 In Asians, ELA had better final MRD1 levels over MMCR (2.93 vs 1.75 respectively). 58 In asymmetrical cases after unilateral ELA, contralateral MMCR was later performed. The choice to undergo MMCR in such cases was due to the presumed notion that the resultant contralateral ptosis is related to decreased sympathetic innervation from Hering's law. The desired symmetrical outcome was achieved in 92.3%. 59 Even in cases with residual ptosis after ELA, MMCR successfully improved MRD1 as a secondary procedure with only 1 case of 1 mm overcorrection. 60
Karam et al found no distinction in aesthetic results in their review. However, improved cosmetic outcomes and more favorable eyelid contours were previously observed in the MMCR group.39,58,61 Cabuk et al, added an objective contour analysis comparison between MMCR and ELA using Bezier curves and four control points. They found a similar temporal shift of the contour peak in both surgical groups. However, subjective cosmetic results were better in the MMCR group. 62 Another similar digital method integration of contour assessment found equal central MRD1 in both ELR and MMCR groups. Yet, there was higher elevation laterally in the ELR group and a flatter contour in the MMCR. 63 Allen et al further summarized that ELA results were less predictable and with higher rates of reoperation when compared to MMCR. Better eyelid contour decreased surgical time and faster healing were additional documented advantages. 45 Moreover, posterior approach surgeries have less risk of injuring sensory nerves within the orbicularis muscle as well as distal branches of the facial nerve. The disadvantage of MMCR in comparison to other surgery is its limited amount of elevation and the need for an additional incision when combined with blepharoplasty. 45
MMCR with blepharoplasty
In some instances, MMCR procedure may be combined with a simultaneous blepharoplasty in patients with dermatochalasis. Most authors noticed no significant difference in the desired outcome with the addition of blepharoplasty.14,19,29,39,64 Alternatively Brown et al found that when MMCR is combined with blepharoplasty, the final eyelid elevation is reduced by approximately 1 mm and advises increasing the resection amount when combining it with blepharoplasty. 65 The discrepancy in results may be due to the incorporation of fat excision and septal violation in some cases thus altering the desired effect. There is no other study to support such a finding.
MMCR in ocular surface disease
As MMCR encompasses conjunctival tissue, there has been concern regarding its implications in patients with glaucoma. Various studies analyzed MMCR in patients with glaucoma filtering blebs and glaucoma drainage. No bleb-related complications in the early postoperative period were reported after the MMCR procedure in any of these patients and they concluded that MMCR was a safe procedure in eyes with previous glaucoma surgeries.66–68 Still, bleb failure after MMCR did occur during the 1-year follow-up period after MMCR in 10.3% (3 patients). 66 A case report of 3 patients on long-term antiglaucoma drops, developed conjunctival scarring, symblepharon, and after MMCR. These patients needed prism correction and 2 patients underwent symblepharon release with mucous membrane graft. It hypothesized that the patients were likely to have pre-operative subclinical conjunctival inflammation and scarring which was further aggravated by MMCR. 69 A case of prolonged foreign body sensation post-MMCR that lasted up to 6 weeks in a patient with filtering glaucoma bleb was reported. One lone transient anterior chamber (AC) reaction case after MMCR was found. They hypothesize MMCR could have triggered bleb-related inflammation which had spillover to the AC. 67
Histopathological comparison of conjunctiva status in those that had undergone MMCR to a control group was conducted in patients aged 48–79 years on an average of 24 months after surgery. Subepithelial fibrosis and inflammation were noted in the post-MMCR group. Goblet cell count was 39 cells/mm in untouched conjunctiva as opposed to 7 cells/mm in the MMCR group. This confirms histological damage and alteration to conjunctiva after MMCR. 70 Whether MMCR increases the risk of dryness or not is not fully known. A study comparing dryness post-MMCR with blepharoplasty versus blepharoplasty alone found no significant difference in both groups. They utilized objective tests like tear production, corneal staining, and Tear breakup time (TBUT) to support their finding. 71 A similar study utilized a subjective dry eye questionnaire, objective assessment of Schirmer, TBUT, corneal staining, and meibomian gland disease (MGD) staging, and found no significant change as well. It added impression cytology from temporal and nasal conjunctiva which failed to report any change in goblet cell densities. 72 Although Dailey et al found no significant effect on tear production by the Schirmer test, there was a transient increase in the subjective symptoms of dryness post MMCR in their sample.38,73 Other studies did however find an increase in objective and subjective feelings of dryness.56,71,74 In patients with ocular surface disease, it is important to note that 1 patient with Reis-Bucklers disease developed a corneal abrasion following the MMCR procedure. 68 The presence of a Boston Keratoprosthesis (KPro) is not a contraindication to undergo MMCR. A case series concludes that MMCR is safe and successful in patients with KPro. Careful patient selection however is recommended with aiming towards post-operative under-correction to protect the integrity of the KPro. 75
Additionally, MMCR was found to have a positive effect on the corneal topography by flattening the superior cornea and restoring it to its normal configuration in patients with pre-operative corneal steepening from the ptotic eyelid pressure. 76 This was noted in patients who had steepening of the cornea as a result of the pressure of the upper eyelid. With such contradictory results when it comes to the effects of MMCR on ocular surface diseases, precaution should be taken and proper patient selection by the surgeons is still warranted.
Conclusion
MMCR is an effective and safe surgical technique for the correction of mild to moderate upper eyelid ptosis with good LPS muscle function. The selection of appropriate candidates and an individualized surgical approach are crucial for achieving optimal outcomes. MMCR can achieve successful outcomes in aponeurotic and congenital ptosis cases. Pre-operative Phenylephrine test response can be predictive of post-operative results and is strongly advised for all patients with a planned MMCR to titrate the amount of resection and predict the outcome and symmetry success. The amount of tissue resection may not be directly related to the eyelid elevation achieved but multiple formulas have been advised. The amount of resection can be titrated based on the degree of ptosis or the Phenylephrine response with successful results reported in each method despite the controversy among different surgeons.
Larger, multicenter prospective studies would help to provide more robust evidence on the efficacy and safety of MMCR as well as quantify predictive factors for success. Additionally, the development of standardized outcome measures and the incorporation of patient-reported outcomes would facilitate the comparison of different surgical techniques and enhance the understanding of patient satisfaction.
Further research is needed to investigate the long-term results, especially on conjunctival surface changes and recurrence rates.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.